

Abstract
Background
Children who visit pediatric emergency departments (EDs) and leave before being seen by a physician may present with particular health problems and may be at risk for preventable health outcomes. We compared children who left without being seen with those who stayed and were seen by a pediatrician, and followed all of the study subjects after they left the ED.
Methods
We asked all parents of children who visited the ED between July 1 and Oct. 31, 2002, to participate. Parents were interviewed by a trained ED research assistant. We abstracted data from the ED medical records. We used the Canadian Emergency Department Triage and Acuity Scale (CTAS) to measure the acuity of the illness or injury. Each child who left without being seen was matched with 2 children who had been seen by selecting the next patients on an alphabetical list by day, sex and age (within 1 year). We did follow-up interviews with parents within 96 hours of the visit to determine the reason for leaving and any treatment and diagnoses received subsequent to the ED visit.
Results
Of the 11 087 children seen in the ED during the study period, 289 (3%) left without being seen. Of the 289, the families of 158 (56%) consented to participate in the study and met the study criteria. The case and control groups thus consisted of 158 and 316 children respectively. Of the children who left without being seen, 24 (15%) were triaged as “urgent,” and none had a CTAS score of less than 3. A total of 99 children (63%) who left were taken by their families elsewhere for further medical care, compared with 89 (28%) of those who stayed. Waiting too long and resolution of symptoms accounted for 92 (58%) and 59 (37%) of the premature departures respectively. One child who left without being seen was subsequently admitted to hospital. Multivariate analysis showed that, after adjustment for time of arrival and time to reach the ED, children who left without being seen had lower acuity than those who stayed (odds ratio [OR] 4.0, 95% confidence interval [CI] 2.2–7.2) and were more likely to register in the ED between midnight and 4 am (OR 5.9, 95% CI 2.8– 12.5). Children in the premature departure group were also more likely to be taken elsewhere for follow-up care (unadjusted OR 4.3, 95% CI 2.9–6.4).
Interpretation
Children who left the ED without being seen had lower acuity levels and were more likely to be taken elsewhere for follow-up care than children who stayed. Most of those who left did so because the wait was too long or their symptoms resolved.
The characteristics of children who visit pediatric emergency departments (EDs) and leave before being seen by a physician are not well documented. Of potential concern are possible adverse outcomes related to a lack of timely assessment and treatment, worsening symptoms and decreased patient satisfaction. Studies conducted in general EDs treating primarily adult patients have shown an increased frequency of patients' leaving without being seen1 and the effect of leaving on patient satisfaction.2 Despite the importance of this problem, there is a paucity of studies on this topic in children.3,4,5,6,7,8,9,10,11,12
Adult patients are more likely to leave the ED as waiting times increase,4,5,12 if they perceive difficulties communicating with the staff, or if they have pressing commitments,4,12 and they are less likely to leave if length of wait is reduced.6 Pediatric studies10,13 and a survey of pediatric ED directors1,4 in North America showed rates of premature departure of 0.2%–3.9%, and a rate of 5.5% was reported from Australia.11 However, none of the authors of the pediatric studies compared the patients who left without being seen with those who stayed, and only 1 group reported the acuity level of pediatric patients.11
We performed a study to determine and compare the clinical and sociodemographic characteristics of children who leave the ED without being seen and of those who stay to be seen. We also wanted to discover why pediatric patients leave the ED, and whether and where they are taken by their families for further medical care.
Methods
The study was conducted between July 1 and Oct. 31, 2002, in the Division of Pediatric Emergency Medicine of a tertiary care children's hospital in Toronto serving about 50 000 patients annually. The study was approved by the Research Ethics Board of The Hospital for Sick Children, Toronto. Seven of the 12 ED admitting clerks were trained by one of us (R.D.G.) to seek informed consent from parents. Only families who registered with these clerks were approached regarding participation in the study.
We grouped the study population into those who left without being seen after being registered and triaged and those who were seen by a pediatrician (control group) (ratio of 1:2). The children in the control group were identified by selecting from the alphabetical list of children who visited the ED on the same day the next 2 children who were of the same sex and within 1 year of age of the child who left without being seen. If a family in the control group could not be reached after 10 attempts, the family of the next matched child was contacted. We excluded patients older than 18 years and those unaccompanied by adults.
Variables obtained from the ED health record included chief complaint, primary care physician (pediatrician or family physician), estimated transportation time from residence to ED, visits to the ED for the same problem in the preceding 48 hours and, for the children who were not seen, time of departure. We conducted a follow-up interview within 96 hours of the visit and obtained information about parent-reported diagnosis and treatment given during subsequent medical care. Families were asked to indicate the reason for leaving the ED from among the following options: “Wait was too long,” “Symptoms were better or resolved,” “Had other commitments,” “Problem with transportation,” “Communication difficulty with the triage nurse or registration clerk” or “Other.” We also obtained information about the parents' age, number of years in Canada, employment status, marital status, primary language spoken and number of children at home.
The Canadian Emergency Department Triage and Acuity Scare (CTAS), the primary exposure variable used in this study, measures the acuity of the child's illness or injury based on a series of clinical indicators.14 It is assigned by an experienced registered triage nurse. The score includes the following categories: “resuscitation” (CTAS 1), “emergent” (CTAS 2), “urgent” (CTAS 3), “semi-urgent” (CTAS 4) and “non-urgent” (CTAS 5).
All of the authors agreed on grouping patients' specific complaints into the following categories: medical, medical–infectious, surgical (including minor trauma) and other complaints, including psychiatric. A severe adverse outcome was defined as a need for hospital admission after leaving the ED prematurely. We defined waiting time as the period between the time of registration and the time the nurse went to place the child in the examination room, or as the period between registration and the time the family stated they were leaving or when the nurse noted the child's absence.
After comparing the frequency of each variable in the 2 groups, we performed univariate analysis to demonstrate any differences in each variable between the 2 groups. We also used stepwise multiple logistic regression analysis to assess the association between triage score, time of the visit, time to reach the hospital and leaving without being seen, controlling for potential confounders. Variables were retained in the regression model if the association was significant at a level of 0.05 or less in order to reduce the chance of including a spurious association.
Results
During the study period 11 087 patients were seen in the ED, of whom 289 (3%) left without being seen. Of the 289, the families of 182 (63%) were asked to sign a consent form; only 2 families refused. Of the remaining 180 children, 22 (12%) were excluded, because of an incorrect phone number (11 cases) or because their families could not be reached by phone (7 cases), refused to complete the questionnaire (2 cases) or spoke a language for which we could not find an interpreter (2 cases). The study group thus consisted of 158 children and the control group, 316 children. In the control group 348 families were approached, but we were unable to contact 32 families. None refused to participate.
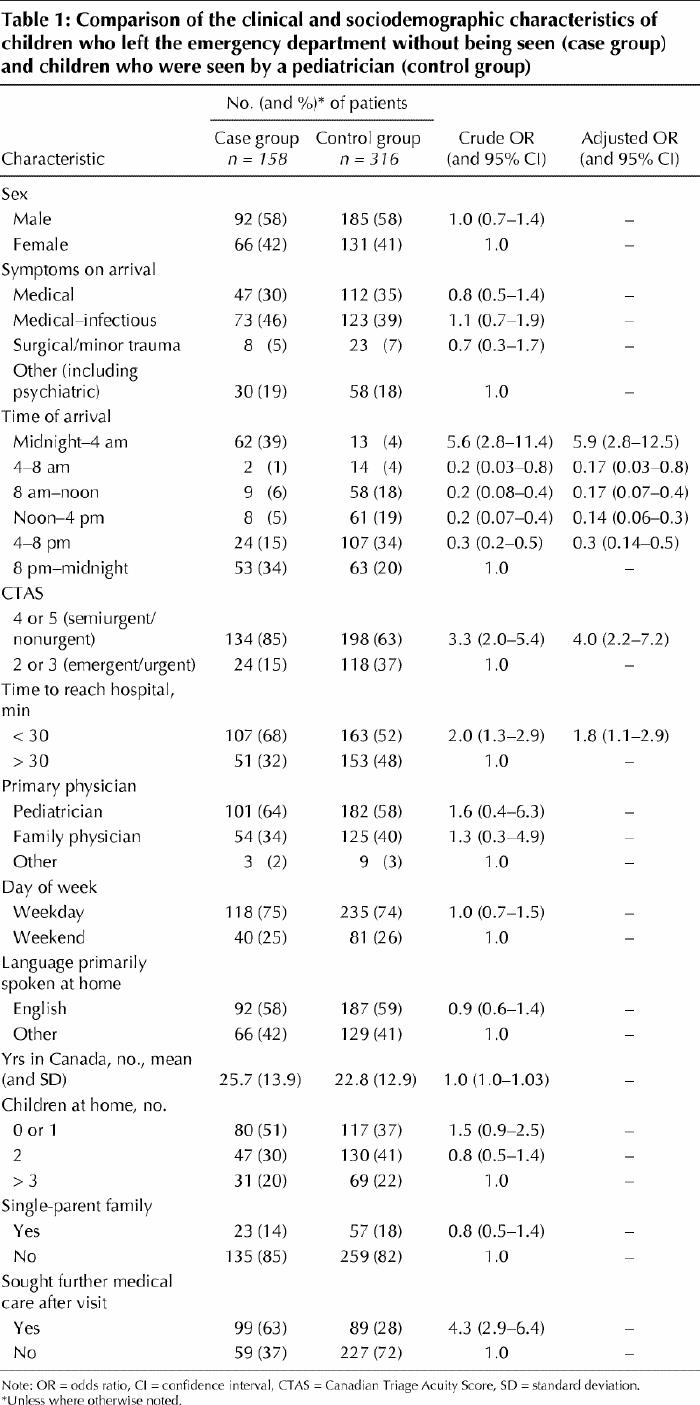
The characteristics of the 2 groups are given in Table 1. The children who left without being seen had higher CTAS scores (lower acuity) than the control group. None had a CTAS score of 2 (“emergent”). Twenty-four (15%) had a CTAS score of 3 (“urgent”), compared with 102 children (32%) in the control group. For those who left without being seen, the average length of stay in the ED (and standard deviation [SD]) was 1.9 (1.2) hours for those with higher acuity (CTAS score 3) and 2.1 (1.2) hours for those with lower acuity (CTAS score 4 or 5). Almost all children who left without being seen had a primary care provider. Significantly more children in this group than in the control group were taken elsewhere for care in the 96 hours following their ED visit (63% v. 28%, odds ratio [OR] 4.3, 95% confidence interval [CI] 2.9–6.4). Overall, the rates of subsequent medical visits were comparable for children with higher acuity and those with lower acuity. Among those who left without being seen, similar proportions with higher and lower acuity were taken elsewhere for further medical care (106 [67%] and 98 [62%] respectively). Similar proportions of children in the unseen and seen groups had been taken to another ED in the 48 hours preceding the current visit (3%). About a quarter of the patients in either group were seen on the weekend (Saturday or Sunday).
Table 1
In the group of patients who left without being seen, the average waiting time from the time they left the ED to the time they were taken elsewhere for follow-up care was 13 (SD 9) hours, compared with 25 (SD 11) hours for the control group (p < 0.001). Only 1 child who left without being seen required subsequent admission to hospital. This was a 3-year-old boy with a minor injury and a CTAS score of 3. On follow-up in our ED he was found to have a limb fracture that required a reduction. Two patients in the control group required subsequent admission: a 15-year-old girl with a psychiatric illness and a 2-year-old with pneumonia were admitted for observation and treatment the day after being discharged from the ED.
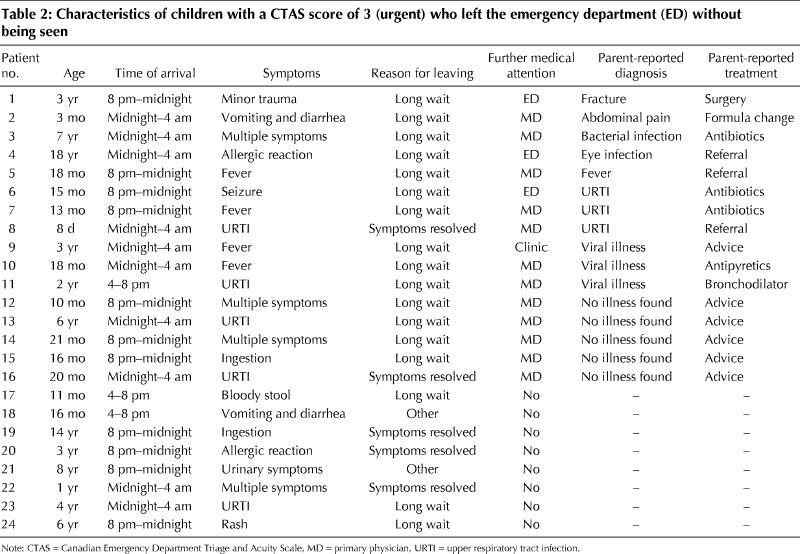
Logistic regression of the factors associated with leaving without being seen are presented in Table 1. Triage score, registration time and estimated travel time to the ED were found to be to be significantly associated with leaving without being seen. Children with a CTAS score of 4 or 5 were more than 4 times as likely to leave than those with a CTAS score of 2 or 3 (OR 4.0, 95% CI 2.2–7.2). Children who left without being seen were significantly more likely than those in the control group to have travelled less than 30 minutes to the hospital and to have registered in the ED between midnight and 4 am (OR 5.9, 95% CI 2.8–12.5). The nature of the complaint, being in a single-parent family and the number of children at home were not associated with leaving without being seen. Children in the premature departure group were more than 4 times as likely as children in the control group to be taken elsewhere for follow-up care (OR 4.3, 95% CI 2.9–6.4). The characteristics of the children who left without being seen who were triaged as “urgent” (CTAS score 3) are shown in Table 2.
Table 2
The reasons that patients reported for leaving the ED included “Wait was too long” (92 [58%]), “Symptoms were better or resolved” (59 [37%]), “Other commitments” (3 [2%]), “Problem with transportation” (1 [1%]) and “Communication difficulty with the triage nurse or registration clerk” (3 [2%]).
Of the 316 patients who stayed for physician assessment, 89 (28%) needed advice only, 51 (16%) received a prescription for antibiotics, and 26 (8%) were admitted, most commonly for infections (8 cases), complicated fractures (4 cases) and asthma (2 cases). Ten (38%) of those admitted received operative treatment.
Interpretation
We found that children who left the ED without being seen had a lower illness or injury acuity level, lived closer to the hospital, were more likely to register in the ED between midnight and 4 am, and were more likely to be taken elsewhere for subsequent medical advice than children who stayed to be seen by a pediatrician.
The rate of leaving without being seen in our study was more than double that reported in a pediatric ED in Chicago13 and double the median rate reported by 18 pediatric ED directors in the United States15 but half the rate reported in Australia.11 More patients in the Chicago study than in our study did not have primary health care providers, so it is possible that parents in the Chicago study used the ED as the primary source of medical care for their child and were therefore less likely to leave the ED. As the sole pediatric hospital in our area, we may have a higher patient load, longer waiting times and higher rate of premature departure. Another possible explanation for the discrepancy is the low reported rate (10%) of spontaneous resolution of symptoms in the Chicago cohort, compared with the rate of 37% in our population.
Previous studies investigating the acuity of patients who left the ED without being seen have given conflicting results. Some studies involving adults have shown a rate of high acuity of 33%,13,15whereas other adult studies16 as well as 1 pediatric study10 showed a high acuity rate of only 4%–15%. In the Australian study the acuity of almost all those who left without being seen was nonurgent.11 One reason for the disparity may be that waiting time is different owing to differences in the total number of patients seen in these EDs. Other factors may include whether the hospital is a primary or tertiary care centre,5 the number of physicians working in the ED,17 a higher number of acute cases, the presence of an observation unit17 and different triage acuity scales.
Our finding that 15% of patients who left without being seen had been triaged as “urgent” is of concern. However, only 1 of these children was subsequently admitted to hospital. A total of 63% of the children who left without being seen were taken elsewhere for medical care, where they may have been seen more quickly and been managed equally well.
Our results are consistent with previous studies showing that the time of day when patients arrive at the ED is associated with rates of premature departure for both adults4 and children.11Arriving between midnight and 4 am increases the odds of leaving without being seen by 5.9 compared with arriving between 8 pm and midnight. Being seen on the weekend is also associated with an increase in the rate of premature departure,13,17,18 perhaps owing to higher patient volumes. In our ED, there was no significant difference in the rate between weekdays and the weekend, probably because we have staff available to care for patients with lower acuity 12 hours per day on the weekend, compared with only 6 hours per weekday.
Waiting time is one challenge that EDs face in providing quality care for their patients. In our study, although 37% of the children who left without being seen had resolution of their symptoms while waiting to be seen, most parents felt that they had waited too long. The growing problem of overcrowding of the ED16,19,20,21 may be one reason for long waiting times. Furthermore, families of children who left without being seen were more likely to live within 30 minutes of the hospital than those who stayed. It is possible that patients who lived closer to the ED came simply because it was faster than seeking health care elsewhere, and perhaps they left without being seen because the families felt they could return quickly if necessary. In contrast, parents who lived further from the hospital tended to stay despite long waiting times, perhaps because of anxiety related to being unable to return in time should the child's symptoms worsen.
One of the strengths of our study is the low probability of recall bias, since patients were interviewed within 96 hours of visiting the ED. Furthermore, the primary exposure variable, the CTAS score, was measured before the decision to leave or patient assessment. However, some of our data were based on information reported by the parents. The sample size and follow-up time may also be limitations. Although 1 patient who initially left without being seen was subsequently admitted to hospital, none of the patients in this group had adverse outcomes. However, these events are relatively rare, and our study may have been underpowered to detect them. Some of the children may have had complications related to their illness after the follow-up period. However, since the follow-up period was the same in both groups, this limits the possibility of differential reporting of follow-up data. In addition, data on waiting times were missing for almost half of the patients who left without being seen, thus precluding an analysis of the influence of actual waiting time on the rate of premature departure.
Our study provides important information about the incidence of premature departure from the pediatric ED. It also provides insight into the clinical and sociodemographic characteristics of patients who leave without being seen and into differences between patients who leave and patients who stay. Further studies can focus on providing more information about the relation between waiting time and premature departure and on examining clinical outcomes of a greater number of children with higher acuity scores who leave without being seen. The effect of leaving the ED without being seen on patient satisfaction and the public image of the ED are other areas for exploration.
Acknowledgments
This study was supported by a research grant from the Canadian Association of Emergency Physicians. It was presented at the Canadian Association of Emergency Physicians Annual Scientific Meeting held in Winnipeg, June 14–17, 2003, and at the American College of Emergency Physicians Scientific Assembly held in Boston, Oct. 17–21, 2003.
Footnotes
This article has been peer reviewed.
Contributors: Ran Goldman initiated the study and was responsible for the formulation of the study proposal, data collection, analysis and writing of the paper. Alison Macpherson and Suzanne Schuh helped in the formation of the study proposal, data analysis and writing of the paper. Crystal Mulligan helped in recruitment of patients, data entry and writing of the paper. Jonathan Pirie supervised the project, helped in the formulation of the study proposal and writing of the paper. All of the authors gave final approval of the version submitted to be published.
Competing interests: None declared.
Correspondence to: Dr. Ran Goldman, Division of Pediatric Emergency Medicine, The Hospital for Sick Children, 555 University Ave,. Toronto ON M5G 1X8; fax 416 813-5043; ran.goldman@sickkids.ca
References
- 1.Bullard M, Rowe BH, Yiannakoulias N, Spooner CA, Holroyd B, Craig W, et al. Recent increases in left without being seen in the emergency department. 2002 Scientific Abstracts #80. Edmonton: Canadian Association of Emergency Physicians; 2002.
- 2.Elliott J. More support for refusing medical treatment. JAMA 1980;243:506-7. [DOI] [PubMed]
- 3.Carmel A, Amital H, Shemer Y, Sahar A. [Why do they leave? Clinical characteristics of patients who leave the emergency room against medical advice.] Harefuah 1998;134(6):445-9,503. [PubMed]
- 4.Fernandes CM, Daya MR, Barry S, Palmer N. Emergency department patients who leave without seeing a physician: the Toronto Hospital experience. Ann Emerg Med 1994;24(6):1092-6. [DOI] [PubMed]
- 5.Bindman AB, Grumbach K, Keane D, Rauch L, Luce JM. Consequences of queuing for care at a public hospital emergency department. JAMA 1991; 266 (8): 1091-6. [PubMed]
- 6.Fernandes CM, Price A, Christenson JM. Does reduced length of stay decrease the number of emergency department patients who leave without seeing a physician? J Emerg Med 1997;15:397-9. [DOI] [PubMed]
- 7.Wartman SA, Taggart MP, Palm E. Emergency room leavers: a demographic and interview profile. J Community Health 1984;9:261-8. [DOI] [PubMed]
- 8.Sainsbury SJ. Emergency patients who leave without being seen: Are urgently ill or injured patients leaving without care? Mil Med 1990;155:460-4. [PubMed]
- 9.Weissberg MP, Heitner M, Lowenstein SR, Keefer G. Patients who leave without being seen. Ann Emerg Med 1986;15(7):813-7. [DOI] [PubMed]
- 10.Dos Santos LM, Stewart G, Rosenberg NM. Pediatric emergency department walk-outs. Pediatr Emerg Care 1994;10(2):76-8. [DOI] [PubMed]
- 11.Browne GJ, McCaskill ME, Giles H, Lam LT, Fasher BJ, Exley B. Paediatric walk-out patients: characteristics and outcomes. J Paediatr Child Health 2001; 37 (3):235-9. [DOI] [PubMed]
- 12.Arendt KW, Sadosty AT, Weaver AL, Brent CR, Boie ET. The left-without-being-seen patients: What would keep them from leaving? Ann Emerg Med 2003; 42(3):317-23. [DOI] [PubMed]
- 13.Dershewitz RA, Paichel W. Patients who leave a pediatric emergency department without treatment. Ann Emerg Med 1986;15:717-20. [DOI] [PubMed]
- 14.National CTAS Working Group. Canadian Emergency Department Triage and Acuity Scale (CTAS). Available: www.caep.ca/002.policies/002-02.ctas.htm (accessed 2004 May 27).
- 15.Shaw KN, Ruddy RM, Gorelick MH. Pediatric emergency department directors' benchmarking survey: fiscal year 2001. Pediatr Emerg Care 2003;19 (3): 143-7. [DOI] [PubMed]
- 16.McNamara KJ. Patients leaving the ED without being seen by a physician: Is same-day follow-up indicated? Am J Emerg Med 1995;13:136-41. [DOI] [PubMed]
- 17.Hobbs D, Kunzman SC, Tandberg D, Sklar D. Hospital factors associated with emergency center patients leaving without being seen. Am J Emerg Med 2000; 18(7):767-72. [DOI] [PubMed]
- 18.Gibson G, Maiman LA, Chase AM. Walk-out patients in the hospital emergency department. JACEP 1978;7:47-50. [DOI] [PubMed]
- 19.Measures to deal with emergency department overcrowding. American College of Emergency Physicians. Ann Emerg Med 1990;19:944-5. [DOI] [PubMed]
- 20.Dickinson G. Emergency department overcrowding. CMAJ 1989;140:270-1. [PMC free article] [PubMed]
- 21.Feferman I, Cornell C. How we solved the overcrowding problem in our emergency department. CMAJ 1989;140:273-6. [PMC free article] [PubMed]