

Dear Editor,
Dissection is defined as the leakage of blood from an intravascular compartment into the vessel wall. Craniocervical dissections are a major cause of stroke, particularly among young adults. Mortality and morbidity rates vary based on the dissected vessel and dissection location. Although mortality rates for extracranial carotid and vertebral artery dissections are reported to be between 5% and 10%, mortality rates increase to above 70% for intracranial carotid and basilar artery dissections (1).
Sildenafil has been commonly used for treating erectile dysfunction since 1998. This study presents a case in which anterior cerebral artery (ACA) dissection occurred after the recent use of sildenafil.
A 45-year-old male was admitted to the emergency department with headache and left-sided weakness. He had a medical history of hypertension and diabetes mellitus, but he was not regularly using any recommended medicine. He had been using sildenafil once or twice a month for the last year for sexual enhancement. He took 100 mg sildenafil 2 h before his complaints had started. He did not have sexual intercourse or trauma before symptom onset. He was a non-smoker. Moreover, he did not have a family history of vascular disease and stroke. At the emergency room, his blood pressure was 160/90 mmHg, and he suffered from a throbbing, persistent headache at the front of his head. He was conscious and oriented. A neurological examination revealed only left-sided hemiplegia. Cranial computed tomography (CT) (Optima CT 660; GE Healthcare, Fairfield, USA) showed hypodensity in the right ACA territory and subarachnoid hemorrhage in the interhemispheric fissure and convexity sulci (Figure 1). Cranial magnetic resonance imaging (Optima MR 450w 1.5 Tesla; GE Healthcare, Fairfield, USA) showed a right ACA acute infarct (Figure 2). Doppler ultrasonography imaging of the carotid and vertebral arteries was normal. Cerebral angiography revealed a dissection at the right ACA between the A1 and A2 segments (Figure 3). Antiplatelet (300 mg/day acetylsalicylic acid) (Coraspin; Bayer, Leverkusen, Germany) and prophylactic antiepileptic (1000 mg/day levetiracetam) (Keppra; UCB, Brussels, Belgium) medication were administered. The high blood glucose level and mildly elevated blood pressure decreased to normal levels with the medication. There was no change in the patient’s level of consciousness. His neurological examination showed stable results. Repeat cranial CT revealed almost full absorption of blood at the subarachnoid space. His physical examination did not indicate any collagen tissue disease symptom. Clinical and laboratory analyses did not reveal any sign of systemic infection. According to his cerebral angiography findings, there was no evidence of cerebral vasculitis or fibromuscular dysplasia. Anti-nuclear antibody (ANA), anti-double stranded DNA (anti-ds DNA), anticardiolipin, anti-Ro, anti-La, and anti-Scl antibodies were within normal limits. The patient did not have migraine-type headache, and his homocysteine level was within normal limits. On the fourth day of admission and under antiepileptic treatment, a left focal motor status epilepticus occurred. Seizures were controlled with phenytoin (Epanutin; Pfizer, NY, USA) at a loading dose of 20 mg/kg, and phenytoin was administered at 300 mg/day as an add-on therapy. On the 17th day, the patient complained of having sudden-onset breathing difficulty. Based on his physical examination and imaging studies, he was diagnosed as having pulmonary embolism and was referred to the intensive care unit. He recovered from the respiratory problem with pulmonary embolism treatment. His physician in the intensive care unit also indicated that his clinical situation had improved. However, the patient died while eating his lunch on the fifth day in the intensive care unit due to acute cardiac arrest.
Figure 1.

Cranial computed tomography: Hypodensity in the right ACA distribution and subarachnoid hemorrhage in the interhemispheric fissure and convexity sulci
Figure 2. a, b.

Right anterior cerebral artery acute infarct: Axial apparent diffusion coefficient map (a) diffusion-weighted imaging (b)
Figure 3.
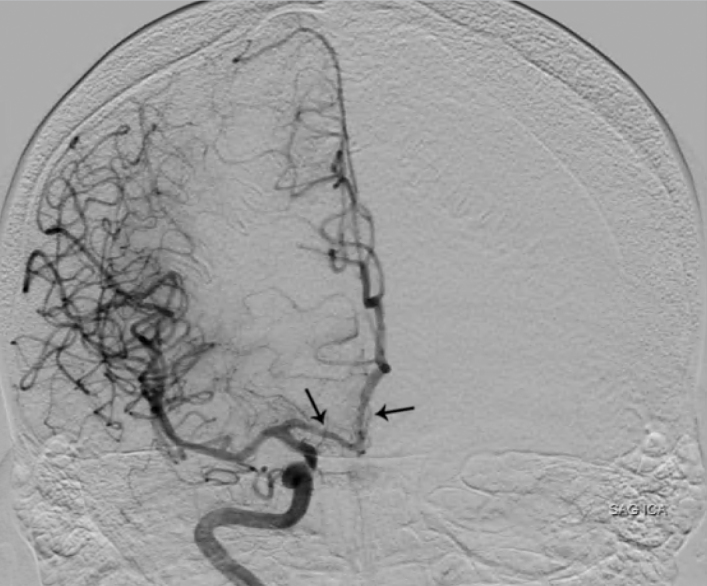
Cerebral angiography: A dissection at the right ACA between the A1 and A2 segments
Since triggering conditions such as sexual intercourse, mechanical stress, and trauma were absent and the dissection was occurred between the peak plasma concentration time and the half-life of sildenafil, sildenafil was considered to be a triggering factor of the dissection, and untreated hypertension and diabetes mellitus were underlying reasons. There are many studies on aortic and vertebral artery dissections after sildenafil use (2,3,4,5). However, to our knowledge, the presented case is the first one to address the relationship between sildenafil use and intracranial artery dissection.
The etiology of spontaneous artery dissections includes collagen tissue diseases, hypertension, systemic infections, migraine, high homocysteine levels, alcohol consumption, and oral contraceptive use. Although the etiological reasons of intracranial and extracranial artery dissections have been found to be similar in many current studies, one study indicated an increase in the prevalence of hypertension in patients with intracranial artery dissections (6). In another study on clinical imaging and neuroimaging in 18 ACA dissection cases, the etiological reasons were hypertension in 8 patients, smoking in 6, and diabetes mellitus in 4 (7). In a study on the relationship between aortic dissection and sildenafil use, the pathological mechanism was proposed to be an increase in the risk of intimal rupture because the vasodilatory property of sildenafil causes a decrease in arterial wall stiffness (5). The antiproliferative effect of sildenafil on human pulmonary artery muscle cell cultures has been observed (8). These etiopathological hypotheses indicate that sildenafil use causes dissection by reducing the endurance of arteries against mechanical stress.
Although the effect of sildenafil on intracranial arteries is not clearly understood, its known side effects such as flushing, headache, and nasal congestion show that its vasodilatation property affects intracranial arteries. The present case indicates that vascular risk factors should be considered before initiating sildenafil use.
Footnotes
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Kidwell CS. Dissection syndromes. 2013. http://emedicine.medscape.com/article/1160482-overview.
- 2.Dersch R, Anastasopoulos C, Hader C, Stich O. Vertebral artery dissection associated with sildenafil abuse. J Clin Neurosci. 2013;20:742. doi: 10.1016/j.jocn.2012.04.023. https://doi.org/10.1016/j.jocn.2012.04.023. [DOI] [PubMed] [Google Scholar]
- 3.Nachtnebel A, Stöllberger C, Ehrlich M, Finsterer J. Aortic dissection after sildenafil-induced erection. Southern Medical Journal. 2006;99:1151–1152. doi: 10.1097/01.smj.0000240732.65859.aa. https://doi.org/10.1097/01.smj.0000240732.65859.aa. [DOI] [PubMed] [Google Scholar]
- 4.Famularo G, Polchi S, Di Bona G, Manzara C. Acute aortic dissection after cocaine and sildenafil abuse. J Emerg Med. 2001;21:78–79. doi: 10.1016/s0736-4679(01)00345-6. https://doi.org/10.1016/S0736-4679(01)00345-6. [DOI] [PubMed] [Google Scholar]
- 5.Tiryakioglu SK, Tiryakioglu O, Turan T, Kumbay E. Aortic dissection due to sildenafil abuse. Interact Cardiovasc Thorac Surg. 2009;9:141–143. doi: 10.1510/icvts.2009.205849. https://doi.org/10.1510/icvts.2009.205849. [DOI] [PubMed] [Google Scholar]
- 6.Shin DH, Hong JM, Lee JS, Nasim R, Sohn SI, Kim SJ, Bang OY. Comparison of potential risks between intracranial and extracranial vertebral artery dissections. Eur Neurol. 2014;71:305–12. doi: 10.1159/000357867. https://doi.org/10.1159/000357867. [DOI] [PubMed] [Google Scholar]
- 7.Ohkuma H, Suzuki S, Kikkawa T, Shimamura N. Neuroradiologic and Clinical Features of Arterial Dissection of the Anterior Cerebral Artery. AJNR Am J Neuroradiol. 2003;24:691–699. [PMC free article] [PubMed] [Google Scholar]
- 8.Tantini B, Manes A, Fiumana E, Pignatti C, Guarnieri C, Zannoli R, Branzi A, Galié N. Antiproliferative effect of sildenafil on human pulmonary artery smooth muscle cells. Basic Res Cardiol. 2005;100:131–138. doi: 10.1007/s00395-004-0504-5. https://doi.org/10.1007/s00395-004-0504-5. [DOI] [PubMed] [Google Scholar]