

Abstract
Background
Death anxiety is regarded as a risk and maintaining factor of psychopathology. While the Arabic Scale of Death Anxiety (ASDA) is a brief, commonly used assessment, such a tool is lacking in Chinese clinical practice.
Aim
The current study was conducted to develop a Chinese version of the ASDA, i.e., the ASDA(C), using a multistage back-translation technique, and examine the psychometric properties of the scale.
Methods
A total of 1372 participants from hospitals and universities located in three geographic areas of China were recruited for this study. To calculate the criterion-related validity of the ASDA(C) compared to the Chinese version of the longer-form Multidimensional Orientation toward Dying and Death Inventory (MODDI-F/chin), 49 undergraduates were randomly assigned to complete both questionnaires. Of the total participants, 56 were randomly assigned to retake the ASDA(C) in order to estimate the one-week, test-retest reliability of the ASDA(C).
Results
The overall Cronbach’s alpha was 0.91 for the whole scale. The one-week, test-retest reliability was 0.96. Exploratory Factor Analysis (EFA) revealed three factors, “fear of dead people and tombs,” “fear of lethal disease,” and “fear of postmortem events,” accounted for 57.09% of the total variance. Factor structure for the three-factor model was sound. The correlation between the total scores on the ASDA(C) and the MODDI-F/chin was 0.54, indicating acceptable concurrent validity.
Conclusions
ASDA(C) has adequate psychometrics and properties that make it a reliable and valid scale to assess death anxiety in Mandarin-speaking Chinese.
Keywords: Arabic Scale of Death Anxiety, Chinese version, psychometric properties
Abstract
背景
死亡焦虑被视为精神病理学症状的风险因素和 持续存在的因素。虽然阿拉伯死亡焦虑量表(ASDA) 是一种简单而常用的评估工具,但是在国内临床实践 中缺少这样的工具。
目标
本研究旨在采用多级回译法开发ASDA 中文版, 即ASDA(C),并研究该量表的心理测量学特性。
结果
量表总的Cronbach’sα 值为0.91。一周后的重测 信度为0.96。探索性因子分析(EFA)显示三个因素,“ 对 死人和坟墓的恐惧,“ 对致命疾病的恐惧” 和“ 对死亡 事件的恐惧”,占总方差的57.09%。因而构建三因素 模型。量表ASDA(C) 总分与MODDI-F/chin 的相关系数 是0.54,表示信度都可以接受。
结论
ASDA(C) 有较好的心理测量学特性,说明这是 一个可靠有效的量表。该量表能用于讲普通话的中国 人群,来评估死亡焦虑。
关键词
阿拉伯死亡焦虑量表;中文版;心理测量 学特性
1. Introduction
Death anxiety is a basic fear underlying numerous psychological conditions.[1]Given the fear of death is described as a “worm at the core” of many mental disorders,[2]such as social anxiety, panic disorders, phobias, and depression, death anxiety is believed to be a trans-diagnostic factor[3] that plays a significant role in the development and degree of severity of a range of anxiety disorders[4] and anxiety-related problems.[5] While death anxiety has been evaluated in many countries, primarily in non-clinical populations[6] of nurses, health care professionals, students, it has also been assessed among individuals facing terminal illness and among patients[7, 8]with anxiety disorders, schizophrenia, and substance addiction.[9] A considerable number of studies reported on the treatment of death anxiety.[10] Greenberg and colleagues[11] claimed that the Terror Management Theory was the leading and most influential approach to death anxiety. The accuracy of outcome measurement for desensitization treatment among students with high death anxiety may be influenced by the choice of death anxiety inventory used,[12] suggesting the importance of using a reliable, valid scale when evaluating the degree of death anxiety.
Tools such as Templer’s Death Anxiety Scale(T-DAS),[13] the Collett Lester Fear of Death Scale(CLFOD),[14] the Spanish Death Anxiety Inventory(SDAI),[15] and the Arabic Scale of Death Anxiety(ASDA),[16] have been developed and demonstrate adequate reliability and validity.
In China, this assessment has not been applied in clinical settings partly because of lackingtools. Chinese culture is influenced by several religious traditions, including Confucianism, Buddhism, and Taoism, that have shaped attitudes toward death. For example, Confucius recommended dedicating oneself selflessly during a limited lifetime, while the Buddha thought of death as a terrifying and mysterious transmigration. Although the Chinese have always avoided discussing death, superstitious thoughts, which are highly prevalent in Chinese societies, are related to death anxiety.[17] With the growing interest in mental health in China, and accumulating evidence to recommend that a death anxiety assessment supplement other measures of mood and psychological functioning[3], it is necessary to develop a scale to assess death anxiety and ensure early treatment of this transdiagnostic construct[3].
In recent years, a Chinese Death Anxiety Inventory(CDAI)[18] was developed based on the T-DAS. The CDAI had been used in the clinical sample in Hong Kong.[19] However, the inventory was developed for Cantonese speakers. Although Cantonese is spoken in Hong Kong, Mandarin is spoken by the majority of Chinese. Since the ASDA is one of the most commonly used self-reporting inventories for death anxiety, it was the basis for our current study. The ASDA consists of 20 statements, whereas the recently developed Multi-dimensional Orientation toward Dying and Death Inventory (MODDI-F/chin)[20, 21] consists of 47-items and is more time-consuming. Although the ASDA was developed in Arabic, it has been translated into and validated in other languages, including Spanish, English,[22, 23] and Turkish (unpublished).
We aimed to examine the psychometric properties of the ASDA Chinese version, i.e., the (ASDA (C)) using a sample population of Chinese medical staffs and undergraduates in three different parts of mainland China. To the best of our knowledge, this is the first study designed to assess the reliability and validity the ASDA (C).
2. Participants and Methods
2.1 Ethical Approval
This study was approved by the Ethics Committee of the Shanghai Mental Health Center. All participants reviewed and signed the written informed consent prior to being included in the study.
2.2 Participants
Participants were primarily medical staff and undergraduates who were recruited from hospitals and universities in three different Chinese provinces: Shanghai, located in the eastern portion of the country; Jiangxi in the central portion; and Heilongjiang in the northern portion. The flow chart of study participation is shown in Figure 1. In total, 1357 participants took part in this study and completed the questionnaire. The convenience sample consisted of 768 university students and 589 hospital staff members. Data collected from 1201 participants (437 men and 764 women) were included in the study; data from 156 participants were excluded because of incomplete questionnaire responses. The ages of participants ranged from 18 to 64 years. To estimate the test-retest reliability, 56 participants were randomly assigned to repeat the questionnaire one week after the initial testing. To test the criterion-related validity, 49 undergraduates were required to also complete the MODDI-F/chin.[21]
Figure 1.
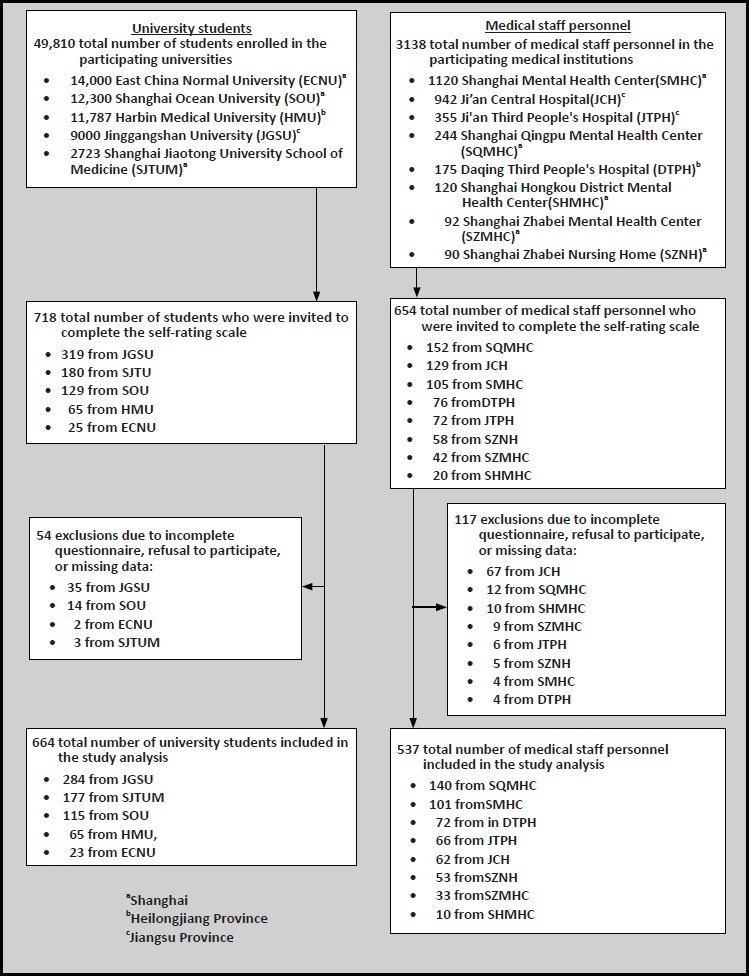
Flowchart of the study
2.3 Assessment tools
2.3.1 The Arabic Scale of Death Anxiety - Chinese Version [ASDA(C)]
The ASDA[16] was developed to assess death anxiety or fear of death, and it was validated in a large sample of undergraduates from three Arab countries: Egypt, Kuwait, and Syria. In its final form, the ASDA consists of 20 short statements. Each item is answered on a 5-point intensity, Likert scale, anchored by 1 = no and 5 = very much. Scores can range from 20 to 100, with higher composite scores indicative of greater perceived death anxiety. The Alpha reliabilities ranged from 0.88 to 0.93; and item-remainder correlations ranged between 0.27 and 0.74. The 1-week, test-retest reliability was 0.90 (Egyptians only), denoting high internal consistency and stability.[16] The ASDA is available in English and Spanish versions.[22, 23] A multistage, back-translation technique[24, 25] was used to develop the Chinese version of the ASDA.[16] The stages of adaptation – including specific items requiring several cycles of translation and back-translation – are shown in Figure 1.
2.3.2 The Multidimensional Orientation toward Dying and Death Inventory (MODDI-F)
The MODDI-F[20] is one of the more recent multidimensional assessment techniques. The 47-item questionnaire was originally developed in German and then adapted for the English language. The tool is based on a 2 × 4 dimensional a priori structure proposed by Collett and Lester with respect to the fear of dying and death and adds a new component on the attitude of acceptance. Each item is rated according to a 4-point Likert scale from 0 (agree not at all) to 3 (agree almost totally). For the German version of the MODDI-F, the internal consistency among a community sample ranged from 0.82 to 0.92.[20] For the Chinese version of the MODDI-F, the internal consistencies of the eight subtests ranged from 0.68 to 0.91.[21] The MODDI- F/ chin was used in the present study as a criterion for the ASDA(C).
2.4 Procedure
Students and medical staff completed the self-rating scale within a class or a department as a group, after giving their informed consent. Forty-nine undergraduates were randomly selected to complete both questionnaires. Of the total participants, 56 were randomly selected to retake the ASDA(C).
2.5 Statistical analysis
All data analysis was conducted using SPSS 19.0 statistical software and Mplus(Version 7; Muthén&Muthén, 2012). The internal consistency reliability was assessed using Cronbach’s alpha coefficient. Test-retest reliability of the scale was examined with the Spearman’s correlation of the two scores obtained one week apart. To test the dimensionality of the ASDA(C), the sample was randomly split into two separate groups. The first group was subjected to an exploratory factor analysis (EFA). The sample adequacy was assessed by the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy. The second group was subjected to a confirmatory factor analysis (CFA). Criterion-related validity of the ASDA(C) was assessed by Pearson correlation coefficients between the factors and total score of the ASDA(C) on one side and the MODDI-F/chin on the other.
3. Results
3.1 Participant characteristics
A total of 1357 participants were enrolled in this study: 768 were recruited from universities and 589 from hospitals. Of the 1357 participants, 1201 completed the questionnaire; 156 participants were excluded because of incomplete questionnaire responses. The demographic details of the total sample are included in Table 1.
Table 1.
Demographic information of participants
| measure | total ((n=1201) |
|---|---|
| Area: 1university in Jiangxi Province; n (%) | 284 (23.6%) |
| 2 hospitals in Jiangxi province; n (%) | 128 (10.7%) |
| 3 universities in Shanghai; n (%) | 315 (26.3%) |
| 5 hospitals in Shanghai; n (%) | 337 (27.9%) |
| 1 university in Heilongjiang province; n (%) | 65 (5.4%) |
| 1 hospital in Heilongjiang province;n (%) | 72 (6.0%) |
| age: mean in years (sd) | 26.6 (9.80) |
| gender: female; n (%) | 764 (63.6%) |
| ethnic group: Han; n (%) | 1188 (98.9%) |
| education: mean in years (sd) | 13.51 (2.45) |
| major: medical staff; n (%) | 537 (44.7%) |
| university students; n (%) | 664 (55.3%) |
| religious: no; n (%) | 1130 (94.1%) |
| ASDA(C) total score: mean (sd) | 42.14 (13.55) |
| medical staff's score: mean (sd) | 41.06 (13.42) |
| university students’ score: mean (sd) | 43.02 (13.60) |
3.2 Reliability
Cronbach’s alpha reliability of the ASDA(C) was 0.91. A sample of 56 participants repeated the ASDA(C) one week later. The 1-week, test-retest reliability was 0.96 for the entire scale. These results indicate high internal consistency and temporal stability.
3.3 Exploratory factor analysis (EFA)
A principal components analysis and Varimax rotation was conducted to study the construct validity, after measuring the sample adequacy by the Bartlett’s test of sphericity (p = 0.0001), and the Kaiser-Meyer-Olkin test (KMO=0.92). For Kaiser criterion eigenvalues greater than 1.0, three factors were identified that accounted for 57.09% of the variance, as shown in Table 2. Factor 1 consisted of 8 items, labeled “fear of dead people and tombs,” (Items 2, 3, 8, 9, 11, 12, 16, and 17) and accounted for 39.84% of the variance. Factor 2 consisted of 7 items, labeled “fear of lethal disease,” (Items 1, 4, 5, 6, 10, 19, and 20) and accounted for 9.66% of the variance. Factor 3 consisted of 5 items, labeled “fear of postmortem events,” (Items 7, 13, 14, 15, and 18) and accounted for 7.58% of the variance. Item loadings ranged from 0.442 to 0.844, as shown in Table 2.
Table 2.
Exploratory factor analysis results of the Chinese version of the Arabic Scale of DeathAnxiety [ASDA(C)] (Half of total sample, n=600)
| factors and corresponding contents of Items | component | ||
|---|---|---|---|
| 1 | 2 | 3 | |
| Fear of dead people and tombs (39.84% of variance) | |||
| Q.3 I fear visiting graves. | 0.827 | 0.114 | 0.058 |
| Q.8 I am afraid of looking at a corpse. | 0.826 | 0.262 | 0.051 |
| Q.2 I fear looking at the dead. | 0.812 | 0.228 | -0.027 |
| Q.12 I dread walking in graveyards. | 0.694 | 0.090 | 0.325 |
| Q.11 Witnessing the burial procedure terrifies me. | 0.688 | 0.199 | 0.379 |
| Q.9 I fear the torture of the grave. | 0.603 | 0.263 | 0.409 |
| Q.17 The sight of a dying person frightens me. | 0.587 | 0.297 | 0.264 |
| Q.16 I get upset by witnessing a funeral. | 0.442 | 0.151 | 0.501 |
| Fear of lethal disease (9.66% of variance) | |||
| Q.19 I am afraid of getting cancer. | 0.098 | 0.844 | 0.134 |
| Q.10 I fear getting a serious disease. | 0.175 | 0.783 | 0.140 |
| Q.20 I fear death. | 0.168 | 0.760 | 0.189 |
| Q.6 I worry that death may deprive me of someone dear to me. | 0.245 | 0.640 | 0.012 |
| Q.1 I fear death whenever I became ill. | 0.100 | 0.537 | 0.325 |
| Q.4 The possibility of having a surgical operation terrifies me. | 0.399 | 0.530 | 0.138 |
| Q.5 I am afraid of suffering a heart attack. | 0.267 | 0.493 | 0.296 |
| Fear of postmortem events (7.58% of variance) | |||
| Q.14 I am afraid of sleeping and not waking up again. | 0.031 | 0.031 | 0.784 |
| Q.13 I am preoccupied with thinking about what will happen after death. | 0.075 | 0.174 | 0.693 |
| Q.18 Talking about death upsets me. | 0.315 | 0.238 | 0.598 |
| Q.7 I am apprehensive of unknown things after death. | 0.234 | 0.344 | 0.544 |
| Q.15 The pain accompanying death terrifies me. | 0.156 | 0.468 | 0.471 |
| Eigenvalue | 7.968 | 1.931 | 1.516 |
| Cronbach’s alpha coefficient | 0.898 | 0.847 | 0.747 |
Q= item numberof ASDA(C)
3.4 Confirmatory factor analysis (CFA)
The CFA was calculated using a maximum likelihood estimation method to examine whether the three-factor model fit the other half sample. The fit of the model was acceptable with the results of the CFA analysis: χ2=1184.175 (df=167, p<0.001). Root Mean square Error of Approximation (RMSEA)=0.099 (90%CI=0.093, 0.104). Comparative Fit Index (CFI)=0.916. Tucker-Lewis index (TLI)=0.905.
3.5 Criterion-related validity
In terms of the scale’s concurrent validity, the correlation between the total scores on the ASDA(C) and the MODDI-F/chin was 0.54 (p < 0.001). The correlation coefficients between the factors of the ASDA(C) and the total score on the MODDI-F/chin ranged from 0.358 to 0.664, as shown in Table 3.
Table 3.
Correlations between factors of the ASDA andthe MODDI-F/ chin (n= 49).
| MODDI-F total | factor 1 | factor 2 | factor 3 | |
|---|---|---|---|---|
| ASDA total | 0.534b | |||
| factor 1 | 0.358a | 1 | ||
| factor 2 | 0.561b | 0.611b | 1 | |
| factor 3 | 0.469b | 0.664b | 0.572b | 1 |
ap<.05 level (2-tailed);
bp<.01level (2-tailed)
4. Discussion
4.1 Main Findings
The participants in our study are a representative sample of the general population as indicated by the fact that 94.1% of participants reported no religious beliefs, which is consistent with results from a 2012 Chinese survey.[26] The participants in the present study were recruited from universities and hospitals. Undergraduates comprised 55% of the sample, while nurses and clinicians accounted for 45%. Health care professionals reported lower levels of death anxiety than undergraduates in the present study, which may be due to the fact health care professionals hold positive attitudes toward death and the dying process during routine work[27].
The average total score of the Chinese version of the ASDA(C) in undergraduates was around 42, which is almost similar to the score of undergraduates from Lebanon, Spain and the United Kingdom, but less than the anxiety reported by undergraduates from Egypt, Kuwait, and Syria.[16, 23] The differences in death anxiety scores among undergraduates might be attributed to country-specific differences in religious beliefs and world views.[28]
Our study shows the Cronbach’s alpha of the ASDA(C) was 0.91 in this sample. Reliability coefficients for other language versions of the ASDA range from 0.86 – 0.93.[16, 29, 30] The test-retest reliability of the Chinese version was 0.96, indicating the ASDA(C) was stable over time.
Previous studies have shown that the ASDA has concurrent validity ranging between 0.60 and 0.74 with Templer’s Death Anxiety Scale.[16] In addition, the Pearson correlations between the total scores on the ASDA and CLFDS were significant among Kuwaiti undergraduates.[31] In the current study, the ASDA(C) is significantly correlated with the (MODDI-F)/chin (r = 0.53, p = 0.0001), which confirms the construct validity of this scale.
With regard to the Egyptian and Syrian samples, the ASDA yielded four factors and were labeled: (a) fear of dead people and tombs, (b) fear of postmortem events, (c) fear of lethal disease, and (d) death preoccupation or death concern.[16] As for the Kuwaiti sample, three factors were extracted: (a) fear of dead people and tombs, (b) fear of lethal disease, and (c) fear of postmortem events.[16] In the present Chinese study, the EFA extracted the same three factors that were extracted from the Kuwaiti study. “Death preoccupation” was not extracted in this study because traditional Chinese beliefs may suppress any kind of death preoccupation. For example, death is a taboo subject that is not to be mentioned or thought about, according to Chinese tradition,[32] and the perception that discussing death can bring bad luck is widespread in Chinese culture.[33] The three factors extracted from this study were similar to the results from the original version, indicating that the ASDA exhibits cross-cultural adaptation and a highly replicable factor structure.[23] Although CFA was not used to confirm the goodness of fit of the other ASDA versions, CFA results in our study demonstrate the data fit the three-factor solution model of the ASDA(C).
4.2 limitations
Although an accessible sample is suitable for exploring the psychometric properties of the death anxiety inventory, the sampling method does have some limitations. The sample is comprised of individuals recruited from universities and hospitals in three geographic areas of China, thus it may not be representative of the Chinese population in general. Previous research showed that age and education influenced the degree of death anxiety.[34] Although the medical staff included doctors, nurses, and workers providing personal care, there was a sample bias in the study. Future research should avoid the sample bias as much as possible. Replications of the present study with a randomized sample would enhance generalizability. Given that death anxiety appears to be a basic fear at the core of a range of mental disorders, including hypochondriasis, panic disorder, anxiety and depressive disorders, further research is warranted to explore the transdiagnostic role of the ASDA(C) in additional clinical and non-clinical populations.
4.3 Importance
Our study demonstrates the adequate reliability and validity of the ASDA(C), which can be a useful tool to assess death anxiety among majority of the Chinese population.
Acknowledgement
We would like to thank all the participants in this study.
Biography

Dr. Qi QIU received a bachelor’s degree from University of South China in 2013 and in the same year began a master’s programin psychiatry and mental health at Shanghai Jiao Tong University Medical College. She is now working as a master’s student at the Department of Geriatrics in the Shanghai Mental Health Center, Shanghai Jiao Tong University Medical College. Her main research interests are cognitive and emotional disorders in the elderly.
Footnotes
Funding/ Support
This work was financially supported by Shanghai Clinical Center for Mental Disorders (2014) and the Medical Guidance Program of Shanghai Science and Technology Committee (No. 15411961400)
Conflict of interest statement
The authors report no competing interests.
Author contributions
QQ performed the statistical analyses and drafted the manuscript. SYZ and XL helped with data analyses and assisted with writing the paper. CXB, HBY, ZWL, JRW, and TW were responsible for data collection and clarification. AMAK provided the English version of the ASDA, supervised the back-translation editing, and edited the manuscript. SFX made substantial contributions to the research and the text. XL formulated and supervised the research and the text. All authors approved the final manuscript.
References
- 1.Furer P, Walker JR. Death anxiety: a cognitive-behavioral approach. J Cog Psychotherapy. 2008; 22(2): 167-182. doi: http://dx.doi.org/10.1891/0889-8391.22.2.167 [Google Scholar]
- 2.Schimel J, Hayes J, Williams T, Jahrig J. Is death really the worm at the core? Converging evidence that worldview threat increases death-thought accessibility. J Pers Soc Psychol. 2007; 92: 789-803. doi: http://dx.doi.org/10.1037/0022-3514.92.5.789 [DOI] [PubMed] [Google Scholar]
- 3.Iverach L, Menzies RG, Menzies RE. Death anxiety and its role in psychopathology: reviewing the status of a transdiagnostic construct. Clin Psychol Rev. 2014; 34(7): 580-593. doi: http://dx.doi.org/10.1016/j.cpr.2014.09.002 [DOI] [PubMed] [Google Scholar]
- 4.Arndt J, Routledge C, Cox CR, Goldenberg JL. The worm at the core: a terror management perspective on the roots of psychological dysfunction. Appl Prev Psychol. 2005; 11(3): 191-213. doi: http://dx.doi.org/10.1016/j.appsy.2005.07.002 [Google Scholar]
- 5.Strachan E, Schimel J, Arndt J, Williams T, Solomon S, Pyszczynski T, et al. Terror mismanagement: evidence that mortality salience exacerbates phobic and compulsive behaviors. Pers Soc Psychol Bull. 2007; 33(8): 1137-1151. doi: http://dx.doi.org/10.1177/0146167207303018 [DOI] [PubMed] [Google Scholar]
- 6.Abdel-Khalek AM, Lester D. Death anxiety as related to somatic symptoms in two cultures. Psychol Rep. 2009; 105(2): 409-410. doi: http://dx.doi.org/10.3389/ fpsyg.2014.01379 [DOI] [PubMed] [Google Scholar]
- 7.Hamang A, Eide GE, Rokne B, Nordin K, Oyen N. General anxiety, depression, and physical health in relation to symptoms of heart-focused anxiety: a cross sectional study among patients living with the risk of serious arrhythmias and sudden cardiac death. Health Qual Life Outcomes. 2011; 9: 100. doi: http://dx.doi.org/10.1186/1477-7525-9-100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stolorow RD. Defensive and arrested developmental aspects of death anxiety, hypochondriasis and depersonalization. Int J Psychoanal. 1979; 60(Pt2): 201-213 [PubMed] [Google Scholar]
- 9.Abdel-Khalek AM. Death anxiety in clinical and non-clinical groups. Death Stud. 2005; 29(3): 251-259. doi: http://dx.doi.org/10.1080/07481180590916371 [DOI] [PubMed] [Google Scholar]
- 10.Barrera I, Spiegel D. Review of psychotherapeutic interventions on depression in cancer patients and their impact on disease progression. Int Rev Psychiatry. 2014; 26(1): 31-43. doi: http://dx.doi.org/10.3109/09540261.2013.864259 [DOI] [PubMed] [Google Scholar]
- 11.Greenberg J. Terror Management Theory: From Genesis to Revelations. Washington, DC, US: American Psychological Association; 2012 [Google Scholar]
- 12.Peal RL, Handal PJ, Gilner FH. A group desensitization procedure for the reduction of death anxiety. OMEGA-J Death Dying. 1982; 12(1): 61-70 [Google Scholar]
- 13.Templer DI. The construction and validation of a Death Anxiety Scale. J Gen Psychol. 1970; 82(2): 165-177. doi: http://dx.doi.org/10.1080/00221309.1970.9920634 [DOI] [PubMed] [Google Scholar]
- 14.Lester D. The factorial structure of the revised Collett-Lester Fear of Death Scale. Death Stud. 2004; 28(8): 795-798. doi: http://dx.doi.org/10.1080/07481180490483472 [DOI] [PubMed] [Google Scholar]
- 15.Tomas-Sabado J, Gomez-Benito J, Limonero JT. The Death Anxiety Inventory: a revision. Psychol Rep. 2005; 97(3): 793-796. [DOI] [PubMed] [Google Scholar]
- 16.Abdel-Khalek AM. The Arabic Scale of Death Anxiety (ASDA): its development, validation, and results in three Arab countries. Death Stud. 2004; 28(5): 435-457. doi: http://dx.doi.org/10.1080/07481180490437572 [DOI] [PubMed] [Google Scholar]
- 17.Wong SH. Does superstition help? A study of the role of superstitions and death beliefs on death anxiety amongst Chinese undergraduates in Hong Kong. Omega (Westport). 2012; 65(1): 55-70. [DOI] [PubMed] [Google Scholar]
- 18.Wu AMS, Tang CSK, Yan ECW. Assessment of death anxiety among Chinese: A study of reliability and validity. Advances in Psychology Research. 2003; 28: 119-128 [Google Scholar]
- 19.Woo J, Lo R, Cheng JO, Wong F, Mak B. Quality of end-of-lifecare for non-cancer patients in a non-acute hospital. J Clin Nurs. 2011; 20(13-14): 1834-1841. doi: http://dx.doi.org/10.1111/j.1365-2702.2010.03673.x [DOI] [PubMed] [Google Scholar]
- 20.Wittkowski J. The construction of the multidimensional orientation toward dying and death inventory (MODDI-F). Death Stud. 2001; 25(6): 479-495. doi: http://dx.doi.org/10.1080/07481180126858 [DOI] [PubMed] [Google Scholar]
- 21.Wittkowski J, Ho SM, Chan WC. The Chinese version of the multidimensional orientation toward dying and death inventory (MODDI-F/chin): an introduction. Omega (Westport). 2011; 64(1): 15-27 [DOI] [PubMed] [Google Scholar]
- 22.Abdel-Khalek AM. Death anxiety in Spain and five Arab countries. Psychol Rep. 2003; 93(2): 527-528 [DOI] [PubMed] [Google Scholar]
- 23.Abdel-Khalek AM, Lester D, Maltby J, Tomas-Sabado J. The Arabic scale of death anxiety: some results from east and west. Omega (Westport). 2009; 59(1): 39-50 [DOI] [PubMed] [Google Scholar]
- 24.Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. 1970; 1(3): 185-216. doi: http://dx.doi.org/10.1177/135910457000100301 [Google Scholar]
- 25.Neimeyer RA, Chapman KM. Self/ideal discrepancy and fear of death: the test of an existential hypothesis. OMEGA: Journal of Death and Dying. 1980; 11(3): 233-240 [Google Scholar]
- 26.Lu YF. [The report of Chinese religious status——According to CFPS(2012) Survey]. Shi Jie Zong Jiao Wen Hua. 2014; 1: 11-25. Chinese [Google Scholar]
- 27.Peters L, Cant R, Payne S, O’Connor M, McDermott F, Hood K, et al. How death anxiety impacts nurses’ caring for patients at the end of life: a review of literature. Open Nurs J. 2013; 7: 14-21. doi: http://dx.doi.org/10.2174/1874434601307010014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Henrie J, Patrick JH. Religiousness, religious doubt, and death anxiety. Int J Aging Hum Dev. 2014; 78(3): 203-227. doi: http://dx.doi.org/10.2190/AG.78.3.a [DOI] [PubMed] [Google Scholar]
- 29.Abdel-Khalek AM, Al-Kandari Y. Death anxiety in Kuwaiti middle-aged personnel. Omega (Westport). 2007; 55(4): 297-310. doi: http://dx.doi.org/10.2190/OM.55.4.d [DOI] [PubMed] [Google Scholar]
- 30.Abdel-Khalek AM, Tomas-Sabado J. Anxiety and death anxiety in Egyptian and Spanish nursing students. Death Stud. 2005; 29(2): 157-169. doi: http://dx.doi.org/10.1080/07481180590906174 [DOI] [PubMed] [Google Scholar]
- 31.Abdel-Khalek AM. Convergent validity of the Templer, Collett-Lester, and Arabic Death Anxiety Scales: rejoinder. Psychol Rep. 2004; 94(3 Pt 2): 1171-1172 [DOI] [PubMed] [Google Scholar]
- 32.Chan K, Lam Z, Chun R, Dai D, Leung A. Chinese patients with terminal cancer. Doyle E, Hanks GWC, MacDonald N. (editors). Oxford Textbook of Palliative Medicine, Second Edition. New York: Oxford; 1998. p. 793-795 [Google Scholar]
- 33.Chan C. Death Awareness and palliative care. In: Psychosocial & Palliative Care. Hong Kong: Hong Kong University Press; 2000. p. 213-232 [Google Scholar]
- 34.Nienaber K, Goedereis E. Death anxiety and education: a comparison among undergraduate and graduate students. Death Stud. 2015; 39(8): 483-490. doi: http://dx.doi.org/10.1080/07481187.2015.1047057 [DOI] [PubMed] [Google Scholar]