

Abstract
Background
An unhealthy lifestyle of college students is an important public health concern, but few studies have been undertaken to examine the role of socio-cultural differences.
Methods
For this cross-sectional comparative study, data on college students’ health-promoting lifestyles (HPL), as measured using the Health-Promoting Lifestyle Profile (HPLP-II) scale, and self-rated health status (SRH) as measured by Sub-Optimal Health Measurement Scale (SHMS V1.0) were collected from 829 college students.
Results
The sample of 829 college students included 504 (60.8%) Chinese and 325 (39.2%) international students. Chinese students had higher scores in overall health-promoting lifestyle (HPL) (P < 0.001, eta squared =0.113) and in all the six subclasses than their international counterparts. In relation to health status evaluation, the two groups varied in physiological health (P < 0.001, eta squared = 0.095) and social health (P = 0.020, eta squared = 0.007) but there was no significant difference in psychological health subscale (P = 0.156, eta squared = 0.002). HPL was predicted by financial status among the Chinese group and by student’s major, age and level of education in the international group. Body mass index (BMI) and financial status emerged as predictors of the three subscales of SHMS V1.0 in the Chinese group and also of physiological and psychological subscales in the international group. Gender was associated with psychological health in both groups. Smoking status was a predictor of psychological health in both groups and also of social health in the international group. The level of education emerged as a predictor of social health in the international group.
Regression analyses revealed a significant association between health status and healthy lifestyle (P < 0.001). In reference to participants with “excellent” lifestyle, participants with moderate lifestyle were at a 4.5 times higher risk of developing suboptimal health status (SHS) (OR: 4.5,95% CI:2.2-9.99) and those with a ‘general’ lifestyle were at a 3.2 times higher risk SHS (OR: 3.2, 95% CI: 1.5-7.18). Good and moderate HPLP-II levels of nutrition are associated with low risk of suboptimal health status (OR: 0,41 and 0,25, respectively). Participants in good and moderate HPLP-II levels of interpersonal relations are associated with higher risk of suboptimal health (OR:2,7 and 3,01 respectively) than those in excellent levels of HPLP-II.
Conclusion
Collectively, these findings provide a convincing body of evidence to support the role of socio-cultural factors as key determinants of the HPL and SRH of college students.
Background
A health-promoting lifestyle (HPL) encompasses a multidimensional pattern of self-initiated perceptions and activities aimed to maintain and improve individual’s health and wellness [1].HPL can decrease the occurrence of disease, lower the death rate and contribute to an improved health status [2, 3]. On the contrary, risky health behaviors are actions that increase the risk of injury and disease in general [4], for instance, tobacco and alcohol use, an unhealthy diet and lack of exercise lead to various chronic diseases. Furthermore, unhealthy behavior and lifestyle are two important factors associated with ten major causes of death [5–10].
Though healthy lifestyle behaviors are important for individuals in all periods of life, this is of primary importance during youth. The period of emerging adulthood is an important age for the formation of health behaviors associated with an increased risk of chronic disease [11]. Unhealthy practices and behaviors established during young ages may resonate across a lifespan and result in increased health risks later in life [12–15]. As such, this unique developmental period may be an ideal time for the effective provision of preventive health information. Therefore, assessment of health promoting behaviors among university students is important, as they are young individuals.
Globalization has led to increased human mobility hence many students travel out of their countries to study abroad. It is estimated that over 300,000 foreign students come to mainland China on an annual basis to study in higher education institutes [16]. This figure is estimated to increase to over half-a-million international students annually by the year 2020 [16]. Non-native students are likely to face challenges as they adjust themselves to a different environment, culture, values, and attitudes, which might influence their personal health, lifestyles, and behaviors. At the same time, these individuals are exposed to a new level of freedom related to lifestyle choices (e.g., eating habits, sleep routines, levels of participation in physical activity, and alcohol/tobacco use). It is well documented that different ethnicities may place different values on health and healthy behaviors [17] and international students may confront different health challenges from those of Chinese locals due to a difference in cultural and social environments and health care systems. Research has revealed that international students generally experience more difficulties adapting to college life abroad than they would in their home countries [18]. This could be attributed to challenges due to homesickness, unfamiliar diets, language barriers, health and financial issues, relationships with peers, daily living activities, religion, and differences in the education systems.
Students native to China are also challenged by unhealthy lifestyles [19]. Over 46–56% of Chinese college students were reported to be in suboptimal health status (SHS) [7]. SHS is defined as medically undiagnosed or functional somatic syndromes [20–22]. SHS is associated with unhealthy lifestyles [7]. Individuals in SHS deteriorate in vitality, physiological function, and the capacity to adapt to varying conditions.
Previous college studies have paid little attention to the influence of culture and modern society on health-promoting lifestyles, especially in China. To the best of our knowledge, no empirical studies have examined the similarities and differences in SRH and health-promoting lifestyle in China. Such a study would fill an important gap in the literature. Hence, we carried out an investigation among college students in Dalian, China to assess SRH and HPL in an international and local sample of college students affiliated with different cultural, social and economic backgrounds. Also, the present study examined the similarities and differences in HPL and SRH between international and Chinese, and associations of health-promoting lifestyle and SRH.
The following research questions were addressed in the study:
Are there differences in health-promoting behaviors and self-rated health between Chinese and international college students?
Is there any association among health behaviors and self-rated health status?
Methods
Design & Participants
A cross-sectional study was carried out between May and July 2016, using a self-administered questionnaire while interviewing a population of college students. The study was conducted at four conveniently selected universities in the city of Dalian. To increase participation and completeness/truthfulness of each questionnaire, recruitment was conducted during lectures. Selected participants were college students who met the following inclusion criteria: enrolled in an academic degree program at all levels, have stayed in China for longer than six months, and had no critical illness or intake of medication in the previous 3 weeks. (Fig. 1).
Fig. 1.
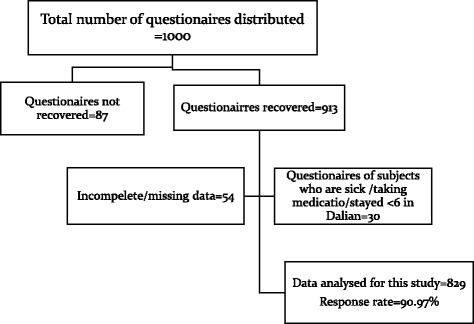
Flowchart showing inclusion and exclusion criteria of the study participants
Sample size
We used the formulae for two independent samples, a dichotomous outcome to estimate our sample size [23].
Where ni is the sample required in each group (i = 1,2) α is the selected level of significance, Z1- α/2, is the value from the standard normal distribution holding 1- α/2, 1-β/2 is the selected power, and Z2−β/2 is the value from standard normal distribution holding 1-β below it.ES is the effect size defined as
Where |p1-p2| is the absolute value of the difference in proportions between the two groups expected under the alternative hypothesis, H1 and P is the overall proportion, based on pooling the data from the two comparison groups. We estimated that 45 and 56% of the international and Chinese students will be in suboptimal health status, respectively. The minimum sample size required to ensure that the power of the test is 80% to detect the difference in proportions taking into account of a drop out of 30% was calculated as follows;
Sample sizes n1 = 324 and, n2 = 324 was needed to ensure that the test of hypothesis had 80% power to detect suboptimal health status in college students. With an estimated 30% drop data; therefore, our target population was; 648*100/70 = 926.
Measures
Socio-demographic characteristics
We employed a self-administered questionnaire to obtain data on respondents’ socio-demographic information including age, gender, level of education, student’s major, smoking status, alcohol consumption, financial status, length of stay in Dalian, body weight and height which were transformed into body mass index (BMI) (kg/m2). This is a statistical measure of the weight of a person scaled according to their height. The following four categories of BMI included being underweight (≤18.5); normal weight (18.6–24.9); overweight (25–29.9); and obese (≥30).
Self-rated health status (SRH)
We adopted the Sub-Optimal Health Measurement Scale Version 1.0 (SHMS V1.0) to evaluate the SRH among the college students. SHMS V1.0 has been shown to be a valid and reliable tool in various ethnic groups, with a Cronbach’s alpha and split-half reliability coefficients of 0.917 and 0.831, respectively. SHMS V1.0 comprises 39 items with 3 dimensions: physiological health (14 items), psychological health (12 items), societal health (9 items), and 4 other items for a health status evaluation, in which participants were asked: "What is your general feeling in terms of physical/psychological/social/general health?" The 35 items of five-point Likert-type (1 = never, 2 = occasionally, 3 = sometimes, 4 = often, 5 = routinely) were used to measure the respondent’s self-reported health problems. Transformed scores were determined to account for reverse questions. The total scores for each SHMS V1.0 domains were transformed to a range of 0 to 100, with the highest scores representing better SRH. The threshold values for SHS in the physiological, psychological and social health dimensions of SHMS V1.0 were fixed at 68,67, and 67 respectively. Because few subjects reported their health to be in the disease state, they were combined with the sub-optimal status group. A dichotomous variable was created (0 = Healthy, 1 = Sub-Optimal health) for self-rated health. The overall scale Cronbach’s alpha in this study was 0.873 and 0.898 for the international and Chinese students, respectively. The sub-scale alpha of SRH physiological health was 0.701 and 0.798, psychological health, 0.788 and 0.846, and societal health 0.854 and 0.798 for the international and the Chinese students respectively.
Health-promoting lifestyle (HPL)
To evaluate the students’ lifestyle, we used the 52-item Health Promoting Lifestyle Profile II (HPLP-II). The measurement has been used widely internationally and has good validity and reliability [24]. We used a previously translated and validated Chinese version for the Chinese and an original English version for international students. It consists of 6 dimensions namely: health responsibility (9 items), spiritual growth (9 items), physical activity (8 items), nutrition (9 items), interpersonal relationships (9 items), and stress management (8 items). To determine the frequency of each behavior, a 4-point Likert scale (1 = “never”, 2 = “sometimes”, 3 = “often”, and 4 = “routinely”) was used. In line with the previous studies, a mean ≥ 2.50 was considered to be a positive response [25] indicating that one is engaging in health-promoting lifestyle. Since all the items of HPLP-II were presented positively, there were no items to be reversed. Scores for each dimension were generated by summing the scores of all items and computing a mean score, which has a possible range from 1 to 4. Following the recommendations of the original authors of the scale, the overall HPLP-II score was obtained by calculating the mean of the responses to all 52 items [1].HPLP-II scores ranged between 52 and 208. To determine the levels of HPLP-II subscales, the scores were divided by quartiles into low (1.00–2.38), moderate (2.39–2.61), good (2.62-2.91) and excellent (2.92–4.00) HPL. High scores indicated a greater frequency of health-promoting behaviors. A Cronbach’s alpha of 0,887 and 0,939 for international students and Chinese group, respectively, regarded as a reliability measure, was obtained in this study.
Data analysis
Data were analyzed with descriptive statistics, multiple linear and binary logistics regression analysis using the Statistical Package for the Social Sciences for Windows (Version 21; SPSS Inc., Chicago, IL). Data were expressed as the mean ± SD for continuous variables or the n (%) for categorical variables. An independent t-test and Chi-square for independence were used to compare mean differences and proportions between the groups, respectively. Pearson/spearman rank correlation was used to explore the relationship between HPLP-II scores and SRH status. One-way analysis of variance (ANOVA) or t-test was performed to examine the effects of demographic characteristics on HPLP-II and SHMS V1.0 scores. Effect sizes (ESs) for independent t-tests and one-way ANOVA were calculated by Eta squared and Cohen’s d (0.1: small effect; 0.6: medium effect; 0.14: large) to assess the magnitude of the significant group differences [26]. Binary logistics was conducted to explore the association between SRH status and HPL among the college students. A p-value of ≤0.05 was considered statistically significant.
Results
Characteristics of the participants
Table 1 depicts the characteristics of the 829 participants; the mean age was 22.18 (range, 18 years). Out of the total participants, 60.80% were female, and 39.20% were international students, while 60.08 were Chinese. There was a significant difference in terms of age (n = 829, t = 6.99, P ≤ 0.050), gender (n = 829, x2 = 14, P < 0.001), BMI (n = 829, x2 = 21.53, P < 0.001), level of education (n = 829, x2 = 23.04, P < 0.001), smoking status (n = 829, x2 = 58.172, P < 0.001), alcohol consumption (n = 829, x2 =40.862, P < 0.001), students’ major (n = 829, x2 = 47.117, P < 0.001) and financial status (n = 829, x2 = 52.23, P < 0.001 ).
Table 1.
Socio-demographic characteristics of the participants
| Parameters | Total sample (n = 829) | International students | Chinese students | x2/t/z |
|---|---|---|---|---|
| Age | 23.04 ± 3.30 | 22.95 ± 3.90 | 21.63 ± 2.77 | t = −6.49* |
| Gender | ||||
| Female | 498(60.1%) | 221 (68%) | 277(55%) | ×2 = 14.00* |
| Male | 331 (39.9%) | 104 (32%) | 227(45%) | |
| BMI | ||||
| < 18.5 | 74 (8.9%) | 32 (9.8%) | 42 (8.3%) | ×2 = 21.03* |
| 18.6–24.9 | 596 (71.9%) | 256 (78.8%) | 340 (67.5%) | |
| 25.0–29.9 | 119 (14.4%) | 27 (8.3%) | 92 (18.3%) | |
| ≥ 30 | 40 (4.8%) | 10(3.1%) | 30 (6.0%) | |
| Level of Education | ||||
| Sophomore/freshman year | 628 (77.0%) | 245(75.4%) | 393 (78.0%) | ×2 = 23.04* |
| Senior year | 168(20.25%) | 60(18.5%) | 108(21.4%) | |
| Post-graduate | 23(2.8%) | 20 (6.2%) | 3(0.6) | |
| Students’ major | ||||
| Medical | 653(78.8%) | 298(91.7% | 355(70.4%) | ×2 = 53.38* |
| Non-Medical | 176(21.2%) | 27(8.3%) | 149(29.6%) | |
| Smoking Status | ||||
| Current Smoker | 73 (8.8%) | 59 (18.2%) | 14 (2.8%) | ×2 = 58.172* |
| Non-smoker | 756 (91.2%) | 266 (81.8%) | 490 (97.2%) | |
| Alcohol Consumption | ||||
| drinker | 254 (30.6%) | 141(43.60%) | 113(22.4%) | ×2 = 40.862* |
| Non-drinker | 575 (69.4%) | 184 (56.40%) | 391 (77.6%) | |
| Financial Status (RMB) | ||||
| ≤ 1000 | 221(26.7%) | 104 (32.0%) | 117(23.3%) | ×2 = 52.23* |
| 1000 ~ 2000 | 464(56.0%) | 203 (62.5%) | 261(51.9%) | |
| > 2000 | 143 (17.3%) | 18 (5.5%) | 126 (24.9%) | |
| Length of stay in Dalian (yrs.) | 1(1) | 2.0 (1.00) | z = −1.202* | |
*P ≤ 0.05
Health-promoting lifestyle (HPL) of college students in Dalian City, China
Average total HPLP-II scores for the Chinese and international group are shown in Fig. 2. For international students, the overall mean score was 2.44 ± 0.42, and the subscale mean scores ranged from 2.16 ± 0.43 to 2.75 ± 0.55. For Chinese students, the overall mean score was 2.74 ± 0.44, and subscale means scores ranged from 2.30 ± 0.61 to 3.00 ± 0.52. The Chinese students had significantly higher scores than the international on the average total HPLP-II (P < 0.001) and for each of the subscales (P < 0.050) (Table 2).
Fig. 2.
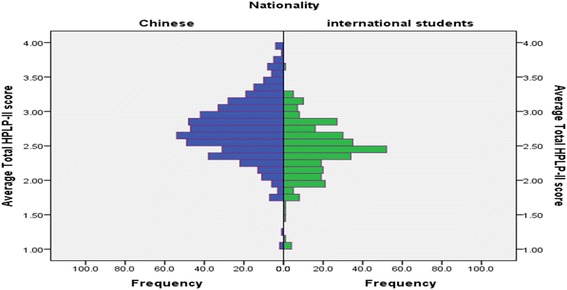
A graphical comparison on HLPLP-scores between the Chinese and international students in Dalian City, China
Table 2.
Effects of socio-demographic characteristics on the health-promoting lifestyle (HPL) in Dalian City, China
| Socio-demographic characteristics | Total HPLP-II Mean ± SD | HR Mean ± SD | SG Mean ± SD | PA Mean ± SD | Nutrition Mean ± SD | IR Mean ± SD | SM Mean ± SD |
|---|---|---|---|---|---|---|---|
| Gender | |||||||
| Female | 2.63 ± 0.47 | 2.28 ± .59 | 2.24 ± .60 | 2.33 ± 0.58 | 2.68 ± 0.60 | 2.89 ± 0.58 | 2.38 ± 0.50 |
| Male | 2.65 ± 0.40 | 2.24 ± 0.57 | 2.88 ± 0.54 | 2.34 ± 0.57 | 2.74 ± 0.55 | 2.89 ± 0.49 | 2.40 ± 0.47 |
| t | −.487 | 1.12 | −.395 | −1.408 | −1.11 | −.079 | −.398 |
| P value | 0.616 | 0.264 | 0.267 | 0.694 | 0.160 | 0.937 | 0.688 |
| 95% CI | -0.08 ~ .05 | −0.04 ~ .13 | −0.13 ~ 0.03 | −0.10 ~ 0.07 | −0.14 ~ 0.02 | −0.08 ~ 0.07 | −0.08 ~ 0.05 |
| Eta squared | 0.000 | 0.002 | 0.001 | 0.001 | 0.002 | 0.000 | 0.000 |
| BMI | |||||||
| < 18.5 | 2.60 ± 0.51 | 2.62 ± 0.63 | 2.85 ± 0.65 | 2.34 ± 0.51 | 2.62 ± 0.63 | 2.85 ± 0.69 | 2.41 ± 0.56 |
| 18.6 - 24.9 | 2.64 ± 0.44 | 2.70 ± 0.59 | 2.92 ± 0.57 | 2.32 ± 0.58 | 2.70 ± 0.59 | 2.90 ± 0.53 | 2.39 ± 0.48 |
| 25.0 - 29.9 | 2.64 ± 0.39 | 2.79 ± 0.53 | 2.85 ± 0.55 | 2.35 ± 0.57 | 2.79 ± 0.54 | 2.86 ± 0.52 | 2.39 ± 0.46 |
| ≥ 30 | 2.69 ± 0.54 | 2.74 ± 0.64 | 2.91 ± 0.63 | 2.44 ± 0.69 | 2.74 ± 0.63 | 2.86 ± 0.65 | 2.37 ± 0.64 |
| F | 0.288 | 1.042 | 0.529 | 0.614 | 1.410 | 0.264 | 0.040 |
| P Value | 0.834 | 0.373 | 0.662 | 0.606 | 0.239 | 0.852 | 0.989 |
| Eta squared | 0.001 | 0.004 | 0.002 | 0.002 | 0.005 | 0.000 | 0.000 |
| Level of education | |||||||
| Sophomore/Freshman year | 2.63 ± 0.44 | 2.22 ± 0.57 | 2.90 ± 0.57 | 2.32 ± 0.58 | 2.70 ± 0.59 | 2.89 ± 0.55 | 2.38 ± 0.49 |
| Senior Year | 2.70 ± .45 | 2.43 ± .58 | 2.90 ± .61 | 2.40 ± .55 | 2.76 ± .58 | 2.91 ± .54 | 2.44 ± .48 |
| Post graduate | 2.47 ± 37 | 2.35 ± .51 | 2.82 ± .50 | 2.22 ± .57 | 2.40 ± 0.39 | 2.59 ± 0.46 | 2.14 ± 0.29 |
| F | 3.061 | 8.401 | 0.166 | 1.523 | 3.125 | 2.934 | 0.040 |
| P value | 0.047 | 0.000 | 0.847 | 0.219 | 0.044 | 0.054 | 0.989 |
| Eta squared | 0.008 | 0.021 | 0.000 | 0.004 | 0.008 | 0.007 | 0.000 |
| Students’ major | |||||||
| Medical | 2.60 ± 0.43 | 2.25 ± 0.55 | 2.87 ± 0.56 | 2.30 ± 0.55 | 2.67 ± 0.58 | 2.85 ± 0.53 | 2.36 ± .49 |
| Non-medical | 2.75 ± 0.49 | 2.33 ± .66 | 2.99 ± .62 | 2.44 ± .65 | 2.85 ± .60 | 3.03 ± 0.58 | 2.50 ± 0.48 |
| t | −3.895 | −1.62 | −2.62 | −3.65 | −2.46 | −3.95 | −3.68 |
| P value | 0.000 | 0.100 | 0.014 | 0.009 | 0.000 | 0.000 | 0.000 |
| 95% CI | −.22 ~ −0.07 | −0.19 ~ 0.02 | −0.22 ~ −0.02 | −0.25 ~ −0.03 | −0.28 ~ −0.09 | −0.27 ~ −0.09 | −0.23 ~ −0.07 |
| Eta squared | 0.019 | 0.003 | 0.003 | 0.003 | 0.005 | 0.019 | 0.017 |
| Smoking status | |||||||
| Current smoker | 2.48 ± 0.42 | 2.30 ± 0.54 | 2.68 ± 0.52 | 2.33 ± 0.54 | 2.46 ± 0.50 | 2.65 ± 0.54 | 2.22 ± 0.47 |
| Non-smoker | 2.65 ± 0.44 | 2.26 ± 0.58 | 2.92 ± 0.58 | 2.33 ± 0.58 | 2.73 ± 0.59 | 2.91 ± 0.54 | 2.41 ± 0.49 |
| t | −3.161 | 0.444 | −3.412 | 0.013 | −3.797 | −3.822 | −3.161 |
| P value | 0.002 | 0.657 | 0.001 | 0.990 | 0.000 | 0.000 | 0.002 |
| 95% CI | -0.28 ~ −0.07 | −0.11 ~ 0.17 | −0.38 ~ −0.10 | −0.14 ~ 0.14 | −0.41 ~ −0.13 | −0.39 ~ −0.12 | −0.28 ~ −0.07 |
| Eta squared | 0.012 | 0.000 | 0.014 | 0.000 | 0.018 | 0.005 | 0.012 |
| Alcohol consumption | |||||||
| drinker | 2.56 ± 0.42 | 2.19 ± 0.56 | 2.80 ± 0.57 | 2.35 ± 0.55 | 2.58 ± 0.53 | 2.79 ± 0.52 | 2.33 ± 0.46 |
| Non-drinker | 2.67 ± 0.45 | 2.30 ± 0.59 | 2.94 ± 0.57 | 2.32 ± 0.59 | 2.76 ± 0.60 | 2.93 ± 0.55 | 2.42 ± 0.50 |
| t | −3.335 | −2.312 | −3.242 | 0.642 | −3.824 | −3.357 | −2.185 |
| P value | 0.001 | 0.021 | 0.001 | 0.521 | 0.000 | 0.001 | 0.029 |
| 95% CI | -0.18 ~ −0.05 | −0.19 ~ −0.02 | −0.23 ~ −0.06 | −0.06 ~ 0.12 | −0.26 ~ −0.08 | −0.22 ~ −0.06 | −0.16 ~ −0.01 |
| Eta squared | 0.014 | 0.007 | 0.013 | 0.000 | 0.018 | 0.014 | 0.006 |
| Financial status | |||||||
| ≤ 1000 | 2.63 ± .49 | 2.24 ± .58 | 2.91 ± .66 | 2.34 ± .61 | 2.66 ± .63 | 2.92 ± .58 | 2.39 ± .54 |
| 1000 ~ 2000 | 2.65 ± .43 | 2.29 ± .59 | 2.91 ± .54 | 2.34 ± .57 | 2.72 ± .57 | 2.88 ± .54 | 2.40 ± .45 |
| > 2000 | 2.62 ± .43 | 2.23 ± .55 | 2.85 ± .55 | 2.30 ± .57 | 2.75 ± .58 | 2.86 ± .53 | 2.35 ± .50 |
| F | 0.229 | 0.762 | 0.549 | 0.212 | 0.983 | 0.657 | 0.499 |
| P value | 0.795 | 0.467 | 0.578 | 0.809 | 0.375 | 0.519 | 0.607 |
| Eta squared | 0.000 | 0.002 | 0.001 | 0.000 | 0.000 | 0.002 | 0.001 |
| Nationality | |||||||
| Chinese | 2.74 ± 0.44 | 2.30 ± 0.61 | 2.98 ± 0.57 | 2.38 ± 0.60 | 2.92 ± 0.54 | 3.00 ± 0.52 | 2.53 ± 0.47 |
| International | 2.44 ± 0.42 | 2.21 ± 0.52 | 2.75 ± 0.55 | 2.24 ± 0.52 | 2.34 ± 0.47 | 2.68 ± 0.52 | 2.16 ± 0.43 |
| P value | 0.000 | 0.030 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| 95% CI | 0.24 ~ 0.36 | 0.01 ~ 0.17 | 0.15 ~ 0.31 | 0.06 ~ 0.23 | 0.51 ~ 0.66 | 0.15 ~ .25 | 0.30 ~ 0.43 |
| Eta squared | 0.113 | 0.006 | 0.037 | 0.015 | 0.257 | .083 | 0.136 |
Socio-demographic characteristics and HPL of college students in Dalian City China
Overall, the average total HPLP-II score was substantially related to the level of education, smoking status, and type of institution. Healthy behaviors were observed among the senior year students (mean = 2.70, P = 0.050), non-smokers (mean = 2.65, P = 0.020), non-drinkers (mean = 2.67, P = 0.010) and in non-medical students (mean = 2.75, P < 0.001). According to HPLP-II subscales with health responsibility as the dependent variable, the highest scores were observed among senior year students (mean = 2.43, P < 0.001) and non-drinkers (mean = 2.30, P = 0.020). With spiritual growth as the dependent variable, the highest scores were observed among the non-medical students (mean = 2.99, P = 0.014), non-smokers (mean = 2.92, P = 0.00) and non-drinkers (mean = 2.94, P = 0.010). In physical activity subscale, non-medical students reported significantly higher scores (mean = 2.44, P = 0.009) than their medical counterparts. With nutrition subscale as the dependent variable, the highest scores were observed among non-medical students (mean = 2.85, P = 0.00,) non-drinkers (mean = 2.76, P < 0.001) and non-smokers (mean = 2.73, P = 0.00). In relation to interpersonal relations subscale: the highest scores were observed among non-medical students (mean = 3.03, P < 0.001), non-smokers (mean = 2.91 ± .54, P = 0.00) and non-drinkers (mean = 2.94, P = 0.00). In stress management subscale, better stress management strategies were observed among the non-medical (mean = 2.50, P < 0.001) and non-smokers students (mean = 2.41, P < 0.001) (Table 2).
Comparison of self-rated health of between the Chinese and international students
The Chinese students had significantly higher scores than the international in societal health subscale (P < 0.001) whereas the international students had significantly higher scores than their Chinese counterparts in the physical health subscale (P < 0.001). There was no significant difference in the mean score of psychological health subscale between the two groups (P = 0.217) (Table 3).
Table 3.
Self-rated health (SRH) status of college students in Dalian City, China
| Socio-demographic characteristics | Physical health ± SD | Psychological health ± SD | Social health ± SD |
|---|---|---|---|
| Gender | |||
| Female | 68.30 ± 9.89 | 66.51 ± 13.53 | 65.52 ± 15.21 |
| Male | 66.48 ± 10.02 | 64.78 ± 12.40 | 64.70 ± 13.91 |
| t | 2.545 | 1.84 | 0.776 |
| P value | 0.011 | 0.067 | 0.438 |
| 95% CI | 0.42 ~ 3.24 | −0.12 ~ 3.58 | −1.27 ~ 2.90 |
| Eta squared | 0.008 | 0.004 | 0.000 |
| BMI | |||
| < 18.5 | 69.19 ± 9.70 | 68.46 ± 11.87 | 67.18 ± 15.38 |
| 18.6 - 24.9 | 68.29 ± 9.99 | 66.65 ± 13.17 | 65.63 ± 14.60 |
| 25.0 - 29.9 | 63.27 ± 9.28 | 61.22 ± 11.97 | 62.81 ± 14.23 |
| ≥ 30 | 66.64 ± 9.14 | 62.28 ± 14.28 | 61.99 ± 15.45 |
| F | 9.201 | 7.585 | 2.232 |
| P Value | 0.000 | 0.000 | 0.083 |
| Eta squared | 0.033 | 0.03 | 0.000 |
| Level of education | |||
| Freshman year/sophomore | 67.36 ± 9.93 | 65.64 ± 13.36 | 64.31 ± 14.96 |
| Senior year | 67.32 ± 9.65 | 66.15 ± 12.31 | 68.07 ± 12.57 |
| Post-graduate | 76.79 ± 10.61 | 68.98 ± 11.30 | 69.60 ± 14.96 |
| F | 8.008 | 0.637 | 5.104 |
| P value | 0.000 | 0.529 | 0.006 |
| Eta squared (h2) | 0.012 | 0.000 | 0.013 |
| Students’ major | |||
| Medical | 67.59 ± 10.20 | 65.35 ± 13.06 | 64.41 ± 14.75 |
| Non-medical | 67.49 ± 9.16 | 67.46 ± 13.17 | 67.97 ± 14.19 |
| t | 0.112 | 0.709 | −2.85 |
| P value | 0.911 | 0.100 | 0.005 |
| 95% CI | -1.58 ~ 1.77 | −4.31 ~ .09 | --6.02 ~ −1.10 |
| Eta squared | 0.00 | 0.00 | 0.01 |
| Smoking status | |||
| Current smoker | 68.48 ± 7.32 | 64.76 ± 13.68 | 58.85 ± 18.18 |
| Non-smoker | 67.48 ± 10.20 | 65.92 ± 13.05 | 65.82 ± 14.16 |
| t | 0.814 | −0.718 | −3.880 |
| P value | 0.416 | 0.473 | 0.000 |
| 95% CI | -1.4 ~ 3.42 | −4.34 ~ 2.02 | −10.51 ~ −3.45 |
| Eta squared | 0.002 | 0.000 | 0.019 |
| Alcohol consumption | |||
| Drinker | 68.12 ± 10.26 | 65.35 ± 12.83 | 63.89 ± 15.09 |
| Non-drinker | 67.32 ± 9.85 | 66.02 ± 13.23 | 65.75 ± 14.50 |
| t | 1.042 | −0.662 | −1.648 |
| P value | 0.298 | .508 | 0.100 |
| 95% CI | -0.71 ~ 2.31 | −2.65 ~ 1.31 | −4.08 ~ .36 |
| Eta squared | 0.00 | 0.007 | 0.013 |
| Financial status | |||
| ≤ 1000 | 68.86 ± 9.89 | 68.35 ± 13.75 | 66.95 ± 14.71 |
| 1000 ~ 2000 | 67.83 ± 10.31 | 65.7564 ± 13.15 | 64.8711 ± 15.03 |
| > 2000 | 64.79 ± 18.52 | 62.1332 ± 11.04 | 63.5172 ± 13.42 |
| F | 7.578 | 9.795 | 2.566 |
| P value | 0.001 | 0.000 | 0.077 |
| Eta squared | 0.019 | 0.0204 | 0.006 |
| Nationality | |||
| Chinese | 65.03 ± 8.01 | 66.25 ± 12.99 | 66.5289 ± 12.43 |
| International | 71.89 ± 11.41 | 65.07 ± 13.29 | 62.9035 ± 17.68 |
| t | −9.10 | 1.234 | 3.105 |
| P value | 0.000 | 0.217 | 0.002 |
| 95% CI | -8.34 ~ −5.38 | −0.70 ~ 3.07 | 1.33 ~ 5.92 |
| Eta squared | 0.094 | 0.002 | 0.012 |
Socio-demographic characteristics and SRH of college students in Dalian City, China
Physiological health
The score of physiological subscale was significantly related to BMI, level of education, and financial status. Students with low BMI perceived their physiological health better than those with high BMI. Students in lower to moderate financial status perceived their health status better than those in high financial status (Table 3).
Psychological health
The score of psychological subscale was significantly related to BMI, and financial status (Table 3).
Social health
The score of social subscale was significantly related to type of institution, smoking status and level of education (Table 3).
Individual factors predicting health promoting lifestyle
Table 4 indicates that financial status negatively predicted health-promoting lifestyle among the Chinese students yielding low (adjusted R2 = 0.014) predictive explanatory power. In the international group, HPL was significantly associated with students’ major (adjusted R2 = 0.035), age (adjusted R2 =0.052) and level of education (adjusted R2 = 0.061).
Table 4.
Stepwise multiple regression predictors of HPL among college students, at Dalian city, China
| Group | Variable | B | SD Error | β | t | p | Tolerance | Variance inflation Factor |
|---|---|---|---|---|---|---|---|---|
| Chinese students | Financial status >2000 RMB | -0.128 | 0.045 | −0.126 | −2.838 | 0.005 | 0.984 | 1.016 |
| International students | Age | 0.028 | 0.007 | 0.240 | 4.021 | 0.000 | 0.893 | 1.120 |
| Student major | 0.180 | 0.077 | 0.0132 | 2.339 | 0.020 | 0.995 | 1.005 | |
| Level of education (post-graduate) | −0.209 | 0.105 | −0.119 | −1.988 | 0.048 | 0.889 | 1.125 |
Individual factors predicting self-rated health status
Table 5 shows the association between the individual factors and the three dimensions of SHMS V1.0.
Table 5.
Stepwise multiple regression predictors of HPL among college students
| Group | SHMV1.0 domain | Predictor | B | SD Error | β | t | p | Tolerance | VIF |
|---|---|---|---|---|---|---|---|---|---|
| Chinese | Physiological Health | BMI-24 ~ 27 | −3.633 | 0.916 | −0.174 | −3.966 | 0.000 | 1.000 | 1.000 |
| Financial status ≤1000RMB | -1.92 | 0.704 | −0.119 | −2.73 | 0.007 | 0.997 | 1.000 | ||
| Psychological Health | Financial status ≥2000 | −4.147 | 1.357 | −0.138 | −3.055 | 0.002 | 0.870 | 1.150 | |
| BMI = 25-29.9 | −4.363 | 1.484 | −0.129 | −2.940 | 0.003 | 0.917 | 1.091 | ||
| Financial status ≤1000 | 4.793 | 1.370 | 0.156 | 3.499 | 0.001 | 0.893 | 1.119 | ||
| Smoking status | 9.267 | 3.462 | 0.113 | 2.677 | 0.008 | 0.992 | 1.009 | ||
| Gender | −2.795 | 1.150 | −0.107 | −2.430 | 0.015 | 0.914 | 1.094 | ||
| Social Health | Financial status ≤1000 | 4.592 | 1.297 | 0.156 | 3.540 | 0.000 | 0.994 | 1.006 | |
| BMI = 25-29.9 | −2.880 | 1.424 | −0.089 | −2.023 | 0.044 | 0.994 | 1.006 | ||
| International students | Physiological health | BMI = 25-29.9 | −4.687 | 2.360 | −0.112 | −1.986 | 0.048 | 0.996 | 1.004 |
| Age | 0.566 | .195 | 0.164 | 2.896 | 0.004 | 0.989 | 1.012 | ||
| Students’ major(medical) | 5.368 | 2.274 | 0.133 | 2.360 | 0.019 | 0.997 | 1.003 | ||
| Smoking (smoker) | −3.574 | 1.629 | −0.125 | −2.194 | 0.029 | 0.988 | 1.012 | ||
| Psychological health | BMI = 25-29.9 | −6.083 | 2.806 | −0.125 | −2.168 | 0.031 | 0.925 | 1.081 | |
| Gender | 4.115 | 1.636 | 0.145 | 2.516 | 0.012 | 0.926 | 1.080 | ||
| Age | 0.984 | 0.223 | 0.245 | 4.413 | 0.000 | 0.997 | 1.003 | ||
| Students’ major(medical) | 6.290 | 2.607 | 0.134 | 2.413 | 0.016 | 0.997 | 1.003 | ||
| Social health | Level of Education (Senior students) | −10.95 | 2.291 | −0.262 | −4.778 | 0.000 | 0.992 | 1.008 | |
| Smoking (smoker) | −7.494 | 2.441 | −0.168 | −3.070 | 0.002 | 0.991 | 1.010 | ||
| Students’ Major (medical) | 9.827 | 3.409 | 0.158 | 2.883 | 0.004 | 0.999 | 1.001 |
Physiological health
Physiological health among the Chinese students was negatively and positively associated with BMI (adjusted R2 =0.029) and financial status (adjusted R2 = 0.040). Besides, BMI (adjusted R2 = 0.025), age (adjusted R2 = 0.038) students’ major (adjusted R2 = 0.051), and smoking (adjusted R2 = 0.061) emerged as strong predictors of physiological health among the international students.
Psychological health
Financial status >2000 (adjusted R2 = 0.045), BMI = 25.0 - 29.9 (adjusted R2 =0.068), financial status ≤1000 (adjusted R2 = 0.089), smoking (adjusted R2 =0.100), and gender (adjusted R20 = .109), predicted psychological health among the Chinese students. BMI = 25.0 - 29.9 (adjusted R2 = 0.056), gender adjusted (R2 = 0.069), age adjusted R2 =0.078), and students’ major (adjusted R2 =0.090), predicted psychological health among international students.
Societal health
Financial status ≤1000 (adjusted R2 =0.025) and BMI = 25-29.9 (adjusted R2 = 0.031) emerged as the predictors for social health among the Chinese students. Bachelors education (adjusted R2 = 0.074), smoking (adjusted R2 = 0.097) and students’ major (adjusted R2 = 0.119), emerged as strong predictors for social health in the international group.
Relationship between health-promoting behaviors and SRH status among college students in Dalian City, China
Total HPLP-II and all its subscales were correlated with the three SHMS V1.0 sub-scales among the Chinese college students. Physiological health (r = 0.34, P < 0.001), psychological health (r = 0.44, P < 0.001) and societal health (r = 0.48, P < 0.001) had a moderate to strong positive relationship with the average total HPLP-II score. In the international group, the average total HPLP-II correlated with the psychological health (r = 0.27, P < 0.001) and societal health (r = 0.296, P < 0.001). There was no significant association between the physiological health and the average total HPLP-II (P = 0.372) in the international group. Table 6 summarizes the correlation between HPLP-II score and SHMS V1.0 sub scales. Figure 3 shows a scatterplot of social health and HPLP-II score among the college students in Dalian City, China as an example that illustrates the strength of the positive relationships between the two variables (Table 6).
Table 6.
Correlation between HPLP-II dimensions and SRH status among college students in Dalian City, China. (n = 829)
| Variables | Physical Health | Psychological Health | Social Health | |||
|---|---|---|---|---|---|---|
| r | P | r | P | r | P | |
| Chinese group (N = 504) | ||||||
| Health R | 0.193 | 0.000 | 0.222 | 0.000 | 0.246 | 0.000 |
| Spiritual Growth | 0.328 | 0.000 | 0.434 | 0.000 | 0.453 | 0.000 |
| Physical Activity | 0.246 | 0.000 | 0.296 | 0.000 | 0.274 | 0.000 |
| Nutrition | 0.240 | 0.000 | 0.320 | 0.000 | 0.342 | 0.000 |
| Interpersonal R | 0.307 | 0.000 | 0.433 | 0.000 | 0.537 | 0.000 |
| Stress Management | 0.300 | 0.000 | 0.387 | 0.000 | 0.409 | 0.000 |
| Total HPLP-II Score | 0.341 | 0.000 | 0.440 | 0.000 | 0.478 | 0.000 |
| International group (N = 296) | ||||||
| Health R | −0.161 | 0.006 | 0.063 | 0.000 | 0.067 | 0.253 |
| Spiritual Growth | 0.272 | 0.000 | 0.406 | 0.000 | 0.397 | 0.000 |
| Physical Activity | −0.038 | 0.519 | 0.111 | 0.056 | 0.052 | 0.371 |
| Nutrition | −0.081 | 0.167 | 0.162 | 0.050 | 0.147 | 0.012 |
| Interpersonal Relations | 0.198 | 0.010 | 0.339 | 0.000 | 0.440 | 0.000 |
| Stress Management | 0.047 | 0.424 | 0.162 | 0.000 | 0.218 | 0.000 |
| Total HPLP-II Score | 0.052 | 0.372 | 0.270 | 0.000 | 0.296 | 0.000 |
Fig. 3.
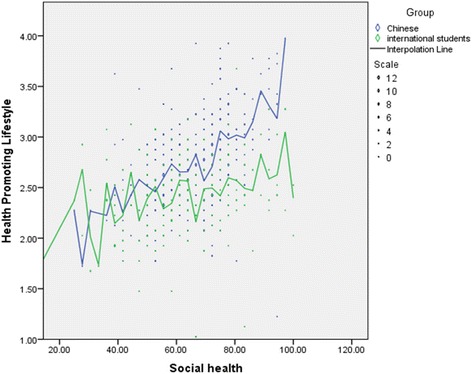
A scatterplot of social health and HPLP-II score in the Chinese and the international group
The logistic regression analysis was performed to assess the influence of HPL dimensions on SRH status which was a dichotomous outcome (Healthy and Sub-Optimal health status). The model contained six HPLP-II dimensions and adjusted for socio-demographic factors. The full model containing all the predictors was statistically significant X2 (17, N = 781) = 124.34, P < 0.001), indicating that the model was able to distinguish the respondents who were in healthy and Sub-Optimal Health Status. The model as a whole explained between 14.7% (Cox and Snell R square) and 20.4% (Nagelkerke R Square) of the variance in SRH status and correctly classified 69.3% of the cases. As shown in the Table 7, three of the HPLP-II dimensions made a statistically significant contribution to the model (physical activity, nutrition, and interpersonal relations). Based on overall lifestyle evaluations, compared with the participants with a healthy lifestyle, after demographic adjustment, subjects with a “moderate” lifestyle were at a 4.5 times at risk of developing SHS (OR: 4.5, 95% CI: 2.0–9.90) and those with a “good” lifestyle were at a 3.3 times higher risk of SHS (OR: 3.3, 95%CI: 1.500–7.18). Good and moderate HPLP-II levels of nutrition are associated with low risk of suboptimal health status (OR: 0.41 and 0.25, respectively). Participants in good and moderate HPLP-II levels of interpersonal relations are associated with higher risk of suboptimal health (OR:2.7 and 3.01, respectively) than those in excellent levels of HPLP-II (Table 7).
Table 7.
Associations between health status and health-promoting lifestyle
| Health promoting life profile | Healthy | SHS | 95% Confidence Interval | |||
|---|---|---|---|---|---|---|
| N | N | OR* | Lower Limit | Upper Limit | P | |
| Overall Evaluation | ||||||
| Poor (13) | 12 | 1 | 0.591 | 0.066 | 5.332 | 0.640 |
| Moderate (296) | 176 | 120 | 4.508 | 2.034 | 9.990 | 0.000 |
| Good (456) | 303 | 153 | 3.282 | 1.500 | 7.180 | 0.003 |
| Excellent Refa (64) | 56 | 8 | 0.000 | |||
| Health Responsibility | ||||||
| Poor (72) | 38 | 34 | 6.55 | 0.683 | 62.884 | 0.100 |
| Moderate (481) | 320 | 161 | 3.89 | 0.432 | 35.066 | 0.220 |
| Good (253) | 167 | 86 | 5.29 | 0.597 | 46.866 | 0.130 |
| Excellent Refa(23) | 22 | 1 | 0.080 | |||
| Spiritual Growth | ||||||
| Poor (14) | 13 | 1 | 0.33 | 0.035 | 3.214 | 0.340 |
| Moderate (160) | 81 | 79 | 3.92 | 1.797 | 8.557 | 0.000 |
| Good(531) | 352 | 179 | 1.61 | 0.845 | 3.079 | 0.150 |
| Excellent Refa (124) | 101 | 23 | 0.000 | |||
| Physical Activity | ||||||
| Poor (46) | 29 | 17 | 2.09 | 0.402 | 10.821 | 0.380 |
| Moderate (451) | 272 | 179 | 2.5 | 0.573 | 10.933 | 0.220 |
| Good (302) | 219 | 83 | 1.36 | 0.321 | 5.794 | 0.670 |
| Excellent refa (30) | 27 | 3 | 0.020 | |||
| Nutrition | ||||||
| Poor (16) | 15 | 1 | 0.03 | 0.003 | 0.391 | 0.010 |
| Moderate (295) | 198 | 97 | 0.25 | 0.109 | 0.583 | 0.000 |
| Good (445) | 283 | 162 | 0.41 | 0.192 | 0.882 | 0.020 |
| Excellent refa (73) | 51 | 22 | 0.002 | |||
| Interpersonal Relations | ||||||
| Poor (8) | 7 | 1 | 9.47 | 0.374 | 23.798 | 0.170 |
| Moderate(185) | 115 | 70 | 2.7 | 1.100 | 6.659 | 0.030 |
| Good (543) | 342 | 201 | 3.01 | 1.389 | 6.515 | 0.010 |
| Excellent Refa (93) | 82 | 11 | 0.040 | |||
| Stress Management | ||||||
| Poor (10) | 9 | 1 | 0.51 | 0.580 | 3.364 | 0.64 |
| Moderate(260) | 162 | 98 | 1.4 | 0.623 | 2.988 | 0.46 |
| Good (478) | 310 | 168 | 1.36 | 0.931 | 1.075 | 0.44 |
| Excellent Ref a(81) | 66 | 15 | 0.764 | |||
aDemographic variables adjusted for included age, gender, BMI, education level, drinking, Smoking, Financial Status
Refa is the reference group
Discussion
The HPLP-II scores indicated that both the Chinese and the international students practiced healthy behaviors in this study. However, there was a significant difference in the overall HPLP-II mean score and in all the subscales between the two groups. Chinese students practice healthy behaviors more than international students. This could be attributed to the fact that Chinese culture favors Chinese students in all aspects of health-promoting lifestyle. Culture influences the value placed on health and health-promoting lifestyles [17]. Furthermore, Chinese students are not only aware of socio-cultural activities but also access support and motivation from family/friends that might encourage them to pay more attention to adopting a healthy lifestyle [27]. On the contrary, the international students’ unfamiliarity with the environmental/social differences and the health care services in China might negatively affect their participation in an HPL.
Notably, our findings also indicated that the two groups differed in the least adopted health-promoting behaviors. The lowest subscale in the Chinese group was health responsibility. This finding is consistent with those of previous studies in China [7, 28]. The lowest subscale in the international group was observed in the stress management. Our finding is consistent with those of previous studies [29]. International students process and manage their daily requirements through financial expenses (e.g. ordering food and beverages through phone calls, hiring private taxi drivers for shopping and moving around the school etc.), which eventually lead to unworthy expenses, poor lifestyle, and private life. Stress management involves one’s ability to change a stressful situation, deal with problems, take care of themselves, and make time for rest and relaxation. Previous research has proposed that it is not the presence of stressors but rather inability to cope effectively with stressful situations that have unfavorable consequences for health status [30]. Therefore, the universities should encourage international students and Chinese to participate in common extracurricular activities within the university to empower their social life in order to cope effectively with stressful situations.
Individual factors have been shown to influence health promotion and lifestyle [31–33]. This current study found that international post-graduate medical students engaged less frequently in HPL. Our findings contradict the findings reported by Wang et al. [34]. A medical degree is often regarded as a particularly demanding program. Most medical students almost entirely spend time to study with very little time left for relaxation and co-curriculum activities. Relaxation techniques have proven to be particularly an effective stress management intervention in (medical) student populations [35].
Risk behaviors, particularly smoking was found to be higher in international students and was negatively associated with their physiological and social health. This could be attributed to poor stress management strategies and less interaction with their environment. Social deinstitutionalization can keep international students constantly to interact with their devices (smartphones or computers) which may consequently lead to less physical activity.
Though the Chinese student’s group had lower BMI than international students, high BMI score and high financial status were negatively associated with physiological and psychological health status. Impaired body image concerns a person’s perception, feelings, and thoughts about his or her body can prevent the exposure and participation in the health promoting activities, particularly physical activity. Poor self-image and a low self-esteem can lead to low degree of satisfaction about oneself in terms of size, shape and general appearance among overweight/obese students [36]. Thus, the psychological instability that associates with body shape and size may contribute to the physical inactivity, social withdrawal, and sub optimal health status. Overweight/obesity may lead to some risk factors of cardiovascular and metabolic derangements such as an increase in elevated blood pressure and blood lipid profiles. Also, the literature shows that the students with higher income levels had increased dietary intake; which may promote the risk of gaining weight and high risk of suboptimal health. The Chinese students who had lower BMI and financial status perceived health better than other Chinese students in this study. A university-based health education program aimed at promoting healthy lifestyles and engaging students in regular medical check-ups are needed to prevent cardio-metabolic risks among the Chinese students.
This study found that good and moderate HPLP-II levels of interpersonal relations were associated with an increased risk of SHS. On the other hand, good and moderate HPLP-II levels of nutrition were associated with lower risk of suboptimal health status in the present study. This study merits further study to consider clinical and laboratory results such as blood pressure, electrocardiography (ECG), lipid profiles and glucose levels to identify the cardio-metabolic risks among the college students.
To the best of our knowledge, this is the first study reporting on the health-promoting lifestyle and self-rated health among college students in terms of differences between international and Chinese students. Therefore, it provides vital information related to health-promoting lifestyle to universities in China, to better support various students.
Certain limitations of the study should be taken into account, especially its cross-sectional design, which limits any causal conclusions. In addition, the data were self-reported and questionnaires were available in only two languages (Chinese and English). To fully accommodate all international students, it would be of great interest to provide other language options. Data were based on self-reports, which are sensitive to social desirability biases meaning that social pressures might interfere with these results.
Conclusion
Collectively, these findings provide a convincing body of evidence to support the role of socio-cultural factors that affect the HPL and SRH of college students. Policy makers should be aware of socio-cultural influences when designing programs to promote health among students from different ethnic/group. Importantly, to reduce chronic illnesses more effectively and improve population health, health education programs should be planned to stimulate the interests of different students according to their socio-cultural characteristics.
Acknowledgement
The authors thank Miss. Kay Benson for editing and polishing the manuscript. We also thank all the participants for their enrollment in the study, and we appreciate our colleagues Joyce Apondi and Yazeed Jamalat for their support in data collection.
Funding
There was no funding available for this research.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available because a public use dataset has not been created yet, but are available from the corresponding author on reasonable request. Such requests would be subjected to the approval of the Scientific Ethics Committee of Dalian Medical University.
Authors’ contributions
Conceived and designed the research concept: LS, and XL. Analyzed data: LS and HT with input from XL. Contributed to the writing of the manuscript: LS, HT and XL. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The Scientific Research Ethics Committee of Dalian Medical University provided approval for the study. The consent to participate was given by the students by filling out the questionnaire.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- ANOVA
Analysis of variance
- BMI
Body mass index
- HPL
Health-promoting lifestyle
- HPLP-II
Health-promoting lifestyle profile II
- SHS
Suboptimal health status
- SHMS V1.0
Suboptimal health measurement scale version 1.0
- SRH
Self-rated health status
Contributor Information
Sainyugu Lolokote, Email: lolokotedr@outlook.com.
Tesfaldet Habtemariam Hidru, Email: tesfye1010@yahoo.com.
Xiaofeng Li, Email: lxf_chen@dmu.edu.cn.
References
- 1.Walker SN, Sechrist KR, Pender NJ. The health-promoting lifestyle profile: development and psychometric characteristics. Nurs Res. 1987;36(2):76–81. doi: 10.1097/00006199-198703000-00002. [DOI] [PubMed] [Google Scholar]
- 2.Ay S, et al. Health-promoting lifestyle behaviour for cancer prevention: a survey of Turkish university students. Asian Pac J Cancer Prev. 2012;13(5):2269–2277. doi: 10.7314/APJCP.2012.13.5.2269. [DOI] [PubMed] [Google Scholar]
- 3.Lee A, et al. Can health promoting schools contribute to the better health and wellbeing of young people? The Hong Kong experience. J Epidemiol Community Health. 2006;60(6):530–6. doi: 10.1136/jech.2005.040121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Liebergall-Wischnitzer M, Buyum M, Ganz FD. Health promoting lifestyle among Israeli adult survivors of childhood cancer. J Pediatr Oncol Nurs. 2016;33(2):146–154. doi: 10.1177/1043454215600177. [DOI] [PubMed] [Google Scholar]
- 5.Gokyildiz S, et al. Health-promoting lifestyle behaviours in pregnant women in Turkey. Int J Nurs Pract. 2014;20(4):390–397. doi: 10.1111/ijn.12187. [DOI] [PubMed] [Google Scholar]
- 6.Mozaffarian D, et al. Changes in diet and lifestyle and long-term weight gain in women and men. N Engl J Med. 2011;364(25):2392–2404. doi: 10.1056/NEJMoa1014296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bi, J.L., et al., Association of lifestyle factors and suboptimal health status: a cross-sectional study of Chinese students. BMJ Open, 2014. 4(6). [DOI] [PMC free article] [PubMed]
- 8.Kastorini CM, et al. The effect of Mediterranean diet on metabolic syndrome and its components: a meta-analysis of 50 studies and 534,906 individuals. J Am Coll Cardiol. 2011;57(11):1299–1313. doi: 10.1016/j.jacc.2010.09.073. [DOI] [PubMed] [Google Scholar]
- 9.Tran T, et al. The association of self-rated health and lifestyle behaviors among foreign-born Chinese, Korean, and Vietnamese Americans. Qual Life Res. 2013;22(2):243–252. doi: 10.1007/s11136-012-0155-1. [DOI] [PubMed] [Google Scholar]
- 10.Molarius A, et al. Socioeconomic conditions, lifestyle factors, and self-rated health among men and women in Sweden. Eur J Pub Health. 2007;17(2):125–133. doi: 10.1093/eurpub/ckl070. [DOI] [PubMed] [Google Scholar]
- 11.Kazemi DM, et al. Health behaviors of mandated and voluntary students in a motivational intervention program. Prev Med Rep. 2015;2:423–428. doi: 10.1016/j.pmedr.2015.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lee RLT, Loke AJTY. Health-promoting behaviors and psychosocial well-being of university students in Hong Kong. Public Health Nurs. 2005;22(3):209–220. doi: 10.1111/j.0737-1209.2005.220304.x. [DOI] [PubMed] [Google Scholar]
- 13.Lowry R, et al. Physical activity, food choice, and weight management goals and practices among US college students. Am J Prev Med. 2000;18(1):18–27. doi: 10.1016/S0749-3797(99)00107-5. [DOI] [PubMed] [Google Scholar]
- 14.Landsberg B, et al. Clustering of lifestyle factors and association with overweight in adolescents of the Kiel obesity prevention study. Public Health Nutr. 2010;13(10A):1708–1715. doi: 10.1017/S1368980010002260. [DOI] [PubMed] [Google Scholar]
- 15.Nelson MC, et al. Emerging adulthood and college-aged youth: an overlooked age for weight-related behavior change. Obesity (Silver Spring) 2008;16(10):2205–2211. doi: 10.1038/oby.2008.365. [DOI] [PubMed] [Google Scholar]
- 16.Hennock M. China rolls out the welcome mat for foreign students. 2012. [Google Scholar]
- 17.Chen MY, James K, Wang EK. Comparison of health-promoting behavior between Taiwanese and American adolescents: a cross-sectional questionnaire survey. Int J Nurs Stud. 2007;44(1):59–69. doi: 10.1016/j.ijnurstu.2005.11.015. [DOI] [PubMed] [Google Scholar]
- 18.Carpenter LJ, Garcia AA. Assessing outcomes of a study abroad course for nursing students. Nurs Educ Perspect. 2012;33(2):85–89. doi: 10.5480/1536-5026-33.2.85. [DOI] [PubMed] [Google Scholar]
- 19.Wang, D., X.H. Xing, and X.B. Wu, Healthy lifestyles of university students in China and influential factors. ScientificWorldJournal, 2013. 2013: p. 412950. [DOI] [PMC free article] [PubMed]
- 20.Schmid G, et al. Assessment of psychological aspects of somatofomi disorders: a study on the German version of the health attitude survey (HAS) Compr Psychiatry. 2014;55(1):155–164. doi: 10.1016/j.comppsych.2013.08.013. [DOI] [PubMed] [Google Scholar]
- 21.Schaefert R, et al. Non-specific, functional, and somatoform bodily complaints. Dtsch Arztebl Int. 2012;109(47):803–U46. doi: 10.3238/arztebl.2012.0803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Henningsen P, Zipfel S, Herzog W. Management of functional somatic syndromes. Lancet. 2007;369(9565):946–955. doi: 10.1016/S0140-6736(07)60159-7. [DOI] [PubMed] [Google Scholar]
- 23.Sullivan LM. Essentials of biostatistics in public health. 2. United States: JONES & BARTLETT LEARNING; 2011. p. 314. [Google Scholar]
- 24.Pinar R, Celik R, Bahcecik N. Reliability and construct validity of the health-promoting lifestyle profile II in an adult Turkish population. Nurs Res. 2009;58(3):184–193. doi: 10.1097/NNR.0b013e31819a8248. [DOI] [PubMed] [Google Scholar]
- 25.Al-Kandari F, Vidal VL, Thomas D. Health-promoting lifestyle and body mass index among College of Nursing students in Kuwait: a correlational study. Nurs Health Sci. 2008;10(1):43–50. doi: 10.1111/j.1442-2018.2007.00370.x. [DOI] [PubMed] [Google Scholar]
- 26.Pallant, J., SPSS survival manual: a step by step guide to data analysis using SPSS. 10 ed. 2007: Allen and Unwin.
- 27.Zhang Y, et al. Facilitators and barriers of adopting healthy lifestyle in rural China: a qualitative analysis through social capital perspectives. Nagoya J Med Sci. 2016;78(2):163–173. [PMC free article] [PubMed] [Google Scholar]
- 28.Chen J, et al. Associations between breakfast eating habits and health-promoting lifestyle, suboptimal health status in southern China: a population based, cross sectional study. J Transl Med. 2014;12:348. doi: 10.1186/s12967-014-0348-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Aqtash S, Van Servellen G. Determinants of health-promoting lifestyle behaviors among Arab immigrants from the region of the Levant. Res Nurs Health. 2013;36(5):466–477. doi: 10.1002/nur.21555. [DOI] [PubMed] [Google Scholar]
- 30.Cheng JR, et al. Self-Rated Health Status and Subjective Health Complaints Associated with Health-Promoting Lifestyles among Urban Chinese Women: A Cross-Sectional Study. Plos One. 2015;10(2).e0117940. [DOI] [PMC free article] [PubMed]
- 31.Nacar M, et al. Health promoting lifestyle behaviour in medical students: a multicentre study from Turkey. Asian Pac J Cancer Prev. 2014;15(20):8969–8974. doi: 10.7314/APJCP.2014.15.20.8969. [DOI] [PubMed] [Google Scholar]
- 32.Kim HJ, et al. Health-promoting lifestyle behaviors and psychological status among Arabs and Koreans in the United Arab Emirates. Res Nurs Health. 2015;38(2):133–141. doi: 10.1002/nur.21644. [DOI] [PubMed] [Google Scholar]
- 33.Kara B, İşcan B. Predictors of health behaviors in Turkish female nursing students. Asian Nursing Research. 10(1):75–81. [DOI] [PubMed]
- 34.Wang, D., X.-H. Xing, and X.-B. Wu, Healthy lifestyles of university students in China and influential factors. Sci World J, 2013. 2013: p. 412950. [DOI] [PMC free article] [PubMed]
- 35.Dehghan-nayeri N, Adib-Hajbaghery M. Effects of progressive relaxation on anxiety and quality of life in female students: a non-randomized controlled trial. Complementary. Ther Medicine. 19(4):194–200. [DOI] [PubMed]
- 36.Dreber H, et al. Who is the treatment-seeking young adult with severe obesity: a comprehensive characterization with emphasis on mental health. PLoS One. 2015;10(12):e0145273. doi: 10.1371/journal.pone.0145273. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available because a public use dataset has not been created yet, but are available from the corresponding author on reasonable request. Such requests would be subjected to the approval of the Scientific Ethics Committee of Dalian Medical University.