

Abstract
Background
Congenital diaphragmatic hernia (CDH) is a congenital abnormality, rare in adults with a frequency of 0.17–6%. Diaphragmatic rupture is an infrequent consequence of trauma, occurring in about 5% of severe closed thoraco-abdominal injuries. Clinical presentation ranges from asymptomatic cases to serious respiratory or gastrointestinal symptoms. Diagnosis depends on anamnesis, clinical signs and radiological investigations.
Methods
From May 2013 to June 2016, six cases (four females, two males; mean age 58 years) of diaphragmatic hernia were admitted to our Academic Department of General Surgery with respiratory and abdominal symptoms. Chest X-ray, barium studies and CT scan were performed.
Results
Case 1 presented left diaphragmatic hernia containing transverse and descending colon. Case 2 showed left CDH which allowed passage of stomach, spleen and colon. Case 3 and 6 showed stomach in left hemithorax. Case 4 presented left diaphragmatic hernia which allowed passage of the spleen, left lobe of liver and transverse colon. Case 5 had stomach and spleen herniated into the chest. Emergency surgery was always performed. The hernia contents were reduced and defect was closed with primary repair or mesh. In all cases, post-operative courses were uneventful.
Conclusion
Overlapping abdominal and respiratory symptoms lead to diagnosis of diaphragmatic hernia, in patients with or without an history of trauma. Chest X-ray, CT scan and barium studies should be done to evaluate diaphragmatic defect, size, location and contents. Emergency surgical approach is mandatory reducing morbidity and mortality.
Keyword: Congenital diaphragmatic hernia, Diaphragmatic rupture, Mesh, Emergency surgery, Laparotomy, Thoracotomy
Background
Congenital diaphragmatic hernia (CDH) is an abnormality found in 1/2500 newborns, with a survival rate of 67% [1]. A primary characterization of CDH is that the diaphragm fails to form properly during embryogenesis. This incomplete formation of the diaphragm allows abdominal contents to herniate into the chest creating a mass-like effect that impedes lung development. Clinical presentation ranges from asymptomatic cases to serious respiratory or gastrointestinal symptoms, and sometimes haemodynamic instability. The broad spectrum of severity in patients with CDH is dependent on the degree of pulmonary hypoplasia and pulmonary hypertension. Posterolateral hernias (Bochdalek hernias) are the most common hernia type (>80%) with the majority occurring on the left side (85%), less frequently on the right side (13%) or bilateral (2%) [2].
Diaphragmatic rupture (DR) is an infrequent complication of trauma that occurs during 5% of trauma, including vehicle accidents [3–5]. Diagnosis is usually delayed; patients may be asymptomatic for years after trauma, until complications occur. Traumatic rupture of the diaphragm is considered an indication for surgical repair, especially in symptomatic patients [6].
However, there is no consensus on the absolute indications to surgery and about the timing. The onset of complications carries highest mortality and morbidity rates; therefore, it makes emergency surgery mandatory. During the past decades, primary suture repair or covering the defect with a synthetic mesh has been the standard procedures. More recently, biologic meshes have been thought to be effective in closing the diaphragmatic defect, inducing limited inflammatory response and minimizing adhesion formation [7]. Laparotomy or thoracotomy are the traditional treatments for patients with DR. Moreover, laparoscopic approaches for repair of hernias have recently gained in popularity [8]. Robotic approach is not yet described as effective approach in emergency, and it is reported in literature in only one case [9] in elective surgery.
This paper includes the surgical experience of congenital or traumatic diaphragmatic hernia of a surgical unit in emergency setting and reports the literature.
Methods
Six cases of diaphragmatic hernia were observed in emergency at our Academic Department, with respiratory and abdominal symptoms. No breath sounds were detected in the left chest area, but bowel sounds were audible. Emergency surgery was performed in all cases. The hernia contents were reduced, and the defect was closed with primary repair or mesh.
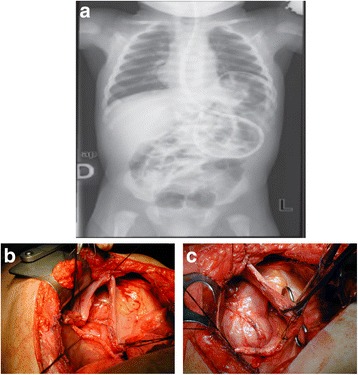
Case 1: A 63-year-old woman was admitted with complaints of bowel obstruction and dyspnoea. Anamnesis revealed chronic abdominal pain, mental retardation and strabismus. In the physical examination, no breath sounds were detected in the left chest area; however, bowel sounds were audible. Chest X-ray and barium enema showed the transverse colon displaced into the left hemithorax above the splenic flexure. Computed tomography suggested collapse of the lung and the mediastinal shift towards the right. The left diaphragmatic hernia contained the transverse and descending colon (Fig. 1a). Emergency laparotomy was performed, and a left diaphragm agenesis, mega colon (diameter 10 cm) and left liver agenesis were found. An intra-operative bronchoscopy revealed hypoplasia of the left lung (Fig. 1b). A subtotal colectomy with ileo-rectal anastomosis was performed, and primary repair of diaphragm was done. The post-operative course was uneventful, and the patient was discharged on the 15th post-operative day. The research of abnormalities of the karyotype, phenotype and genetic pattern was negative for all the known congenital syndromes.
Fig. 1.
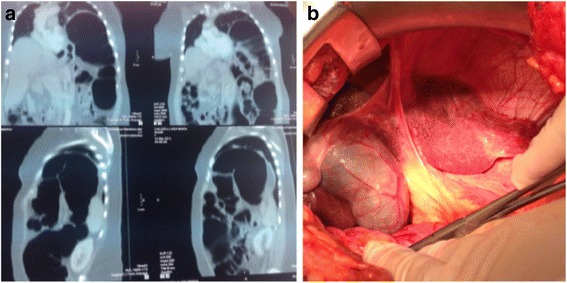
a CT scan shows collapse of the lung and the mediastinal shift towards to the right side. The left diaphragmatic hernia contained the transverse and descending colon. b Intraoperative evidence: diaphragmatic defect allows migration of viscera
Case 2: A 50-year-old woman was admitted with complaints of dyspnoea, chest and abdominal pain. No breath sounds were detected in the left chest area. There was no history of trauma. Chest X-ray revealed mediastinal shift towards the right and bowel gas in the left chest. CT scan showed large annular diaphragmatic defect which allowed passage of the stomach, spleen and colon (Fig. 2). An emergency combined chest-abdominal approach was performed, and contents were reduced repairing the defect with Mersilene mesh®. Thoracotomy approach was used to release the thoracic dense adhesion between the chest and the abdominal contents. Before placing the mesh, the anaesthesiologist increased the tidal volume to expand the collapsed left lower lobe of the lung and a chest drain was placed in the left pleural space. Immediate post-operative chest X-ray showed expansion of the left lung with minimal pleural effusion. Post-operative course was uneventful, and post-operative stay was 13 days.
Fig. 2.

CT scan shows in left side, large diaphragmatic defect which allows passage of the stomach, spleen and colon (referred to as Bochdalek hernias) and complete collapse of left lung
Case 3: A 73-year-old woman arrived with complaint of breathlessness and dysphagia. No history of trauma was evident in anamnesis. Her current medical history included hypertension and hypothyroidism. Chest X-ray and barium studies demonstrated the presence of stomach in left hemithorax. CT scan revealed the presence of large diaphragmatic hernia which allowed the stomach to herniate into the chest. Emergency laparoscopy was performed; hernia contents were reduced; and a repair of the defect with Proceed mesh® was done (Fig. 3). The post-operative course was uneventful, and patient was discharged 7 days after surgery.
Fig. 3.
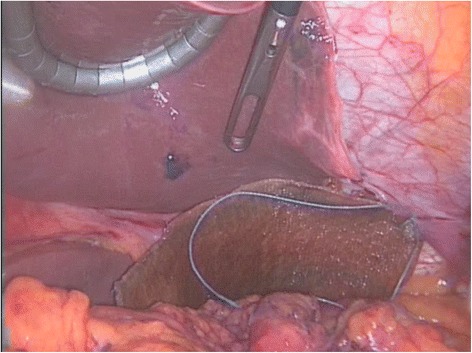
Laparoscopic image during correction of defect with synthetic mesh
Case 4: A 63-year-old woman was admitted with complaints of breathlessness for 2 days, which was gradually progressive and associated with left-sided chest pain and a dry cough. There was a history of a vehicle accident 6 years ago. The initial chest radiograph revealed an elevated left hemi diaphragm with presence of a colon gas shadow in the lower half of the hemithorax. CT scan suggested left diaphragmatic hernia which allowed passage of the spleen, left lobe of liver and transverse colon (Fig. 4a). Surgery was performed in emergency, reducing contents and repairing the defect with biological mesh (Fig. 4b; Tutomesh, bovine pericardium mesh ®). The patient was discharged on the 10th post-operative day, without complications.
Fig. 4.
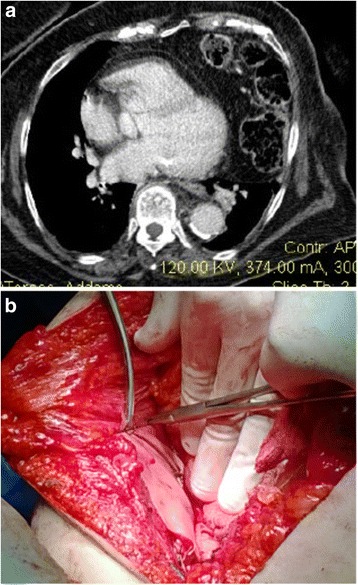
a CT scan suggests left diaphragmatic hernia which allowed migration of colon in left chest. b Intraoperatively, biological mesh repairing defect
Case 5: A 50-year-old man was involved in a work accident. He was managed in accordance with Advanced Trauma Life Support protocol. He arrived in the emergency room with decreased breath sounds on the left side, dyspnoea, fever, left hypochondrium hematoma, subcutaneous emphysema, and chest and abdominal pain. His current medical history included obesity and treated hypertension. Initial chest radiography and barium studies demonstrated stomach in the left hemithorax. CT scan revealed stomach and spleen in left hemithorax, consistent with a traumatic diaphragmatic rupture with complete disruption of all muscular layers, collar sign and multiple rib fractures, fractured left humerus and scapula (Fig. 5a, b). At exploratory laparotomy, traumatic defect in the left diaphragm was found, with stomach and spleen in the left thorax (Fig. 5c). The hernia contents were reduced and the defect was closed with biologic mesh (Tutomesh bovine pericardium mesh ®). Post-operatively, the patient was placed in an intensive care unit. He was transferred from the ICU on the 8th post-operative day and discharged on the 20th day.
Fig. 5.
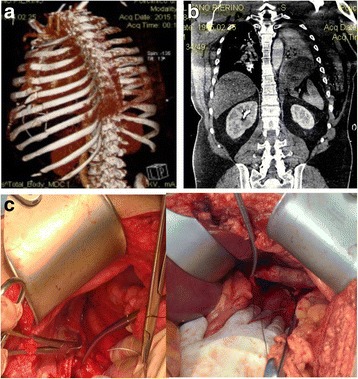
a 3D-CT scan shows rib fractures. b CT scan shows stomach and spleen in the left hemi-thorax, complete disruption of all muscular layers. c Intraoperatively, repair of traumatic defect in the left diaphragm
Case 6 [10]: A 51-year-old man, referred to a history of 5 months of dyspnea, abdominal pain, nausea and vomiting. These symptoms had increased in severity during the previous 2 weeks. Anamnesis revealed left splenopancreatectomy 4 years earlier for non-Hodgkin’s lymphoma. The physical examination revealed a moderate peritoneal effusion without a peritoneal reaction. The introduction of a nasogastric tube remarkably improved symptoms. The chest X-ray showed a large fluid level beneath an apparently raised left hemi diaphragm (Fig. 6a) hypothesizing a left hemi diaphragmatic rupture with gastric herniation; diagnosis was confirmed by barium studies and a thoracic-abdominal computed tomography. An emergency left thoracotomy was performed, revealing a volvulus of the stomach, with some intestinal loops. Part of the transverse colon was incarcerated herniating through the torn diaphragm. The hernia was localized into the posterior side of the left hemi diaphragm with a diameter of 12 cm. During surgery, dense adhesions between the herniated organs and the left pleura-lung, as well as a marked reduction in left lung volume and an inflammatory mass in the greater omentum adherent to the diaphragm, were found. Thus, a reduction of the volvulus, an adhesiolysis and a resection of the mass were performed. Finally, a direct suture of the left diaphragmatic defect was employed (Fig. 6b, c). The patient had an uneventful recovery and histology showed Hodgki’s lymphoma.
Fig. 6.
a X-ray shows herniated stomach into the chest. b Thoracotomy shows large diaphragmatic defect. c Repair of defect
Review of the literature
A systematic review was performed by consulting PubMed/MEDLINE from 1983 to 2017 using the terms “emergency surgery”, associated with “traumatic diaphragmatic rupture”, and “congenital diaphragmatic hernia”. The search returned 555 papers (Fig. 7). Three hundred twenty-three publications were excluded because these articles were not written in English (N = 87), presented cases in childhood (<19 years old; N = 178) or were not interesting human species (N = 58); 32 papers were excluded because regarded hiatal hernia, 40 paraesophageal hernia and 59 elective setting. Consequently, the full texts of 101 articles were assessed for eligibility: the ethiopathogenesis was traumatic in 697 patients and congenital in 38 (Table 1).
Fig. 7.
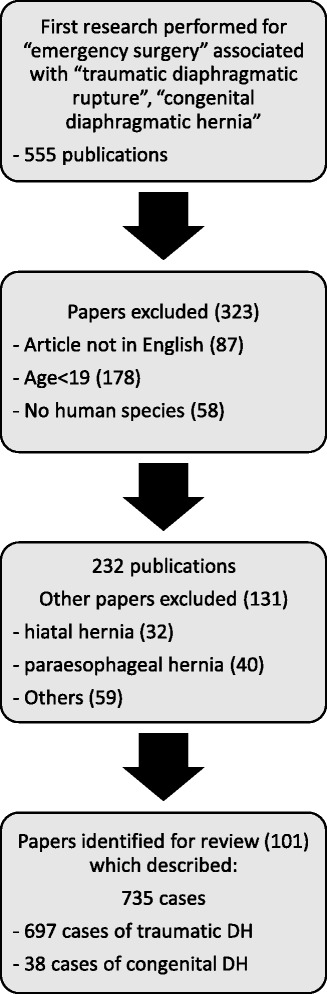
Flow chart of the literature selection process
Table 1.
Review of literature showing demographics data, diagnosis and treatment
| Authors, references |
Number of patient, sex, age (years) | Aetiology | Diagnosis | Treatment | Type of hernia | Herniated organs |
|---|---|---|---|---|---|---|
| Lu J et al. Medicine 2016 [41] | 1, M, 51 | Traffic accident | Barium enema CT scan | Splenectomy | Left hemi diaphragm | Splenic flexure of the colon |
| 1, M, 45 | Traffic accident | Chest X-ray, gastrografin contrast | Splenectomy | Left hemi diaphragm | Stomach and small bowel | |
| 1, M, 47 | Traffic accident | Chest X-ray, gastrografin contrast | Splenectomy | Left hemi diaphragm | Stomach and omentum | |
| 1, M, 30 | Traffic accident | Chest X-ray, Gastrografin contrast | Nonoperative treatment | Left hemi diaphragm | Stomach and omentum | |
| 1, M, 33 | Traffic accident | Chest X-ray, gastrografin contrast | Nonoperative treatment | Left hemi diaphragm | Stomach and omentum | |
| 1, M, 29 | Penetrating injury | Chest X-ray, gastrografin contrast | Nonoperative treatment | Left hemi diaphragm | Stomach and omentum | |
| Manabu Harada, Int J Surg Case Rep. 2016 [42] | 1, M, 78 | Bochdalek hernia | Chest radiography and computed tomography | Laparoscopic Primary closure | Left hemi diaphragm | Omentum, transverse colon, and small intestine |
| De la Cour CD; Ugeskr Laeger. 2016 [43] | 1, F, 27 | Partum | Chest radiography and computed tomography | Primary closure | Left hemi diaphragm | |
| Razi K; J Surg Case Rep. 2016 [44] | 1, F, 83 | Morgagni hernia | Chest radiography and computed tomography | Mesh closure | Left hemi diaphragm | Transverse colon, greater curvature of the stomach and a partial gastric volvulus |
| Manson HJ Ann R Coll Surg Engl. 2016 [45] | 1, F, 30 | Bochdalek hernia | Chest radiography and computed tomography | Total gastrectomy with primary Roux-en-Y reconstruction, splenectomy and insertion of a feeding jejunostomy | Left hemi diaphragm | Gangrenous stomach and spleen, cardiac arrest |
| Massloom HS; N Am J Med Sci. 2016. [46] | 1, M, 50 | Bochdalek hernia | Computed tomography | Laparotomy and thoracotomy for repairing of defect | Left hemi diaphragm | Bowel |
| Kumar, J Surg Case Rep. 2016 [47] | 1, M, 80 | Morgagni hernia | Computed tomography | Laparotomy primary suture | Left hemi diaphragm | Gastric outlet obstruction |
| Manipadam JMJ Clin Diagn Res. 2016 [48] | 1, M, 23 | Bochdalek hernia | Chest X-ray | Laparotomy, sleeve resection of the gangrenous portion of the stomach | Left hemi diaphragm | Organoaxial volvulus of the stomach |
| Harada M, Int J Surg Case Rep. 2016 [49] | 1, M, 78 | Bochdalek hernia | Chest radiography and computed tomography | laparoscopic repair with primary closure | Left hemi diaphragm | Omentum, transverse colon, and small intestine |
| Siow SL; J Med Case Rep. 2016 [50] | 1, M, 32 | Traffic accident | Computed tomographic scan | Laparoscopic surgery with synthetic mesh repair | Left hemi diaphragm | |
| A.L. Andreev JSLS 2010 [51] | 1, M, 40 | Traffic accident 12 years earlier |
CT scan | Laparoscopic primary suture | Left hemi diaphragm | Large intestine and greater omentum and acute colon obstruction |
| 1, M, 46 | Surgery for a stab wound to the chest with injury to the heart 5 months before |
Chest X-ray | Laparoscopic primary suture | Left hemi diaphragm | Transverse colonic segment |
|
| Bhatt NR, Trauma Mon. 2016 [52] |
1, M, 23 | Multitrauma 2 y before | Chest X-ray and CT scan | Laparotomy, adhesiolisis and primary repair | Left hemi diaphragm | Small bowel, omentum and large bowel obstruction |
| Abdullah M, Stonelake P BMJ case rep 2016 [53] | 1, F 65 | Trauma | Chest X-ray, CT scan | Emergency operation, laparotomy | Left hemi diaphragm | Perforated colon |
| Razi K; Journal of Surgical Case Reports, 2016 [54] | 1, F, 83 | Diaphragmatic Morgagni Hernia | Chest X-ray and CT scan | Laparoscopic repair with a composite mesh with an absorbable tic fixation on the diaphragm |
Left hemi diaphragm | Transverse colon, the greater curvature of the stomach with a partial gastric volvulus |
| A Wigley J Ann R Coll Surg Engl 2014 [55] | 1, F, 72 | Traffic accident | ||||
| Atef Mejri Medicine 2015 [56] |
1, M, 56 | Bochdalek hernia | Chest X-ray, barium studies and CT scan | Primary repair Laparoscopy was converted laparotomy | Left hemi diaphragm | Gastric volvulus |
| Mahmut Tokur Ulus Travma Acil Cerrahi Derg, July 2015 [57] |
1, F, 27 | Congenital DH | Chest X-ray, CT scan | Thoracotomy, primary repair | Left hemi diaphragm | Gastro thorax |
| Topuz Mustafa Ulus Travma Acil Cerrahi Derg. 2014 [58] |
1, F, 55 | Traffic accident | Chest X-ray, CT scan | Laparotomy primary repair | Right hemi diaphragm | Liver causing mechanic compression on ventricle |
| Moussa G Ann R Coll Surg Engl. 2014 [17] |
1, F, 65 | Previous history of pericardial window fenestration and sarcoidosis | Chest X-ray, CT scan | Laparoscopy, mesh repair | Right hemi diaphragm | Left lobe of liver, stomach and colon |
| Nakamura T, Ulus Travma Acil Cerrahi Derg. 2014 [18] | 1, M, 81 | History of HCC treated with Radiofrequency ablation | Chest US, CT scan | Laparotomy, primary hernia repair, small bowel resection | Right hemi diaphragm | Liver, incarcerated small bowel |
| Haratake Naoki Surgery today 2015 [59] |
1, F, 50 | CT scan | Laparotomy, primary hernia repair | Right hemi diaphragm | Heterotopic endometriosis in a patient with Chilaiditi syndrome | |
| Gali BM, Niger J Med. 2014 [60] | 1, M, 28 | Penetrating injury years before | CT scan | Laparotomy, primary repair | Left hemi diaphragm | Bowel |
| Michael Joseph Newman, BMJ Case Rep 2014 [61] |
1, M, 25 | Bochdalek hernia | Chest X-ray, CT scan | Laparotomy, primary repair, gastric resection | Left hemi diaphragm | Stomach and bowel |
| Tyagi Sam, Ann Thorac Surg. 2014 [62] |
1, M, 36 | Morgagni hernia | Chest X-ray, CT scan | Laparoscopy Gore-Tex fixed with a spiral tacker | Left hemi diaphragm | Omentum and transverse colon |
| Kurniawan N, Acta Chir Belg. 2013 [32] | 1, M, 17 | Bochdalek hernia | Chest X-ray, CT scan | Laparoscopy primary sutture | Left hemidiaphragm | Stomach, spleen colon |
| Ota H Ann Thorac Cardiovasc Surg. 2014 [63] |
1, M, 62 | Fall accident | ECO FAST, Chest X-ray, CT scan |
Video assisted mini thoracotomy Primary suture |
Right hemi diaphragm | Hemothorax |
| G, et al. BMJ Case Rep 2013 [64] | 1, M, 60 | Fall | Chest X-ray, CT scan | Laparoscopy and laparotomy | Left diaphragm | Stomach, bowel and spleen |
| Sonthalia N, J Emerg Med. 2013 [65] | 1, F, 78 | Morgagni hernia | Chest X-ray, CT scan, barium studies | Thoracotomy | Left diaphragm | Gastric volvulus |
| Nayak HK BMJ Case Rep. 2012 [66] |
1, M, 50 | Blunt trauma | EGDS, barium studies, CT SCAN | Laparoscopic repair | Left hemi diaphragm | Gastric volvulus and duodenum |
| Vernadakis S, Transplant Proc. 2012 [67] |
1, F, 46 | Liver donor | Chest X-ray, CT scan, barium studies | Laparotomy | Right diaphragm | Bowel |
| Ngai I, BMJ Case Rep. 2012 [68] |
1, F, 31 | Pregnancy | MRI | Nasogastric tube | Left hemi diaphragm | Spleen, bowel, stomach and pancreas |
| Elangovan A J Emerg Med. 2013 [69] |
1, M, 30 | Accident | Chest X-ray and CT scan | Laparoscopy | Left hemi diaphragm | Stomach |
| Kuppusamy A, Ulus Trauma Acil Cherrai Derg 2012 [70] | 1, M, 28 | Trauma | CT scan | Thoracotomy | Right hemi diaphragm | Liver |
| Ismail Okan, Ulus Travma Acil Cerrahi Derg. 2011 [71] |
10 cases, 44,3 y |
Trauma | CT scan | 7 laparotomy 1 thoracic-abdominal approach 2 thoracic |
9 left side | |
| Ioannis Baloyiannis General Thoracic and Cardiovascular Surgery 2011 [72] |
1, M, 56 | Trauma | Laparotomy | |||
| Vassileva CM Ann Thorac Cardiovasc Surg. 2012 [73] |
1, F, 25 | Morgagni hernia | Chest X-ray, CT scan | Laparoscopic repair | Right hemi diaphragm | Omentum |
| Agrafiotis AC Acta Chir Belg. 2011 [74] |
1, F, 52 | Bochdalek hernia | Chest X-ray, CT scan | Laparoscopic approach, and mini laparotomy prosthetic polypropylene mesh | Left hemi diaphragm | Small bowel loops and the right colon |
| Tan K K, Singapore Med J 2009 [75] | 14, median age 38 y | Trauma | Chest X Ray, CT Scan, RMN | Laparotomy, thoracotomy or VATS Primary repair (85.7%) patients or patch repair |
five (35.7%) right-sided and nine (64.3%) left-sided diaphragmatic ruptures | |
| Akhtar K, Br J Hosp Med (Lond). 2009 [76] |
1, M, 27 | Bochdalek hernia | Chest X Ray, Upper gastrointestinal endoscopy, CT scan |
Laparoscopy Goretex dual mesh |
Left hemi diaphragm | Small bowel, ascending and transverse colon, and spleen |
| Ozpolat B, Ulus Travma Acil Cerrahi Derg. Nov; 2009 [77] |
1, M, 52 | Tube thoracostomy at the seventh left intercostal | Chest X-ray, MRI | Left standard thoracotomy, primary suture | Left hemi diaphragm | Omentum |
| Altinkaya N Hernia. 2010 [78] | 12 patients mean age of 60 years, ten were female. |
Morgagni hernia | CT scan | Six patients had surgery. 1 emergency surgery for hernia, 2 laparoscopic hernia repair, 3 trans-abdominal repair and 1 transthoracic repair | Right hemi diaphragm | Omentum and colon |
| Syed Murfad Peer, Int J Surg. 2009 [79] | 2496 patients25 (86%) males4 (14%) females mean age 33.6 y | Trauma | Chest X-ray diagnostic in 20 (69%) patients CT scan in 4 (14%) patients. Intra-operative diagnosis of rupture diaphragm was made in 5 (17%) patients. | 29 (1.1%) underwent to surgery 20 thoracotomy (69%) 8 laparotomy (27.5%) 1 Thoracoabdominal approach (3.5%) |
Right defect: 6 left defect:23 |
|
| Sung HY J Korean Med Sci. 2009 [80] |
1, F, 49 | Congenital hernia | Chest radiography | Thoracotomy | Left hemi diaphragm | Stomach, spleen, splenic flexure of the colon bowel loops |
| Ouazzani A Acta Chir Belg. 2009 [81] |
1, M, 24 | Trauma | Chest X-ray computed tomography | Laparoscopically, with mesh | Left diaphragm | Stomach |
| Kavanagh D Acta Chir Belg. 2008 [82] |
1, M, 76 | Bochdalek hernia | Chest radiograph and computed tomogram | Laparotomy, primary repair | Right diaphragm | Strangulation of a portion of transverse colon |
| Yeh-Huang Hung; J Chin Med Assoc. 2008 [83] | 1, M, 74 1, F, 75 |
Bochdalek hernia Bochdalek hernias |
Chest X-ray CT scan MRI |
Laparotomy Transthoracic repair |
Left diaphragm Right diaphragm |
Intestinal obstruction Small and large bowels |
| Sano A Surg Today. 2008 [16] |
1, F, 25 | Diaphragm hernia during pregnancy | Chest radiograph and computed tomography | Emergency caesarean section sutures and a Gore-Tex sheet |
Left diaphragm | Bowel loop |
| Gourgiotis S, Turkish Journal of Trauma & Emergency Surgery 2008 [84] | 1, M, 25 | Trauma | Chest X-ray CT scan |
Laparoscopic primary repair | Left diaphragm | |
| Walchalk LR, J Emerg Med. 2010 [85] | 1, F, 57 | Trauma | ||||
| Mohammadhosseini B, J Coll Physicians Surg Pak. 2008 [86] | 1, M | Bochdalek hernia | ||||
| Boyce S, Obes Surg. 2008 [87] | Diaphragmatic hernia post surgery | CT of the chest and abdomen | Laparotomy an repair of hernia | Left diaphragmatic hernia | Ischemic small bowel | |
| Tsuboi K, Surg Today. 2008 [88] | 1, M, 50 | 16 months after surgery | Computed tomography of the chest | Laparotomy | Left diaphragmatic hernia | Stomach had herniated into the thoracic cavity |
| Vogelaar Obes Surg. 2008 [89] | 1, F, 37 | Six months after gastric banding | Chest X-ray computed tomography scan | Laparotomy | Left diaphragm | Intra thoracic stomach distended, rotated, and perforated at the orifice of the hernia |
| Young-Shun Wu; Am J Emerg Med. 2008 [90] | History of left-sided upper abdominal blunt injury 2 months before | CT scan | Thoracotomy and primary repair | Left traumatic diaphragm rupture | ||
| Igai H, Y Gen Thorac Cardiovasc Surg. 2007 [91] | 1, M, 48 | Trauma | Chest X-ray, CT scan | Right diaphragm rupture | Hepatothorax | |
| Rifki Jai S Arch Gynecol Obstet. 2007 [92] | 1, F, 27 | 32-week gestation no history of trauma |
Chest X-ray CT scan |
Emergency laparotomy | Left hemi diaphragm. | Stomach, transverse colon and greater omentum herniated in the left hemithorax |
| Rout S Hernia. 2007 [93] |
1, F, 35 | Bochdalek hernias | Chest X-ray CT scan |
Emergency laparotomy defect was repaired using non-absorbable sutures | Right-sided Bochdalek hernia | Colon |
| Campbell AS Hernia. 2007 [94] | 1, M, 85 | Chest X-ray CT scan | Emergency laparotomy identified a massive diaphragmatic defect which was not amenable to primary closure. A colopexy procedure was performed | Left hemi diaphragm. | Diaphragmatic herniation of bowel | |
| Testini M Surg Today. 2006 [10] | 1, M, 51 | Left splenopancreatectomy 4 years earlier |
Chest X-ray, CT scan, MRI | Left thoracotomy | Left hemi diaphragm | Stomach |
| Luu TD, Ann Thorac Surg 2006 [95] | 1, F, 34 | 33 weeks’ gestation | Chest roentgenogram, CT scan, barium study Esophagoscopy | the patient went into preterm labour and had a spontaneous vaginal delivery of a healthy new-born at 34 weeks’ gestation. left thoracotomy | Left hemi diaphragm | Necrotic stomach |
| Iso Y., Hernia 2006 [96] |
1, F, 81 | Morgagni’s hernia | Chest X-ray | The diaphragm defect was sutured first, and partial resection of the transverse colon | Right thorax | transverse colon |
| Eglinton T, ANZ J Surg. 2006 Jul [97] | 3 cases | During third trimester of pregnancy | Chest X-ray | Laparotomy and thoracotomy in one case. Delivery was by Caesarean section at the time of emergency surgery | ||
| Barbetakis N, World J Gastroenter ol. 2006 Apr 21 [98] | 1, F, 31 | Bochdalek hernias during pregnancy (23-week gestation) | Chest X-ray, chest ultrasound | Left thoraco- abdominal incision, segmental resection of the involved portion of large bowel. The diaphragmatic defect was repaired with interrupted sutures | Left hemi thorax | Strangulated Right and transverse colon, necrotic the greater omentum and stomach |
| Barret J, J Emerg Med. 2006 [99] | 1,M, 50 | Trauma | Electrocardiogram and CT scan | Left hemi thorax and pericardium | ||
| Abboud B, J Med Liban. 2004 [100] | 1 M | Trauma | Chest X-ray, exploratory laparotomy | Laparotomy, colectomy resection of ileum with anastomosis | left hemi thorax | Transverse colon and a proximal small bowel |
| Hsu YP, Hepatogastroenterology. 2005 [101] | 78 patients | Trauma | Chest roentgenogram | Only 20% of elderly patients were operated on within 24 h of trauma, 87% of young patients | ||
| P Ransom Emerg Med J 2005 [102] | 1, M, 21 | Trauma | Chest radiograph, ultrasound, oesophago-gastro- duodenoscopy | Thoracotomy | Left diaphragm | Stomach and a loop of colon had herniated through a 6 cm defect |
| Tiberio GA Acta Chir Belg. 2005 Feb [103] | 33 p | Blunt (22 patients) or penetrating injury | Chest X-ray, CT scan | Laparotomy | ||
| Barakat MJ, BMC Surg. 2005 [19] | 1, F, 43 | CDH in Marfan’s syndrome | Chest X-ray, CT scan | Laparoscopy | Right hemi diaphragm | Perforated gangrenous appendix |
| Gupta V Eur J Emerg Med. 2005 [104] | 1, M, 43 | Spontaneous rupture | CT scan | Left hemi diaphragm | ||
| Kara E Ann Acad Med Singapore 2004 [105] | 1, M, 28 | Trauma | Chest X-ray, CT scan | Left thoracotomy | Left hemi diaphragm | Gastric fundus |
| Sirbu H Hernia. 2005 [106] | 1, M, 67 | Trauma | CT scan | Laparotomy and right thoracotomy | Delayed bilateral diaphragmatic ruptures | |
| Dalton AM Emerg Med J. 2004 [107] | 1, M, 43 | Bochdalek hernia | Chest radiograph | Thoracotomy | Left hemi thorax | Stomach, transverse colon, and spleen in to the chest. |
| Niwa T Respiration. 2003 [108] | 1, F, 53 | Bochdalek hernia | Chest X-ray | Thoracotomy | Left hemithorax | Stomach and greater omentum |
| Genc MR, Obstet Ginecol 2003 [109] |
1, M, 29 | Bochdalek hernia during pregnancy | Chest X-ray, CT scan | Antepartum repair | Left hemithorax | Bowel obruction |
| Sato M, Jpn J Thorac Cardiovasc Surg. 2002 [110] | 1, M, 57 | Traffic accident | Chest X-ray, CT scan, MRI | Toracoscopy | Right hemidiaphragm | Liver |
| Guven H, Acta CHir Belg 2002 [111] | 2 cases | Morgagni hernia | Bowel perforation Upper gastrointestinal bleeding |
|||
| Kanazawa A, Surg Today 2002 [112] | 1 F 63 y | Bochdalek hernia | Chest X-ray, CT scan, | Thoraco-Laparotomy Primary suture |
Right hemidiaphragm | Colon and right kidney |
| Fisichella PM, Ann Ital CHIR 2001 [113] | 1 F 55 y | Bochdalek hernia | Computed tomography | Thoracotomy and laparotomy | Right hemidiaphragm | Liver intestinal maloration |
| Bergeron E, J Trauma 2002 [15] | 160 cases | Trauma | ||||
| Carreno G, Surg Endosc 2001 [114] | 1, M, 52 | Bochdalek hernia | CT scan | Laparoscopic approach | Left hemi thorax | Colon and volvulated stomach |
| Prieto Nieto I, Acta chir Belg 2001 [115] | 1, M, 36 | 8 months after trauma | CT scan | Laparotomy, repair of defect, gastric perforation were closed | Left hemi diaphragm | Gastric incarceration and perforation |
| Nursal TZ, Hernia 2001 [116] | 26 cases | Trauma | Chest X-ray, CT scan, | 92% Primary repair | 92% left hemi diaphragm | 31.8% stomach 27,2 colon |
| Bujanda L, J Clin Gastroenterol 2001 [117] | 1 | Bochdalek hernia | Left hemi diaphragm | Gastric volvulus | ||
| Pross M, J Laparoendosc Adv Surg Tech A 2000 [118] | 1, M, 20 | Trauma | Diagnostic laparoscopy | Laparoscopy primary repair | Left hemi diaphragm | Stomach |
| Saito Y, Surg Today 2000 [119] | 1, M, 51 | 3 years after pleuropneumectomy for mesotelioma | Laparotomy | Left hemi thorax | Ulcer of stomach, which was displaced into the thorax, had perforated aorta | |
| De Waele JJ, J Accid Emerg Med 1999 [120] | 1, M, 45 | Trauma | Chest X-ray, Chest tube; ultrasound, | Laparotomy, resection of spleen | Left hemi thorax | Spleen completely disrupted |
| Colliver C, J Trauma 1997 [121] | 1, M, 80 | Trauma | Echocardiograph, ultrasonography | Left hemi diaphragm | Stomach Intrapericardial hernia | |
| Zantut LF, Rev Paul Med 1993 [122] | 1, M, 33 | Trauma | Chest X-Ray, liver scintigraphy, CT scan, MRI, diagnostic laparoscopy | Laparoscopy | Bilateral diaphragmatic rupture | |
| Allen MS, J Thorac Cardiovasc Surg 1993 [123] | 147 cases 5 emergency setting |
Chest X-ray CT scan | Left hemi diaphragm | Stomach | ||
| Girzadas DV Jr Ann Emerg Med. 1991 [124] |
1, F, 71 | Trauma | Chest radiograph | Pericardial sac | Omentum and transverse colon | |
| Thomas S Jpn J Surg. 1991 [125] |
2 cases | Bochdalek hernia | X-ray of the chest and contrast studies of the gastrointestinal tract | Laparotomy | Left hemi diaphragm | Intestinal obstruction |
| Bush CA, South Med J 1990 [126] |
2 cases | Trauma | Chest X-ray, barium studies of the gastrointestinal tract, CT scans, ultrasonography, laparoscopy, and radionuclide scanning | Laparoscopy | Left hemi diaphragm | Intestinal obstruction |
| Feliciano DV, J Trauma 1988 [127] | 16 cases | Penetrating trauma | Chest X-ray | Laparotomy | ||
| Chidamdaram M Thorac Cardiovasc Surg. 1988 [128] |
1, M, 32 | Trauma | Chest X-ray | Thoracotomy | Left hemi diaphragm | Stomach |
| Symbas PN, Ann Thorac Surg 1986 [129] | 194 cases | Trauma | Chest X-ray, barium studies exploratory laparotomy | Laparotomy Primary repair In a case Prolene mesh |
||
| Saber WL, J Emerg Med 1986 [130] | 111 cases 8 emergency surgery |
Trauma | Chest X-ray | 7 left 1 right hemi diaphragm |
||
| Gardezi SA, J Pak Med Assoc 1986 [131] | 2 cases 1, M, 43 |
Bochdalek hernia | Chest X-ray | Laparotomy | Left hemi diaphragm | Transverse colon and splenic flexure |
| 1 M 26 y | CDH | Chest X-ray | Laparotomy | Left hemi diaphragm | Greater curvature of stomach, a small part of jejunum, left part of transverse colon and greater omentum | |
| Brown GL, Ann Thorac Surg 1985 [132] | 41 cases | Trauma | Chest X-ray | 23 laparotomy, 13 thoracotomy, 5 combined | 29 Left, 14 Right-sided, hemi diaphragm. |
|
| Clark DE, Surgery 1983 [133] | 10 cases median age 40 |
Trauma | Chest X-ray | Left hemi diaphragm |
M male, F female Y years
Pathogenetic mechanism
Diaphragmatic rupture with abdominal organ herniation was first described in 1541 by Sennertus [11]. Congenital diaphragmatic hernias are prenatally or during the neonatal period diagnosed. On the contrary, CDH in adulthood are exceedingly rare and can occur through an anterior parasternal Morgagni foramen or through a posterolateral, mainly left-sided, named as Bochdalek hernia, firstly described in 1848 [12]. The aetiology is still under study, but the disease is due to the failure of closure of the canal between the septum transversum and the oesophagus during the 8th week of gestation. Morgagni hernia is a rare disease caused by the defective development of the sternal attachments to the diaphragm. Traumatic diaphragmatic hernias are thought to be produced by a sudden increase in the pleuroperitoneal pressure gradient occurring at areas of potential weakness along embryological points of fusion [13].
DR usually result from blunt or penetrating injuries or iatrogenic causes and result in entry of an abdominal hollow viscus or the omentum into the pleural cavity, which may lead to incarceration and even strangulation with a fatal outcome. Traumatic diaphragmatic hernias are frequently caused by a penetrating injury (10–19%), sometimes by blunt thoracic-abdominal trauma (5%) [14, 15]. Moreover, some authors described rare and particularly cases of DR after surgery or pregnancy; that is Sano A. et al. reported a case of a pregnant woman in the 28th week of pregnancy, who was underwent to emergency caesarean section and repair of the diaphragm [16]; Moussa G. et al., described a right DR in a patient with previous history of window fenestration and sarcoidosis [17]; Nakamura T. et al., reported a case of right DR in patient with a history of hepatic carcinoma treated with radiofrequency ablation [18]. Furthermore, there was an association between Marfan’s syndrome and CDH as Barakat et al. reported [19].
Site of rupture
CDH formation is found 80% on the left side [20]. Also, 88–95% of diaphragmatic ruptures occurred on the left side [21], especially, blunt trauma causes large diaphragmatic defects, commonly involving (>80%) the left posterolateral diaphragm [22]. The right haemidiaphragm is stronger than the left one because of the size of the liver which has a protective effect. For this reason, the side ruptures are very rare and associated with high mortality and morbidity rate [23].
The review of literature reported in this study confirmed the high frequency of left defect 80%, and only two cases of bilateral DR were reported.
Presenting symptom and investigations
Nayak et al. described severe symptoms, in 46% of CDH cases with 32% of mortality due to visceral strangulation [24]. Moreover, the literature analysis shows a variable rate of delayed symptoms (5–45.5%) [25, 26]. Late-presenting CDH of left sided typically produces acute, obstructive, gastrointestinal symptoms, chronic dyspnea, chest pain, recurrent abdominal pain, postprandial fullness and vomiting, evolving to cardiorespiratory failure [27]. Indeed, right-sided CDH is usually associated with only respiratory issues because partial liver displacement may block the further herniation of hollow viscera [1]. Although the presence of bowel sounds within the chest and the absence of breath sounds are typical findings associated with a CDH, a misdiagnosis rate of 38% has been reported [28]. Obviously, in totally asymptomatic cases, diagnosis is very hard. On the contrary, when acute presentations occur because of the increasing of abdominal pressure and consequent rapid visceral displacement into the chest or due to rapid distension of previously herniated viscera, diagnosis is clear [29, 30]. Chest X-ray and barium studies are useful for determining which viscera have herniated into the thorax. The most common reported radiological finding of CDH is the opaqueness of the hemithorax usually associated with mediastinal shift to the contralateral side. Moreover, the position of the nasogastric tube in the chest cavity will provide an important indicator and prompt correct diagnosis. Computed tomography can be considered the gold standard technique for diagnosis, offering the unique opportunity to evaluate the presence, size and location of a diaphragmatic defect, as well as the contents of various types of diaphragmatic hernias [31] and showing sensitivity and specificity of 14–82% and 87%, respectively [32]. MRI is also useful, but usually it is not performable in emergency. However, it is usually employed in stable patients or where the CT scan is equivocal [33]. According with literature, in this reported experience, a definitive diagnosis was made with CT scan and barium studies.
Late-presenting CDH is considered as a benign condition but it can rapidly becomes a life-threatening disease [1, 27, 28, 31, 33]; consequently, an immediate surgical treatment is mandatory. Associated anomalies in late-presenting CDH patients, such as congenital heart disease, Fryns syndrome and trisomy 18, have been reported in 8.6–80% of cases [1, 2, 27, 28], significantly increasing the mortality rate. At this proposal, in case 1, even if there was a high suspicion of congenital syndrome, surprisingly it was not confirmed by genetic studies.
Surgical treatment
Surgical repair typically involves primary or patch closure of the diaphragm through an open abdominal approach. When the diagnosis is delayed, due to suspicions of adhesions between viscera and chest, thoracotomy or combined thoracic-abdominal approach is preferred, as in the reported case 2. Some authors have reported success with thoracoscopic approach but vitiated by an increased incidence of hernia recurrence [34–36]. Furthermore, during thoracoscopy, an intraoperative pulmonary hypertension with subsequent hemodynamic instability could develop; moreover, the placement and management of a patch results in substantially longer operating times. For these reasons, thoracoscopic repair of CDH is preferred in the presence of small diaphragmatic defects and/or mild pulmonary hypertension [37]. Nowadays, the laparoscopic approach is safe and feasible for CDH and it could be an excellent option [37], as in case 3.
However, emergency surgery is the treatment of choice for diaphragmatic rupture. In delayed cases, thoracic approach is recommended to reduce viscera-pleural adhesions and to avoid intra-thoracic visceral perforation with catastrophic complications [38]. When the suspicion of intestinal obstruction is evident, an abdominal approach may also be required to control organs. Although the type of closure used for diaphragmatic hernias is still a matter of debate, it is generally accepted that most defects can be primarily closed with a non-absorbable suture [39]. Mesh repair usually is used when the defect is too large to be primarily closed and the use of tension free mesh is vital to the success of the procedures. Recently, biologic mesh has been introduced to replace the synthetic one because of its lower rate of hernia recurrence, higher resistance to infections and lower risk of displacement [7, 40]; however, limited evidence in literature yet exists about their superiority. Indeed, in our previous experience, biologic meshes have also been used in contaminated surgical fields with favourable results [40]. However, because of the rarity of this condition, clinicians should be encouraged to publish their experience with biologic meshes in diaphragmatic hernia repair [7].
Conclusions
When a diaphragmatic hernia is diagnosed, surgery is the treatment of choice, above all in emergency setting. A multidisciplinary approach in dedicated centres is advisable.
Acknowledgements
The authors would like to thank Dr Channielle Mascarenhas and Dr Luke Palma for the English language revision.
Funding
This study did not receive funding.
Availability of data and materials
All data and materials are available in case of request.
Authors’ contributions
Authors contributed to this study as follows: MT contributed to the conception and design. AG contributed to the writing acquisition of the data. RMI contributed to writing. GC and AD contributed to the critical revision. AP contributed to the review of literature. AG contributed to the conception and design and critical revision. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
Ethics approval and consent was waived because this study is a review of literature with a retrospective case series based on six patients that gave consent to participate for publication.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- CDH
Congenital diaphragmatic hernia
- CT
Computed tomography
- DR
Diaphragmatic rupture
- MRI
Magnetic resonance imaging
Contributor Information
Mario Testini, Email: mario.testini@uniba.it.
Antonia Girardi, Email: tonegirar@gmail.com.
Roberta Maria Isernia, Email: roberta_isernia@hotmail.it.
Angela De Palma, Email: adepalma@chirtor.uniba.it.
Giovanni Catalano, Email: giovcatalano@virgilio.it.
Angela Pezzolla, Email: angela.pezzolla@uniba.it.
Angela Gurrado, Email: angelagurrado@libero.it.
References
- 1.Baerg J, Kanthimathinathan V, Gollin G. Late-presenting congenital diaphragmatic hernia: diagnostic pitfalls and outcome. Hernia. 2012;16:461–466. doi: 10.1007/s10029-012-0906-5. [DOI] [PubMed] [Google Scholar]
- 2.Torfs CP, Curry CJ, Bateson TF, Honoré LH. A population-based study of congenital diaphragmatic hernia. Teratology. 1992;46:555–65. doi: 10.1002/tera.1420460605. [DOI] [PubMed] [Google Scholar]
- 3.Pancholi CK, Hombalkar NN, Dalvi SB, Gurav PDY. Left sided hydro-pneumothorax in a operated case of left diaphragmatic hernia repair: a diagnostic dilemma. J Clin Diagn Res. 2015;9:PD03-4. doi: 10.7860/JCDR/2015/11879.5759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Meyers BF, McCabe CJ. Traumatic diaphragmatic hernia. Occult marker ofserious injury. Ann Surg. 1993;218:783–790. doi: 10.1097/00000658-199312000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kozak O, et al. Late presentation of blunt right diaphragmatic rupture (hepatic hernia) Am J Emerg Med. 2008;26(5):638. doi: 10.1016/j.ajem.2007.10.032. [DOI] [PubMed] [Google Scholar]
- 6.DeAlwis K, Mitsunaga EM. Sudden death due to nontraumatic diaphragmatic hernia in an adult. Am J Forensic Med Pathol. 2009;30:366–368. doi: 10.1097/PAF.0b013e318187e013. [DOI] [PubMed] [Google Scholar]
- 7.Antoniou SA, Rudolph P. Frontiers in surgery October 2015. 2015. The use of biological meshes in diaphragmatic defects an evidence-based review of the literature. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Izzo BG, Maffettone V, et al. Laparoscopic treatment of Bochdalek hernia without the use of a mesh. Surg Endosc. 2003;17:1497–1498. doi: 10.1007/s00464-002-4288-0. [DOI] [PubMed] [Google Scholar]
- 9.Chen B, Finnerty BM, Schamberg NJ, Watkins AC, DelPizzo J, Zarnegar R. Transabdominal robotic repair of a congenital right diaphragmatic hernia containing an intrathoracic kidney: a case report. J Robot Surg. 2015;9(4):357–60. doi: 10.1007/s11701-015-0530-3. [DOI] [PubMed] [Google Scholar]
- 10.Testini M, Vacca A, Lissidini G, Di Venere B, Gurrado A, Loizzi M. Acute intrathoracic gastric volvulus from a diaphragmatic hernia after left splenopancreatectomy: report of a case. Surg Today. 2006;36(11):981–4. doi: 10.1007/s00595-006-3281-y. [DOI] [PubMed] [Google Scholar]
- 11.Farhan Rashid, Mallicka M Chakrabart, Rajeev Singh and Syed Y Iftikhar. A review on delayed presentation of diaphragmatic rupture. World J Emerg Surg 2009, 4:32 doi:10.1186/1749-7922-4-32 [DOI] [PMC free article] [PubMed]
- 12.Yeh-Huang H, Yu-Hon C, Sheng-Lei Y, Ming-Feng C. Adult Bochdalek hernia with bowel incarceration. J Chin Med Assoc. 2008;71:10. doi: 10.1016/S1726-4901(08)70162-X. [DOI] [PubMed] [Google Scholar]
- 13.Jing Lu, MDa, Bo Wang, MDb, Xiangming Che, MD, PhDa, Xuqi Li, MDa, Guanglin Qiu, MDa, Shicai He, MDa, Lin Fan, MDa. Delayed traumatic diaphragmatic hernia: a case-series report and literature review. Medicine 2016 [DOI] [PMC free article] [PubMed]
- 14.Mariadason JG, Parsa MH, Ayuyao A, Freeman HP. Management of stab wounds to the thoracoabdominal region. A clinical approach. Ann Surg. 1988;207:335–40. doi: 10.1097/00000658-198803000-00019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bergeron E, Clas D, Ratte S, Beauchamp G, Denis R, Evans D, et al. Impact of deferred treatment of blunt diaphragmatic rupture: a 15-year experience in six trauma centers in Quebec. J Trauma. 2002;52(4):633–40. doi: 10.1097/00005373-200204000-00004. [DOI] [PubMed] [Google Scholar]
- 16.Sano A, Kato H, Hamatani H, Sakai M, Tanaka N, Inose T, Kimura H, Kuwano H. Diaphragmatic hernia with ischemic bowel obstruction in pregnancy: report of a case. Surg Today. 2008;38(9):836–40. doi: 10.1007/s00595-007-3718-y. [DOI] [PubMed] [Google Scholar]
- 17.Moussa G, Thomson PM. Bohra A Volvulus of the liver with intrathoracic herniation. Ann R Coll Surg Engl. 2014;96(7):e27–29. doi: 10.1308/003588414X13946184903324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Nakamura T, Masuda K, Thethi RS, Sako H, Yoh T, Nakao T, Yoshimura N. Successful surgical rescue of delayed onset diaphragmatic hernia following radiofrequency ablation for hepatocellular carcinoma. Ulus Travma Acil Cerrahi Derg. 2014;20(4):295–9. doi: 10.5505/tjtes.2014.03295. [DOI] [PubMed] [Google Scholar]
- 19.Barakat MJ, Vickers JH. Necrotic gangrenous intrathoracic appendix in a marfanoid adult patient: a case report. BMC Surg. 2005;5:4. doi: 10.1186/1471-2482-5-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Brown SR, Horton JD, Trivette E, et al. Bochdalek hernia in the adult: demographics, presentation, and surgical management. Hernia. 2011;15:23–30. doi: 10.1007/s10029-010-0699-3. [DOI] [PubMed] [Google Scholar]
- 21.Goh BK, Wong AS, Tay KH, Hoe MN. Delayed presentation of a patient with a ruptured diaphragm complicated by gastric incarceration and perforation after apparently minor blunttrauma. Canad J Emerg Med. 2004;6(4):277–280. doi: 10.1017/s148180350000926x. [DOI] [PubMed] [Google Scholar]
- 22.Ravinder Kaur, Anuj Prabhakar1, Suman Kochhar1, Usha Dalal2 Blunt traumatic diaphragmatic hernia: pictorial review of CT signs. Indian J Rad Imaging / August 2015 / Vol 25 / Issue 3 [DOI] [PMC free article] [PubMed]
- 23.Kelly J, Condon E, Kirwan W, Redmond H. Post-traumatic tension faecopneumothorax in a young male: case report. World J Emerg Surg. 2008;3:20. doi: 10.1186/1749-7922-3-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nayak HK, Maurya G, Kapoor N, Kar P. Delayed presentation of congenital diaphragmatic hernia presenting with intrathoracic gastric volvulus: a case report and review. BMJ Case Rep. 2012 Nov 28;2012. pii: bcr2012007332. [DOI] [PMC free article] [PubMed]
- 25.Kitano Y, Lally KP, Lally PA. Congenital diaphragmatic hernia study group: late presenting congenital diaphragmatic hernia. J Pediatr Surg. 2005;40:1839–1843. doi: 10.1016/j.jpedsurg.2005.08.020. [DOI] [PubMed] [Google Scholar]
- 26.Baglaj M. Late-presenting congenital diaphragmatic hernia in children: a clinical spectrum. Pediatr Surg Int. 2004;20:658–669. doi: 10.1007/s00383-004-1269-5. [DOI] [PubMed] [Google Scholar]
- 27.Hosgor M, Karaca I, Karkiner A, Ucan B, Temir G, Erdag G, et al. Associated malformations in delayed presentation of congenital diaphragmatic hernia. J Pediatr Surg. 2004;39:1073–1076. doi: 10.1016/j.jpedsurg.2004.03.050. [DOI] [PubMed] [Google Scholar]
- 28.Elhalaby EA, Abo Sikeena MH. Delayed presentation of congenital diaphragmatic hernia. Pediatr Surg Int. 2002;18:480–485. doi: 10.1007/s00383-002-0743-1. [DOI] [PubMed] [Google Scholar]
- 29.Lawrence B, David S, Sigmund H, Barry S. The late-presenting pediatric bochdalek hernia: a 20-year review. J Ped Surg. 1988;23:735–39. doi: 10.1016/S0022-3468(88)80414-7. [DOI] [PubMed] [Google Scholar]
- 30.Joel AF, John L, Samuel E, James F, Louis MB. Diaphragmatic hernia masquerading as pneumothorax in two toddlers case report. Ann Emerg Med. 1993;22:1221–4. doi: 10.1016/S0196-0644(05)80995-3. [DOI] [PubMed] [Google Scholar]
- 31.Chao PH, Chuang JH, Lee SY, Huang HC. Acta Paediatr. 2011;100:425–428. doi: 10.1111/j.1651-2227.2010.02025.x. [DOI] [PubMed] [Google Scholar]
- 32.Kurniawan N, Verheyen L, Ceulemans Acute chest pain while exercising: a case report of Bochdalek hernia in an adolescent. J Acta Chir Belg. 2013;113(4):290–2. doi: 10.1080/00015458.2013.11680930. [DOI] [PubMed] [Google Scholar]
- 33.Ravinder Kaur, Anuj Prabhakar1, Suman Kochhar1, Usha Dalal2. Blunt traumatic diaphragmatic hernia: pictorial review of CT signs Indian Journal of Radiology and Imaging / August 2015 / Vol 25 / Issue 3 [DOI] [PMC free article] [PubMed]
- 34.Gander JW, Fisher JC, Gross ER, et al. Early recurrence of congenital diaphragmatic hernia is higher after thoracoscopic than open repair: a single institutional study. J Pediatr Surg. 2011;46(7):1303–1308. doi: 10.1016/j.jpedsurg.2010.11.048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lansdale N, Alam S, Losty PD, Jesudason EC. Neonatal endosurgical congenital diaphragmatic hernia repair: a systematic review and meta-analysis. Ann Surg. 2010;252(1):20–26. doi: 10.1097/SLA.0b013e3181dca0e8. [DOI] [PubMed] [Google Scholar]
- 36.Tsao K, Lally PA, Lally KP. Minimally invasive repair of congenital diaphragmatic hernia. J Pediatr Surg. 2011;46(6):1158–1164. doi: 10.1016/j.jpedsurg.2011.03.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Badillo A, Gingalewski C. Congenital diaphragmatic hernia: treatment and outcomes. Semin Perinatol. 2014;3(8):92–96. doi: 10.1053/j.semperi.2013.11.005. [DOI] [PubMed] [Google Scholar]
- 38.Mansour KA. Trauma to the diaphragm. Chest Surg Clin N Am. 1997;7(2):373–383. [PubMed] [Google Scholar]
- 39.Soper NJ, Teitelbaum EN. Laparoscopic paraesophageal hernia repair: current controversies. Surg Laparosc Endosc Percutan Tech. 2013;23(5):442–445. doi: 10.1097/SLE.0b013e3182a12680. [DOI] [PubMed] [Google Scholar]
- 40.Coccolini F, Agresta F, Bassi A, Catena F, Crovella F, Ferrara R, Gossetti F, Marchi D, Munegato G, Negro P, Piccoli M, Melotti G, Sartelli M, Schianodi Visconte M, Testini M, Bertoli P, Capponi MG, Lotti M, Manfredi R, Pisano M, Poiasina E, Poletti E, Ansaloni L. Italian Biological Prosthesis Work-Group (IBPWG): proposal for a decisional model in using biological prosthesis. World J Emerg Surg. 2012;7:34. doi: 10.1186/1749-7922-7-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Lu J, Wang B, Che X, Li X, Qiu G, He S, Fan L. Delayed traumatic diaphragmatic hernia: a case-series report and literature review. Medicine (Baltimore) 2016;95(32):e4362. doi: 10.1097/MD.0000000000004362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Manabu H, Harada M, Tsujimoto H, Nagata K, Ito N, Yamazaki K, Kanematsu K, Horiguchi H, Kajiwara Y, Hiraki S, Aosasa S, Yamamoto J, Hase K. Successful laparoscopic repair of an incarcerated Bochdalek hernia associated with increased intra-abdominal pressure during use of blow gun: A case report. Int J Surg Case Rep. 2016;23:131–3. [DOI] [PMC free article] [PubMed]
- 43.De la Cour CD, Teklay B. Acute post-partum presentation of Bochdalek hernia in a grown-up woman Ugeskr Laeger. 2016 Oct 31;178(44). [PubMed]
- 44.Razi K1, Light D2, Horgan L. Emergency repair of Morgagni hernia with partial gastric volvulus: our approach. J Surg Case Rep. 2016 Aug 31;2016(8). [DOI] [PMC free article] [PubMed]
- 45.Manson HJ, Goh YM, Goldsmith P, Scott P, Turner P. Congenital diaphragmatic hernia causing cardiac arrest in a 30-year-old woman. Ann R Coll Surg Engl. 2017;99(2):e75–e77. doi: 10.1308/rcsann.2016.0345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Massloom HS. Acute bowel obstruction in a giant recurrent right Bochdalek’s hernia: a report of complication on both sides of the diaphragm. N Am J Med Sci. 2016;8(6):252–5. doi: 10.4103/1947-2714.185036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Kumar, J. Morgagni hernia presenting as gastric outlet obstruction in an elderly male. Surg Case Rep. 2016 2016 Jul 18;2016(7). [DOI] [PMC free article] [PubMed]
- 48.Manipadam JM, Sebastian GM, Ambady V, Hariharan R. Perforated gastric gangrene without pneumothorax in an adult Bochdalek hernia due to volvulus. J Clin Diagn Res. 2016;10(4):D09–10. doi: 10.7860/JCDR/2016/18032.7552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Harada M, Tsujimoto H, Nagata K, Ito N, Yamazaki K, Kanematsu K, Horiguchi H, Kajiwara Y, Hiraki S, Aosasa S, Yamamoto J, Hase K. Successful laparoscopic repair of an incarcerated Bochdalek hernia associated with increased intra-abdominal pressure during use of blow gun: a case report. Int J Surg Case Rep. 2016;23:131–3. doi: 10.1016/j.ijscr.2016.03.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Siow SL1,2, Wong CM3,4, Hardin M5, Sohail M6. Successful laparoscopic management of combined traumatic diaphragmatic rupture and abdominal wall hernia: a case report. J Med Case Rep. 2016 Jan 18;10:11. doi: 10.1186/s13256-015-0780-8. [DOI] [PMC free article] [PubMed]
- 51.Andreev AL, Protsenko AV, Globin AV. Laparoscopic repair of a posttraumatic left-sided diaphragmatic hernia complicated by strangulation and colon obstruction. JSLS. 2010;14:410-3. doi: 10.4293/108680810X12924466006648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Bhatt NR, McMonagle M. Recurrence in a laparoscopically repaired traumatic diaphragmatic hernia: case report and literature review. Trauma Mon. 2016;21:e20421. doi: 10.5812/traumamon.20421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Abdullah M1, Stonelake P2. Tension pneumothorax due to perforated colon. BMJ Case Rep. 2016 May 31;2016. [DOI] [PMC free article] [PubMed]
- 54.Razi K, Light D2, Horgan L2. Emergency repair of Morgagni hernia with partial gastric volvulus: our approach. Journal of Surgical Case Reports, 2016 J Surg Case Rep. 2016 Aug 31;2016(8). [DOI] [PMC free article] [PubMed]
- 55.Wigley J, Noble F, King A. Thoracoabdominal herniation—but not as you know it. Ann R Coll Surg Engl. 2014;96:e1–2. doi: 10.1308/003588414X13814021679032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Atef M, Emna T. Bochdalek Hernia with gastric volvulus in an adult: common symptoms for an original diagnosis. Medicine (Baltimore) 2015;94:e2197. doi: 10.1097/MD.0000000000002197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Tokur M, Demiröz ŞM, Sayan M. Non-traumatic tension gastrothorax in a young lady. Ulus Travma Acil Cerrahi Derg. 2015;21(4):306–8. doi: 10.5505/tjtes.2015.71245. [DOI] [PubMed] [Google Scholar]
- 58.Topuz M, Ozek MC. Right ventricle collapse secondary to hepatothorax caused by diaphragm rupture due to blunt trauma. Ulus Travma Acil Cerrahi Derg. 2014;20:463–5. doi: 10.5505/tjtes.2014.27547. [DOI] [PubMed] [Google Scholar]
- 59.Haratake N, Yamazaki K, Shikada Y. Diaphragmatic hernia caused by heterotopic endometriosis in Chilaiditi syndrome: report of a case. Surg Today. 2015;45(9):1194–6. doi: 10.1007/s00595-014-1001-6. [DOI] [PubMed] [Google Scholar]
- 60.Gali BM, Bakari AA, Wadinga DW, Nganjiwa US. Missed diagnosis of a delayed diaphragmatic hernia as intestinal obstruction: a case report. Niger J Med. 2014;23(1):83–5. [PubMed] [Google Scholar]
- 61.Newman MJ1. A mistaken case of tension pneumothorax. BMJ Case Rep. 2014 May 16;2014. pii: bcr2013203435. [DOI] [PMC free article] [PubMed]
- 62.Tyagi S, Steele J, Patton B, Fukuhara S, Cooperman A, Wayne M. Laparoscopic repair of an intrapericardial diaphragmatic hernia. Ann Thorac Surg. 2014;97(1):332–3. doi: 10.1016/j.athoracsur.2013.04.127. [DOI] [PubMed] [Google Scholar]
- 63.Ota H, Kawai H, Matsuo T. Video-assisted minithoracotomy for blunt diaphragmatic rupture presenting as a delayed hemothorax. Ann Thorac Cardiovasc Surg. 2014;20(Suppl):911–4. doi: 10.5761/atcs.cr.13-00201. [DOI] [PubMed] [Google Scholar]
- 64.Safdar G, Slater R, Garner JP. Laparoscopically assisted repair of an acute traumatic diaphragmatic hernia. BMJ Case Rep. 2013 Jun 24;2013. [DOI] [PMC free article] [PubMed]
- 65.Sonthalia N, Ray S, Khanra D, Saha A,Maitra S, Talukdar A; Gastric volvulus through morgagni hernia: an easily overlooked emergency. J Emerg Med. 2013 [DOI] [PubMed]
- 66.Nayak HK, Maurya G, Kapoor N, Kar P. Delayed presentation of congenital diaphragmatic hernia presenting with intrathoracic gastric volvulus: a case report and review. BMJ Case Rep. 2012;28:2012. doi: 10.1136/bcr-2012-007332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Vernadakis S, Paul A, Kykalos S, Fouzas I, Kaiser GM, Sotiropoulos GC. Incarcerated diaphragmatic hernia after right hepatectomy for living donor liver transplantation: case report of an extremely rare late donor complication. Transplant Proc. 2012;44(9):2770–2. doi: 10.1016/j.transproceed.2012.09.014. [DOI] [PubMed] [Google Scholar]
- 68.Ngai I, Sheen JJ, Govindappagari S, Garry DJ. Bochdalek hernia in pregnancy. BMJ Case Rep. 2012;11:2012. doi: 10.1136/bcr-2012-006859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Elangovan A, Chacko J, Gadiyaram S, Moorthy R. Ra traumatic tension gastrothorax and pneumothorax. J Emerg Med. 2013;44(2):e279–80. doi: 10.1016/j.jemermed.2012.07.043. [DOI] [PubMed] [Google Scholar]
- 70.Kuppusamy A, Ramanathan G, Gurusamy J, Ramamoorthy B, Parasakthi K. Delayed diagnosis of traumatic diaphragmatic rupture with herniation of the liver: a case report. Ulus Travma Acil Cerrahi Derg. 2012;18(2):175–7. doi: 10.5505/tjtes.2012.79477. [DOI] [PubMed] [Google Scholar]
- 71.Okan I, Baş G, Ziyade S, Alimoğlu O, Eryılmaz R, Güzey D, Zilan A. Delayed presentation of posttraumatic diaphragmatic hernia. Ulus Travma Acil Cerrahi Derg. 2011;17(5):435–9. doi: 10.5505/tjtes.2011.89804. [DOI] [PubMed] [Google Scholar]
- 72.Baloyiannis I, Kouritas VK, Karagiannis K, Spyridakis M, Efthimiou M. Isolated right diaphragmatic rupture following blunt trauma. Gen Thorac Cardiovasc Surg. 2011;59(11):760–2. doi: 10.1007/s11748-010-0759-8. [DOI] [PubMed] [Google Scholar]
- 73.Vassileva CM, Shabosky J, Boley T, Hazelrigg S. Morgagni hernia presenting as a rigright middle lobe compression. Ann Thorac Cardiovasc Surg. 2012;18(1):79–81. doi: 10.5761/atcs.cr.11.01690. [DOI] [PubMed] [Google Scholar]
- 74.Agrafiotis AC, Kotzampassakis N, Boudaka W. Complicated right-sided Bochdalek hernia in an adult. Acta Chir Belg. 2011;111(3):171–3. doi: 10.1080/00015458.2011.11680730. [DOI] [PubMed] [Google Scholar]
- 75.Tan KK, Yan ZY, Vijayan A, Chiu MT. Management of diaphragmatic rupture from blunt trauma. Singap Med J. 2009;50(12):1150–3. [PubMed] [Google Scholar]
- 76.Akhtar K, Qurashi K, Rizvi A, Isla R. Emergency laparoscopic repair of an obstructed Bochdalek hernia in an adult. Br J Hosp Med (Lond) 2009;70(12):718–9. doi: 10.12968/hmed.2009.70.12.45511. [DOI] [PubMed] [Google Scholar]
- 77.Ozpolat B, Doğan OV, Yücel E. Delayed diaphragmatic hernia: an unusual complication of tube thoracostomy. Ulus Travma Acil Cerrahi Derg. 2009;15(6):617–8. [PubMed] [Google Scholar]
- 78.Altinkaya N, Parlakgümüş A, Koc Z, Ulusan S. Morgagni hernia: diagnosis with multidetector computed tomography and treatment. Hernia. 2010;14(3):277–81. doi: 10.1007/s10029-009-0608-9. [DOI] [PubMed] [Google Scholar]
- 79.Peer SM, Devaraddeppa PM, Buggi S. Traumatic diaphragmatic hernia—our experience. Int J Surg. 2009;7(6):547–9. doi: 10.1016/j.ijsu.2009.09.003. [DOI] [PubMed] [Google Scholar]
- 80.Sung HY, Cho SH, Sim SB, Kim JI, Cheung DY, Park SH, Han JY, Lee SM, Noh CH, Park YB, Jung SE, Lee SH, Choi KY. Congenital hemidiaphragmatic agenesis presenting as reversible mesenteroaxial gastric volvulus and diaphragmatic hernia: a case report. J Korean Med Sci. 2009;24(3):517–9. doi: 10.3346/jkms.2009.24.3.517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Ouazzani A, Guerin E, Capelluto E, Landolfo G, Roman A, Bruyns J, Cadiere GB. A laparoscopic approach to left diaphragmatic rupture after blunt trauma. Acta Chir Belg. 2009;109(2):228–31. doi: 10.1080/00015458.2009.11680410. [DOI] [PubMed] [Google Scholar]
- 82.Kavanagh DO, Ryan RS, Waldron R. Acta Chir Belg. Acute dyspnoea due to an incarcerated right-sided Bochdalek’s hernia. 2008 Sep-Oct;108(5):604–6. [DOI] [PubMed]
- 83.Hung YH, Chien YH, Yan SL, Chen MF. Adult Bochdalek hernia with bowel incarceration. J Chin Med Assoc. 2008;71(10):528–31. doi: 10.1016/S1726-4901(08)70162-X. [DOI] [PubMed] [Google Scholar]
- 84.Gourgiotis S, Rothkegel S, Germanos S. Combined diaphragmatic and urinary bladder rupture after minor motorcycle accident (report of a case and literature review) Ulus Travma Acil Cerrahi Derg. 2008;14(2):163–6. [PubMed] [Google Scholar]
- 85.Walchalk LR, Stanfield SC. Delayed presentation of traumatic diaphragmatic rupture. J Emerg Med. 2010;39(1):21–4. doi: 10.1016/j.jemermed.2007.09.044. [DOI] [PubMed] [Google Scholar]
- 86.Mohammadhosseini B, Shirani S. Incarcerated Bochdalek hernia in an adult. J Coll Physicians Surg Pak. 2008;18(4):239–41. [PubMed] [Google Scholar]
- 87.Boyce S, Burgul R, Pepin F, Shearer C. Late presentation of a diaphragmatic hernia following laparoscopic gastric banding. Obes Surg. 2008;18(11):1502–4. doi: 10.1007/s11695-008-9515-x. [DOI] [PubMed] [Google Scholar]
- 88.Tsuboi K, Omura N, Kashiwagi H, Kawasaki N, Suzuki Y, Yanaga K. Delayed traumatic diaphragmatic hernia after open splenectomy: report of a case. Surg Today. 2008;38(4):352–4. doi: 10.1007/s00595-007-3627-0. [DOI] [PubMed] [Google Scholar]
- 89.Vogelaar FJ, Adhin SK, Schuttevaer HM. Delayed intrathoracic gastric perforation after obesity surgery: a severe complication. Obes Surg. 2008;18(6):745–6. doi: 10.1007/s11695-007-9388-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Wu YS, Lin YY, Hsu CW, Chu SJ, Tsai SH. Massive ipsilateral pleural effusion caused by transdiaphragmatic intercostal hernia. Am J Emerg Med. 2008;26(2):252. doi: 10.1016/j.ajem.2007.04.018. [DOI] [PubMed] [Google Scholar]
- 91.Igai H, Yokomise H, Kumagai K, Yamashita S, Kawakita K, Kuroda Y. Delayed hepatothorax due to right-sided traumatic diaphragmatic rupture. Gen Thorac Cardiovasc Surg. 2007;55(10):434–6. doi: 10.1007/s11748-007-0158-y. [DOI] [PubMed] [Google Scholar]
- 92.Rifki Jai S, Bensardi F, Hizaz A, Chehab F, Khaiz D, Bouzidi A. A late post-traumatic diaphragmatic hernia revealed during pregnancy by post-partum respiratory distress. Arch Gynecol Obstet. 2007;276(3):295–8. doi: 10.1007/s00404-007-0347-z. [DOI] [PubMed] [Google Scholar]
- 93.Rout S, Foo FJ, Hayden JD, Guthrie A, Smith AM. Right-sided Bochdalek hernia obstructing in an adult: case report and review of the literature. Hernia. 2007;11(4):359–62. doi: 10.1007/s10029-007-0188-5. [DOI] [PubMed] [Google Scholar]
- 94.Campbell AS, O'Donnell ME, Lee J. Mediastinal shift secondary to a diaphragmatic hernia: a life-threatening combination. Hernia. 2007;11(4):377–9. doi: 10.1007/s10029-007-0202-y. [DOI] [PubMed] [Google Scholar]
- 95.Luu TD, Reddy VS, Miller DL, Force SD. Gastric rupture associated with diaphragmatic hernia during pregnancy. Ann Thorac Surg. 2006;82(5):1908–10. doi: 10.1016/j.athoracsur.2006.02.083. [DOI] [PubMed] [Google Scholar]
- 96.Iso Y, Sawada T, Rokkaku K, Furihata T, Shimoda M, Kita J, Kubota K. A case of symptomatic Morgagni’s hernia and a review of Morgagni’s hernia in Japan (263 reported cases) Hernia. 2006;10(6):521–4. doi: 10.1007/s10029-006-0123-1. [DOI] [PubMed] [Google Scholar]
- 97.Eglinton T, Coulter GN, Bagshaw P, Cross L. Diaphragmatic hernias complicating pregnancy. ANZ J Surg. 2006;76(7):553–7. doi: 10.1111/j.1445-2197.2006.03776.x. [DOI] [PubMed] [Google Scholar]
- 98.Barbetakis N, Efstathiou A, Vassiliadis M, Xenikakis T, Fessatidis Bochdaleck’s hernia complicating pregnancy: case report. World J Gastroenterol. 2006;12(15):2469–71. doi: 10.3748/wjg.v12.i15.2469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Barrett J, Satz W. Traumatic, pericardio-diaphragmatic rupture: an extremely rare cause of pericarditis. J Emerg Med. 2006;30(2):141–5. doi: 10.1016/j.jemermed.2005.04.017. [DOI] [PubMed] [Google Scholar]
- 100.Abboud B, Jaoude JB, Riachi M, Sleilaty G, Tabet G. Intrathoracic transverse colon and small bowel infarction in a patient with traumatic diaphragmatic hernia. Case report and review of the literature. J Med Liban. 2004;52(3):168–70. [PubMed] [Google Scholar]
- 101.Hsu YP, Chen RJ, Fang JF, Lin BC. Blunt diaphragmatic rupture in elderly patients. Hepatogastroenterology. 2005;52(66):1752–8. [PubMed] [Google Scholar]
- 102.Ransom P, Cornelius P. Stabbing chest pain: a case of intermittent diaphragmatic herniation. Emerg Med J. 2005;22(6):460–1. doi: 10.1136/emj.2003.012468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Tiberio GA, Portolani N, Coniglio A, Baiocchi GL, Vettoretto N, Giulini SM. Traumatic lesions of the diaphragm. Our experience in 33 cases and review of the literature. Acta Chir Belg. 2005;105(1):82–8. [PubMed] [Google Scholar]
- 104.Gupta V, Singhal R, Ansari MZ. Spontaneous rupture of the diaphragm. Eur J Emerg Med. 2005;12(1):43–4. doi: 10.1097/00063110-200502000-00013. [DOI] [PubMed] [Google Scholar]
- 105.Kara E, Kaya Y, Zeybek R, Coskun T, Yavuz C. A case of a diaphragmatic rupture complicated with lacerations of stomach and spleen caused by a violent cough presenting with mediastinal shift. Ann Acad Med Singapore. 2004;33(5):649–50. [PubMed] [Google Scholar]
- 106.Sirbu H, Busch T, Spillner J, Schachtrupp A, Autschbach R. Late bilateral diaphragmatic rupture: challenging diagnostic and surgical repair. Hernia. 2005;9(1):90–2. doi: 10.1007/s10029-004-0243-4. [DOI] [PubMed] [Google Scholar]
- 107.Dalton AM, Hodgson RS, Crossley C. Bochdalek hernia masquerading as a tension pneumothorax. Emerg Med J. 2004;21(3):393–4. doi: 10.1136/emj.2002.004697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Niwa T, Nakamura A, Kato T, Kutsuna T, Tonegawa K, Kawai A, Itoh M. An adult case of Bochdalek hernia complicated with hemothorax. Respiration. 2003;70(6):644–6. doi: 10.1159/000075213. [DOI] [PubMed] [Google Scholar]
- 109.Genc MR, Clancy TE, Ferzoco SJ, Norwitz E. Maternal congenital diaphragmatic hernia complicating pregnancy. Obstet Gynecol. 2003;102(5 Pt 2):1194–6. doi: 10.1016/s0029-7844(03)00680-x. [DOI] [PubMed] [Google Scholar]
- 110.Sato M, Minimally invasive diagnosis and treatment of traumatic rupture of the right hemidiaphragm with liver herniation. Jpn J Thorac Cardiovasc Surg. 2002 [DOI] [PubMed]
- 111.Guven H, Malazgirt Z, Dervisoglu A, Danaci M, Ozkan K. Morgagni hernia: rare presentations in elderly patients. Acta Chir Belg. 2002;102(4):266–9. doi: 10.1080/00015458.2002.11679311. [DOI] [PubMed] [Google Scholar]
- 112.Kanazawa A, Yoshioka Y, Inoi O, Murase J, Kinoshita H. Acute respiratory failure caused by an incarcerated right-sided adult bochdalek hernia: report of a case. Surg Today. 2002;32(9):812–5. doi: 10.1007/s005950200156. [DOI] [PubMed] [Google Scholar]
- 113.Fisichella PM, Perretta S, Di Stefano A, Di Carlo I, La Greca G, Russello D, Latteri F. Chronic liver herniation through a right Bochdalek hernia with acute onset in adulthood. Ann Ital Chir. 2001;72(6):703–5. [PubMed] [Google Scholar]
- 114.Carreño G, Sánchez R, Alonso RA, Galarraga MA, Moriyón C, Magarzo A, Bouzón F, Makdissi Z, Obregón RA. Laparoscopic repair of Bochdalek’s hernia with gastric volvulus. Surg Endosc. 2001;15(11):1359. doi: 10.1007/s004640040028. [DOI] [PubMed] [Google Scholar]
- 115.Prieto Nieto I, Pérez Robledo JP, Rosales Trelles V, De Miguel IR, Fernández Prieto A, Calvo Celada A. Gastric incarceration and perforation following posttraumatic diaphragmatic hernia. Acta Chir Belg. 2001;101(2):81–3. [PubMed] [Google Scholar]
- 116.Nursal TZ, Ugurlu M, Kologlu M, Hamaloglu E. Traumatic diaphragmatic hernias: a report of 26 cases. Hernia. 2001;5(1):25–9. doi: 10.1007/BF01576161. [DOI] [PubMed] [Google Scholar]
- 117.Bujanda L, Larrucea I, Ramos F, Muñoz C, Sánchez A, Fernández I. Bochdalek's hernia in adults. J Clin Gastroenterol. 2001;32(2):155–7. doi: 10.1097/00004836-200102000-00013. [DOI] [PubMed] [Google Scholar]
- 118.Pross M, Manger T, Mirow L, Wolff S, Lippert H. Laparoscopic management of a late-diagnosed major diaphragmatic rupture. J Laparoendosc Adv Surg Tech A. 2000;10(2):111–4. doi: 10.1089/lap.2000.10.111. [DOI] [PubMed] [Google Scholar]
- 119.Saito Y, Yamakawa Y, Niwa H, Kiriyama M, Fukai I, Kondo S, Fujii Y. Left diaphragmatic hernia complicated by perforation of an intrathoracic gastric ulcer into the aorta: report of a case. Surg Today. 2000;30(1):63–5. doi: 10.1007/PL00010049. [DOI] [PubMed] [Google Scholar]
- 120.De Waele JJ, Vermassen FE. Splenic herniation causing massive haemothorax after blunt trauma. J Accid Emerg Med. 1999;16(5):383–4. doi: 10.1136/emj.16.5.383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Colliver C, Oller DW, Rose G, Brewer D, 1 Traumatic intrapericardial diaphragmatic hernia diagnosed by echocardiography. J Trauma. 1997;42(1):115–7. doi: 10.1097/00005373-199701000-00021. [DOI] [PubMed] [Google Scholar]
- 122.Zantut LF, Machado MA, Volpe P, Poggetti RS, Birolini D. Bilateral diaphragmatic injury diagnosed by laparoscopy. Rev Paul Med. 1993;111(3):430–2. [PubMed] [Google Scholar]
- 123.Allen MS, Trastek VF, Deschamps C, Pairolero PC. Intrathoracic stomach. Presentation and results of operation. J Thorac Cardiovasc Surg. 1993;105(2):253–8. [PubMed] [Google Scholar]
- 124.Girzadas Jr1 DV, Fligner DJ. Delayed traumatic intrapericardial diaphragmatic hernia associated with cardiac tamponade. Ann Emerg Med. 1991;20(11):1246–7. [DOI] [PubMed]
- 125.Thomas S, Kapur B. Adult Bochdalek hernia—clinical features, management and results of treatment. Jpn J Surg. 1991;21(1):114–9. doi: 10.1007/BF02470876. [DOI] [PubMed] [Google Scholar]
- 126.Bush CA, Margulies R. Traumatic diaphragmatic hernia and intestinal obstruction due to penetrating trunk wounds. South Med J. 1990;83(11):1347–50. doi: 10.1097/00007611-199011000-00033. [DOI] [PubMed] [Google Scholar]
- 127.Feliciano DV, Cruse PA, Mattox KL, Bitondo CG, Burch JM, Noon GP, Beall AC., Jr Delayed diagnosis of injuries to the diaphragm after penetrating wounds. J Trauma. 1988;28(8):1135–44. doi: 10.1097/00005373-198808000-00005. [DOI] [PubMed] [Google Scholar]
- 128.Chidamdaram M, Eyres KS, Szabolcs Z, Ionescu MI. Management problems of coincident traumatic diaphragmatic hernia and myocardial infarction. Thorac Cardiovasc Surg. 1988;36(3):167–9. doi: 10.1055/s-2007-1020070. [DOI] [PubMed] [Google Scholar]
- 129.Symbas PN, Vlasis SE, Hatcher C., Jr Blunt and penetrating diaphragmatic injuries with or without herniation of organs into the chest. Ann Thorac Surg. 1986;42(2):158–62. doi: 10.1016/S0003-4975(10)60510-3. [DOI] [PubMed] [Google Scholar]
- 130.Saber WL, Moore EE, Hopeman AR, Aragon WE. Delayed presentation of traumatic diaphragmatic hernia. J Emerg Med. 1986;4(1):1–7. doi: 10.1016/0736-4679(86)90106-X. [DOI] [PubMed] [Google Scholar]
- 131.Gardezi SA, Chaudhry AM, Sial GA, Ahmad I, Rashid M, Yusuf A, Siddique S, Gardezi JR, Shafique T. Congenital diaphragmatic hernia in the adult. J Pak Med Assoc. 1986;36(1):16–20. [PubMed] [Google Scholar]
- 132.Brown GL, Richardson JD. Traumatic diaphragmatic hernia: a continuing challenge. Ann Thorac Surg. 1985;39(2):170–3. doi: 10.1016/S0003-4975(10)62559-3. [DOI] [PubMed] [Google Scholar]
- 133.Clark DE, Wiles CS, 3rd, Lim MK, Dunham CM, Rodriguez A. Traumatic rupture of the pericardium. Surgery. 1983;93(2):495–503. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data and materials are available in case of request.