

Abstract
Introduction:
Hyperacusis is defined as a reduction in tolerance to ordinary environmental sounds. Hyperacusis can occur in individuals of all age groups, making daily life difficult for the sufferers. Although there is no objective test to accurately diagnose hyperacusis, questionnaires are useful for the assessment of hyperacusis. The aim of this study was to explore the reduced sound tolerance in university students using a hyperacusis questionnaire (HQ).
Materials and Methods:
A total of 536 university students (300 females and 236 males) aged between 18 and 25 years, with a mean age of 21.34 ± 1.87 years, were assessed using an HQ developed by Khalfa. The mean total score of all the participants was 16.34 ± 7.91, and 5.78% of the participants had total scores indicating hyperacusis, where a majority of them were females.
Results:
Females had significantly higher scores than men in terms of both the total and the attentional and emotional dimensions. The scores of the participants who reported noise exposure or a decrease in their tolerance to noise were significantly higher than those of the other participants. Even among young adults, there was a group of participants suffering from some problems related to decreased tolerance to everyday sounds.
Discussion:
Although the Turkish translation of the HQ seems to be a reliable tool for evaluating hyperacusis in young adults, further work with various populations of different age groups is required to establish validity and to assess the psychometric qualities of the Turkish form.
Keywords: Hyperacusis, intolerance to sound, noise annoyance, questionnaires
Introduction
Hyperacusis is a condition that describes the discomfort experienced by a person toward ordinary environmental sounds.[1,2] Patients with hyperacusis have difficulty in tolerating sounds that are acceptable to most people with normal hearing.[3] The characteristics and severity of a situation can vary from person to person.[2] Some patients with hyperacusis report pain upon exposure to sound.[4] Some patients may find that certain sounds are more difficult to listen to than other sounds. In such patients with loudness hyperacusis, uncomfortable loudness level (ULL) − the intensity level where sound is perceived to be uncomfortably loud − may be abnormally lower than what would be expected for their audiometric thresholds.[5] Because of a wide range of symptoms, hyperacusis has been defined in several different ways in the literature including as auditory hypersensitivity, hyperresponsiveness to sound, phonophobia, and misophonia.[4] Although phonophobia (fear of sound) and misophonia (severely negative reactions to specific “trigger” sounds) are sometimes used in the place of hyperacusis, both these conditions describe aversive emotional responses to sounds.[2,4] Tyler et al. [4] focused on loudness, annoyance, fear, and pain as the different forms of hyperacusis and stated that patients with hyperacusis can experience these different reactions individually or in combination. In this study, we use the umbrella term “hyperacusis” to describe “decreased tolerance to ordinary environmental sounds,”[6,7] without making any distinction among the subtypes.
Possibly due to the differences in assessment procedures applied and lack of a clear definition for hyperacusis, prevalence rates reported in the literature vary.[4] Andersson et al.,[8] describing hyperacusis as an unusual intolerance to ordinary environmental sounds and using postal and internet questionnaires, found a prevalence of 8.6% in a sample of the general population. A study from Poland[9] investigated hyperacusis in a large sample of 10,349 individuals using a questionnaire by personal interview and found a prevalence of 15.2%. Unfortunately, this conference report[9] did not state how hyperacusis was defined. A Swedish study[10] focusing on the use of hearing protection and self-reported hearing-related symptoms to investigate tinnitus and hyperacusis among adolescents reported that 17.1% of the 1238 participants aged 13–19 years had noise sensitivity.
The mechanisms underlying hyperacusis have not yet been understood.[3] It is discussed that hyperacusis may be related to both an increased gain in the central auditory pathways and an increased anxiety or emotional response to sound.[11] Hyperacusis is often observed along with tinnitus and is considered as a precursor to tinnitus.[12] Some conditions involving the peripheral auditory system (e.g., noise-induced hearing loss, Bell’s palsy, and Méniére’s disease) are thought to be among the possible etiologies of hyperacusis.[2] However, in most cases, the cause of the condition remains unknown.[3] Hyperacusis can affect the quality of life interfering everyday activities. Individuals with hyperacusis may avoid any public and social setting, as they find sounds loud, annoying, or painful. In addition, hyperacusis may have an impact on a patient’s emotional well being, sleep, and concentration.[4,5]
Hyperacusis can affect individuals of all age groups, including children.[7,13] It was stated that the patients suffering from hyperacusis are relatively young as compared to the patients suffering from tinnitus or the individuals suffering from a noise-induced hearing loss.[14] Although hyperacusis is an important problem for individuals of all ages, it may have a great impact particularly on “emerging adults,” by limiting their activities and full participation in society. Emerging adulthood is a phase of life between 18 and 29 years of age.[15] In this period, individuals who start to become a fully independent person and explore their identity and various life possibilities can face more challenges and stressful situations than any other stage of their lives.[15,16] Decreased sound tolerance may contribute to the stress that the emerging adults have in their own lives. It is noted that the elimination of hyperacusis decreases general anxiety and stress.[13] On the contrary, emotional problems that are likely to occur in this period[17] may contribute to or cause hyperacusis. A relationship was shown to exist between hyperacusis and emotional problems, particularly anxiety and depression. Whether an increased sensitivity to sounds may evoke anxiety and depression or whether there would be common and cooperating mechanisms underlying hyperacusis and anxiety is yet under discussion.[4,18] In addition, studies noted that young adults may be at a risk of experiencing auditory problems such as hearing loss, tinnitus, or hyperacusis as a result of their health risk behaviors, for example, exposing themselves to loud levels of sounds and listening to loud music through headphones.[19,20,21] For the aforementioned reasons, an assessment of hyperacusis in the population of young adults is important. However, there is no standard and objective method for evaluating hyperacusis. Numerous patients with hyperacusis have normal audiometric thresholds.[14] Although measuring ULLs is thought to be an approach to help diagnose the condition,[2] it is important to point out that hyperacusis is a highly subjective phenomenon.[22] Listening to the patient’s description of the condition has been observed to be an important part of the initial evaluation. Questionnaires are among the tools that are used to obtain information about the characteristics and severity of the symptoms that can be related to hyperacusis. In addition, questionnaires are easy-to-use tools to reach young adults who may be unaware that their discomfort for sounds could be an indicator of a problem requiring a detailed examination. The aim of this study was to explore hyperacusis among young adults in Turkey. To achieve this purpose, two steps were followed. First, a “hyperacusis questionnaire” (HQ) was adapted to Turkish, and its reliability was tested. Second, the reduced sound tolerance and an increased sound sensitivity were assessed in university students using HQ.
Materials and Methods
Sample
Data were collected using the HQ distributed to a random sample of students from three faculties, where the researchers have conducted courses. A sample comprising 536 university students (300 females and 236 males) aged between 18 and 25 years was created, with a mean age of 21.34 ± 1.87 years. The questionnaires were administered during the classes and completed immediately.
The hyperacusis questionnaire
Khalfa et al.’s[1] HQ was used in this study to evaluate hearing sensitivity. The questionnaire is divided into two parts. The first part of the questionnaire includes three binary questions on general information including auditory disorders, noise exposure, and tolerance to noise. The second part of the questionnaire, which is the scored part of the questionnaire, includes fourteen self-rating items. Answers to each item are scored on a four-point Likert scale ranging from “no” (0 points), “yes, a little” (1 point), “yes, quite a lot” (2 points), to “yes a lot” (3 points). The mean total score ranging from 0 to 42 and obtaining a higher total score indicate greater sensitivity. A total score that is >28 is accepted as an indicator of strong auditory hypersensitivity. Items of the questionnaire can be interpreted by distributing them into the following three dimensions: attentional dimension, social dimension, and emotional dimension.[1]
Translation process
Prior to the distribution of questionnaires to the participants, the original questionnaire was translated into the target language using a forward–backward translation method. In the first step, two native speakers who are health professionals and competent in both languages independently translated the original questionnaire into Turkish. Thereafter, a meeting involving two translators, two researchers of the current study, and a psychological counselor was conducted to review and reconcile the work. The comprehensibility of the questionnaire was tested on 10 students who had not been included in the study group, and their opinions were used to prepare the final version of the questionnaire. In the second step, a bilingual translator, whose native language is Turkish, and who had no knowledge of the questionnaire back translated the target language work into the source language. The original and back-translated questionnaires were compared, and most of the items were found to be in good agreement. To determine the equivalence of language, the original and translated questionnaires were administered to 30 students who understand both the languages. The interval between the administering of both questionnaires was kept as 2 weeks. Correlation of the two sets of scores generated by the same students when the questionnaire was administered twice was calculated.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences version 17.0 software (SPSS Inc., Chicago, IL, United States). Pearson correlations and paired samples t-test were used to assess the language equivalence. The internal consistency reliability of the translated questionnaire was estimated by using Cronbach’s coefficient alpha. Chi-square test was used to compare the proportions. Differences between the mean values were investigated by independent samples t-test. The obtained values were considered significant when P < 0.05.
Results
No difference existed between the results obtained from the original and translated versions of the questionnaire (P > 0.05). Pearson’s correlation coefficient between the scores of English and Turkish versions of the questionnaire, which was given to the same participants, was 0.93 ranging from 0.80 to 0.98 among items, at the level 0.00. The respective Cronbach’s α values of the translated questionnaires were 0.70 for attentional dimension, 0.78 for social dimension, and 0.79 for emotional dimension. The mean total score for all the participants was 16.34 ± 7.91.
Figure 1 shows the distribution of the total scores obtained from the HQ. Examination of the participant’s distribution according to the mean total score of the study revealed that 52.1% of the participants had scores that were ≤16, whereas 47.9% of the participants had total scores that were >16. We also wanted to see the proportion of the participants obtaining a score ≥16 because some studies suggested a cutoff of 16 instead of the cutoff of 28, as will be mentioned in the discussion.[23] It was observed that 5.78% of the participants had total scores >28. Table 1 lists the mean total scores and the scores for each of the three dimensions according to sex. As shown in Table 1, the mean scores of females were significantly higher than those of males, both in terms of the total score of the questionnaire and in terms of the attentional and emotional dimensions. Among 31 participants with a total score that was >28, 67.7% were females. Of the 536 participants, 53.4% answered “yes” to the question “are you or have you been exposed to noise,” and 50% stated that they could tolerate a noise less effectively, as compared to what they could do a few years ago. Chi-square analysis revealed that a significantly greater proportion of females (55.3%) than males (43.2%) reported a decrease in their tolerance to noise-over-time (X 2 = 7.75, P < 0.01). Table 2 shows the mean scores of the participants obtained according to the responses to two questions, which are not included in the scoring of the questionnaire. As shown in Table 2, the participants who responded “yes” to the noise-related questions in the first part of the questionnaire had significantly higher mean scores than the other participants.
Figure 1.
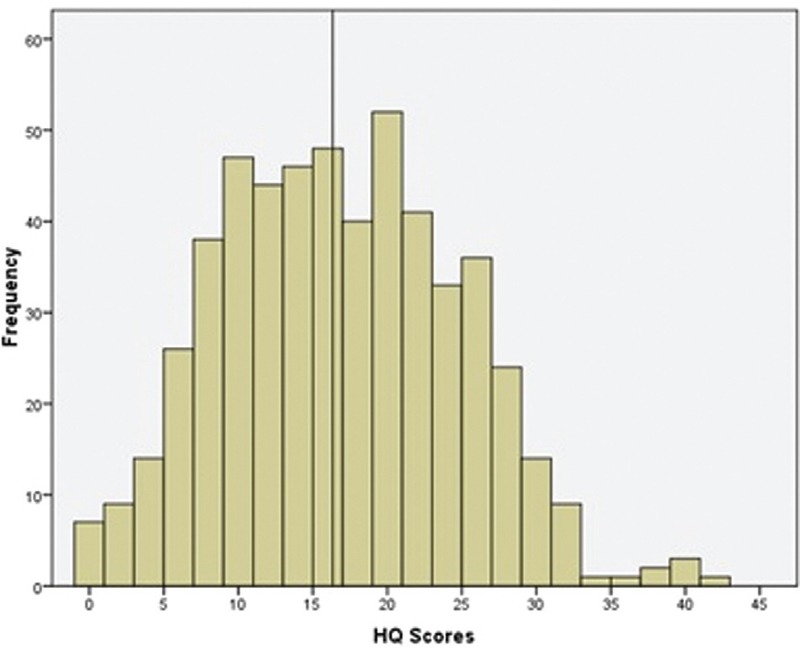
Distribution of HQ total scores (the mean score for the current study is presented with a line)
Table 1.
Means of total scores and scores for each dimension by sex
| Dimensions | Scores (mean ± SD) | P values | |
|---|---|---|---|
|
|
|||
| Females (n = 300) | Males (n = 236) | ||
| Attentional | 4.98 ± 2.36 | 4.23 ± 2.32 | <0.05 |
| Social | 6.04 ± 3.92 | 5.82 ± 3.73 | >0.05 |
| Emotional | 6.26 ± 2.99 | 5.44 ± 2.91 | <0.05 |
| Total | 17.11 ± 7.91 | 15.37 ± 7.75 | <0.05 |
Table 2.
Means of total scores by answers to noise-related yes/no questions in the questionnaire
| Scores (mean ± SD) | P values | ||
|---|---|---|---|
|
|
|||
| Yes | No | ||
| Are you or have you been exposed to noise? | 18.30 ± 7.67 (n = 286) | 14.10 ± 7.50 (n = 250) | <0.01 |
| Do you tolerate noise less well as compared to a few years ago? | 18.88 ± 7.43 (n = 268) | 13.80 ± 7.49) (n = 268) | <0.01 |
Discussion
In this study, approximately 6% of the participants obtained a total score that was >28 points. Khalfa et al.[1] suggested that an individual who had a total score that was >28 could be considered as hyperacusic. It was observed that previous studies present rather variable prevalence rates for hyperacusis ranging from 6 to 15%.[8,9] However, in a study that used the HQ, it was found that 1.1% of the participants met the critical value for hyperacusis.[22] Estimating the prevalence of hyperacusis with good precision is thought to be difficult because a universally accepted definition of the condition and a standard method to determine it do not exist.[4] Therefore, it appears difficult to interpret whether the rate of occurrence of hyperacusis in young adults obtained in the current study is high or low from the estimated prevalence of hyperacusis in young adults. To our knowledge, there is only one previous study investigating hyperacusis in a young population similar to ours, indicating a prevalence of 19.7 in the 16–19 age group.[10] Although Widén and Erlandsson[10] explored the presence of hyperacusis asking some questions regarding noise sensitivity and the use of earplugs as we did in this study, the questionnaires used in these two studies were different.
The mean total score was 16.34 ± 7.91. We can say that this value is quite close to the value of 15 ± 6.7 obtained in the study of Khalfa et al.[1] Shabana et al.[24] investigated the HQ scores in three groups, identifying the presence of hyperacusis based on the participants’ complaints of hypersensitivity to everyday environmental sounds. These groups included (1) individuals complaining of hyperacusis with tinnitus, (2) individuals complaining of hyperacusis without tinnitus, and (3) the control group. In their study, significant differences were found among the mean total scores of the three groups (hyperacusis group = 20 points, hyperacusis + tinnitus group = 28.9 points, and control group = 9.6 points). Shabana et al.[24] noted that the control group included individuals not complaining of hypersensitivity to sound or tinnitus. When we examined the scores of the participants who did not report a decrease in sound tolerance, assuming them to have no complaints of hypersensitivity to sound, we found that their mean score (=13.80) was significantly lower than that of the others (=18.88). The proportion of participants who reported noise exposure or a decrease in their tolerance to noises was significantly greater among the ones with a total score greater than the mean score in the current study (P < 0.05). This made us believe that the participants’ thoughts on the effect of noise on their lives were clearly reflected in the scores obtained from the questionnaire. It was observed that 47.9% of the participants had a total score that was greater than the mean score of the current investigation [Figure 1]. This result is in agreement with that of Fackrell et al.,[2] who found that the mean score of 47% of the participants was higher than that obtained in their study. In the study of Fackrell et al.,[2] it was observed that only 7% of the participants attained a criterion of 28 points, as suggested by Khalfa et al.[1] for the determination of hyperacusis. In spite of the similarity to our results, where 5.78% of the participants were assessed to be hyperacusic, it should be noted that Fackrell et al.[2] used an HQ to evaluate the participants suffering from tinnitus. Although we did not question whether the participants suffered from tinnitus, two participants reported “ringing in their ears” when they were asked in the first part of the questionnaire if they ever had hearing problems. Considering that hyperacusis is more prevalent among individuals with tinnitus,[25] the rate of occurrence of hyperacusis in our participants may be thought to be relatively high as compared to the results of studies conducted on tinnitus patients.[2,23,26] Only two participants’ suffering from hyperacusis in our study, however, should be interpreted with caution, because tinnitus was not questioned specifically.
We saw that the mean total score for the participants who reported a decrease in their tolerance to noises (according to non-scored questions) was approximately 19 [Table 2]. This made us think that there may be potential hyperacusis sufferers among the participants scoring <28 on the HQ. Critical value of 28 for the HQ score for classifying hyperacusis has been questioned by several researchers.[18,22,23,26] As it is seen in Shabana et al.’s[24] study, the mean total HQ score of the hyperacusis group was 20. Meeus et al.[26] stated that 28 was too high because the majority of the patients with hyperacusis complaints in their study scored lower than 28 on the HQ. Fioretti et al.[23] using the HQ to measure sensitivity to sounds in individuals suffering from tinnitus suggested a cutoff of 16. Similarly, Jüris et al. [18] proposed that the cutoff for the Swedish version of the HQ should be lowered.
A greater proportion of females than males reported that they experienced a decrease in their tolerance to sound with time. In addition, females had significantly higher scores in terms of both the total scores and the attentional and emotional dimensions than males had. This result was in good agreement with the findings of Khalfa et al.,[1] who reported that females had higher total, emotional, and attentional scores. Shabana et al.[24] found a gender effect similar to our results only in the emotional scores. This can be interpreted in two ways, as Khalfa et al. stated. First, females could be more vulnerable to sounds. Or second, they could express their discomfort more readily than males.[1] It was reported that high levels of emotional exhaustion make females more sensitive to sounds. For this reason, the importance of assessing emotional exhaustion for the correct diagnosis of hyperacusis is emphasized upon, particularly in women.[27] In addition, the role of hormone-related variability in sensory processing in women is discussed among the possible causes of hyperacusis with unknown etiology.[28] Women may be more sensitive to sounds and experience more emotional or auditory distress in association with hormone-related variability or changes in emotional state. Consequently, women may experience more threats from sounds and focus their attention on the negative effects of noise, which in turn may lead to hyperacusis.
Hyperacusis is a condition that can be extremely distressing and has a negative impact on patients’ lives. Individuals with decreased sound tolerance may experience social, attentional, or emotional problems due to some sounds, and they have to take appropriate measures to avoid exposure to noisy environments. Given that this condition is subjective, the patients with hyperacusis often suffer from a lack of understanding from others.[5] In addition, young patients with decreased sound tolerance may not be able to identify the fact that this is a medical condition that requires investigation. An important finding of this study is that although the participants reported a reduction in their tolerance to sounds or obtained a score indicating this, none of the participants took the problem too seriously to search for a solution to their annoyance. Besides, the results show that women exhibit a greater tendency to experience attentional and emotional problems related to reduced tolerance to sounds. After language adaptation of the questionnaire, it was found that the Turkish translation of the HQ was conceptually equivalent to the original and had good level of reliability (r = 0.93, α ≥ 0.70). However, the participants were healthy university students within a narrow age range. For this reason, although the findings support the reliability of the questionnaire, further testing with various populations of different ages is needed to establish the validity and to assess the psychometric qualities of the Turkish form of the HQ. Questionnaires such as the HQ make it possible to reach a large number of people and to detect the presence of experiences related to hyperacusis. In conclusion, it can be said that even among young adults, there exists a group of participants who exhibit some problems that may be related to decreased tolerance to everyday sounds. In addition, a gender difference is evident in the findings showing that the HQ scores of females were higher than those of males. Investigation of sound sensitivity and its consequences via the HQ may help to determine the need for a detailed interview and to diagnose the presence of hyperacusis as early as possible. This is especially important for emerging adults, who are in a transitional phase of their lives, because hyperacusis may hinder their ability to overcome challenges they face in this phase of life. Identifying hyperacusis early and providing required support can help reduce the long-term impact of hyperacusis on emerging adults’ lives.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Khalfa S, Dubai S, Veuillet E, Perez DF, Jouvent R, Collet L. Psychometric normalization of a hyperacusis questionnaire. ORL J Otorhinolaryngol Relat Spec. 2002;64:436–42. doi: 10.1159/000067570. [DOI] [PubMed] [Google Scholar]
- 2.Fackrell K, Fearnley C, Hoare DJ, Sereda M. Hyperacusis questionnaire as a tool for measuring hypersensitivity to sound in a tinnitus research population. Biomed Res Int. 2015;2015:290425. doi: 10.1155/2015/290425. doi: 10.1155/2015/290425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Katzenell U, Segal S. Hyperacusis: Review and clinical guidelines. Otol Neurotol. 2001;22:321–7. doi: 10.1097/00129492-200105000-00009. [DOI] [PubMed] [Google Scholar]
- 4.Tyler RS, Pienkowski M, Roncancio ER, Jun HJ, Brozoski T, Dauman N, et al. A review of hyperacusis and future directions: Part I. Definitions and manifestations. Am J Audiol. 2014;23:402–19. doi: 10.1044/2014_AJA-14-0010. [DOI] [PubMed] [Google Scholar]
- 5.Pienkowski M, Tyler RS, Roncancio ER, Jun HJ, Brozoski T, Dauman N, et al. A review of hyperacusis and future directions: Part II. Measurement, mechanisms, and treatment. Am J Audiol. 2014;23:420–36. doi: 10.1044/2014_AJA-13-0037. doi: 10.1044/2014_AJA- 13-0037. [DOI] [PubMed] [Google Scholar]
- 6.Vernon JA. Pathophysiology of tinnitus: A special case − Hyperacusis and a proposed treatment. Am J Otol. 1987;8:201–2. [PubMed] [Google Scholar]
- 7.Hall AJ, Humphriss R, Baguley DM, Parker M, Steer CD. Prevalence and risk factors for reduced sound tolerance (hyperacusis) in children. Int J Audiol. 2016;55:135–41. doi: 10.3109/14992027.2015.1092055. [DOI] [PubMed] [Google Scholar]
- 8.Andersson G, Lindvall N, Hursti T, Carlbring P. Hypersensitivity to sound (hyperacusis): A prevalence study conducted via the Internet and post. Int J Audiol. 2002;41:545–54. doi: 10.3109/14992020209056075. [DOI] [PubMed] [Google Scholar]
- 9.Fabijanska A, Rogowski M, Bartnik G, Skarzynski H. Epidemiology of tinnitus and hyperacusis in Poland. In: Hazell J, editor. Proceedings of the 6th International Tinnitus Seminar. London, UK: The Tinnitus and Hyperacusis Centre; 1999. pp. 569–71. [Google Scholar]
- 10.Widén SE, Erlandsson SI. Self-reported tinnitus and noise sensitivity among adolescents in Sweden. Noise Health. 2004;7:29–40. [PubMed] [Google Scholar]
- 11.Aazh H, McFerran D, Salvi R, Prasher D, Jastreboff M, Jastreboff P. Insights from the first international conference on hyperacusis: Causes, evaluation, diagnosis and treatment. Noise Health. 2014;16:123–6. doi: 10.4103/1463-1741.132100. [DOI] [PubMed] [Google Scholar]
- 12.Jastreboff PJ, Hazell JW. A neurophysiological approach to tinnitus: Clinical implications. Br J Audiol. 1993;27:7–27. doi: 10.3109/03005369309077884. [DOI] [PubMed] [Google Scholar]
- 13.Jastreboff PJ, Jastreboff MM. Decreased sound tolerance. In: Snow JB, editor. Tinnitus: Theory and Management. USA: BC Decker Inc; 2004. pp. 8–15. [Google Scholar]
- 14.Anari M, Axelsson A, Eliasson A, Magnusson L. Hypersensitivity to sound − Questionnaire data, audiometry and classification. Scand Audiol. 1999;28:219–30. doi: 10.1080/010503999424653. [DOI] [PubMed] [Google Scholar]
- 15.Arnett JJ. Emerging adulthood: A theory of development from the late teens through the twenties. Am Psychol. 2000;55:469–80. [PubMed] [Google Scholar]
- 16.Riggs SA, Han G. Predictors of anxiety and depression in emerging adulthood. J Adult Dev. 2009;16:39–52. [Google Scholar]
- 17.Lisznyai S, Vida K, Némethb M, Benczúr Z. Risk factors for depression in the emerging adulthood. Eur J Counsel Psychol. 2014;3:54–68. [Google Scholar]
- 18.Jüris L, Ekselius L, Andersson G, Larsen HC. The hyperacusis questionnaire, loudness discomfort levels, and the hospital anxiety and depression scale: A cross-sectional study. Hear Balance Commun. 2013;11:72–9. doi: 10.3109/21695717.2013.780409. [Google Scholar]
- 19.Chung JH, Des Roches CM, Meunier J, Eavey RD. Evaluation of noise-induced hearing loss in young people using a web-based survey technique. Pediatrics. 2005;115:861–7. doi: 10.1542/peds.2004-0173. [DOI] [PubMed] [Google Scholar]
- 20.Maria A, Zocoli F, Morata TC, Marques JM, Corteletti LJ. Brazilian young adults and noise: Attitudes, habits, and audiological characteristics. Int J Audiol. 2009;48:692–9. doi: 10.1080/14992020902971331. [DOI] [PubMed] [Google Scholar]
- 21.Widen SE, Holmes AE, Johnson T, Bohlin M, Erlandsson SI. Hearing, use of hearing protection, and attitudes towards noise among young American adults. Int J Audiol. 2009;48:537–45. doi: 10.1080/14992020902894541. [DOI] [PubMed] [Google Scholar]
- 22.Wallén MB, Hasson D, Theorell T, Canlon B. The correlation between the hyperacusis questionnaire and uncomfortable loudness levels is dependent on emotional exhaustion. Int J Audiol. 2012;51:722–9. doi: 10.3109/14992027.2012.695874. doi: 10.3109/14992027.2012.695874. [DOI] [PubMed] [Google Scholar]
- 23.Fioretti A, Tortorella F, Masedu F, Valenti M, Fusetti M, Pavaci S. Validity of the Italian version of Khalfa’s questionnaire on hyperacusis. Acta Otorhinolaryngol Ital. 2015;35:110–5. [PMC free article] [PubMed] [Google Scholar]
- 24.Shabana MI, Selim MH, Refaie A, Dessouky TM, Soliman RY. Assessment of hyperacusis in Egyptian patients: Evaluation of the Arabic version of the Khalfa questionnaire. Audiol Med. 2011;9:127–34. [Google Scholar]
- 25.Baguley DM. Hyperacusis. J R Soc Med. 2003;96:582–5. doi: 10.1258/jrsm.96.12.582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Meeus OM, Spaepen M, Ridder DD, Heyning PH. Correlation between hyperacusis measurements in daily ENT practice. Int J Audiol. 2010;49:7–13. doi: 10.3109/14992020903160868. [DOI] [PubMed] [Google Scholar]
- 27.Hasson D, Theorell T, Bergquist J, Canlon B. Acute stress induces hyperacusis in women with high levels of emotional exhaustion. PLoS One. 2013;8 doi: 10.1371/journal.pone.0052945. doi: 10.1371/journal.pone.0052945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Baribeau J. Hormonal related variability in auditory dysfunctions. Annu Rev Cyberther Telemed. 2007;5:107–13. [Google Scholar]