

Abstract
The Nashville Area Metropolitan Planning Organization (MPO) is among the first MPOs in the United States to recognize the interplay of transportation and public health, particularly regarding physical activity, air pollution, and traffic crashes. The Nashville MPO has taken a multifaceted approach to simultaneously improve the transportation system, quality of life, and health status of the region’s population. The purpose of this paper is to describe the multiple programs and projects that the MPO has undertaken to this end, so that other cities might learn from Nashville’s example.
The MPO’s strategy comprised six processes. First, the MPO conducted the Regional Bicycle and Pedestrian Study in 2009 and 2014 that established priority issues to be addressed by bicycle and pedestrian projects in Regional Transportation Plans. Second, the MPO responded to public opinion by adopting new transportation policies in the 2035 and 2040 Regional Transportation Plans, including increasing bicycle and pedestrian options and expanding public transit. Third, the MPO created scoring criteria for proposed roadway projects that prioritized health impacts. Fourth, the MPO reserved funding for projects selected under the new criteria and established a new funding program, the Active Transportation Program. Fifth, the MPO conducted the Middle Tennessee Transportation and Health Study, one of the first regional studies in the nation linking transportation and health. Finally, the MPO implemented the Integrated Transport and Health Impact Model which predicts and monetizes population-level health impacts of shifting the population towards active transportation modes.
Recent inventories of bicycle and pedestrian infrastructure suggest these interrelated processes are increasing opportunities for walking, bicycling, and public transit use in the region. Further, each of these projects has contributed to a growing appreciation in the region of the links between transportation and health, and continued evaluation efforts can determine if transportation behaviors and health outcomes are changing.
1.0 Introduction
The Nashville Area Metropolitan Planning Organization (MPO) is the federally-designated regional transportation planning agency for 1.5 million people in a seven-county region around Nashville, Tennessee (1). The MPO performs strategic planning for the region’s multi-modal transportation system and serves as a forum for collaboration among local communities and state leaders to allocate federal transportation dollars for transportation projects and programs. The MPO works with its members, which include local governments, public transit agencies, and the Tennessee Department of Transportation, to identify likely regional transportation needs at least two decades in the future (as required by federal law), and then allocate funding for projects to address these needs. Through transportation planning, the Nashville Area MPO aims to positively impact public and environmental health while providing access and mobility for the people who live and work in the region.
The Nashville region faces several important transportation and health problems. Nashville is among the most congested large US cities, with commuters experiencing 45 hours of annual traffic delay on average (2). Nashville is the capital of Tennessee, which has the second highest prevalence of adult inactivity among US states, with 62% of adults failing to meet aerobic physical activity guidelines (3). Additionally, many adult Tennessee residents are overweight (37%, ranked third among states) or obese (29%, ranked 15th among states) (3), which increases the risk for several chronic diseases. The Nashville Area MPO recognized the potential to address adverse transportation and health outcomes created by traditional transportation planning. The purpose of this paper is to describe the efforts the MPO has undertaken to this end.
The MPO’s approach to improve transportation and health in the region consisted of six actions that produced data or established policies and procedures that prioritized public health impacts in transportation decision making. Integral to the approaches were significant public engagement to inform both MPO staff and policy makers that interest in and demand for walking and bicycling facilities was wide-spread. Specifically, the MPO:
Conducted a Regional Bicycle and Pedestrian Study in 2009 and 2014 that resulted in a prioritized list of bicycle and pedestrian projects in the MPO region
Responded to public opinion by adopting three guiding transportation policies in the 2035 and 2040 Regional Transportation Plans
Created scoring criteria for roadway projects as part of the 2035 and 2040 Regional Transportation Plans that prioritized health and complete streets components (4)
Reserved funding for projects selected under the new scoring criteria and established an Active Transportation Program to fund additional bicycle and pedestrian projects and programs
Conducted the Middle Tennessee Transportation and Health Study, one of the first regional studies in the nation about the relationship between transportation and health
Implemented the Integrated Transport and Health Impact Model which estimates and monetizes population-level health impacts of shifting transportation trips from motorized personal vehicles to active transportation modes.
This paper provides a description of each of the six actions so that other transportation or public health organizations interested in pursuing similar goals can learn from Nashville’s experience. Each action is described sequentially in section 2, but in practice, many actions were done simultaneously.
2.0 Description of Components
2.1 Conducting a Regional Bicycle and Pedestrian Study
The Regional Bicycle and Pedestrian Study (RBPS) was first conducted in 2009 to establish a strategic vision for improving walking and bicycling opportunities in the greater Nashville region. A detailed explanation of the RBPS is publicly available (5). The study was a collection of projects that together shared four objectives, including creating an inventory of existing bicycle and pedestrian facilities; informing the public about the health and transportation benefits of improved walking and bicycling infrastructure connectivity; guiding development of a process to select bicycle and pedestrian projects for the MPO’s regional transportation plans; and providing guidance on future engineering, education, enforcement, encouragement, and evaluation activities around walking and bicycling safety. The 2009 and 2014 editions of the study were led by the MPO’s Bicycle and Pedestrian Advisory committee, which was first convened in 2008 and comprised of stakeholders from bicycle and pedestrian non-profit organizations, local and state governments, transit agencies, law enforcement, medical colleges, public schools and others.
The RPBS began with an inventory of bicycle and pedestrian facilities on collector roads, arterial roads, and greenways to provide data for the five projects of the RPBS, which are presented in Table 1. The results of the five projects were ranked for importance by the bicycle and pedestrian committee and used to create a 100-point scoring system that identified the locations in the region that were the most important priorities for expanding bicycle and pedestrian infrastructure. This score was also added to project proposals submitted to the MPO for consideration in the 2035 and 2040 Regional Transportation Plans so that projects that provided bicycle and pedestrian facilities to Health Priority Areas (Table 1) were ranked appropriately.
Table 1.
Components of the 2009 and 2014 Regional Bicycle and Pedestrian Studies, Nashville Area MPO
| Project | Description | Results |
|---|---|---|
| Bicycle/Pedestrian Latent Demand Model | Uses parcel-level information on housing, land use, employment, and destination proximity to predict the number of bicycling and walking trips that might be expected if walking and bicycling infrastructure were already in place | Identified parts of the region that might produce the most users for bicycle and pedestrian infrastructure |
| Bicycle/Pedestrian Level of Service | Based on the Transportation Research
Board’s 2010 Highway Capacity Manual (3) Considers multiple factors such as shoulder width, traffic volume, and separation from vehicles to provide an index of pedestrian and bicyclist comfort for a given corridor or street segment Assigns a score of A (best) through F (worst) |
Approximately two-thirds of arterials and
collectors scored at least a C Identified corridors that are not appealing to bicyclists and pedestrians |
| Health Priority Areas | Four demographic characteristics were shown to
be associated with poor health: low income, high unemployment, age
>65 years, and lack of car ownership Areas with three or more of the above factors were classified as having high health needs and were priorities for healthy transportation infrastructure |
Identified areas of the city with demographics that suggest poor population health |
| Dangerous Corridors | Created a map all recorded pedestrian and bicycle crashes in the area | Identified areas that would most benefit from safety improvements |
| Congested Corridors | Classified vehicle corridors according to volume to capacity ratios | Identified corridors that would most benefit from shifting mode share away from personal automobiles |
While conducting the RPBS, the committee and MPO staff were unable to find publicly-available health data at a geographic scale smaller than a county. This forced them rely on demographics to identify areas that likely suffered from poorer health than other areas in the region (Table 1). The lack of local health data inspired the 2012 Middle Tennessee Transportation and Health Study (see section 2.5), the results of which were combined with census data to update Health Priority Areas in the 2014 edition of the RPBS.
2.2 Shifting Policy
After the 2009 Regional Bicycle and Pedestrian Study, the MPO conducted a telephone-based transportation opinion survey among 1,100 randomly-selected households in the region. Participants were slightly older than the general population of the Nashville-Davidson Metropolitan Statistical Area (median age: 50 years in the survey, 36 years in the 2010 US Census (6)). One of the most striking results was that residents of the seven-county MPO region ranked lack of options for public transit, walking, and bicycling as the most important transportation problems in greater Nashville, while lack of sufficient roads was the least important transportation problem. Engaging public opinion is important in transportation planning and may be helpful in demonstrating to decision makers the desire for transportation choices. As a result, the MPO publicly shifted its stated policy focus towards greater support for public transit, walking and bicycling, and existing roadway preservation over new road construction, as expressed in the guiding principles and goals in the 2035 and 2040 regional plans (7, 8). The shift in policy was approved by the MPO executive committee and included extensive public input, which is explained further in section 4.3. By aligning its policies to the desires of the people of greater Nashville, the MPO demonstrated that it listened and responded to the transportation opinions of its constituents. The official shift in policy priorities was also important because it provided justification for prioritizing projects and programs that focused on these priority areas.
2.3 Creating Scoring Criteria
In the United States, MPOs are not required to use a particular method or set of criteria to select projects for construction. As such, they have used a broad range of methods to score and select proposed projects for construction (9). In 2010, while developing the 2035 regional transportation plan, the Nashville Area MPO was among the first to incorporate quantitative measures of potential health impact into this process. The MPO began with eight broad-reaching transportation categories, ranked from most to least important by the MPO’s staff and technical advisory committee. Based primarily on the technical committee rankings, each category was assigned a weight and thus contributed a fixed number of points to a 100-point project scoring scale (Table 2). Of the eight categories, five (quality growth, multi-modal options, road congestion management, safety and security, and health and environment) contained explicit provisions for non-motorized transportation, public transit, complete streets components, or dense/walkable design. These five categories accounted for 60 of 100 points for projects in the 2035 plan. After updating the scores for the 2040 plan, the five categories above constituted 80 of 100 possible points, which has dramatically raised the profile of projects that address health-oriented transportation and planning elements. Before the new scoring criteria were used, approximately 2% of funded projects contained healthy transportation and planning elements, but after the new scores were adopted, 67% (2035 plan) and 77% (2040 plan) of funded projects contained these elements.
Table 2.
Project scoring criteria, and selected health-related sub-criteria from the 2035 and 2040 regional transportation plans, Nashville Area Metropolitan Planning Organization
| Points per category | ||
|---|---|---|
| 2035 Plan | 2040 Plan | |
| 1. System preservation and enhancement | 15 | 10 |
| 2. Quality growth, sustainable development, and economic prosperity | 15 | 15 |
| Project improves accessibility/connection to residential population | ||
| Project improves accessibility/connection to existing jobs | ||
| Project incorporates streetscaping/enhancements | ||
| 3. Multi-modal options | 15 | 15 |
| Project includes sidewalk improvements | ||
| Project includes bicycle facility improvements | ||
| Project includes multi-modal treatments (cross-walks, shelters, etc) | ||
| 4. Congestion Management | 10 | 15 |
| Project addresses corridor congestion | ||
| Project provides additional non-motorized mode capacity | ||
| Project improves transit capacity | ||
| 5. Safety and Security | 10 | 20 |
| Primary project purpose is to improve safety | ||
| Project is on local/state high crash corridor designation | ||
| Project addresses specific location with high crash prevalence | ||
| 6. Freight and goods movement | 10 | 5 |
| 7. Health and environment | 10 | 15 |
| Project located in high health impact area | ||
| Project provides alt. transportation choices for underserved groups | ||
| Project provides multi-modal options near schools | ||
| 8. Project history | 15 | 5 |
|
| ||
| Total points: | 100 | 100 |
2.4 Allocating Funding
In response to the heightened importance of multi-modal and complete streets transportation projects outlined previously (section 2.3), the MPO needed to ensure that funds would be available to cover this diverse set of projects. To this end, the MPO had two points of emphasis: first, it reserved 70% of its largest revenue source, the Surface Transportation Program funding from the US Department of Transportation (10), to fund the Complete Streets projects selected under the new roadway scoring criteria detailed in section 2.3. In addition, the MPO reserved 15% of Surface Transportation Program funds for a newly-created Active Transportation Program for bicycle-and pedestrian-specific infrastructure and programs. These projects include facilities such as greenways or sidewalks that were not included in a roadway project proposal, and non-infrastructure needs related to education, encouragement, and enforcement activities for bicycle and pedestrian travel (e.g. community classes on bicycle and pedestrian safety or walking to school programs). By comparison, in 2014, an estimated 3.0% of the $10.1 billion in Surface Transportation Program funding in the United States was spent on walking and bicycling facilities (11). Reserving 15% of the Nashville Area MPO Surface Transportation Program funding for active transportation projects in addition to utilizing 70% for complete streets projects represents a significant commitment to walking and bicycling by the Nashville Area MPO.
2.5 Measuring Health
When developing the 2035 Regional Transportation Plan, the MPO was not able to obtain publicly-available information on health disparities and chronic disease prevalence at a geographic scale smaller than a county. Such small-scale health data are necessary if individual road projects are to be prioritized by potential impact to local health. Therefore, in 2012 the MPO conducted the Middle Tennessee Transportation and Health Study (MTTHS). A report of the methods and results of the MTTHS are available from the MPO’s website (12) and are summarized briefly here. Modeled after the National Household Travel Survey (13), the MTTHS collected transportation data for approximately 5,000 households, 11,000 individuals, 9,000 vehicles, and 40,000 trips. In addition to travel data, all respondents answered six health questions related to diet, physical activity, sitting time, height and weight, and general health status (Table 3). A 10% subsample of adult respondents was recruited into an expanded health sub-study that included four days of tracking physical activity through accelerometer and GPS measurements, in addition to a food diary and expanded health questionnaire.
Table 3.
Health questions for all respondents, Middle Tennessee Transportation and Health Study, 2012
| General Health Question Text | Response Options |
|---|---|
| During the last 7 days, how much time did you usually spend sitting on a weekday? (Please report in hours; for example: 8.5 hours) | Number of hours |
|
| |
| Which of the following statements best describes how physically active you are in a typical week. | • I rarely or never do any physical
activity • I do some light or moderate physical activities • I do some vigorous physical activities |
|
| |
| In general, how healthy is your overall
diet? Would you say that, in general, your health is: |
• Excellent • very good • good • fair • poor |
|
| |
| About how much do you weigh without
shoes? About how tall are you without shoes? |
Open ended |
For the six health questions asked of all respondents, residents of greater Nashville reported an average of 448 minutes of weekday sitting time, and over half (55%) reported doing “some light or moderate physical activities” in a given week. Nearly 70% of respondents reported either very good (32%) or good (37%) diet quality; a similar distribution was found for general health status. The average BMI for adults ≥20 years was in the overweight category at 27.1 kg/m2, and over half of respondents reported a BMI that was classified as overweight (34%) or obese (24%).
The results of the MTTHS largely confirm previous work in this region. For example, the 2012 Behavioral Risk Factor Surveillance System reports that 29% of adults in the 14-county metropolitan statistical area were obese, which is similar, but slightly higher than the 7-county MTTHS findings (24%) (14). While the summary statistics are mostly confirmatory, the MTTHS provides information at a much smaller geographic level than what is publicly available, and this fine resolution has provided the MPO with greater ability to model areas of high health need. In particular, the MPO used the health status data to refine and validate the Health Priority Areas (explained in section 2.1) previously identified by demographics alone (low income, high unemployment, and older age). Further, the health data has allowed the MPO to model the potential health impacts of increasing active transportation in the region using the Integrated Transport and Health Impact Modeling tool (ITHIM).
2.6 Modeling Health and Fiscal Impacts
The MPO was interested in estimating and monetizing the potential population health impacts of increasing walking, bicycling, and public transit use in the region in order to strengthen its messaging around these initiatives. To this end, the MPO used data from the MTTHS and other sources to calibrate and run ITHIM. The details of the Nashville implementation of ITHIM have been previously published and are summarized here (15). ITHIM estimates the population-level health impacts of changes in physical activity, air pollution emissions, and transportation collision patterns that might occur for a given change in transportation mode share. To date, ITHIM has not been used in a sprawling, southern US city like Nashville which spans more than 3,000 square miles and has an urban core and an abundance of suburban and rural land. Background on the development of and mathematical calculations in ITHIM have been previously published by Woodcock et al (16) and Maizlish et al (17). For the Nashville implementation, multiple data sources requiring collaboration across the state, local, and federal levels of government were used to gather the requisite calibration data on baseline travel and physical activity behaviors, population disease burdens, vehicle miles traveled, emissions of particulate matter less than 2.5 micrometers in diameter, roadway injuries, and demographics.
Once the model was calibrated, three preliminary scenarios (conservative, moderate, and aggressive) were developed to estimate the health effects of shifting a proportion of vehicle miles traveled to walking and bicycling while holding total miles traveled constant. Calibration data revealed an average of one mile per capita per week of active transportation in greater Nashville, with walking more common than bicycling (0.7 versus 0.3 miles, respectively). In the conservative scenario, per capita miles per week were increased to 1.7 for walking and 1.0 for biking. Given walking and biking speeds in the area, this translated to an average net increase of three minutes of per capita active transportation per day. In the moderate scenario, these values were increased to 3.7 and 1.5 per capita miles per week, or roughly 10 additional minutes per day. A final, aggressive scenario was developed where the average resident of greater Nashville performed enough active transportation to meet the aerobic physical activity guideline of 150 minutes per week (18), which equated to 5.7 and 3.0 miles per capita per week for walking and bicycling, respectively.
The ITHIM results suggest that all three scenarios could result in a net decrease in the number of premature deaths in the region (Figure 1). For the conservative scenario, prevention of chronic disease averts 38 premature deaths, but 14 roadway fatalities are incurred, for a net prediction of 24 deaths averted. This pattern is repeated in the other scenarios, with proportional increases in magnitude. ITHIM also provides estimated disease-specific impacts. For example, under the moderate scenario, the model predicts a 3% reduction in population-level cardiovascular disease and diabetes, as well as approximately 1% reductions in depression, dementia, breast cancer, and colon cancer.
Figure 1. Change in premature deaths across three scenarios: Integrated Transport and Health Impact Modeling tool, Nashville, TN – 2012.
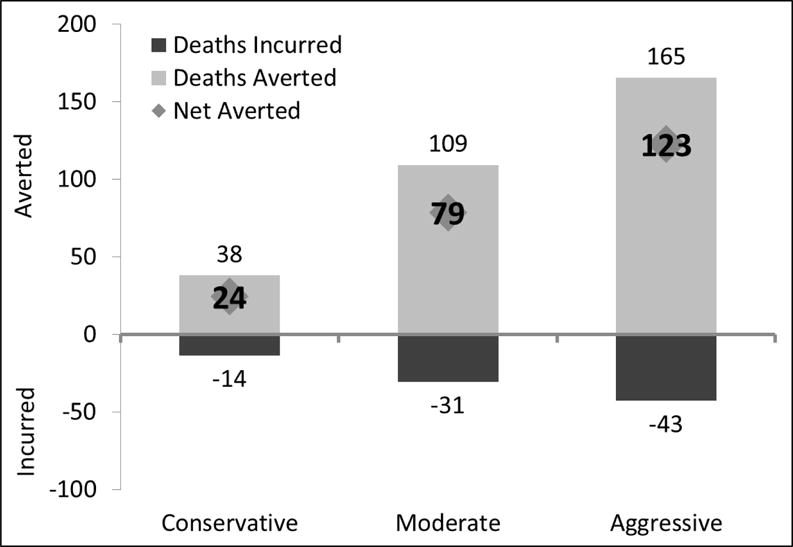
Footnote: The average baseline per capita active transportation was three minutes per day. The conservative scenario modeled an average increase of three minutes per day. The moderate scenario modeled an increase of 10 additional minutes per day. The aggressive scenario modeled an average per capita active transportation participation of 150 minutes per week, which is the aerobic physical activity guideline for moderate intensity physical activity.
The MPO wanted to estimate the financial impacts of improved health through transportation in the region, as this would likely be of interest for policy makers, stakeholders, and citizens. For 10 of the 13 conditions considered in ITHIM, the model scales national estimates of direct healthcare costs and indirect costs of lost productivity to the population of greater Nashville. Then, the model adjusts these values by the predicted change in each condition. Across the conservative, moderate, and aggressive scenarios, the model predicted annual cost reductions of $10 million, $32 million, and $63 million, respectively.
The results from ITHIM are subject to several limitations. Behavior change and prevention of chronic diseases are modeled as instantaneous which likely over-values benefits because the latent periods of several chronic diseases will delay prevention impacts. Conversely, the risks of collisions while walking and bicycling could increase more quickly, resulting in immediate costs. The net benefits could also be underestimated because ITHIM does not model emerging benefits of shifting travel behavior such as reduced noise pollution and mental health benefits (19, 20). Despite the limitations, the usefulness of having the economic benefit component of the model is to help place potential health savings and transportation spending in a common metric (US dollars). Typically, expenditures for healthcare and for transportation are not compared with one another, nor has there been a method of comparison that can relate transportation expenditures with predicted changes in health expenditures. Although the model does not factor into consideration specific transportation infrastructure facilities and costs, the health savings predicted in the model can be compared to the typical costs of implementing transportation infrastructure, thereby helping to relate the two in terms of fiscal impact.
3.0 Outcomes and Evaluation
The MPO’s efforts to increase walking, bicycling, and public transit use have had important successes in changing the transportation built environment in greater Nashville. The 2014 inventory in the Regional Bicycle and Pedestrian Study (section 2.1) revealed a 57% increase in miles of sidewalks; a 19% increase in miles of bicycle lanes, shared routes, and multi-use paths; and a 36% increase in miles of greenways compared to the 2009 edition. Since the revised scoring criteria were implemented (as described in section 2.3), nearly 70% of funded projects in the 2035 Regional Transportation Plan and 77% in the 2040 Regional Transportation Plan contain at least one element related to complete streets designs, up from an estimated 2% in the 2030 Regional Transportation Plan. Since funding the Active Transportation Program in 2012 (section 2.4), $13.6 million has been awarded for active transportation infrastructure and education projects and the 2040 regional plan reserves an additional $206 million for the program over the coming 25 years. These are all important milestones in expanding transportation options beyond privately-owned vehicles.
A thorough evaluation of the MPO’s efforts to increase population participation in walking, bicycling, and public transit use will require time. Projects selected for construction take time to complete and behavior change may lag behind facility construction (21), so monitoring participation in walking, bicycling, and transit use will need to continue after these networks are expanded. However, there is preliminary evidence of changing transportation patterns in the region. According to the American Community Survey, between 2009 and 2014, the proportion of workers in the Nashville-Davidson County area that drove alone to work decreased slightly from 80.8% to 79.5% (22). The national trend over the same period was in the opposite direction, increasing from 75.9% to 76.4% (22). While the change in Nashville cannot be solely attributed to the MPOs efforts, the shifting commute pattern (merely one facet of regional daily transportation behaviors) does offer evidence of the underlying desire for more transportation options in the region. Further, several of the components explained here can serve as baseline measures for future evaluation efforts. For example, future estimates of total miles of bicycle facilities can be compared to data from the 2009 and 2014 Regional Bicycle and Pedestrian Studies (section 2.1), and future travel survey findings on mode shares can be compared to the 2012 MTTHS (section 2.5). In this manner, the work and investments that the MPO has already made will continue to be valuable in future MPO operations.
4.0 Discussion
Understanding of the context of the MPO’s prioritization of health may be beneficial for other communities that wish to follow Nashville’s example. Below we discuss the origins of health and transportation initiatives in Nashville, the political context of the region, public engagement practices, and challenges and opportunities for other communities interested in transportation and health.
4.1 Origins of linking health and transportation in greater Nashville
The Nashville region is one of many urban areas in the United States that historically prioritized vehicular transportation over transit, walking, and bicycling. However, beginning with the Intermodal Surface Transportation Efficiency Act of 1991 and subsequent transportation acts, there has been an increasing focus in the US on the importance of providing multiple options for transportation including facilities for walking, bicycling, and mass transit. In Nashville, the shift in prioritizing people over vehicles began with the creation of the city’s first bicycle and pedestrian advocacy organization in 1998. In 2003, Walk/Bike Nashville partnered with the Nashville Community Health and Wellness Coalition and the Metro Nashville departments of Health and Planning on a Robert Wood Johnson Foundation Active Living by Design grant. The grant focused on Safe Routes to School, bicycle and pedestrian safety education, and events to promote walking, bicycling, and other activities. This effort supported Nashville’s first city-sponsored master plan for sidewalks and bikeways and another master plan for greenways and parks. The public and private collaboration together with clear visioning helped set the stage for health-oriented transportation planning in the region.
In 2006, the MPO hired its first bicycle and pedestrian planner who had been involved in the bicycle and pedestrian advocacy and grant work. With the increased recognition of rising obesity prevalence in the U.S. and the link to physical activity, the MPO’s new planner recognized the MPO’s potential to influence not only physical activity and obesity, but also air quality and transportation related injury. This person also had experience working to improve walking and bicycling to school, and this became a key conversation around transportation and health in the region. Childhood obesity and other health concerns were important topics of interest to a broad audience, and the role of transportation planning was clear in terms of where sidewalks and bikeways could be located to connect neighborhoods to schools. This early focus area helped define the role of the MPO in transportation and health for the region.
After the hire of the MPO bicycle and pedestrian planner, the MPO began educating elected officials on the economic benefits of bicycle and pedestrian facilities such as increased property values, and attraction of companies and residents looking to move to new communities. The MPO Executive Board is primarily comprised of city and county elected officials who have great interest in strategies that can increase economic development and tax revenue in their communities. By emphasizing the economic benefits first, the MPO staff were then able to discuss the additional benefits such as safer roadways, cleaner air, mobility and accessibility for those who do not drive, and opportunities for physical activity. Education on community planning and impacts is particularly import for elected officials who must wear many hats and come from a variety of professional backgrounds.
4.2 Political context
The greater Nashville area consists of seven counties with a diverse mix of people and places. As such, transportation policies and priorities can vary. However, the acceptance of previous approaches to transportation planning that emphasized vehicle travel time began to change as communities realized that there is not enough funding or space to fully address congestion, and that providing more room for cars typically simply attracts more cars (23). In addition, providing facilities for vehicles is often much more expensive than providing walking, bicycling and even some public transit facilities. When combined with the potential economic benefits explained previously, elected officials, stakeholders, and the public gained interest in transportation alternatives. In particular, investing in transportation facilities for short trips (e.g. walking and bicycling trips) that make up a large portion of daily trips was increasingly viewed as a wise use of transportation dollars that could create vehicular space on roadways without having to build additional infrastructure.
4.3 Public engagement
As noted previously, public engagement has been an important part of the MPO’s health and transportation activities. The formal shift in policy statements (section 2.2) was largely in response to stated public opinion from a transportation opinion survey of the region. In addition, the MPO sought public input through meetings with stakeholder groups, live web-casts of public meetings that allowed input via email or social media, and pedestrian and bicycle opinion surveys. The MPO also used citizen-based advisory committees for transit, freight, and bicycle and pedestrian plans. Public interest in the process was evident after the MPO created a video on the development of the regional transportation plan received several thousand internet views. In addition to various direct public engagement techniques, the MPO also partnered with stakeholder groups around housing, health, Smart Growth principles (24), food access, disabilities, the elderly, and others who could then help to disseminate and gather information from members. These combined strategies resulted in numerous opportunities for public input from a variety of residents and workers in the region.
4.4 Key opportunities and challenges for other communities
Other communities that want to incorporate public health into the transportation process may not be able to follow all of the activities described in this report, but can focus on a core set of attainable projects. For example, changing the project scoring criteria (section 2.3) was a low-cost method of emphasizing construction projects that featured health-promoting design elements (25). Project selection methods currently in use in the US can vary widely, so challenges to making such a change will likely also vary from place to place.
The Nashville Area MPO was fortunate to have skilled modelers, mappers, and analysts on staff to assist with these activities described here. Other jurisdictions, especially those serving smaller towns, may lack the staff or budget to take on similar activities. One option is forming relationships with local universities or other organizations that can provide student interns interested in some of these areas, including statistics, engineering, planning, or public health promotion. For example, the Nashville MPO received technical assistance from a post-doctoral fellow during the ITHIM implementation (section 2.6).
Another potential starting point for a transportation planning agency interested in public health is the public health department for their city, county, or state (or equivalent government units in other countries). Many health departments will have staff who work on chronic and respiratory disease prevention, which are two areas potentially impacted by transportation system changes (26, 27).
Lastly, lack of data does not have to be a barrier in changing policy or prioritizing projects. New data repositories such as Community Commons (28) and the CDC’s 500 cities project (29) can provide local-level data on chronic diseases and risk factors. Although funding for data collection and studies may often be seen as a barrier, the Nashville Area MPO utilized the flexibility of federal transportation dollars to conduct surveys and data collection around transportation and health, as well as funding non-infrastructure projects such as education, encouragement and enforcement activities for bicycle and pedestrian travel. Other communities are encouraged to take a close look at the flexibility of funding sources available to them that many not have been used previously for these types of activities.
5.0 Conclusions
The Nashville Area MPO has made significant progress in integrating health into the transportation planning process by changing policy and project funding, redesigning project scoring criteria, performing transportation research, and using health impact modeling. By thinking comprehensively about the health impacts of transportation, the MPO is strategically using public resources in a way that meets the objectives of providing accessibility and mobility of people and goods, while minimizing negative impacts on population and environmental health. The Nashville Area MPO’s experiences can serve as a useful guide to others.
Acknowledgments
The initiatives described here were partially supported by a grant from the Kresge Foundation Health, Environment, and Arts and Culture Programs.
Footnotes
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
References
- 1.Nashville Area MPO. About the MPO. Nashville TN: Nashville Area MPO; Dec 5, 2016. Available from: http://www.nashvillempo.org/about_mpo/ [Google Scholar]
- 2.Texas A&M Transportation Institute. Urban Mobility Scorecard and Appendices. 2016 Jan 27;:2015. Available from: http://mobility.tamu.edu/ums/report/
- 3.Centers for Disease Control and Prevention. Nutrition, Physical Activity and Obesity: Data Trends and Maps. 2016 Jan 27; Available from: http://nccd.cdc.gov/NPAO_DTM/LocationSummary.aspx?statecode=124.
- 4.Smart Growth America. National Complete Streets Coalition. Washington DC: Smart Growth America; p. 2016. [5 December 2016]; Available from: https://smartgrowthamerica.org/program/national-complete-streets-coalition/ [Google Scholar]
- 5.Nashville Area MPO. Regional Bicycle and Pedestrian Study – A Study for the Nashville Region. Nashville TN: Nashville Area MPO; Dec 5, 2016. Available from: http://www.nashvillempo.org/regional_plan/walk_bike/regional_study09.aspx. [Google Scholar]
- 6.United States Census Bureau. American Community Survey Table QT-P1. Washington DC: United States Census Bureau; Jan 27, 2016. Available from: http://factfinder.census.gov/faces/nav/jsf/pages/index.xhtml. [Google Scholar]
- 7.Nashville Area MPO. Nashville Area Regional Transportation Plan. Nashville TN: Nashville Area MPO; 2010. p. 2035. [Google Scholar]
- 8.Nashville Area MPO. Middle Tennessee Connected 2016–2040 Regional Transportation Plan. Nashville TN: Nashville Area MPO; 2016. [Google Scholar]
- 9.Center for Urban Transportation Research. Review of MPO Long Range Transportation Plans and Estimate of Statewide 2035 Metropolitan Area Financial Shortfall. Tallahassee FL: 2013. [Google Scholar]
- 10.Federal Highway Administration. Surface Transportation Program. Washington DC: United States Department of Transportation; Jan 27, 2016. Available from: https://www.fhwa.dot.gov/map21/factsheets/stp.cfm. [Google Scholar]
- 11.Federal Highway Administration. Bicycle and Pedestrian Program – Funding. Washington DC: United States Dapartment of Transportation; Jan 27, 2016. Available from: http://www.fhwa.dot.gov/environment/bicycle_pedestrian/funding/bipedfund.cfm. [Google Scholar]
- 12.Nashville Area MPO. Middle Tennessee Transportation and Health Study Final Report. Nashville TN: Nashville Area MPO; 2013. [5 December 2016] Available from: http://nashvillempotest.nashville.gov/docs/research/Nashville_Final_Report_062513.pdf. [Google Scholar]
- 13.Federal Highway Administration. NHTS National Household Travel Survey – Our Nation’s Travel. Washington DC: United States Department of Transportation; 2016. [5 December 2016]; Available from: http://nhts.ornl.gov/ [Google Scholar]
- 14.Centers for Disease Control and Prevention. Chronic Disease and Health Promotion Indicators. Atlanta GA: Centers for Disease Control and Prevention; 2016. [5 December 2016]; Available from: https://chronicdata.cdc.gov/Behavioral-Risk-Factors/Behavioral-Risk-Factors-Selected-Metropolitan-Area/j32a-sa6u. [Google Scholar]
- 15.Whitfield G, Meehan L, Maizlish N, Wendel A. Journal of Transport & Health. Tennessee, USA: Implementation steps and lessons learned; 2016. The integrated transport and health impact modeling tool in Nashville. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Woodcock J, Edwards P, Tonne C, Armstrong BG, Ashiru O, Banister D, et al. Public health benefits of strategies to reduce greenhouse-gas emissions: urban land transport. Lancet. 2009 Dec 05;374(9705):1930–43. doi: 10.1016/S0140-6736(09)61714-1. [DOI] [PubMed] [Google Scholar]
- 17.Maizlish N, Woodcock J, Co S, Ostro B, Fanai A, Fairley D. Health cobenefits and transportation-related reductions in greenhouse gas emissions in the San Francisco Bay area. Am J Public Health. 2013 Apr;103(4):703–9. doi: 10.2105/AJPH.2012.300939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.United States Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. Washington DC: United States Department of Health and Human Services; [5 December 2016] Available from: https://health.gov/paguidelines/pdf/paguide.pdf. [Google Scholar]
- 19.Mueller N, Rojas-Rueda D, Basagana X, Cirach M, Cole-Hunter T, Dadvand P, et al. Urban and Transport Planning Related Exposures and Mortality: A Health Impact Assessment for Cities. Environ Health Perspect. 2016 Jun 27; doi: 10.1289/EHP220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Khreis H, Warsow KM, Verlinghieri E, et al. The health impacts of traffic-related exposures in urban areas: Understanding real effects, underlying driving forces and co-producing future directions. Journal of Transport & Health. 2016;3:249–67. [Google Scholar]
- 21.Chaney H. Review Of Before And After Usage Documentation Of Pedestrian And Bicycle Facilities. Chapel Hill NC. 2005 [Google Scholar]
- 22.United States Census Bureau. American Community Survey Table S0801. Washington DC: United States Census Bureau; [27 January 2016] Available from: http://factfinder.census.gov/faces/nav/jsf/pages/index.xhtml. [Google Scholar]
- 23.Duranton G, Turner MA, National Bureau of Economic Research . The fundamental law of road congestion evidence from US cities. Cambridge, MA: National Bureau of Economic Research; 2009. Available from: http://www.nber.org/papers/w15376. [Google Scholar]
- 24.U.S. Environmental Protection Agency. Smart Growth. [November 25, 2014]; Available from: http://www.epa.gov/smartgrowth/index.htm.
- 25.Community Preventive Services Task Force. The Community Guide Physical Activity Task Force Findings. Atlanta GA: Centers for Disease Control and Prevention; p. 2016. [6 December 2016]; Available from: https://www.thecommunityguide.org/topic/physical-activity. [Google Scholar]
- 26.Association of State and Territorial Health Officials. Chronic Disease Prevention and Health Promotion. Arlington VA: Dec 6, 2016. 2016. Available from: http://www.astho.org/Programs/Prevention/Chronic-Disease-Prevention-and-Health-Promotion/ [Google Scholar]
- 27.National Association of County & City Health Officials. Chronic Disease. Washington DC: National Association of County & City Health Officials; p. 2016. [6 December 2016]; Available from: http://www.naccho.org/programs/community-health/chronic-disease. [Google Scholar]
- 28.Commons C. Maps and Data. Columbia MO: Institute for People, Place, and Possibility; 2016. [6 December 2016]; Available from: https://www.communitycommons.org/maps-data/ [Google Scholar]
- 29.Centers for Disease Control and Prevention. 500 Cities: Local data for better health. Atlanta GA: Centers for Disease Control and Prevention; 2016. [6 December 2016]; Available from: https://www.cdc.gov/500cities/ [Google Scholar]