

Abstract
Background
Rates of musculoskeletal disorders in construction remain high. Few studies have described barriers and facilitators to the use of available ergonomic solutions. This paper describes these barriers and facilitators and their relationship to the level of adoption.
Methods
Three analysts rated 16 proposed ergonomic solutions from a participatory ergonomics study and assessed the level of adoption, six adoption characteristics, and identified the category of adoption from a theoretical model.
Results
Twelve solutions were always or intermittently used and were rated positively for characteristics of relative advantage, compatibility with existing work processes, and trialability. Locus of control (worker vs. contractor) was not related to adoption. Simple solutions faced fewer barriers to adoption than those rated as complex.
Conclusions
Specific adoption characteristics can help predict the use of new ergonomic solutions in construction. Adoption of complex solutions must involve multiple stakeholders, more time, and shifts in culture or work systems.
Keywords: intervention, transfer technology, implementation and dissemination, injury prevention, musculoskeletal disorder
Introduction
Rates of musculoskeletal disorders (MSD) in construction are responsible for high rates of both workers’ compensation claims and personal health claims (CPWR – The Center for Construction Research and Training, 2013, Dale, et al., 2015, Lipscomb, et al., 2015a, Lipscomb, et al., 2015b) and implementation of sustainable ergonomic solutions to prevent MSD in construction work is a challenge (Hecker, et al., 2001, Hess, et al., 2004, Kramer, et al., 2010, Rinder, et al., 2008, Schneider, 1995, Weinstein, et al., 2007). An ergonomic solution is defined as an available new device or technology that can be used to reduce musculoskeletal disorder (MSD) risk factors in construction related tasks, and may include equipment, positioners, hand tools, power tools, manual material handling devices (MMH), and personal protective equipment (PPE) (Bernard, 1997, Dale, et al., 2016b). Information on available ergonomic solutions for construction applications has grown dramatically over the past ten years through online resources promoted by CPWR (2016) and publications by NIOSH (2007, 2013). However, the adoption process of solutions by individuals and organizations has been slow (Dale, et al., 2016b, Kramer, et al., 2010, Welch, et al., 2015).
The diffusion of innovations (Rogers, 1995) theoretical framework has been used to describe the adoption continuum for ergonomic solutions in construction (Kramer, et al., 2010, Weinstein, et al., 2007). A construction ergonomics intervention matrix was developed as a tentative model for conceptualizing the application of ergonomic solutions in construction (Kramer, et al., 2010, Weinstein, et al., 2007). There are four categories for Weinstein’s Solution Matrix based on the complexity of the solution (simple or complex) and the time necessary to implement (short-term or long-term) (see Figure 1). Adoption of interventions depends upon the commitment of the organization to initiate the intervention and of the workers to implement its use (Welch, et al., 2015). There is little known about the barriers to dissemination of interventions into construction projects. This study was undertaken to examine the use of ergonomic solutions by individuals, describe the facilitators or barriers related to use of these solutions, and to show the relationship between characteristics of diffusion of solutions to the extent of adoption. We further compared the category of adoption from Weinstein’s Solution Matrix to level of adoption observed in the study.
Figure 1.
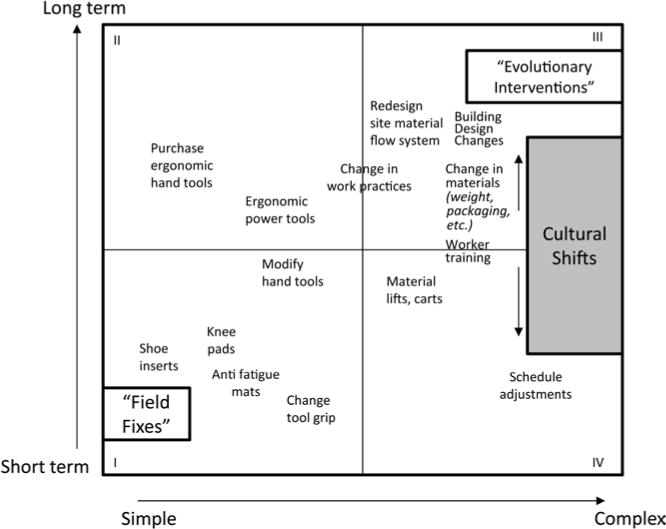
Construction ergonomic-Solution Matrix
Materials and Methods
A previous participatory ergonomics (PE) study among construction workers from three trades set the foundation for our current study. In brief, we conducted a PE study among construction workers from three trades: floor laying, carpentry, and sheet metal (Dale, et al., 2016a, Jaegers, et al., 2014) and seven contractors, following each project for approximately six months. We provided training to enable workers to identify ergonomic risks in work tasks such as high force, awkward postures, repetition, contact stress, and vibration, and to identify ergonomic solutions such as tools, equipment, scheduling, and work practices. Examples of worker identified problems and related solutions are displayed in Table I.
Table I.
Examples of worker identified injury risk tasks and related solutions from a participatory ergonomics study
| Trade/Job | Photo Descriptions | Injury Risk Task | Identified Solutions |
|---|---|---|---|
| Floor Layer / Remodel carpet flooring. | 1a. Manually tearing out carpet with high grip pulling forces. 1b. Operating an electric carpet puller, reducing manual gripping and pulling. |
1a.
|
1b.
|
| Sheet Metal / Duct installation. | 2a. Manually crimp small duct parts using high grip force. 2b. Operate a power crimper attachment on powered drill using low grip force. |
2a.
|
2b.
|
| Floor Layer/ Spread adhesive | 3a. Spread adhesive with hand trowel in prolonged kneeling. 3b. Spread adhesive with stand-up trowel. |
3a.
|
3b.
|
| Sheet Metal/ Cutting metal duct | 4a. Manual hand snips using repetitive, forceful grip. 4b. Cutter attachment on a powered drill using low grip force. |
4a.
|
4b.
|
Methods for Analyzing Barriers and Facilitators
We first reviewed all solutions identified in the PE study; one analyst extracted a list of potential ergonomic solutions (n=28) identified by workers, contractors, and industry professionals, and researchers during the study period. An analyst then compiled all available descriptive data for each selected solution including a photograph of the device, if applicable, a description of the problem work task, and descriptions of the context surrounding the trial to use the solution. Many of the solutions had been examined during the trial use in the field, and may have included worker recorded usability ratings (effort, speed, quality, productivity) during trials with the usual method and with the new solution. Our team of 3 analysts (an occupational medicine physician and two occupational therapists) then reviewed the available data for each of the 28 solutions and selected a sample of 16 solutions that had sufficient descriptive data to allow characterization using Weinstein’s criteria.
Next, the analysts independently rated characteristics of those solutions that were hypothesized to facilitate or impede their use according to the characteristics for adoption and rating definitions (Table II) modified from Weinstein (2007) and Rogers (2003). The analysts rated the five characteristics described by Weinstein (Relative advantage, Compatibility, Complexity, Trialability and Observability) as well as a rating of Usability in order to assess workers use of the ergonomic solution. Although usability is implied in several other characteristics (compatibility and observability), it was important to obtain a measure of use for the specific purpose of this study. Ratings were based on data from focus groups (n=6), survey results from all workers (n=86), field notes from researcher observations, and interviews with contractors and industry representatives. Analysts examined all data for each solution then rated the solution based on the characteristics in Table II. Each analyst independently assigned ratings to each quality as positive (+) or negative (−) as it applied to the use of the ergonomic device or innovation. Analysts noted whether each characteristic was a facilitator or barrier for each solution and provided explanations and examples to justify the assignment. The analysts compared independent ratings and discussed differences to reach a group consensus. The consensus ratings described each characteristic for each solution as a facilitator (+), barrier (−) or mixed (+/−).
Table II.
Rating Definitions and Adapted Criteria for Describing the Facilitators and Barriers to Adoption of Ergonomic Solutions
| Rating | Definitions |
|---|---|
| Primary Control | The person, group or organization with the main power to implement a solution (e.g. worker, contractor, both or other). |
| Adoption | Uptake of an innovation by the target audience based its presence and use in a worksite. |
| Facilitator (+) | Criteria: assists with or facilitates implementation of the solution. |
| Barrier (−) | Criteria: prevents, limits, restrains, or acts as barriers to implementation of the solution. Inhibits the adoption of the innovation. |
|
| |
| Criteria | Definitions |
|
| |
| Relative Advantage | The ability to project a relative advantage in the quality of the work with using the tool or equipment, productivity, quality effects, initial costs, durability or maintenance costs, and injury prevention. Based on the components of return on investment (ROI). |
| Usability | The extent to which a device is user-friendly, intuitive to use, quick to learn or master operation (trainability), easy to use, convenient, and useful. |
| Compatibility | The extent to which the innovation is compatible with the norms and practices of the subsystem. |
| Complexity | The extent to which the innovation is easy or difficult to introduce and use on a worksite and the extent to which it requires reorganization of the work process. |
| Trialability | The ability of an individual or organization to experiment with an innovation prior its adoption. |
| Observability | Refers to the transparency of the impact of a given innovation or device as compared to the regular method and provides a readily observable advantage. |
In addition to these six characteristics, each solution was assigned a locus of control for the implementation of the solution; the team reached consensus on whether the worker or contractor was responsible for acquiring each solution to make it available for implementation. For instance, work technique is typically in the worker’s control while implementation of motorized manual material handling (MMH) equipment is in the contractor’s control. The responsibility for providing devices on these union projects is primarily based on the labor-management agreement for the trade. Contractors are primarily responsible for large equipment, power hand tools, and specialty task-specific devices. Workers are responsible for providing manual tools and personal protective equipment (PPE). The 16 ergonomic solutions were also categorized according to type of tool: equipment, positioners, power tools, hand tools, MMH devices, PPE, and design for safety technology (shown in Table III). Finally, each solution was assigned to one of the four categories in the solution matrix shown in Figure 1.
Table III.
Description of Identified Ergonomic Solutions
| Ergonomic Solutions | Description |
|---|---|
| Equipment | |
| Overhead drill press | Inverted drill press device to drill overhead. |
| Ride-on scraper | Motorized ride-on device for flooring removal. |
| Electric carpet puller | Clamp and winch machine for tearing out carpet. |
| Positioners | |
| Positioners for work tasks | Surfaces such as carts, bakers scaffold, saw horses, or extra materials. |
| Rolling chest support | Supportive chest pad mounted on a rolling stool with knee padding, |
| Power Tools | |
| Power crimper | An attachment for cordless drill to crimp metal duct. |
| Power shears / snips | Attachment for cordless drill to cut sheet metal. |
| Hand Tools | |
| Pry bar – extended | Pry bar for jacking up office cubicle furniture. |
| Stand up trowel | Trowel attached to a pole for spreading adhesives while standing. |
| Grout sponge roller basin | Grout sponge rinsing system in specialized bucket. |
| Carpet puller – manual | Serrated clamp with large handle to improve grip when pulling carpet. |
| Manual Material Handling | |
| Various rolling carts | Rolling carts used for transporting loads. |
| Personal Protective Equipment | |
| Vibration dampening gloves | Glove for dampening vibration or impact to the hand from tools. |
| Custom fit knee & shin pads | Knee padding device to protect the knee and shin while kneeling. |
| Knee pad with body support | Knee padding device and body support for kneeling and sitting. |
| Design for Safety Technology | |
| 3D Laser Scanning | Locates ceiling drilling points to improve accuracy and reduce ladder use. |
Dependent variable
Using the same data sources, we determined the extent to which each solution was adopted based on the frequency the solution was used by work groups within tasks relevant to the solution during the PE study. In order for us to rate adoption, the innovation 1) must have been known by the person, work group, or trade on the project, 2) there must have been a need for the innovation within the worker’s tasks (since workers will not trial an innovation without a real world need), and 3) workers had the device or innovation available to try. If any of these three conditions were unknown, we were unable to assess adoption, so the solution was excluded from the analysis.
The two researchers who conducted the PE program (AMD and LJ) independently assigned adoption ratings without referring to the characteristic for adoption. Adoption ratings were “always” used, “intermittently” used, “rarely” used, “not used” during the study, or the use could not be determined (“unknown”). Disagreements in ratings were discussed to reach consensus.
Our original participatory study protocol was reviewed and approved by the Institutional Review Boards of Washington University and Saint Louis University. All subjects provided informed consent to participate in this study.
Analysis
We examined whether or not there was an association between each category of independent predictors and the level of use of the 16 identified solutions. The relationship between ratings of each adoption characteristic and the extent of adoption was quantified using chi square tests. Similar tests of association were conducted between the 4 categories of the solution matrix and extent of adoption, and between locus of control and extent of adoption. To assess the extent to which multiple characteristics improved the prediction of adoption, we computed the total number of facilitators and number of barriers from the six adoption characteristics, and used Poisson regression analysis to test the association between adoption (always or intermittently) and the number of facilitators in one model. We repeated the analysis to test the relationship between adoption and the number of barriers.
Results
Table IV provides narrative descriptions recorded by the analysts during the rating sessions and used to rate each criteria as a facilitator or barrier to adoption. There were many more facilitators described in support of solutions that were always and intermittently adopted and more barriers listed for solutions that were not adopted. Many barriers and facilitators are quite specific to the tool. Table V displays characteristics for the 16 solutions including locus of control, adoption ratings, solution matrix category, rating for adoption characteristics, and the number of facilitators and barriers for each characteristic. Table VI presents a sum of the frequency of positive, negative or mixed ratings for each characteristic for adoption, comparing the group of solutions adopted always or intermittently to solutions adopted rarely or never.
Table IV.
Facilitators and barriers for each innovation
| Ergonomic Solutions | Facilitators | Barriers |
|---|---|---|
| Power crimper | Low cost, faster, less effort to crimp metal than manual method; overall positive (offset of cost); contractor will purchase when job needs it; worker sees benefit, increased return on investment, quality of crimp, | Infrequent task for some contractors, need for crimper may be low; requires additional and separate designated drill, more to carry onto the worksite |
| Pry bar – extended | Less ratcheting of jacks, improved productivity; less complex than ratchets/jacks; cheap, fast; “no brains” required; better leverage, load of 140# not significant so effort required to use device is low, but does not replace load or effort of the task; not difficult; low cost, easy to transport, easy fit in area; less ratcheting, increased productivity; workers adopted it even though it was a concrete tool; workers paid for this to trial even though it was $90; easy to see the advantage | Potential safety risk, load shifts when no force holding it |
| Grout sponge roller basin | Faster, affordable, user friendly, simple design; Increased production; reduces frequency of hand squeezing; spread by word of mouth; no extra steps; workers lending to others for trial; easy to see impact, decreased repetition. | Purchase before trialing, more equipment to clean; not available for trial unless you know someone |
| Electric carpet puller | Easy to use, accepted among floor layers; more efficient, fewer man-hours more than offsets the cost; quality, they are buying them; device available to trial by two companies in the study | Not used for small jobs, slow speed; transport, room size |
| Carpet puller – manual | Easy to use and see advantage, accepted among workers; accommodation of simple tools leads to complexity – carrying, bringing, owning, etc.; benefit outweighs barriers having to carry it to have available; low cost, simple to use; comfort, durability; accepted norm; does not require reorganization [of tasks]; must be available when needed – may be carried in a bucket with other equipment used to demo carpet; easy to see | Extra tool to carry; only replaces a portion of the carpet demo task |
| Positioners for work tasks | Dual purposes, low cost; using available equipment at site or very inexpensive to trial | Availability, transport, and placement may affect work flow; depends upon how well the positioner interfaces at the task, how long to adjust |
| Overhead drill press | Improved quality of holes, cleaner air, faster process; able to roll it in and use; easy to procure; high observability to early adopter; less dust; less fatigue, less force, [better] posture; housekeeping; Return On Investment good in some circumstances; better productivity in some settings; so easy even apprentice can use it, trainability | Can’t use if ceilings are too high; sheet metal trade school and union members did not easily observe the benefits of this device; wheels too big, [limited use to only] large jobs, have to transport [to worksite], lock up [concern for theft] |
| Various rolling carts | Easier to transport loads, able to move more at one time, accepted in the workplace, widely available, easy to see the benefits, culturally accepted; able to carry more at one time, cost; accepted; not significant cost, generally owned by contractor; good for long periods of packing heavy items or few workers; available to assist, carts are beneficial | May slow work down, malfunctioning wheels (need maintenance); often specific to task; may not be readily available; need to plan to have at site, need maintenance |
| Power shears / snips | Low cost, faster, less effort to cut metal than manual method; no hot metal [from other methods]; no cord; overall positive, but there are some limitations; contractor would purchase for roof work. Worker would purchase on his own; easy to learn; see other below; no change in work process; faster to work with much less effort; improve safety, less cords; simple, may decrease need for tools, only use one tool | Workforce norms, difficult to use overhead; may be perceived as too different from the way work has always been done for tinners, but does not introduce different work process; snips do just as good of a job; heavy and awkward to use overhead (2-part tool, must hold both); have to charge batteries, heavy and durability [unknown] |
| Custom fit knee and shin pads | Easy to see the benefits for knee comfort; simple to use; decreased fatigue, comfort; accepted, only because most guys wear them all of the time | Unable to trial before purchase. Initial cost to worker; not useful on slippery surface unless the worker adds friction tape, raises worker further from the floor so may cause increased low back flexion [poor posture]; some behavior change limitations to use them all the time; cost to worker limits trials |
| Ride-on scraper | Increased productivity, able to rent / trial; savings on labor cost; faster job; training from supplier, cost of large curve; easy to see benefit | Initial cost if purchasing, cost for learning curve; transport, side prep; maintenance cost for breakdown. |
| Vibration dampening gloves | Easy to see the advantages for protecting the hand from impact and vibration; good, provided that gloves are flexible/good fit | Gloves must be chosen correctly for the task; bulkiness, temperature, finger dexterity are potential barriers to the task; changing gloves, hot, bulky, interfere with some tasks; remove glove for some series of steps, have gloves onsite when needed |
| Knee pad with body support (K2S) | Easy to see benefits for knee comfort and supporting body weight; decreased body weight on legs, decreased fatigue; less stress on knees, workers open to it; no reorganization [in work tasks]; makes sense; provide upper body support; easy to see impact of use; readily available online; simple; | Unable to trial before purchase. Initial cost to worker; more a barrier than other knee pads, ; limited use with intermittent kneeling task; easy to use when on floor, but difficult to walk in, can’t use for all tasks; [perceived as] sitting down on the job; requires using more than 1 type of knee pad for kneeling task; unable to rent or trial before purchase; prolonged kneel [posture during use]; strap on [to don] |
| 3D Laser Scanning | Newer technology, reduces kneeling and ladder climbing; worker useful skill, decreased floor work, “way of the future” may help them get [bid] larger jobs better work flow in theory | Costly, uncertain return on investment, large learning curve for IT team/GC team, different from low tech/current process, requires large changes in work processes; planning, coordinating with GC, IT team; all in or nothing |
| Stand up trowel | Easy to see benefits of standing versus working on hands and knees; improved postures; workers open to trialing it; might be faster and more comfortable; work faster and larger in an upright position; workers feel it will benefit their body; probably 1 day learning curve; no big change; just replaces the hand trowel; cleaning similar; easy to see advantage | Not widely available for purchase. Unable to spread all types of adhesives; may not be accepted due to workforce norms; difficult to control glue and use device for good quality; need time to train with it, one session not enough; may be barrier to floor laying culture, workers are used to using a hand trowel; not typical way to do the work; not useful for many work conditions; they want it to work, but found it was difficult; now need 2 devices instead of one (need to cut in with hand trowel) |
| Rolling chest support | Easy to see the benefits; easy to use; no training needed; outweighs barrier; better for low back; maybe great for some jobs; chest support to decrease fatigue | How to carry other equipment supplies [while using the device]; only usable for certain tasks. may not be accepted due to workforce norms; not available so must purchase to trial; need open floor; limited utility; others perceive you aren’t doing the job right, increased cost, must transport to site; sitting down on job; might object work organization; how to move equipment and cost |
Table V.
Ergonomic Solutions Ratings
| Ergonomic Solutions (N=16) | Locus of Control | Adoption | Solution matrix group | Criterion for Adoption
|
Total facilitator count | Total barrier count | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Relative Advantage* | Usability | Compatibility* | Complexity | Trialability* | Observability** | ||||||
| Always Adopted (n=2) | |||||||||||
| Power crimper | C | A | II | + | 6 | 0 | + | + | + | 6 | 0 |
| Pry bar – extended | W | A | II | + | 6 | 0 | + | + | + | 6 | 0 |
| Intermittently Adopted (n=10) | |||||||||||
| Grout sponge roller basin | W | I | II | + | 0 | 0 | + | + | + | 6 | 0 |
| Electric carpet puller | C | I | II | + | 6 | 0 | + | + | + | 6 | 0 |
| Carpet puller – manual | W | I | II | + | 6 | 0 | + | + | + | 6 | 0 |
| Positioners for work tasks | W | I | I/II | + | 6 | 2 | + / − | + | + | 6 | 2 |
| Overhead drill press | C | I | II | + / − | 6 | 2 | + | + | + | 6 | 2 |
| Various rolling carts | C | I | IV | + / − | 6 | 3 | + / − | + | + | 6 | 3 |
| Power shears / snips | C | I | II | + | 5 | 1 | + | + | + | 5 | 1 |
| Custom fit knee & shin pads | W | I | I | + | 5 | 1 | + | − | + | 5 | 1 |
| Ride-on scraper | C | I | II | + | 4 | 2 | − | + | + | 4 | 2 |
| Vibration dampening gloves | W | I | I | + | 4 | 2 | − | + | + | 4 | 2 |
| Rarely Adopted (n=2) | |||||||||||
| Knee pad with body support | W | R | II | + / − | 4 | 3 | + | − | + | 4 | 3 |
| 3D Laser Scanning | C | R | III | + / − | 3 | 5 | − | − | + | 3 | 5 |
| Not Adopted (n=2) | |||||||||||
| Stand up trowel | W | N | II | + / − | 4 | 4 | + | − | + | 4 | 4 |
| Rolling chest support | W | N | II | − | 2 | 4 | − | − | + | 2 | 4 |
+ = Facilitators, − = Barriers, W=Worker, C=Contractor, A=Always used, I=Intermittently used, R=Rarely used, N=Not used
chi-square test, p<0.05,
no test of association
Table VI.
Frequency of Adoption Criteria Ratings for Ergonomic Solutions (N=16)
| Solution Adopted Always or Intermittently (n=12) |
Solution Adopted Rarely or Never (n=4) |
|||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Facilitator | Barrier | Mixed | Total | Facilitator | Barrier | Mixed | Total | |
| Relative Advantage | 10 | – | 2 | 12 | – | 1 | 3 | 4 |
| Usability | 7 | 2 | 3 | 12 | 1 | 2 | 1 | 4 |
| Compatibility | 11 | 1 | – | 12 | 1 | 2 | 1 | 4 |
| Complexity | 8 | 2 | 2 | 12 | 2 | 2 | – | 4 |
| Trialability | 11 | 1 | – | 12 | – | 4 | – | 4 |
| Observability | 12 | – | – | 12 | 4 | – | – | 4 |
|
| ||||||||
| Total | 59 (82%) | 6 (8%) | 7 (10%) | 72 | 8 (33%) | 11 (46%) | 5 (21%) | 24 |
Of the 16, two of the solutions were always adopted, more than half (n=10) were adopted intermittently, two were rarely adopted, and two were not adopted during the duration of the PE study. All 16 innovations received facilitator ratings for observability, suggesting observability may be a necessary characteristic, but not sufficient.
The power crimper, extended prybar, grout sponge roller basin, electric carpet puller and manual carpet puller showed positive ratings for all of the characteristics; the first two of these solutions were always adopted and the other three solutions were intermittently adopted. Two devices, stand-up trowel and rolling chest support, were not adopted and showed barriers for trialability and compatibility, suggesting these may be necessary characteristics for adoption.
Poisson regression analysis results showed the non-adopted solutions are expected to have more than three times more barriers among the six adoption characteristics than adopted solutions (Anti-log of coefficient: 3.67, Wald chi square 12.24, p<0.001). On the other hand, adopted solutions were expected to have nearly two times more facilitators than non-adopted solutions, although the association was not significant (Anti-log of coefficient: 1.7, Wald chi square 3.01, p=0.08). These results show that assessing more than one characteristic improves the prediction of adoption.
For the solutions that were always or intermittently adopted, 82% of the ratings were positive facilitators to adoption, 10% were mixed, and 8% were negative barriers to adoption. Among rarely or not adopted solutions, 33% of ratings were positive/facilitators to adoption, 21% were mixed and 46% were negative/barriers to adoption.
Almost half of the solutions identified in this study were under the primary control of the contractor (7/16) and nearly all of these solutions were intermittently or fully adopted. However, there was no statistical association between adopted solutions and locus of primary control of the solutions.
There are four categories for Weinstein’s Solution Matrix based on the complexity of the solution (simple or complex) and the time necessary to implement (short-term or long-term) (see Figure 1). Most of the solutions fell in Category II (simple, long-term time for adoption), two in Category I (simple, short-term time for adoption) and one crossed Categories I and II. All worker-controlled solutions (n=9) were assigned the “simple” categories. The two solutions in the complex categories (III and IV) were under the contractors’ control. However, most of the solutions (n=13) were in the long-term time for adoption categories (II or III) of the solution matrix. There was no association between location on the solution matrix and adoption.
Discussion
We found, among a small sample of ergonomic solutions, that the six adoption characteristics based on those proposed by Weinstein are associated with the likelihood of adoption. However, even if all characteristics were uniformly positive, some solutions were only intermittently adopted, suggesting that these six characteristics alone do not fully capture the characteristics that make an ergonomic solution take hold. A solution with a positive relative advantage and compatibility with current norms and practices was more likely to be adopted. Having the ability to trial the solution also increased the likelihood of adoption. Multiple barriers among the characteristic decreased the likelihood of adoption.
In 2007, Weinstein proposed a theoretical framework which could be used to predict diffusion of ergonomic solutions in the construction industry. His theory has been evaluated once (Kramer, et al., 2010) and we extend that evaluation. Kramer and colleagues (2010) used a similar approach to assessing adoption of solutions in construction, collecting data through interviews with 15 employers and questionnaires from 54 workers. Similar to results in the current study, Kramer concluded that relative advantage and usability were the most important characteristics for adoption, and solutions had to have multiple positive attributes to be adopted. As expected, there were many fewer barriers for the solutions that were adopted; of the solutions with low adoption, there were many more barriers and somewhat weaker facilitators. The barriers for each solution were often particular to the task and therefore to the trade.
Comments from workers and contractors tell us that in the two cases of full adoption, the ergonomic solution was a “no brainer,” worked dramatically better than other options for the task, was applicable to most situations of the task, and only one trial would convince the user to adopt it. The power crimper was introduced at a worksite by the research team and workers immediately preferred it over manually hand crimping small, round metal duct. In contrast, other solutions received positive facilitator ratings for all adoption characteristics and yet were not fully adopted. For example, the electric carpet puller was described as easy to use, was accepted among floor layers, was more efficient and the fewer man-hours more than offset the cost, and it improved quality. However, workers described that it could not be used for small jobs, and it was difficult to transport. It was often the case that solutions that were intermittently adopted did not work for all types of applications; this was the case for the overhead drill press, ride on scraper, electric carpet puller, positioners, power shears, and carts. If these devices could be further developed to be more universally applicable, we anticipate their more frequent adoption as a practical alternative to the current tools and equipment.
Trialability was an important characteristic for adoption success. Tools that were owned by coworkers, easily purchased at local stores for a reasonable price, or obtainable through local suppliers were available to trial during the relevant tasks for using the tool. Some tools such as the power crimper and power shears were readily adopted by the workers after they were made available to trial by the research team. Dissemination for adoption of these useful tools and devices that reduce physical exposures must include the means for workers to gain access to tools for trialing.
The solutions for this study were identified within a participatory ergonomics program of subcontractor work groups consisting of workers and one contractor representative. By contractual agreement with the unions, contractors must provide all equipment for the project and workers provide the hand tools. There were a similar number of solutions within the responsibility of the contractor and the worker; we observed no difference in adoption based on the locus of control. Most of the solutions were considered “simple” in Weinstein’s solution matrix and these were more readily made available and used by workers, showing positive, consistent adoption during the project. Simple solutions such as the extended pry bar and manual carpet puller, involve fewer actors and require less impact on the organizational system in order to be adopted. The majority of the solutions identified within our study were simple solutions, but not all workers were familiar with the suggested devices.
Complex solutions may require a shift in culture, particularly if the new tool or work process does not fit within the norm and requires a large shift in the work processes of the system. In the current study, there were two solutions in Weinstein’s “complex” categories (III and IV) with adoption scores of intermittent and rare. Both of these solutions (rolling carts and 3D laser scanner) were within the contractor control and required a large number of resources and preplanning to incorporate them into the system. These complex solutions involve multiple actors (workers, managers, multiple contractors, suppliers, designers) (Boatman, et al., 2015) and a concerted effort to monitor the integration of the new work process into the daily activities of the project. Adoption of complex solutions requires time and knowledge about the solution, and a positive working relationship between the contractor and workers. Complex solutions that require changing the system involve both organization as well as individual change (Greenhalgh, et al., 2004). The characteristics in the solution matrix do not account for all issues in the process of adoption, particularly for complex solutions.
Our sample of solutions would be best described as a convenience sample. These were solutions known to the investigators, workers, or contractors and which had probably already passed some basic screen for usability and compatibility (commonly referred to as the “laugh test”) before being offered to the group. This would mean that some of the characteristics had already been applied, and that if we had tested a wider range of solutions we would have found more that were not adopted. Furthermore, we did not assess the capacity for use of the solutions within the work tasks, although the analysts considered the opportunity for use in assigning the rating for adoption. Our solutions were focused on a subset of trades and projects and were limited to the solutions that were available at the time of the study, the stage of the building process, and the context and environment in which the builds occurred. To minimize rater bias, we selected solutions with data from multiple sources (worker focus groups and surveys, contractor interviews, and researcher observations and manufacturers information) and had three analysts independently rate characteristics as facilitators and barriers before consensus discussions. The group of analysts selected the sample of solutions with adequate information to complete ratings of the characteristics and this may have biased our sample of solutions toward selecting those that were more likely to be adopted. The information available for the study and period of time for monitoring the adoption of solutions may have been inadequate to know if the solution was fully adopted; our data address short-term utilization of solutions rather than long-term adoption. Facilitators and barriers to solutions likely vary for each solution if the solution is applied in different build situations and applications.
Conclusion
This study used detailed, qualitative information (from worker and researcher) to determine factors related to the adoption of a number of ergonomic solutions during construction projects. The criteria described by Weinstein (2007) were important characteristics to assess adoption of a tool but they do not fully assess the process of adoption; we know that change to improve ergonomics in the construction industry needs more than a few new good tools. The criteria also offers a means to assess the characteristics during ergonomic tool development, to incorporate simpler designs (complexity), that are compatible with work practices, easier to test on a trial basis (Trialability), cost effective (Relative Advantage), and observed as beneficial to the users. While our results support the use of the Solution Matrix for determining the likelihood of adoption for solutions labeled simple compared to those in the complex categories, additional factors must be addressed to support the adoption of complex solutions. The The successful introduction of new tools or technology relies on the involvement of stakeholders and a simultaneous understanding of the construction culture, and need a long-term commitment from all parties (Baker, et al., 2015, Welch, et al., 2015). To understand change in the industry we need good metrics, such as the Weinstein criteria for adoption, process measurement, stakeholder engagement, and patience.
Acknowledgments
We would like to thank the St. Louis-Kansas City Carpenters Regional Council, Sheet Metal Workers’ Local 36 and the contractors, carpenters, and sheet metal workers, who participated in this study. The authors would like to thank Anna Kinghorn for her assistance in preparing the manuscript and Skye Buckner-Petty on his statistical assistance.
Funding: Grant sponsor: National Institute for Occupational Safety and Health/Centers for Disease Control to CPWR— the Center for Construction Research and Training; Grant number: NIOSH U60 OH009762. Its contents are solely the responsibility of the authors; the study sponsors had no specific involvement in this manuscript; and the findings do not necessarily represent the official views of CDC/NIOSH.
Footnotes
Authors’ contributions: All coauthors participated in this study. Drs. Dale, Jaegers, and Evanoff planned and conducted the research; Drs. Dale, Jaegers, Welch, and Evanoff were involved in interpretation of the data analysis. Drs. Dale, Jaegers, and Welch were the primary writers, with all other authors contributing to and editing portions of the manuscript. All authors reviewed the final manuscript. All authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Institution at which the work was performed: Washington University School of Medicine, St. Louis, MO.
Institution and Ethics approval and informed consent: The Washington University and St. Louis University’s Institutional Review Boards provided the ethical approval of this study. All participants provided written informed consent and were compensated for their participation.
Disclosure (Authors): The authors declare that they have no conflicts of interest relevant to the publication of this manuscript; Drs. Dale, Jaegers, Welch, and Evanoff report a grant from CDC/NIOSH during the conduct of the study.
Disclaimer: None
References
- Albers JT, Estill CF. Simple solutions: Ergonomics for construction workers. Cincinatti, OH: 2007. (DHHS (NIOSH) Publication No. 2007–122). [Google Scholar]
- Baker R, Chang CY, Bunting J, Betit E. Triage for action: Systematic assessment and dissemination of construction health and safety research. Am J Ind Med. 2015;58:838–848. doi: 10.1002/ajim.22477. [DOI] [PubMed] [Google Scholar]
- Bernard BP. Musculoskeletal disorders and workplace factors: A critical review of epidemiologic evidence for work-related musculoskeletal disorders of the neck, upper extremity, and low back. Cincinnati, OH: National Institute for Occupational Safety and Health (NIOSH); 1997. (dhhs (niosh) publication no. 97-141). [Google Scholar]
- Boatman L, Chapman D, Teran S, Welch L. Creating a climate for ergonomic changes in the construction industry. Am J Ind Med. 2015;58:858–869. doi: 10.1002/ajim.22499. [DOI] [PubMed] [Google Scholar]
- CPWR – The Center for Construction Research and Training. The construction chart book: The united states construction industry and its workers. 5th. Silver Spring MD: CPWR – The Center for Construction Research and Training; 2013. http://www.cpwr.com/sites/default/files/publications/5th%20Edition%20Chart%20Book%20Final.pdf. [Google Scholar]
- CPWR – The Center for Construction Research and Training. Construction solutions. 2016 http://www.cpwrconstructionsolutions.org/
- Dale AM, Jaegers L, Welch L, Gardner BT, Buchholz B, Weaver N, Evanoff BA. Evaluation of a participatory ergonomics intervention in small commercial construction firms. Am J Ind Med. 2016a;59:465–475. doi: 10.1002/ajim.22586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dale AM, Miller K, Gardner BT, Hwang CT, Evanoff B, Welch L. Observed use of voluntary controls to reduce physical exposures among sheet metal workers of the mechanical trade. Appl Ergon. 2016b;52:69–76. doi: 10.1016/j.apergo.2015.06.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dale AM, Ryan D, Welch L, Olsen MA, Buchholz B, Evanoff B. Comparison of musculoskeletal disorder health claims between construction floor layers and a general working population. Occup Environ Med. 2015;72:15–20. doi: 10.1136/oemed-2014-102313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: Systematic review and recommendations. Milbank Q. 2004;82:581–629. doi: 10.1111/j.0887-378X.2004.00325.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hecker S, Gibbons B, Barsotti A. Making ergonomic changes in construction: Worksite training and task intervention. In: Alexander D, Raboum R, editors. Appl ergon. London: Taylor & Francis; 2001. pp. 162–189. [Google Scholar]
- Hess JA, Hecker S, Weinstein M, Lunger M. A participatory ergonomics intervention to reduce risk factors for low-back disorders in concrete laborers. Appl Ergon. 2004;35:427–441. doi: 10.1016/j.apergo.2004.04.003. [DOI] [PubMed] [Google Scholar]
- Jaegers L, Dale AM, Weaver N, Buchholz B, Welch L, Evanoff B. Development of a program logic model and evaluation plan for a participatory ergonomics intervention in construction. Am J Ind Med. 2014;57:351–361. doi: 10.1002/ajim.22249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kramer DM, Bigelow PL, Carlan N, Wells RP, Garritano E, Vi P, Plawinski M. Searching for needles in a haystack: Identifying innovations to prevent msds in the construction sector. Appl Ergon. 2010;41:577–584. doi: 10.1016/j.apergo.2009.12.003. [DOI] [PubMed] [Google Scholar]
- Lipscomb HJ, Schoenfisch AL, Cameron W. Non-reporting of work injuries and aspects of jobsite safety climate and behavioral-based safety elements among carpenters in washington state. Am J Ind Med. 2015a;58:411–421. doi: 10.1002/ajim.22425. [DOI] [PubMed] [Google Scholar]
- Lipscomb HJ, Schoenfisch AL, Cameron W, Kucera KL, Adams D, Silverstein BA. Workers’ compensation claims for musculoskeletal disorders and injuries of the upper extremity and knee among union carpenters in washington state, 1989–2008. Am J Ind Med. 2015b;58:428–436. doi: 10.1002/ajim.22433. [DOI] [PubMed] [Google Scholar]
- NIOSH. Simple solution for home building workers: DHHS (NIOSH) Publication No. 2013-111. 2013. [Google Scholar]
- Rinder MM, Genaidy A, Salem S, Shell R, Karwowski W. Interventions in the construction industry: A systematic review and critical appraisal. Human Factors and Ergonomics in Manufacturing. 2008;18:212–229. [Google Scholar]
- Rogers E. Diffusion of innovations. 5. Simon and Schuster; 2003. p. 576. [Google Scholar]
- Rogers EM. Lessons for guidelines from the diffusion of innovations. The Joint Commission Journal on Quality Improvement. 1995;21:324–328. doi: 10.1016/s1070-3241(16)30155-9. [DOI] [PubMed] [Google Scholar]
- Schneider S. Ergonomics: Implement ergonomic interventions in construction. Appl Occup Environ Hyg. 1995;10:822–824. [Google Scholar]
- Weinstein MG, Hecker SF, Hess JA, Kincl L. A roadmap to diffuse ergonomic innovations in the construction industry: There is nothing so practical as a good theory. Int J Occup Environ Health. 2007;13:46–55. doi: 10.1179/107735207800245054. [DOI] [PubMed] [Google Scholar]
- Welch LS, Russell D, Weinstock D, Betit E. Best practices for health and safety technology transfer in construction. Am J Ind Med. 2015;58:849–857. doi: 10.1002/ajim.22456. [DOI] [PubMed] [Google Scholar]