

Abstract
Fibrous dysplasia (FD) of the bone is characterized by the medullary cavity of bones becoming filled with fibrous tissue, and its etiology remains unknown. It is usually asymptomatic and found incidentally on imaging studies that are performed for other purposes. FD may closely mimic the appearance of bony metastatic disease on radiological examinations. We report the case of a 45-year-old female patient, which appeared to have multiple bone lesions on initial workup images. Subsequently, the bone lesions that showed increased FDG uptake on PET/CT in right femur and tibia were identified as FD. The present case is a useful addition to the current body of literature of false positive F-18 FDG PET/CT due to a benign skeletal pathology and underscores the importance of high index of suspicion and careful correlation, whenever one comes across such an unusual PET/CT finding.
Keywords: Fibrous dysplasia, polyostotic, mimick metastasis, FDG PET/CT
Introduction
Fibrous dysplasia (FD) of the bone is a slowly progressive bone disorder on which normal bone is replaced by abnormal fibro-osseous tissue.[1,2] The true incidence and prevalence rates of FD are difficult to estimate, but the lesions are not rare. The disease may involve single bone (monostotic-60%) or multiple bones (polyostotic-40%) with a predilection for the craniofacial bones, ribs, pelvis, and long bones.[3] Whole body F-18 flourodeoxyglucose PET/CT (FDG PET/CT) has been widely used in tumor imaging. Several FDG PET/CT reports suggested that the appearance of FD could mimic a malignant process. Therefore, this case was presented with the aim of guiding physicians in evaluating bone lesions.
Case Report
A 45-year-old female patient presented with pain in the right leg and x-ray tibia showed sclerotic areas with bony expansion. There is no history of any malignancy. She was referred for whole body bone scintigraphy, which showed intense uptake in shaft of right femur and tibia [Figure 1]. FDG PET/CT was done for detection of other site involvement and rule out primary malignancy. Whole body PET/CT showed intense tracer uptake in the right femur and tibia [Figure 2]. Fused FDG PET/CT and CT showed uptake in expansile, multifocal, endosteal scalloping soft tissue lesions “ground glass” pattern of the bone and surrounded by a distinct rim of reactive bone in the medullary cavity of right femur and tibia, with an SUV max of 8 to 10 [Figure 3], arrows. A diagnosis of polyostotic FD was made and she underwent internal fixation for both femur and tibia to prevent fracture.
Figure 1.
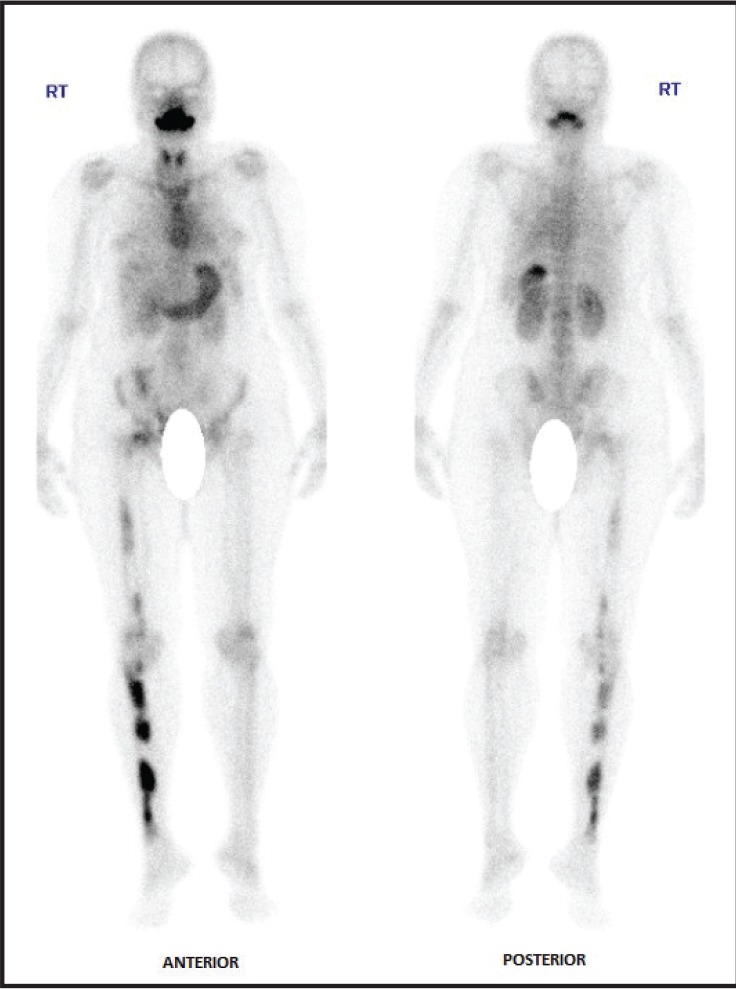
Whole body Tc99m-MDP bone scintigraphy image showing intense uptake in the right femur and tibia. Also thyroid and gastric muscosa due to free pertechnetate seen
Figure 2.

Whole body F-18 FDG PET/CT showing intense tracer uptake in the right femur and tibia. Mild degenrative heterogenity in vertebra and sacrum noted.
Figure 3.
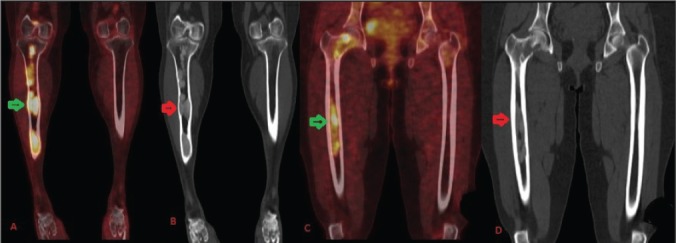
Coronal fused PET/CT (A and C, green arrows) and CT (B and D, red arrows) showed expansile, multifocal, endosteal scalloping soft tissue “ground glass” pattern of the bone and surrounded by a distinct rim of reactive bone in the medullary cavity of right femur and tibia, charecteristic of FD
Discussion
FD is a benign disorder of bone-forming mesenchyme, comprising around 10% of all benign bone tumors.[1,2] The ribs, femur, tibia, calvarium, bones, spine, pelvis, and shoulder girdle are the frequently involved sites.[3] It is caused by an activating somatic mutation in the alpha subunit of the Gs protein, resulting in abnormal osteoblastic differentiation and increased bone turnover.[3] It is known to be difficult to make the radiologic differential diagnosis between FD and malignant neoplasm. The MR signal intensity of FD is low to intermediate on the T1 images and it is variable on the T2-weighted sequences.[4] Histopathologic examination of the T2 hyperintense cases revealed fewer bony trabeculae, less cellularity and fewer collagen fibers than that of the T2 hypointense cases. FD usually shows increased uptake on bone scintigraphy. In a conventional three-phase bone scan, it shows hyperemia, increased blood pool, and intense tracer uptake in the delayed cortical phase. This is related to the high bone turnover associated with the immature woven bone, a characteristic feature of this disorder.[5] CT is still the best technique for demonstrating the typical radiographic descriptions of FD, which are the “ground glass” pattern of the bone and the lesion being surrounded by a distinct rim of reactive bone. Therefore, thorough interpretation of the CT information from FDG PET/CT study is helpful to make a correct diagnosis.[6]
With regard to FDG PET/CT, it is known that there is large variability in the FDG avidity of FD.[7] There are several reports that FD showed increased FDG uptake and this mimicked malignant bone involvement.[8,9] However, the discrimination between FD and malignant bone tumor is not well-defined because of a large SUV max overlap. The SUV max values of FD have ranged from 3.8 to 7.2 in the previous case reports. There are several possible explanations for the different degree of FDG hypermetabolism. Histiocytic and giant cell containing benign bone lesions in particular can show FDG hyper metabolic activity, and the turnover of the remodeling process may have various rates in different patients who have different stages of this disease. In addition, fibroblasts predominately proliferate in FD lesions, and the difference in the amount of proliferating fibroblasts or their metabolic turnover may result in a discrepancy of FDG uptake among FD lesions.[9] This case highlights the potential pitfalls in the interpretation of bone scans and FDG PET/CT when widespread abnormal areas of increased uptake are seen, particularly in the context of suspected malignancy. Polyostotic FD may closely mimic the appearance of bony metastatic disease. In these instances, clinical and radiological correlation is helpful in determining the etiology.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest.
References
- 1.Resnick D. Tuberous sclerosis, neurofibromatosis, and fibrous dysplasia. In: Resnick D, editor. Diagnosis of bone and joint disorders. 3rd ed. Philadelphia, London, Toronto, Montreal, Sydney, Tokyo: Saunders; 1995. pp. 4057–70. [Google Scholar]
- 2.Mandell GA, Harcke HT. Pediatric bone scanning. In: Collier BD, Fogelman I, Rosenthall L, editors. Skeletal nuclear medicine. St. Louis, MO: Mosby; 1996. pp. 343–4. [Google Scholar]
- 3.DiCaprio MR, Enneking WF. Fibrous dysplasia. Pathophysiology, evaluation, and treatment. J Bone Joint Surg Am. 2005;87:1848–64. doi: 10.2106/JBJS.D.02942. [DOI] [PubMed] [Google Scholar]
- 4.Jee WH, Choi KH, Choe BY, Park JM, Shinn KS. Fibrous dysplasia: MR imaging characteristics with radiopathologic correlation. AJR Am J Roentgenol. 1996;167:1523–7. doi: 10.2214/ajr.167.6.8956590. [DOI] [PubMed] [Google Scholar]
- 5.Zhibin Y, Quanyong L, Libo C, Jun Z, Hankui L. The role of radionuclide bone scintigraphy in fibrous dysplasia of bone. Clin Nucl Med. 2004;29:177–80. doi: 10.1097/01.rlu.0000113856.77103.7e. [DOI] [PubMed] [Google Scholar]
- 6.Berrebi O, Steiner C, Keller A, Rougemont AL, Ratib O. F18 fluorodeoxyglucose (FDG) PET in the diagnosis of malignant transformation of fibrous dysplasia in the pelvic bones. Clin Nucl Med. 2008;33:469–71. doi: 10.1097/RLU.0b013e3181779259. [DOI] [PubMed] [Google Scholar]
- 7.Aoki J, Watanabe H, Shinozaki T, Takagishi K, Ishijima H, Oya N. FDG PET of primary benign and malignant bone tumors: standardized uptake value in 52 lesions. Radiology. 2001;219:774–7. doi: 10.1148/radiology.219.3.r01ma08774. [DOI] [PubMed] [Google Scholar]
- 8.Aras M, Ones T, Dane F, Nosheri O, Inanir S, Erdil TY. False positive FDG PET/CT resulting from fibrous dysplasia of the bone in the work-up of a patient with bladder cancer: Case report and review of the literature. Iran J Radiol. 2012;10:41–4. doi: 10.5812/iranjradiol.10303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lee JH, Kim SY, Lee JE, Cho EY, Choi YL, Choi JY. Polyostotic fibrous dysplasia mimicking multiple bone metastases in a patient with ductal carcinoma in situ. J Breast Cancer. 2014;17:83–7. doi: 10.4048/jbc.2014.17.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]