

Abstract
A 20-year-old woman presented to our outpatient clinic with a 5-week history of recurrent right lumbar back pain. Contrast-enhanced computed tomography scan showed a Bosniak class IV renal cyst. She was treated with radical nephrectomy. Histopathology revealed xanthogranulomatous pyelonephritis.
Keywords: Bosniak class IV renal cyst, Radical nephrectomy, Xanthogranulomatous pyelonephritis
Xanthogranulomatous pyelonephritis (XGP) is a rare, distinct form of chronic pyelonephritis in which the involved areas of the kidneys are destroyed and replaced by granulomatous tissues containing lipid-laden macrophages.1 It is more commonly seen in middle-aged women, although infants and older men are also affected.2,3 The exact pathogenesis remains unclear, but a number of causes have been proposed, including urinary tract obstruction, recurrent urinary tract infection, altered immune response, lymphatic obstruction, abnormal lipid metabolism, and renal ischemia.4 We describe a case of XGP with radiologic diagnosis of a Bosniak class IV cyst in a 20-year-old woman.
Case History
A 20-year-old woman presented to us with a 5-week history of recurrent right lumbar back pain. Past medical and surgical histories and physical examination findings were unremarkable. Laboratory tests revealed a serum hemoglobin level of 10 mg/dL. Results of serum urea, creatinine, liver function, coagulation profile, and other routine blood tests were normal. Urine culture was sterile.
Ultrasonography showed a 4.2 × 4-cm complex renal cyst arising from the mid part of the right kidney, maintaining the renal contour. Contrast-enhanced computed tomography (CT) scan showed a 4.3 × 4.2-cm complex renal cyst arising from the mid part of the right kidney with evidence of hypodense areas, contrast-enhanced nodules, and septal structures (Bosniak type IV cyst; Figure 1).
Figure 1.
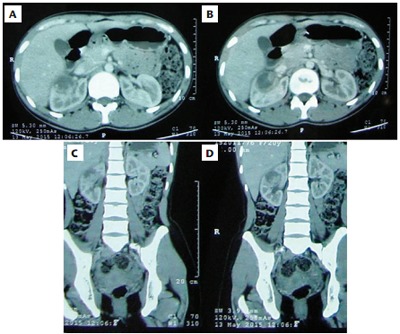
Contrast-enhanced computed tomography scan showing a 4.3 × 4.2-cm complex renal cyst arising from the mid part of right kidney (Bosniak type IV cyst).
Microscopic examination showed evidence of chronic inflammation with a large number of foamy histiocytes suggestive of XGP.
We first attempted a laparoscopic partial nephrectomy, but, due to severe adhesions, this was converted to an open procedure and radical nephrectomy was performed. Histopathologic examination showed macroscopically a cystic mass with areas of necrosis at the middle portion of the kidney (3 × 2.5 × 2 cm); cut surface was greyish-white to greyish-yellow (Figure 2). Microscopic examination showed evidence of chronic inflammation with a large number of foamy histiocytes suggestive of XGP (Figure 3). The patient remained asymptomatic during the next 12 months of follow-up.
Figure 2.

Gross pathology examination showing a cystic mass with areas of necrosis at the middle portion of the kidney (3 × 2.5 × 2 cm); cut surface was greyish white to greyish yellow.
Figure 3.
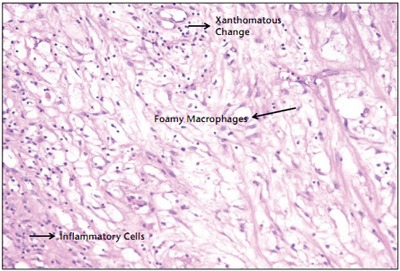
Microscopic examination showing evidence of chronic inflammation with a large number of foamy histiocytes suggestive of xanthogranulomatous pyelonephritis.
Discussion
XGP was first described by Schlagehaufer in 1916, and occurs in 1% of all renal infections.1 Patients usually present with abdominal pain, fever, anorexia, weight loss, hematuria, dysuria, urinary tract infection resistant to antibiotics, or a palpable abdominal mass. The most common offending organisms are Proteus mirabilis and Escherichia coli, although sterile urine is found in approximately one-third of cases.4 Malek and Elder5 have classified it into three stages: Stage I, nephric disease confined to the kidney; Stage II, infiltration into the Gerota fascia; and Stage III, disease extending into adjacent perinephric space and other retroperitoneal structures. It has been described as a great imitator, owing to its varied clinical presentations; it is often misdiagnosed as a renal mass.6,7
Ultrasonography can differentiate between the two forms of XGP…
Ultrasonography can differentiate between the two forms of XGP: diffuse (83%-90%) and focal (10%-17%). In the diffuse form there is diffuse renal enlargement with multiple hypoechoic areas and hyperechoic foci. Hypoechoic areas represent calyceal or pelvicalyceal dilatation and parenchymal destruction; hyperechoic foci with posterior acoustic shadowing represents renal calculi and debris in hydronephrosis. The focal form is usually confined to one part or pole of the kidney.8
CT scan is considered the imaging modality of choice. The characteristic features (not pathognomonic) in diffuse XGP are generalized renal enlargement, perinephric fat stranding, and thickening of the Gerota fascia. A “bear paw sign” is seen in diffuse XGP and refers to the cross-sectional appearance of the kidney, which resembles the paw of a bear. The renal pelvis is contracted whereas the calyces are dilated, mimicking the toe pads of the paw. In focal XGP, the CT scan shows focal mass lesion, occupying one pole or an enhancing lowdensity mass lesion, surrounding dilated, stone-filled calyces.9
CT scan is considered the imaging modality of choice.
The differential diagnosis includes pyonephrosis, malacoplakia, lymphoma, and renal neoplasm. However, sometimes it is very difficult to differentiate these conditions. The most important diagnostic challenge at histology is misinterpretation of “foam cells” as “clear cells.”
The Bosniak renal cyst classification system is used in evaluation of cystic renal masses.10 It is based on contrast-enhanced CT scan findings and permits a cystic mass to be classified into one of five classes (I, II, IIF, III, and IV). Bosniak class IV cysts are considered cystic neoplasms and nephrectomy is indicated in such cases.
Our case is unusual in its presentation: apart from abdominal pain, the patient had no other symptoms suggestive of kidney inflammation. Results of her routine blood tests and urine examination were also noncontributory. All the images indicated a Bosniak class IV complex renal cyst without any evidence of any calculi or hydronephrosis. A diagnosis of cystic renal tumor was not ruled out preoperatively; hence, nephrectomy was done. The diagnosis was only made after the histopathologic analysis of the resected specimen. This kind of presentation of XGP as a Bosniak class IV cyst without calculi in adults is extremely rare in the literature.
Our experience suggests that XGP should be given due consideration in the differential diagnosis of type IV renal cystic diseases. Careful evaluation, including clinical findings, laboratory investigations, and imaging studies, are mandatory for a correct diagnosis and management of this rare clinical disorder. Otherwise, patients will receive inadequate treatment.
Main Points.
Xanthogranulomatous pyelonephritis (XGP) is a rare, distinct form of chronic pyelonephritis in which the involved areas of the kidneys are destroyed and replaced by granulomatous tissues containing lipid-laden macrophages.
Computed tomography scan is considered the imaging modality of choice. The characteristic features (not pathognomonic) in diffuse XGP are generalized renal enlargement, perinephric fat stranding, and thickening of the Gerota fascia.
The differential diagnosis includes pyonephrosis, malacoplakia, lymphoma, and renal neoplasm.
XGP should be given due consideration in the differential diagnosis of type IV renal cystic diseases. Careful evaluation, including clinical findings, laboratory investigations, and imaging studies are mandatory for a correct diagnosis and management.
Informed consent from the patient was received with regard to the publication of her case and all related photographs, according to the guidelines of the institutional ethics committee.
References
- 1.Parsons MA, Harris SC, Longstaff AJ, et al. Xanthogranulomatous pyelonephritis: a pathological, clinical and aetiological analysis of 87 cases. Diagn Histopathol. 1983;6:203–219. [PubMed] [Google Scholar]
- 2.Matthews GJ, McLorie GA, Churchill BA, et al. Xanthogranulomatous pyelonephritis in pedriatric patients. J Urol. 1995;153:1958–1959. [PubMed] [Google Scholar]
- 3.Lee HN, Kim KH, Ryu IW, et al. Xanthogranulomatous pyelonephritis in an infant. Korean J Urol. 2006;47:1367–1370. [Google Scholar]
- 4.Chuang CK, Lai MK, Chang PL, et al. Xanthogranulomatous pyelonephritis: experience in 36 cases. J Urol. 1992;147:333–336. doi: 10.1016/s0022-5347(17)37229-4. [DOI] [PubMed] [Google Scholar]
- 5.Malek RS, Elder JS. Xanthogranulomatous pyelonephritis: a critical analysis of 26 cases and review of the literature. J Urol. 1978;119:589–593. doi: 10.1016/s0022-5347(17)57559-x. [DOI] [PubMed] [Google Scholar]
- 6.Arrighi N, Antonelli A, Zani D, et al. Renal mass with caval thrombus as atypical presentation of xantogranulomatous pyelonephritis. A case report and literature review. Urologia. 2013;80(suppl 22):44–47. doi: 10.5301/ru.2013.11050. [DOI] [PubMed] [Google Scholar]
- 7.Zorzos I, Moutzouris V, Petraki C, Katsou G. Xanthogranulomatous pyelonephritis–the “great imitator” justifies its name. Scand J Urol Nephrol. 2002;36:74–76. doi: 10.1080/003655902317259418. [DOI] [PubMed] [Google Scholar]
- 8.Kim J. Ultrasonographic features of focal xanthogranulomatous pyelonephritis. J Ultrasound Med. 2004;23:409–416. doi: 10.7863/jum.2004.23.3.409. [DOI] [PubMed] [Google Scholar]
- 9.Goldman SM, Hartan DS, Fisman EK, et al. CT of xanthogranulomatous pyelonephritis: radiologicpathologic correlation. Am J Roentgenol. 1984;142:963–969. doi: 10.2214/ajr.142.5.963. [DOI] [PubMed] [Google Scholar]
- 10.Bosniak MA. The current radiological approach to renal cysts. Radiology. 1986;158:1–10. doi: 10.1148/radiology.158.1.3510019. [DOI] [PubMed] [Google Scholar]