

Abstract
Background
Sexually transmitted infections (STIs) are ongoing concerns. The best method for preventing the transmission of these infections is the correct and consistent use of condoms. Few studies have explored the use of games in interventions for increasing condom use by challenging the false sense of security associated with judging the presence of an STI based on attractiveness.
Objectives
The primary purpose of this study was to explore the potential use of computer simulation as a serious game for sex education. Specific aims were to (1) study the influence of a newly designed serious game on self-rated confidence for assessing STI risk and (2) examine whether this varied by gender, age, and scores on sexuality-related personality trait measures.
Methods
This paper undertook a Web-based questionnaire study employing between and within subject analyses. A Web-based platform hosted in the United Kingdom was used to deliver male and female stimuli (facial photographs) and collect data. A convenience sample group of 66 participants (64%, 42/66) male, mean age 22.5 years) completed the Term on the Tides, a computer simulation developed for this study. Participants also completed questionnaires on demographics, sexual preferences, sexual risk evaluations, the Sexual Sensation Seeking Scale (SSS), and the Sexual Inhibition Subscale 2 (SIS2) of the Sexual Inhibition/Sexual Excitation Scales-Short Form (SIS/SES - SF).
Results
The overall confidence of participants to evaluate sexual risks reduced after playing the game (P<.005). Age and personality trait measures did not predict the change in confidence of evaluating risk. Women demonstrated larger shifts in confidence than did men (P=.03).
Conclusions
This study extends the literature by investigating the potential of computer simulations as a serious game for sex education. Engaging in the Term on the Tides game had an impact on participants’ confidence in evaluating sexual risks.
Keywords: sex education, personality, STI, gender, computer simulation
Introduction
Background
Sexually transmitted infections (STI), including human immunodeficiency virus (HIV) are ongoing concerns. Rates of new STI diagnoses are increasing in most countries of the world, particularly among young people [1]. The best method for preventing the spread of these infections is the correct and consistent use of condoms [2,3]. However, people continue to engage in risky sexual behaviors, such as having condomless sex [4] and using condoms incorrectly [5,6]. Given these threats to individual and public health, many strategies and intervention programs have been developed to encourage consistent and correct condom use; these interventions have met with varied levels of success [7].
There are several reasons for variation in the impact of interventions. First, a “one-size-fits-all” approach is unlikely to be effective with all the intended recipients, given that they will vary in age, sexual preferences, sexual experience, and sexual attitudes [8-10]. Kirby and Laris [9] noted that it is important for a sex education program to meet the needs of the audience, taking into account different backgrounds and community values. Recent research has shown that personality traits, as well as perceived attractiveness, can significantly affect the perception of sexual risk [11]. Henderson et al [12] demonstrated how individuals high in Sensation Seeking (SS), compared with those lower in SS, rate potential partners as more attractive and are more willing to have sex with those partners, but they feel that they are less likely to contract an STI. Results of a similar study showed that participants who were engaged in a wider range of potentially risky sexual behaviors were characterized by higher Sexual Sensation Seeking Scale (SSS) [13]. These results support the idea that sex education programs may benefit from the inclusion of components aimed at teaching young people to satisfy their preferences for SSS through sexual behaviors involving minimum risk.
In addition to SSS, another measure that might be relevant is Sexual Inhibition (SI), particularly a subscale from the Sexual Inhibition/Sexual Excitation Scales (SIS/SES), which assesses sexual inhibition due to performance consequences (Sexual Inhibition Subscale 2, SIS2). In a sample of gay men, Bancroft et al [14] showed that condomless anal sex was more likely among those who scored lower on sexual inhibition due to the “threat of performance consequences” (eg, threat of an STI). In samples of both heterosexual men and women, research has supported the association between scores on SIS2 and sexual risk taking behavior [15,16].
Second, some people feel less vulnerable to STIs based on their belief that they can ascertain whether a potential partner is likely to be infected or not on the basis of the way that they look or some other superficial characteristic. It has been shown that men feel that they would be able to make judgments about other people’s sexual health status based on perceived attractiveness [8,17]. In one study, participants believed that judgments of sexual unfaithfulness could be made of the face alone, without consideration of behavioral cues [18]. Hence, one main aim of sex education programs, but one that has been seldom addressed in interventions to date, should be to challenge this false sense of security.
Third, many sex education programs have been described, particularly by young people, as being “boring” or “irrelevant” to their needs [19]. Carswell et al [20] emphasized the importance of Web-based sex education interventions, pointing out how attractive they are for young people, as they offer a confidential and convenient medium for accessing health information, avoiding the embarrassment of discussions with teachers and health providers, and overcoming potential boredom by using an interesting game format. DeSmet et al [21] and D’Cruz et al [22] highlighted the importance of certain game design features that should be considered when developing a game for sex education, such as individual tailoring, goal-setting, narrative or story, audiovisual effects, interactivity, challenge on different levels, rewards, and immediate feedback.
Bearing in mind these three issues, one direction in which sexual health interventions could profitably develop involves the use of serious games. As young people are very familiar with computer and video game playing [23,24], they may find it easier and more motivating to engage with this format of sex education intervention [25,26]. Serious games could focus on increasing understanding of the risks and addressing misconceptions [27] in the complex area of STI transmission. This could happen if people are given the potential to engage with a simulated world of people and their sexual interactions, in order to see how easy it is for diseases to spread. In serious games, it is predominantly the players who direct events and are therefore actively involved in the learning process [28,29], in contrast to traditional sex education interventions, where learners are generally relatively passive [30,31].
There has been some previous research exploring the use of games for sex education. The Source [19] is an alternative reality game that was delivered over 5 weeks to young people aged between 13 and 18 years. Each week focused on a different topic (including sexual health) that was taught using various methods, such as puzzles, board games, digital media tasks, and scavenger hunts. No behavioral outcome data were reported. However, participants enjoyed the tasks and some of them reported that The Source reinforced their decisions to engage in safer sex, although many of them commented that they found the board games boring and not as interactive as the computerized tasks.
Verran et al [32] explored the idea of using a computer simulation called SimZombie for educational activities about the epidemiology of an infectious disease (albeit not a sexually transmitted one) carried out at the Manchester Science Festival 2011. SimZombie makes use of the fact that many young people show interest in zombies and therefore it helps them engage more than they would do with a “one-way” mode of communication, such as a leaflet explaining the epidemiology of diseases. In the activities designed by Verran and colleagues, 10 teams of 4-6 participants (predominantly families or teenagers) had to answer 3 rounds of questions about monsters, microbiology, and general scientific knowledge. After each round, their answers were marked by being inserted into the simulation. Enthusiastic feedback given by participants evidenced learning through these activities.
Shegog et al [33] developed a stand-alone Web-based game of 13 lessons, called It’s Your Game (IYG). IYG lessons, which target early adolescents, include activities like interactive 2D exercises, quizzes, animations, and peer video. An evaluation of this game [34] showed no significant difference in the delay of sexual activity between intervention and control students; however, there was a significant positive between-group difference on psychological variables related to STI and condom knowledge, perceived norms about sex and condom use self-efficacy.
Although previous studies have suggested potential positive benefits of serious games in health education, very little research has been carried out to investigate the influence of computer simulations for sex education specifically. As it is possible that the benefits of such games will vary according to age [35], gender [19], and sexual attitudes [8], it would be useful to investigate the possible impact of these variables.
Aim of This Study
The primary purpose of this study was to explore the potential of computer simulation as a serious game for sex education and how the effects of a serious game might be moderated by personality traits, age, and gender. The research questions were (1) Do gender, age, and personality traits influence levels of confidence in evaluating sexual risk? (2) Does a simulation in the form of a serious game influence participants’ confidence regarding the assessment of sexual risk? and (3) Do gender, age, and personality traits influence the impact of the serious game in altering participants’ confidence in evaluating sexual risks?
Methods
Sample and Recruitment
Men and women in Southampton and surrounding areas were recruited via social media (Facebook, Twitter), posters at the University, and community advertisement boards. Potential participants were informed that data would be collected using an electronic quiz in order to investigate the use of a serious game in the form of a computer simulation for sex education. The posters contained the following information: “I would like to see how you will perform in a game we have developed for sex education.” Inclusion criteria were 18-30 years of age and English speaking. A total of 42 men, 22 women, and 2 participants who chose “other” for the question on gender were screened and all met the inclusion criteria.
Data were collected in May 2016. In total, 22 participants completed the experiment online at home, with a further 44 doing so in the lab. All participants were provided with a study information sheet and indicated electronic informed consent. The study took approximately 25 min.
Study Design
This was a Web-based questionnaire study (that used between and within subject analyses). The study employed a quiz to collect data. A draft quiz was initially trialed on 6 pilot study participants and was then refined on the basis of their feedback during individual “think aloud” sessions. “Think aloud” is a commonly used protocol for usability testing of an intervention [36].
Measures
The final questionnaire comprised four sections: (1) demographic information, (2) the participant’s sexual risk evaluations, (3 personality trait questionnaires (SSS [37] and SIS2 of the SIS/SES – Short Form [38]), and (4) the Term on the Tides quiz. The order of the 10 test questions in the quiz was fully randomized for each participant.
Demographics and Sexual Behavior
Participants were asked about their age, ethnicity, gender, and sexual orientation. Ethnicity options included white, black, Asian, mixed, and other. Gender options were “male,” “female,” “other,” and “prefer not to say,” and for sexual orientation (preference), “men,” “women,” “both,” or “none.”
Personality Traits Questionnaires
The SSS [37] assesses the tendency to seek out varied, novel, and complex sexual experiences and the desire to take personal, physical, and social risks in order to enhance sexual sensations. A sample item is “I am interested in trying out new sexual experiences.” The SSS can be used with both men and women, and shows good construct validity and internal consistency (Cronbach alpha=.83 for men and Cronbach alpha=.81 for women) [37]. Questions were answered on a 4-point scale, ranging from 1 (not at all like me) to 4 (very much like me). The sums of the scores are calculated to produce a total score on SSS, with a higher score indicating higher levels of the trait.
The SIS2 assesses individual propensity to inhibit arousal because of threat of performance consequences (such as contracting an STI) [38]. This scale is one of three subscales of the SIS/SES – SF. A sample item is “If I realize there is a risk of catching a sexually transmitted disease, I am unlikely to stay sexually aroused.” SIS/SES-SF can be used with both men and women, shows good construct validity and test-retest reliability [38]. Response options range from 1 (strongly disagree) to 4 (strongly agree); after suitable recoding, scores are summed to produce a total score, with a higher score indicating higher levels of inhibition.
Evaluation of Sexual Risk
Participants were asked to respond to the following statement: “Risks taken during unprotected sex are easy to evaluate.” Response options ranged from 1 (strongly agree) to 5 (strongly disagree). This item was used as a measure of the participants’ confidence in evaluating sexual risk.
Participants also rated their level of agreement with this statement: “The risk that someone takes when they have unprotected sex depends on the risk taking behavior of the other people in the sexual population.” Response options ranged from 1 (strongly agree) to 5 (strongly disagree). This item was included to assess the extent to which participants felt that they were in control of potential risky situations.
Both items were completed before (t1), and immediately after (t2), completion of the Term on the Tides quiz.
Game Description: Term on the Tides
The quiz concerns a cruise called Term on the Tides, developed for this study, where the user of the game is asked to answer some questions about the sexual health status of people on the cruise, at different stages of the simulation (developed in Java).
The storyboard was introduced with the following: “You embarked on a singles love cruise sailing from Mykonos down to Ibiza. The ship is full of heterosexual single men and women who are looking for easy, no-strings attached sexual encounters with each other. Passengers have not been medically examined and therefore are unaware of whether are carrying a sexually transmitted disease or not. The journey time to your destination is 1 week. The ship is fully prepared for any lengthy journey and it is well-stocked with food and supplies including an inexhaustive supply of condoms. Due to the nature of the cruise, everyone is unconcerned with forming a relationship. So whether they will choose to have sex with someone, with or without a condom, is purely based on physical appearance.” The main task of the participants was to give the right answer to 10 questions or scenarios regarding the sexual health status of certain people on the cruise.
The scenarios presented in the questions were based on the responses of male participants in a previous study [8], regarding their reported condom use intentions according to their perceptions of women’s attractiveness. These responses were used in order to produce the profiles of the people in the simulation (Figure 1). Each person’s profile had two characteristics: (1) how their condom use intentions and their judgments of STI likelihood varied with the attractiveness of a potential sexual partner, and (2) how the STI likelihood judgments of the person varied with the attractiveness of a potential sexual partner. For example, the Type A man shown in Figure 1 tends to use condoms less with women he finds more attractive (therefore he gets a “−” sign in the first box of his profile) and also believes that STI status is not associated with perceived attractiveness (therefore he gets a “=” in the second box of his profile). As nine different profiles could be created using combinations of the three symbols (“+,” “−,” “=”), nine different types of men were created and several copies (clones, ie, people with similar behavior) of those were included in the simulation. The number of clones of each type used was proportional to the number of participants in the first study [8] who fitted those types, based on their responses. In total, there were 100 men in the simulation.
Figure 1.
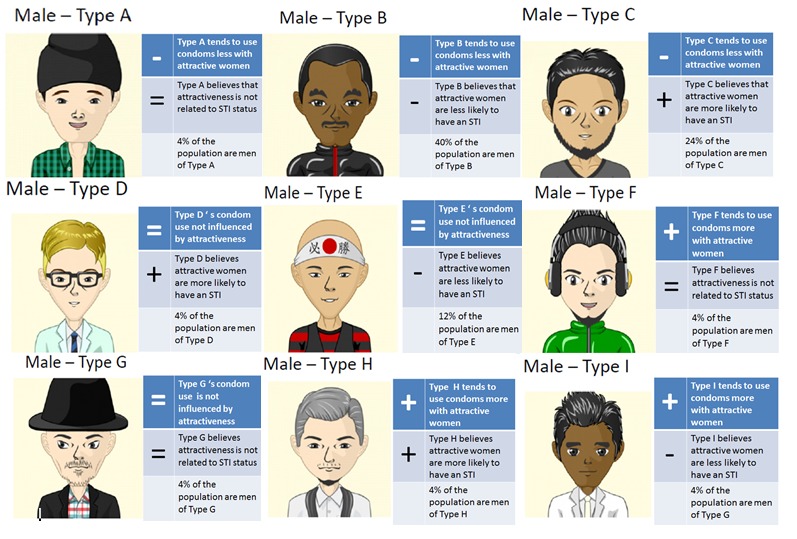
Male profiles in the computer simulation. Each type has two symbols to describe his personality. For the top one, a “+” indicates that a person uses condoms more with women that they find attractive, a “−” indicates that a person uses condoms less with women that they find attractive, and an “=” indicates that condom use is not affected by attractiveness. The bottom symbol represents the belief of a person with regards to the relationship between sexually transmitted infection (STI) risk and attractiveness: “+” means the person believes that attractive women are more likely to have an STI, “−” means that they believe attractive women are less likely to have an STI, and “=” means that the person believes that attractiveness is not related to STI.
A summary of attractiveness ratings given by each man in the previous study to each woman was shown to the users throughout the game (Figure 2). The profiles of the women were chosen in a similar way to that described above for men, with the difference being that we constructed the female profiles based on how men rated female pictures in the first study [8]. Ten types of women were chosen and we tried to include as much variability in attractiveness and STI ratings as possible. Ten clones of each one of those profiles was included in the simulation, leading to a total of 100 simulated women.
Figure 2.
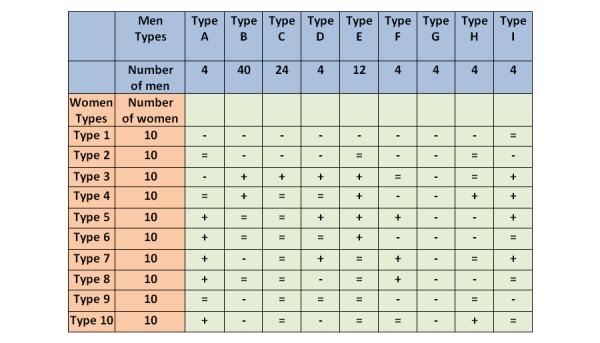
Attractiveness table. A “+” indicates that the specified man is attracted to the specified woman, a “−” indicates that the man specified is not attracted to the specified woman, and an “=” means that the man does not find the woman either attractive or unattractive.
There were various different framings used and each one of them clearly specified the precise situation of the people in the simulation. For example, in one, the user is asked to predict the outcome of an encounter between a man of Type A and a Type 4 woman versus an encounter between a man of Type A and a Type 7 woman (see Figure 3). When participants were able to correctly judge which sexual interaction was most risky, they were awarded 1 point. Ten scenarios were presented; therefore, the score for someone who did not make any correct estimates would be 0 and for someone who accurately answered all scenarios would be 10.
Figure 3.
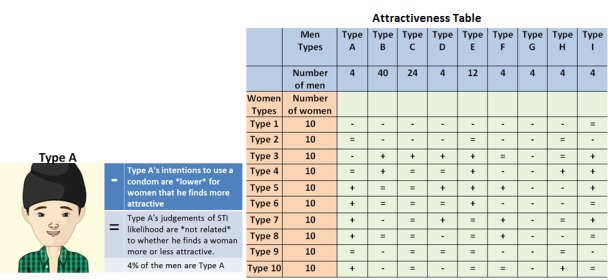
Example question: Is a type A man more likely to get an infection from a Type 4 woman or a Type 7 woman?
The final stage of the game was the feedback provided to the users. Users watched a series of encounters between men and women in the simulated population, and they received information on how well they managed to estimate risk in each scenario, by receiving an overall score for the quiz and appropriate feedback to each question (see Figure 4).
Figure 4.
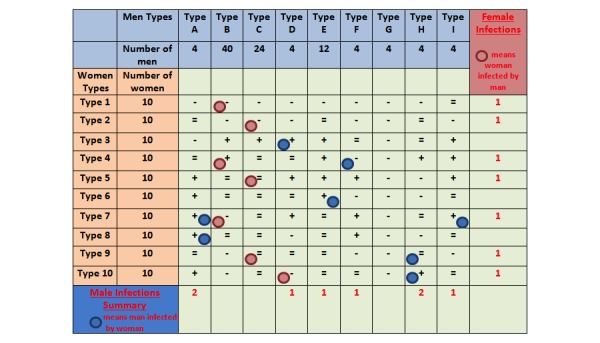
Feedback given to the participants.
In order to determine the correct answers to the questions, the computer simulation makes use of the attractiveness and condom use intentions of each person on the cruise. At the beginning of each simulation, infections are allocated to the population at random. People have the chance to meet each other and decide (1) whether to have sex or not, and, if they decide to have sex, (2) whether to have sex with or without a condom, based on the variables of attractiveness and condom use intentions specified for their type. There is a very high chance of an STI transmission when someone has condomless sex with another person who carries an infection. An average over 100 simulations was used for this quiz.
In order to account for possible biases stemming from the appearance of the images used for each type of person in the game, a random selection of pictures was allocated at the beginning of the game, from a selection of three different versions (white, black, and Asian faces).
Procedure
After providing informed consent, each participant completed the self-administered questionnaires followed by the quiz. A £100 Amazon voucher was offered as an incentive to the person with the highest score on the quiz. The Ethics Committee of the University of Southampton approved the study.
Data Analysis
To identify factors influencing the confidence ratings and the levels of change of confidence of evaluating sexual risk, a series of bivariate associations (Pearson correlation coefficients) and independent t test were conducted between the main variables examined (age, gender, personality traits, quiz score, and confidence of evaluating sexual risk before and after the game). Matched pairs t test was used to test whether participants’ confidence in evaluating STI risk changed from t1 to t2, that is, before and after the simulation.
Results
Descriptive Statistics
Demographics
A total of 66 participants (42 men, 22 women, and 2 “other”) had a mean age of 22.5 years (SD 3.3, min 18, max 29). The majority of participants were identified as white (80%, 53/66) and as heterosexual (approximately 88% [58/66]; see Table 1).
Table 1.
Sample demographics.
| Variable | n | |
| Ethnicity | ||
| White | 53 | |
| Black | 3 | |
| Asian | 7 | |
| Mixed | 1 | |
| Other | 2 | |
| Gender | ||
| Men | 42 | |
| Women | 22 | |
| Prefer not to say | 2 | |
| Age (in years) | ||
| 18-24 | 46 | |
| 25-30 | 20 | |
Personality Variables
On the SSS, the mean score for men was 23.1 and for women was 22.5. Higher scores indicated greater sexual sensation seeking. There was no significant gender difference in this measure (t62=0.42, not significant [ns]).
On the SIS2, the higher a participant scored, the higher the propensity for sexual arousal to be reduced in the face of threats of performance consequences. The mean SIS2 score for women (12.9) was significantly higher than that for men (11.2) (t62=3.05, P<.005).
Research Question 1: Do Gender, Age, and Personality Traits Influence Levels of Confidence in Evaluating Sexual Risk?
At t1, women believed that risk was easier to assess than did men, with the mean ratings 3.82 and 3.25, respectively (t62=1.99, P=.05); however, the belief that risk depends on the other people did not differ between men and women (t62=0.19, ns).
Age showed no significant correlations with participants’ confidence in evaluating risk (r=.11, n=66, ns) or their belief that risk depends on others in the population (r=−.05, n=66, ns).
At t1, no significant correlations between SSS or SIS2 and participants’ confidence in evaluating sexual risk (r=.15 and r=.10, respectively, n=66, ns) or in believing that the sexual risk depends on others in the population (r=.15 and r=.13, respectively, n=66, ns) were found.
Research Question 2: Does a Simulation in the Form of a Serious Game Influence Participants’ Confidence Regarding the Assessment of Sexual Risk?
In response to the statement “Risks taken during unprotected sex are easy to evaluate,” the mean score before the game was 3.47, and after the game it was 2.98. A matched pairs t test showed that the change in confidence was significant (t63=5.81, P<.001). Before the intervention, 56% agreed that it was easy to evaluate risk, whereas only 44% did so after the intervention. Similarly, 24% disagreed before the game compared with 38% after the game.
In response to the statement “The risk that someone takes when they have unprotected sex depends on the risk taking behavior of the other people in the sexual population,” the mean score before the game was 3.74, and after the game it was 3.77. A matched pairs t test revealed that the difference between these mean scores was not significant (t65=0.27, ns).
Research Question 3: Do Gender, Age, and Personality Traits Influence the Impact of the Serious Game in Altering Participants’ Confidence in Evaluating Sexual Risks?
There was a significant gender difference in the impact of the game on confidence ratings; women had a greater reduction in confidence regarding their perceived ability to evaluate sexual risk than did men (mean change scores for men 0.30 and 0.82 for women; t60=3.11, P<.005). There were no gender differences in change scores for believing that risk depends on other people (mean change scores for men 0.05 and −0.18 for women; t62=0.92, ns). Age did not correlate with either of the risk measures (for easy, r=.12, n=64, ns, and for risk depends on others, r=−.18, n=60, ns).
Similarly, there was no correlation between the changes in confidence ratings concerning assessment of sexual risk before and after the game, and scores on SSS or SIS2 (r=−.06, n=64, ns and r=.11, n=64, ns, respectively). Finally, there was also no correlation between the changes in confidence ratings concerning sexual risk depending on others before and after the game, and scores on SSS or SIS2 (r=.20, n=66, ns, and r=−.03, n=66, ns, respectively).
Additional Results on Quiz Scores
The average score on the quiz across the 66 participants was 5 out of 10 (min=2, max=8; the mean for men was 5.1, and 4.8 for women; t62=0.79, ns). There were no differences in scores according to age (r=−.13, n=66, ns) or whether participants completed the study at home or in the laboratory (r=.20, n=66, ns). Anecdotal reports after the study indicated that many participants found the game very interesting and thought provoking, but also quite challenging.
No significant correlation was found between scores on the quiz and confidence in evaluating sexual risk at t1 (r=−.06, n=66, ns and r=−.07, n=66, ns, for risk for self and risk for others, respectively), or the change in confidence regarding risk-assessment between t1 and t2 (r=−.01, n=64, ns and r=−.06, n=66, ns, respectively).
Discussion
Principal Findings
This study sheds some light on the use of computer simulations as a serious game for sex education. There was a significant change in participants’ confidence in evaluating sexual risk in the Term on the Tides game. Before they played the game, the majority of the participants believed that it was easy to evaluate the risks of unprotected sex. The serious game challenged individuals’ confidence to evaluate risks and, as a result of this, approximately 40% of participants reported lower confidence after playing the game than they did at the t1 baseline. The fact that overall confidence in evaluating risks reduced after the participants had engaged with the game illustrates a potentially positive public health outcome. It would be expected that lower confidence in evaluating sexual risks would lead to greater caution in sexual encounters.
Age and the personality trait variables—SSS and SIS2—were not correlated with the confidence of evaluating risk or with the level of change in confidence before and after the game. Gender, however, did have an effect, as women demonstrated a bigger shift in confidence of evaluating sexual risk than men. This finding agrees with a previous study on The Source, an alternative reality game [19], which suggested that women were influenced more by engaging in the game than men. Brüll et al [39] argued that males prefer the use of more explicit terminology to describe sexual activity in a game than females.
Previous studies have shown that the difficulty of a game is a major determinant of the influence that it has on users, mainly because users get discouraged if the game is very difficult or they get bored if it is too easy [40,41]. Although in this case participants were not asked directly to comment on the difficulty of the game, we observed that many reflected on the experience and discussed with the researcher what they had learned from the game. Most of them found it “challenging,” and may have been motivated to continue because the person with the highest score would win an Amazon voucher.
Future research should investigate the effect of age on the influence of a sex education game using a bigger sample, as there were not enough older participants in this study to report findings regarding this variable with confidence. Additionally, the relationship status and relationship power of the participants should be investigated, as this might significantly change the way they associate with the characters of the game and therefore their evaluation of sexual risk [42]. Moreover, different ways to enhance immersion in the game should be examined, in order to keep the interest of the users high and keep them engaged with the educational activity for as long as possible; for example, by using a virtual reality (360) simulation, which will challenge the users’ sexual health knowledge and attitudes on various difficulty levels using a somewhat less artificial and sterile environment or characters [43]. Sexual arousal during the sex education game could also be investigated as it is a factor that influences condom use in real-life contexts [44].
This study is a step toward the design of tailored and relevant sex education interventions, as called for by DeSmet [21] and D’Cruz [22]. Although this study includes several features recommended by these authors, for example, goal-setting, narrative, and so on, it might be profitable to explore greater interactivity and the use of audiovisual stimuli.
Strengths and Limitations
Some limitations of the study need to be acknowledged. Participants were not asked systematically about the difficulty of the game and therefore we only have anecdotal information about this variable. Also, we used a relatively small convenience sample and no behavioral outcomes or behavioral theory were assessed. Notwithstanding these limitations, this study is the first to explore the influence of computer simulations in the form of a serious game for sex education in relation to risk perception, and to investigate the impact that individual difference variables (age, gender, and personality) may have on the outcome. The results would be particularly useful for serious games designers for sex education as they provide some limited but promising insight into which aspects of games-tailoring could be beneficial and worth investigating further.
Conclusions
Computer simulations, presented in the form of a serious game, had an impact on participants’ confidence in evaluating sexual risk, especially for women. This suggests that serious games developed for use in this setting should be further investigated and perhaps gender-tailored. Working toward these goals might contribute to a reduction in STI rates. Personality traits and age were not related to the change in participants’ confidence in evaluating sexual risks before and after engaging in the game.
Acknowledgments
This work was supported by an EPSRC Doctoral Training Centre grant (EP/G03690X/1).
Abbreviations
- HIV
human immunodeficiency virus
- IYG
It’s Your Game
- SES
Sexual Excitation Scale
- SI
Sexual Inhibition
- SIS2
Sexual Inhibition Subscale 2
- SS
Sensation Seeking
- SSS
Sexual Sensation Seeking Scale
- STI
sexually transmitted infection
Footnotes
Authors' Contributions: AE led the study design, game development, conducted the research, and prepared early drafts of the article. SB, CG, and RI helped with the design of the study and the game development. RI and AE carried out the analyses. All authors read and commented on drafts of the article, and approved the final version.
Conflicts of Interest: None declared.
References
- 1.World Health Organization WHO. 2016. [2016-09-01]. Sexually Transmitted Infections: Fact Sheet http://www.who.int/mediacentre/factsheets/fs110/en/
- 2.Padian NS, Buvé A, Balkus J, Serwadda D, Cates W. Biomedical interventions to prevent HIV infection: evidence, challenges, and way forward. Lancet. 2008 Aug;372(9638):585–599. doi: 10.1016/S0140-6736(08)60885-5. http://psycnet.apa.org/?&fa=main.doiLanding&doi=10.1037/a0029041. [DOI] [PubMed] [Google Scholar]
- 3.Warner L, Stone KM, Macaluso M, Buehler JW, Austin HD. Condom use and risk of gonorrhea and Chlamydia: a systematic review of design and measurement factors assessed in epidemiologic studies. Sex Transm Dis. 2006 Jan;33(1):36–51. doi: 10.1097/01.olq.0000187908.42622.fd. [DOI] [PubMed] [Google Scholar]
- 4.Sanders SA, Reece M, Herbenick D, Schick V, Dodge B, Fortenberry JD. Condom use during most recent vaginal intercourse event among a probability sample of adults in the United States. J Sex Med. 2010 Oct;7(Suppl 5):362–73. doi: 10.1111/j.1743-6109.2010.02011.x. [DOI] [PubMed] [Google Scholar]
- 5.Crosby R, Yarber WL, Sanders SA, Graham CA. Condom discomfort and associated problems with their use among university students. J Am Coll Health. 2005;54(3):143–7. doi: 10.3200/JACH.54.3.143-148. [DOI] [PubMed] [Google Scholar]
- 6.Baxter S, Blank L, Guillaume L, Squires H, Payne N. Views regarding the use of contraception amongst young people in the UK: a systematic review and thematic synthesis. Eur J Contracept Reprod Health Care. 2011 Feb 21;16(3):149–160. doi: 10.3109/13625187.2011.556762. http://psycnet.apa.org/?&fa=main.doiLanding&doi=10.1037/a0029041. [DOI] [PubMed] [Google Scholar]
- 7.Scott-Sheldon LA, Huedo-Medina TB, Warren MR, Johnson BT, Carey MP. Efficacy of behavioral interventions to increase condom use and reduce sexually transmitted infections: a meta-analysis, 1991 to 2010. J Acquir Immune Defic Syndr. 2011 Dec 15;58(5):489–98. doi: 10.1097/QAI.0b013e31823554d7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Eleftheriou A, Bullock S, Graham CA, Stone N, Ingham R. Does attractiveness influence condom use intentions in heterosexual men? An experimental study. BMJ Open. 2016 Jun;6(6):e010883. doi: 10.1136/bmjopen-2015-010883. http://bmjopen.bmj.com/cgi/pmidlookup?view=long&pmid=27315834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kirby D, Laris B. Effective curriculum-based sex and STD/HIV education programs for adolescents. Child Dev Perspect. 2009;3(1):21–29. doi: 10.1111/j.1750-8606.2008.00071.x. [DOI] [Google Scholar]
- 10.Shegog R, Markham C, Peskin M, Dancel M, Coton C, Tortolero S. “It's your game”: an innovative multimedia virtual world to prevent HIV/STI and pregnancy in middle school youth. Stud Health Technol Inform. 2007;129(Pt 2):983–7. doi: 10.3233/978-1-58603-774-1-983. [DOI] [PubMed] [Google Scholar]
- 11.Henderson V, Hennessy M, Barrett D, Curtis B, McCoy-Roth M, Trentacoste N, Fishbein M. When risky is attractive: sensation seeking and romantic partner selection. Pers Individ Dif. 2005;38(2):311–325. doi: 10.1016/j.paid.2004.04.010. [DOI] [Google Scholar]
- 12.Henderson V, Hennessy M, Barrett D, Martin S, Fishbein M. Tell me more: sensation seeking and information seeking in evaluating romantic partners. J Res Pers. 2006;40(5):611–630. doi: 10.1016/j.jrp.2005.06.002. [DOI] [Google Scholar]
- 13.Gutiérrez-Martínez O, Bermúdez MP, Teva I, Buela-Casal G. Sexual sensation-seeking and worry about sexually transmitted diseases (STD) and human immunodeficiency virus (HIV) infection among Spanish adolescents. Psicothema. 2007 Nov;19(4):661–6. [PubMed] [Google Scholar]
- 14.Bancroft J, Janssen E, Strong D, Carnes L, Vukadinovic Z, Long JS. Sexual risk-taking in gay men: the relevance of sexual arousability, mood, and sensation seeking. Arch Sex Behav. 2003;32(6):555–572. doi: 10.1023/A:1026041628364. [DOI] [PubMed] [Google Scholar]
- 15.Carpenter DL, Janssen E, Graham Ca, Vorst H, Wicherts J. Women's scores on the Sexual Inhibition/Sexual Excitation Scales (SIS/SES): gender similarities and differences. J Sex Res. 2008;45:36–48. doi: 10.1080/00224490701808076. [DOI] [PubMed] [Google Scholar]
- 16.Bancroft J, Janssen E, Carnes L, Goodrich D, Strong D, Long JS. Sexual activity and risk taking in young heterosexual men: the relevance of sexual arousability, mood, and sensation seeking. J Sex Res. 2004 May;41(2):181–92. doi: 10.1080/00224490409552226. [DOI] [PubMed] [Google Scholar]
- 17.Leonard T. citeseerx.ist. 2008. Richard H Thaler, Cass R Sunstein, Nudge: Improving decisions about health, wealth, and happiness http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.364.5470&rep=rep1&type=pdf.
- 18.Rhodes G, Morley G, Simmons LW. Women can judge sexual unfaithfulness from unfamiliar men's faces. Biol Lett. 2013 Feb 23;9(1):20120908. doi: 10.1098/rsbl.2012.0908. http://rsbl.royalsocietypublishing.org/cgi/pmidlookup?view=long&pmid=23221873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bouris A, Mancino J, Jagoda P, Hill B, Gilliam M. Reinvigorating adolescent sexuality education through alternate reality games: the case of The Source. J Sex Educ. 2015:1–15. doi: 10.1080/14681811.2015.1101373. [DOI] [Google Scholar]
- 20.Carswell K, McCarthy O, Murray E, Bailey JV. Integrating psychological theory into the design of an online intervention for sexual health: the sexunzipped website. JMIR Res Protoc. 2012;1(2):16. doi: 10.2196/resprot.2114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.DeSmet A, Shegog R, Van Ryckeghem D, Crombez G, De Bourdeaudhuij I. A systematic review and meta-analysis of interventions for sexual health promotion involving serious digital games. Games Health J. 2015 Apr;4(2):78–90. doi: 10.1089/g4h.2014.0110. [DOI] [PubMed] [Google Scholar]
- 22.D'Cruz J, Santa MD, Dube S, Markham C, McLaughlin J, Wilkerson JM, Peskin MF, Tortolero S, Shegog R. Promoting parent-child sexual health dialogue with an intergenerational game: parent and youth perspectives. Games Health J. 2015 Apr;4(2):113–22. doi: 10.1089/g4h.2014.0080. http://europepmc.org/abstract/MED/26181805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.McGonigal J. Reality is broken: Why games make us better and how they can change the world. London: Penguin Books; 2011. [Google Scholar]
- 24.Graafland M, Dankbaar M, Mert A, Lagro J, De Wit-Zuurendonk L, Schuit S, Schaafstal A, Schijven M. How to systematically assess serious games applied to health care. JMIR Serious Games. 2014;2(2):e11. doi: 10.2196/games.3825. http://games.jmir.org/2014/2/e11/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chu SK, Kwan AC, Reynolds R, Mellecker RR, Tam F, Lee G, Hong A, Leung CY. Promoting sex education among teenagers through an interactive game: reasons for success and implications. Games Health J. 2015 Jun;4(3):168–74. doi: 10.1089/g4h.2014.0059. [DOI] [PubMed] [Google Scholar]
- 26.Kashibuchi M, Sakamoto A. The educational effectiveness of a simulation/game in sex education. Simul Gaming. 2001 Sep 01;32(3):331–343. doi: 10.1177/104687810103200304. [DOI] [Google Scholar]
- 27.Masaro CL, Dahinten VS, Johnson J, Ogilvie G, Patrick DM. Perceptions of sexual partner safety. Sex Transm Dis. 2008;35(6):566–571. doi: 10.1097/OLQ.0b013e3181660c43. [DOI] [PubMed] [Google Scholar]
- 28.Bonsignore E, Hansen D, Kraus K, Ruppel M. Alternate reality games as platforms for practicing 21st-century literacies. Int J Learning Media. 2012 Jan;4(1):25–54. doi: 10.1162/IJLM_a_00086. [DOI] [Google Scholar]
- 29.Gilliam M, Orzalli S, Heathcock S, Sutherland E, Jagoda P, Menendez A, Ojengbede O. From intervention to invitation: reshaping adolescent sexual health through story telling and games. Afr J Reprod Health. 2012 Jun;16(2):189–96. [PubMed] [Google Scholar]
- 30.Greitzer F, Kuchar O, Huston K. Cognitive science implications for enhancing training effectiveness in a serious gaming context. J Educ Resour Comput. 2007;7(3):2. doi: 10.1145/1281320.1281322. [DOI] [Google Scholar]
- 31.Arnab S, Brown K, Clarke S, Dunwell I, Lim T, Suttie N, Louchart S, Hendrix M, de Freitas S. The development approach of a pedagogically-driven serious game to support Relationship and Sex Education (RSE) within a classroom setting. Comput Educ. 2013 Nov;69:15–30. doi: 10.1016/j.compedu.2013.06.013. [DOI] [Google Scholar]
- 32.Verran J, Crossley M, Carolan K, Jacobs N, Amos M. Monsters, microbiology and mathematics: the epidemiology of a zombie apocalypse. J Biol Educ. 2013 Oct 29;48(2):98–104. doi: 10.1080/00219266.2013.849283. [DOI] [Google Scholar]
- 33.Shegog R, Peskin MF, Markham C, Thiel M, Karny E, Addy RC, Johnson KA, Tortolero S. It's your game-tech: toward sexual health in the digital age. Creat Educ. 2014 Aug;5(15):1428–1447. doi: 10.4236/ce.2014.515161. http://europepmc.org/abstract/MED/25705561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Peskin MF, Shegog R, Markham CM, Thiel M, Baumler ER, Addy RC, Gabay EK, Emery ST. Efficacy of It's Your Game-Tech: a computer-based sexual health education program for middle school youth. J Adolesc Health. 2015 May;56(5):515–21. doi: 10.1016/j.jadohealth.2015.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kamel BM, Gammon S, Dixon MC, MacRury SM, Fergusson MJ, Miranda RF, Mourinho BT, Yang SP. Digital games for type 1 and type 2 diabetes: underpinning theory with three illustrative examples. JMIR Serious Games. 2015;3(1):e3. doi: 10.2196/games.3930. http://games.jmir.org/2015/1/e3/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Yardley L, Morrison LG, Andreou P, Joseph J, Little P. Understanding reactions to an internet-delivered health-care intervention: accommodating user preferences for information provision. BMC Med Inform Decis Mak. 2010;10:52. doi: 10.1186/1472-6947-10-52. http://www.biomedcentral.com/1472-6947/10/52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kalichman S. Handbook of Sexuality Related Measures. New York: Routledge; 2011. pp. 564–565. [Google Scholar]
- 38.Carpenter D, Janssen E, Graham C, Vorst H, Wicherts J. Handbook of Sexuality Related Measures. New York: Routledge; 2011. Sexual Inhibition/Sexual Excitation Scales-Short Form; pp. 236–238. [Google Scholar]
- 39.Brüll P, Ruiter RA, Wiers RW, Kok G. Gaming for safer sex: young German and Turkish people report no specific culture-related preferences toward educational games promoting safer sex. Games Health J. 2016 Sep 28;5(6):357–365. doi: 10.1089/g4h.2016.0016. [DOI] [PubMed] [Google Scholar]
- 40.Juul J. Fear of failing? the many meanings of difficulty in video games. New York: Routledge; 2009. pp. 237–252. [Google Scholar]
- 41.Qin H, Rau P, Salvendy G. Effects of different scenarios of game difficulty on player immersion. Interact Comput. 2010;22(3):230–239. doi: 10.1016/j.intcom.2009.12.004. [DOI] [Google Scholar]
- 42.Pulerwitz J, Amaro H, De Jong W, Gortmaker SL, Rudd R. Relationship power, condom use and HIV risk among women in the USA. AIDS Care. 2002 Dec;14(6):789–800. doi: 10.1080/0954012021000031868. [DOI] [PubMed] [Google Scholar]
- 43.Shegog R, Brown K, Bull S, Christensen JL, Hieftje K, Jozkowski KN, Ybarra ML. Serious games for sexual health. Games Health J. 2015 Apr;4(2):69–77. doi: 10.1089/g4h.2014.0139. [DOI] [PubMed] [Google Scholar]
- 44.Ariely D, Loewenstein G. The heat of the moment: the effect of sexual arousal on sexual decision making. J Behav Decis Making. 2006 Apr;19(2):87–98. doi: 10.1002/bdm.501. [DOI] [Google Scholar]