

Abstract
Background:
The need for a correct follow-up for medical advices of health givers is the cornerstone for avoiding drug-related complications in especial period of elderly people life. There isn’t any data about drug therapy regimens adherence of elderly people of Isfahan. In this study, we aimed to cover this deficit.
Materials and Methods:
In this cross-sectional study which was carried out in Isfahan (Iran) in 2013 senior citizens (aged 65 or more) who were taking at least one medication and had no record of residency in nursing homes were included. We used Morisky medication adherence scale (after validation and reliability assessment for using this questionnaire in Persian language) to evaluate the level of adherence in the study population.
Results:
A total of 200 elderly participants were fully studied (n = 200, 61% females), and 52% of them had poor medication adherence. 77.5% of participants were suffered from at least four medical illnesses, and 18.5% of them were taking more than eight medications per day. We have not found any significant statistical relationship between vision or hearing loss disorders and the medication adherence of the participants). There was a significant positive relationship between the level of education and medication adherence (P = 0.001), (χ2 = 0.29).
Conclusion:
Low Medication adherence is a common and important drug issue in the elderly in Isfahan. This issue can lead to medical complications and huge cost if it is not addressed appropriately.
Keywords: Aged patients-Iran, medication adherence, patient compliance
INTRODUCTION
Human aging is an important issue worldwide, and the growth of the elderly population is increasingly progressive in many parts of the world.[1,2,3,4,5,6] This means that soon or late the population of over 65 years old in these countries will proceed the population of under 14-year-old youngsters which may be attributed in some parts to the improvement of health care facilities and medical supports in these countries.[7] Today, more than half of the world's elderly population are living in Asia and will continue to rise till 2025[4] according to united nations’ definition.[3] Iran with a more than 5 million inhabitants aged more than 60 years old (7.3% of the whole population) is taking its way to have an old population of inhabitants in the near future which could be considered as the direct result of the health promotion policies of the government in recent years.[8,9,10,11,12,13,14]
The process of aging in human biologic systems makes the elderly years of life companion with a more than ever needed health seeking behavior and poly-pharmacy practice for this population is a common problem which should be considered with great concern.[15] Although pharmacotherapy along with other treatment measures (e.g., physiotherapy, psychotherapy and etc.) tries to upgrade the quality-of-life in this special population of the society but still drug-based treatments has its major role in this regard.[5] Drug therapy is an important choice in most medical treatments, and its appropriate use can ensure effective treatment and improved health. Inappropriate medication use entails high harmful medicinal reactions and a need to more health care. Patients may receive various medicines, which, in turn, may increase harmful effects especially in patients with multiple diseases.[16,17,18] In the United States, the elderly receive 33% of all the prescribed medicines although they only form 13% of the American population.[2] Iran is also considered among the world's top 20 countries with highest visits to doctors and medicine prescriptions.[19,20,21] Obviously, seeking for a prescription and filling it in a pharmacy is not the whole story for the sake of health improvement in the elderly and it is of more importance to accomplish the details of usage for the prescribed drugs as directed by the physician and the pharmacy. In other words, patients should comply with and adhere to the recommended drugs in practice. This is called drug adherence which is also a worldwide issue for concern in geriatric care.[22]
Adherence refers to a consistent agreement between the prescriber and the patient and estimates correct observance and implementation of medicinal orders. It also denotes the consistency in taking medicines during the course of treatment.
Many factors are considered as obstacles for a good and consistent drug adherence in geriatric population and the most important of them is that these patients normally live alone in the house and obtaining the drug from a near pharmacy, keeping them in a suitable place (e.g., cold, dry, and not under direct sunrise) and remembering the correct time and the correct dose of drugs are all really difficult for them. The other problem is some co-morbidities such as hearing loss and visual loss in these ages which makes it difficult to understand the correct details of drug use from the physician or the pharmacist. They also may be shy of asking for what they have not understood. Rheumatologic problems is another obstacle for the patient for obtaining the drug and also to take it on time.[10] Unfortunately, it is estimated that more than 5% of hospital admittances and 1–3% of emergency visits pertain to inappropriate medication consumption.[15]
Adherence researches for drug utilization in the geriatric population are previously done in many countries[22] but published data from Iran for this population do not seem enough. Serving as the capital of Iran, the metropolitan of Tehran offers many job vacancies and unique health care facilities which makes it different from a normal and consistent population of inhabitants. There is a population difference of about 3 million between the day population and the population at night. These make the investigation of drug adherence with a reasonable sampling distribution very difficult and for this reason we have chosen Isfahan for our study. Isfahan is the second large city of Iran with about 2.5 million inhabitants and is considered with a high level of social community standards and health facilities with 6.9% of geriatric inhabitants in 2012.[6]
Considering the recommendations of the World Health Organization to investigate national and regional health behaviors and health plan for each community, and due to the fact that in spite of many studies on drug utilization patterns in Iran, considering the cultural differences between provinces there isn’t any study on medication adherence among elderly people (65 and older) in Isfahan, therefore, the aim of this study was to investigate the drug therapy regimens adherence and its relationship with demographic and contextual traits of elderly people of Isfahan.
MATERIALS AND METHODS
In this cross-sectional study which was carried out in Isfahan (Iran) in 2013 till November to January senior citizens (aged 65 or more) who were taking at least one medication and had no record of residency in nursing homes were included.
Based on the estimating proportions statistical formula for calculating the needed sample size for estimating a trait (adherent/nonadherent)[11] and considering a 5% margin of error and preassumption of 50% nonadherence (P = 0.5, for estimating the maximum needed count), 200 human subjects were needed to be included in this study.
We used random cluster sampling. 20 clusters were chosen of health centers in the city. The first address in each cluster was determined randomly. Regarding the research ethics, the researcher explained the purpose of research to the subjects or their caregivers and their written permission was collected. The subjects were briefed on the purpose of the research, and their written consent was taken. Permission to conduct the research was granted by vice-chancellor for research and vice-chancellor for health in Isfahan University of Medical Sciences.
Data collected through interviewing the participants or their caregivers. We have recorded the demographic data of the study participants including age, sex, occupation, health insurance, sight or hearing disorder, education, number of health problems, and number of medicines taken. For measuring the adherence of the elderly participants to their drug therapy regimens we used the Morisky medication adherence questionnaire which includes eight questions (Yes: 1 and No: 0) for determining the adherence at three levels: Low (2<), average (1–2), and high (0).[12] The questionnaire was translated into Persian language and later back-translated into English to ensure the precision by a bilingual. Validity of the tools for data collection was measured using content validity method based on the comments of 10 academic members of nursing and midwifery and pharmacology schools.
Reliability of the tools was achieved determining Chronbach's alpha coefficient after a pilot study on 10 subjects (α = 0.84). Data were analyzed using SPSS version 22(IBM Corp.: Armonk, NY) and descriptive-inferential statistics. To render the description of the data, frequency distribution, mean, and standard deviation tables were used. To analyze and show the relationships, Chi-square and Pearson indexes were applied.
RESULTS
In this study, we have studied a total of 200 elderly participants. More than half of the elderly were females. 67.5% of participants placed at younger old group (65–74) and 0.5% of them placed at older old group (>95 year).
43.6% of the participants had the Iranian social security insurance coverage for the private sector and 32% had the insurance coverage for the governments’ employees and others had other kinds of insurances and 0.6% announced they have no insurance coverage.
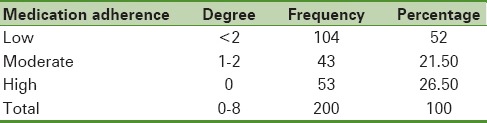
More than one-half of the total participants (52%) showed low medication adherence [Table 1].
Table 1.
Frequency of medication adherence among the study participants according to the Morisky medication adherence scale
About 75% of the elderly had sight disorder and 50% of them had overcome it using glasses, medical lens or have previously done ophthalmologic surgery.
About one-third (33.5%) of elderly had apparent hearing disorders.
We have not found any significant statistical relationship between vision or hearing loss disorders and the medication adherence of the participants (P = 0.09 and P = 0.29, respectively).
More than two-third (77.5%) of participants were suffered from at least four illnesses, and 18.5% of them were taking more than eight medications on a daily basis.
Our findings showed 65.6%of participants were illiterate or with a minimum capability of reading and writing. Among the elderly with low medication adherence, more than two-third (77%) were illiterate, but 56% of the elderly with high medication adherence had at least elementary or even university level of literacy. We found a positive and direct statistical relationship between the literacy of the participants and medication adherence (χ2 = 0.29, P = 0.001) [Table 2].
Table 2.
The relationship between the literacy and medication adherence in the study participants

DISCUSSION
In this study, we have investigated medication adherence to drug therapy regimens in a random cohort of Isfahanian elderly people. Our results indicated a weak medication adherence, so only one-fourth of participants demonstrated a high level of adherence. Lack of medication adherence is a fairly common problem in other parts of the world as well. The world's medication adherence among 60 years old and above is between 41% and 74%.[14] In a research by Jackevicius et al. aiming to investigate medication adherence among the elderly with acute coronary syndrome, it was shown that only 40% of the subjects were adherent to medication use despite their special clinical condition.[9]
It is estimated that more than 5% of hospital admissions and between 1% and 3% of emergency referrals pertain to inappropriate medication use. Those with better medication consumption (80–100%) are less likely to be hospitalized following a health problem.[1] This is a fact that patients who take their medicines regularly and are hopeful about the treatment procedure experience fewer medical problems.
Vision capability plays an important role in adherence to medication use. Ability to see and spot medicines can affect medication adherence and the disease. Therefore, for the sake of a good medication adherence, the elderly need to be able to read and understand the medication orders, doses, consumption time, and side effects.[19]
Based on the present study, a quarter of the subjects suffered from vision loss disorders which were not possible to be corrected even with glasses, contact lenses, surgery and, etc. Furthermore, one third of the participants had hearing-impairment and only a few of them worn hearing aids. In the cohort of elderly people we have studied, only 19% did not suffer from hearing or vision loss disorders. Ability to hear medicinal orders of the pharmacist or the caregiver is critical for medication adherence. An elderly may not be able to hear his/her health provider's advice about disposing of old medicine well. In the present study, there was no significant relationship between sight and hearing problems and level of medication adherence.
Ability to read can also affect medication adherence. Most of the times, medicinal orders which are written on drug packages cannot be read correctly by the elderly. Based on the findings of the present study, medication adherence corresponds to the level of education in the elderly. In a study conducted by Shokri in Isfahan, there was a positive direct relation between education level and cooperation in medicine consumption.[20] Mårdby et al. had also similarly showed that there was a direct significant relation between the level of patients education and medication consumption cooperation.[13] Therefore, the findings of this study provide a valuable source for the planning for improving medication adherence in elderly people of Isfahan.
Our study had some limitations. Access problem for the researcher to reach the elderly, poor communication desire in these elderly patients (especially in men) was among the most important ones. We suggest a larger study with the help of the local authorities and also performing some educational programs with the theme of drug usage education inside the elderly community of this metropolitan city.
CONCLUSION
Low Medication adherence is a common and important drug issue in the elderly in Isfahan. This issue can lead to medical complications and huge cost if it is not addressed appropriately. Medication adherence seems to be related to the education level of the elderly drug users. Therefore, planning for trainings and educational programs on the significance of proper medication use in the elderly may help to improve the health in this senior population.
Financial support and sponsorship
Faculty of Nursing and Midwifery, Isfahan University of Medical Science, Iran.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This study was a thesis research for M. Sc. degree in Geriatric care nursing which was financially supported by the vice-chancellery of research at the Isfahan University of Medical Sciences. Authors would like to thank all authorities and colleagues who helped sincerely during the research period and especially all those elderly senior citizens who accepted to participate in the study.
REFERENCES
- 1.Barnett K, McCowan C, Evans JM, Gillespie ND, Davey PG, Fahey T. Prevalence and outcomes of use of potentially inappropriate medicines in older people: Cohort study stratified by residence in nursing home or in the community. BMJ Qual Saf. 2011;20:275–81. doi: 10.1136/bmjqs.2009.039818. [DOI] [PubMed] [Google Scholar]
- 2.Büla C. Medication usage in the elderly: Outrage and delight. Rev Med Suisse. 2011;7:2163–4. [PubMed] [Google Scholar]
- 3.De Grey A. D. The desperate need for a biomedically useful definition of “aging”. Rejuvenation Res. 2013;16:89–90. doi: 10.1089/rej.2013.1428. [DOI] [PubMed] [Google Scholar]
- 4.Diamond J. Population history: Human melting pots in Southeast Asia. Nature. 2014;512:262–3. doi: 10.1038/512262a. [DOI] [PubMed] [Google Scholar]
- 5.Eckardt R, Steinhagen-Thiessen E, Kämpfe S, Buchmann N. Polypharmacy and drug prescription in the elderly. Strategies for optimization. Z Gerontol Geriatr. 2014;47:293–301. doi: 10.1007/s00391-013-0562-0. [DOI] [PubMed] [Google Scholar]
- 6.Golestannejad A. Isfahan Statstical Year Book. Vol. 1. Isfahan: Isfahan Municipality; 2013. pp. 41–92. [Google Scholar]
- 7.Huber M, Blumberg A, Chatterjee S, Haenisch B, Schlosser-Weber G, Broich K. Drug safety: Challenge in an aging society. Nervenarzt. 2014;85:1352–62. doi: 10.1007/s00115-014-4088-5. [DOI] [PubMed] [Google Scholar]
- 8.Imani-Nasab MH, Seyedin H, Majdzadeh R, Yazdizadeh B, Salehi M. Development of evidence-based health policy documents in developing countries: A case of Iran. Glob J Health Sci. 2014;6:27–36. doi: 10.5539/gjhs.v6n3p27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA. 2002;288:462–7. doi: 10.1001/jama.288.4.462. [DOI] [PubMed] [Google Scholar]
- 10.Lo R. Geriatric pharmacotherapy: Problems with adherence. Int J Psychiatr Nurs Res. 2001;7:806–14. [PubMed] [Google Scholar]
- 11.Normand SL, Zou KH. Sample size considerations in observational health care quality studies. Stat Med. 2002;21:331–45. doi: 10.1002/sim.1020. [DOI] [PubMed] [Google Scholar]
- 12.Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens (Greenwich) 2008;110:348–54. doi: 10.1111/j.1751-7176.2008.07572.x. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 13.Mårdby AC, Akerlind I, Hedenrud T. General beliefs about medicines among doctors and nurses in out-patient care: A cross-sectional study. BMC Fam Pract. 2009;10:35. doi: 10.1186/1471-2296-10-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Miller CA. Nursing for Wellness in Older Adults, Latin Book. 5th ed. Philadelphia: Publish by Wolters Kluwer Health/Lippincott Williams & Wilkins; 2009. pp. 305–408. [Google Scholar]
- 15.Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf. 2014;13:57–65. doi: 10.1517/14740338.2013.827660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.McLaughlin SJ. A Public Health Approach to the Challenges of an Aging Society. Gerontologist. 2014;9(7):723–34. [Google Scholar]
- 17.Merchant EK. Global population: History, geopolitics, and life on earth. Glob Public Health. 2015;10:129–31. doi: 10.1080/17441692.2014.976241. [DOI] [PubMed] [Google Scholar]
- 18.Mannucci PM, Nobili A REPOSI Investigators. Multimorbidity and polypharmacy in the elderly: Lessons from REPOSI. Intern Emerg Med. 2014;9:723–34. doi: 10.1007/s11739-014-1124-1. [DOI] [PubMed] [Google Scholar]
- 19.Son KY, Park SM, Lee J, Kim CY. Difference in adherence to and influencing factors of a healthy lifestyle between middle-aged and elderly people in Korea: A multilevel analysis. Geriatr Gerontol Int 2014. Geriatrics & Gerontology International. 2014:1–11. doi: 10.1111/ggi.12335. PMID: 25256663. [DOI] [PubMed] [Google Scholar]
- 20.Shokri S. The Compliance of Dialysis Patients with their Treatment Regimens [Thesis for PharmD degree], in Department of Clinical Pharmacy and Pharmacy Practice. Iran: Isfahan University of Medical Sciences; 2009. p. 94. [Google Scholar]
- 21.Shariatirad S, Maarefvand M. Sanctions against Iran and the impact on drug use and addiction treatment. Int J Drug Policy. 2013;24:636–7. doi: 10.1016/j.drugpo.2013.04.003. [DOI] [PubMed] [Google Scholar]
- 22.Tsai KT, Chen JH, Wen CJ, Kuo HK, Lu IS, Chiu LS, et al. Medication adherence among geriatric outpatients prescribed multiple medications. Am J Geriatr Pharmacother. 2012;10:61–8. doi: 10.1016/j.amjopharm.2011.11.005. [DOI] [PubMed] [Google Scholar]