

Abstract
Patient: Male, 15
Final Diagnosis: Lymphatic malformations
Symptoms: Abdominal pain
Medication: —
Clinical Procedure: Navigation surgery
Specialty: Surgery
Objective:
Unusual or unexpected effect of treatment
Background:
We used indocyanine green (ICG) fluorescence imaging to completely resect lymphatic malformations (LMs). This is the first report of navigation surgery utilizing ICG fluorescence imaging for resection of LMs.
Case Report:
A 15-year-old boy was diagnosed with LMs in the abdominal wall. The extent of the tumor was determined by an ultrasound, and ICG (Diagnogreen®, Daiichi-Sankyo Pharma, Tokyo, Japan) was injected subcutaneously and intradermally into the core and 2 marginal regions of the tumor (3 injections in total), respectively. During surgery, the extent of the tumor was confirmed with a photodynamic eye, and the tumor was completely resected. A fluorescent portion macroscopically estimated as normal was additionally resected and no residual fluorescence or tumor were confirmed in the remaining tissue. Abnormal lymphatic vessels were histopathologically observed in the additionally resected tissue, indicating the invasion of LMs. The surgery had a good outcome with no evidence of recurrence.
Conclusions:
We performed near-infrared fluorescence-guided imaging surgery for the resection of LMs in the abdominal wall. This is a single case study; therefore, assessment of more cases is warranted for further validation. This procedure could provide significant benefit to patients requiring resection of LMs.
MeSH Keywords: Indocyanine Green; Lymphangioma; Optical Imaging; Spectroscopy, Near-Infrared
Background
Lymphatic malformations (LMs) are benign refractory tumors characterized by proliferation of lymphatic vessels. Macrocystic LMs are effectively treated by sclerosing agents such as OK-432; however, the treatment of microcystic LMs is challenging. Surgical resection has been the criterion standard of treatment for microcystic LMs, but total resection is difficult in cases of diffused, nonencapsulated masses. Residual LMs can cause complications, such as lymphatic fluid retention and leakage, infection, and frequent recurrence [1].
Indocyanine green (ICG) fluorescence lymphography has recently been introduced to visualize lymph flow using a near-infrared camera. LMs have dilated lymphatic channels and do not have connections to the normal lymphatic system. They exhibit congested lymph flow; therefore, congestion of ICG within LMs after injection into the skin above the tumor was expected. We report the novel use of ICG fluorescence imaging for intraoperative identification of precise surgical margins of LMs. This is the first report of navigation surgery utilizing ICG fluorescence imaging for successful resection of LMs.
Case Report
The patient was a 15-year-old boy who was diagnosed with LMs in the abdominal wall at the age of 2 and had undergone sclerotherapy with OK-432 three times. The cystic lesion had disappeared, but a cavernous lesion 20×30×45 mm in size remained. Bleeding from bruises frequently occurred; therefore, surgical resection was planned. Preoperative magnetic resonance imaging (MRI) failed to clearly determine the extent of the tumor (Figure 1). Before the surgery, off-label use of ICG was approved by our Institutional Review Board, and informed consent was obtained from the patient and his parents. The extent of the tumor was re-examined by ultrasound, and 0.05 mL (0.125 mg) ICG (Diagnogreen®, Daiichi-Sankyo Pharma, Tokyo, Japan) was injected subcutaneously and intradermally into the core and 2 marginal regions of the tumor (a total of 3 injections). About 20 h after the injection, fluorescence images of LMs were obtained with a photodynamic eye (PDE; Hamamatsu Photonics, Shizuoka, Japan), which activates ICG with light emitted at a wavelength of 760 nm and filters out light at wavelengths below 830 nm. The fluorescence signal provided a real-time image of the LMs. Although the border was not clearly visualized because of ICG spillage, the extent of the tumor was confirmed with the PDE during surgery, and the tumor was completely resected (Figure 2). A fluorescent portion estimated to be normal macroscopically was additionally removed, and no residual fluorescence or tumor were confirmed in the remaining tissue. Abnormal lymphatic vessels were histopathologically observed in the additionally resected subcutaneous tissue, indicating the invasion of LMs. These endothelial cells lining the vessel structures were immunohistochemically reactive with D2–40 and CD31 and nonreactive with CD34. A slide of the additionally resected portion showed fluorescence signal (Figure 3). The patient has been followed up with echography every 4 weeks after surgery. The surgery had a good outcome with no lymphatic fluid retention and no evidence of recurrence.
Figure 1.
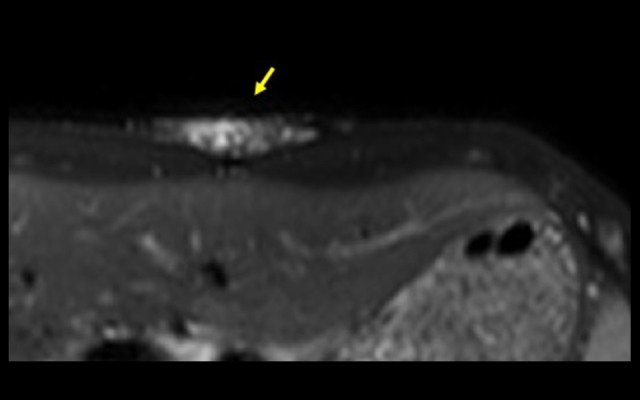
Preoperative MRI scan.
Figure 2.
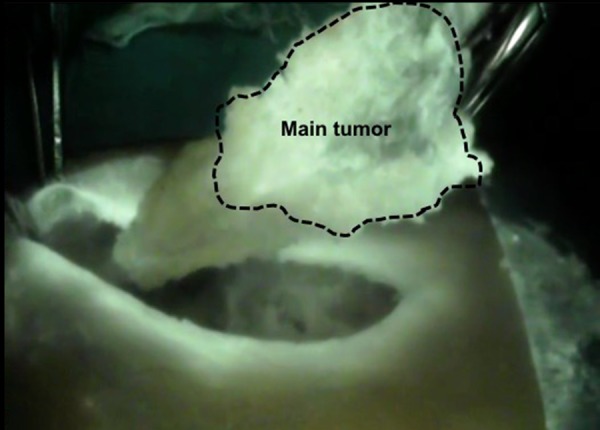
The tumor was resected by confirming the extent of the tumor with PDE during surgery.
Figure 3.
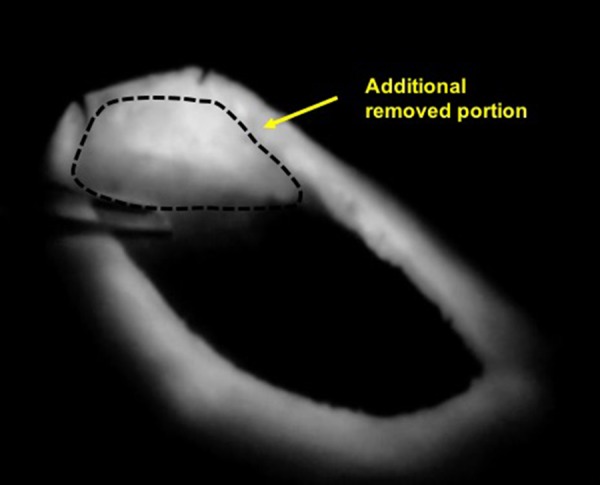
The additionally resected portion showing ICG fluorescence.
Discussion
LMs are rare, nonmalignant, and proliferative changes of lymph vessels [2]. LMs invade the surrounding tissues and have obscure borders; therefore, recurrence from residual tissue is a problem. The tumor borders are macroscopically and microscopically vague because LMs are nonencapsulated. Since LMs are benign tumors, large resection of LMs should be avoided because of cosmetic disadvantages, such as resection wounds and depressed scars; therefore, surgeons struggle to find the appropriate balance between thorough and minimal resection.
Near-infrared fluorescence-guided imaging surgery with ICG has been recently employed in various types of surgeries [3–6]. ICG is a very safe compound that has been widely used in a variety of clinical situations, such as examination of hepatic and cardiac functions and retinal angiography. ICG primarily binds to albumin, which drains into the lymphatic vessels. This property of ICG, as well as of methylene blue, has been used in lymphatic imaging for evaluating lymphedema and mapping sentinel nodes in various types of cancers by fluorescence navigation [7–9]. ICG fluorescence imaging is a safe and minimally invasive technique.
To our knowledge, the use of ICG fluorescence imaging in the treatment of LMs has not yet been reported. Based on lymph flow congestion in LMs, we expected congestion of ICG within LMs after injecting ICG into the skin above the tumor (subcutaneously and intradermally). The ICG dosage was determined on the basis of previous reports [10–12]. Subcutaneous injection of ICG directly above the tumor has been previously performed for mapping sentinel lymph nodes. Based on this assumption, we expected absorption of ICG after subcutaneous injection directly above the LMs [8,13]. The best injection site remains to be determined; however, since LMs have dilated lymphatic channels and no connections to the normal lymphatic system, once ICG is absorbed into the abnormal tissue in LMs, it will be retained and completed in every detail of LMs. One study revealed that photodynamic hyperthermal therapy using ICG and near-infrared light source induces apoptosis [14]. In the next stage of this application, we will introduce a photodynamic therapy using ICG for LMs.
Conclusions
We performed near-infrared fluorescence-guided imaging surgery for the resection of LMs in the abdominal wall following subcutaneous and intradermal injections of ICG into the skin directly above the tumor. To our knowledge, this is the first report of navigation surgery utilizing ICG fluorescence imaging for the resection of LMs. This, however, is a single case study, and assessment of more cases is warranted for further validation. This procedure could provide significant benefit to patients requiring resection of LMs.
Footnotes
Conflicts of interest
None declared.
References:
- 1.Ono S, Tsuji Y, Baba K, et al. New operative strategy for refractory microcystic lymphangioma. Surg Today. 2014;44(6):1184–87. doi: 10.1007/s00595-013-0806-z. [DOI] [PubMed] [Google Scholar]
- 2.Swarnakar RN, Hazarey JD, Dhoble C, et al. A 36-year-old female with recurrent left sided pleural effusion: A rare case of mediastinal lymphangioma. Am J Case Rep. 2016;17:799–804. doi: 10.12659/AJCR.895258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zhu B, Sevick-Muraca EM. A review of performance of near-infrared fluorescence imaging devices used in clinical studies. Br J Radiol. 2015;88(1045):20140547. doi: 10.1259/bjr.20140547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zhang YM, Shi R, Hou JC, et al. Liver tumor boundaries identified intraoperatively using real-time indocyanine green fluorescence imaging. J Cancer Res Clin Oncol. 2017;143:51–58. doi: 10.1007/s00432-016-2267-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zelken JA, Tufaro AP. Current trends and emerging future of indocyanine green usage in surgery and oncology: An update. Ann Surg Oncol. 2015;22(3):S1271–83. doi: 10.1245/s10434-015-4743-5. [DOI] [PubMed] [Google Scholar]
- 6.Keating J, Judy R, Newton A, Singhal S. Near-infrared operating lamp for intraoperative molecular imaging of a mediastinal tumor. BMC Med Imaging. 2016;16:15. doi: 10.1186/s12880-016-0120-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Collarino A, Vidal-Sicart S, Perotti G, Valdes Olmos RA. The sentinel node approach in gynaecological malignancies. Clin Transl Imaging. 2016;4(5):411–20. doi: 10.1007/s40336-016-0187-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Troyan SL, Kianzad V, Gibbs-Strauss SL, et al. The FLARE intraoperative near-infrared fluorescence imaging system: A first-in-human clinical trial in breast cancer sentinel lymph node mapping. Ann Surg Oncol. 2009;16(10):2943–52. doi: 10.1245/s10434-009-0594-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Isik A, Karavas E, Peker K, et al. Male Mondor’s disease is a rare entity. Breast J. 2016;22(6):700–1. doi: 10.1111/tbj.12657. [DOI] [PubMed] [Google Scholar]
- 10.Yoshida M, Kubota K, Kuroda J, et al. Indocyanine green injection for detecting sentinel nodes using color fluorescence camera in the laparoscopy-assisted gastrectomy. J Gastroenterol Hepatol. 2012;27(Suppl. 3):29–33. doi: 10.1111/j.1440-1746.2012.07067.x. [DOI] [PubMed] [Google Scholar]
- 11.Shibasaki J, Hara H, Mihara M, et al. Evaluation of lymphatic dysplasia in patients with congenital pleural effusion and ascites using indocyanine green lymphography. J Pediatr. 2014;164(5):1116–20 e1111. doi: 10.1016/j.jpeds.2013.12.052. [DOI] [PubMed] [Google Scholar]
- 12.Yamamoto T, Narushima M, Doi K, et al. Characteristic indocyanine green lymphography findings in lower extremity lymphedema: The generation of a novel lymphedema severity staging system using dermal backflow patterns. Plast Reconstr Surg. 2011;127(5):1979–86. doi: 10.1097/PRS.0b013e31820cf5df. [DOI] [PubMed] [Google Scholar]
- 13.Ballardini B, Santoro L, Sangalli C, et al. The indocyanine green method is equivalent to the (9)(9)mTc-labeled radiotracer method for identifying the sentinel node in breast cancer: A concordance and validation study. Eur J Surg Oncol. 2013;39(12):1332–36. doi: 10.1016/j.ejso.2013.10.004. [DOI] [PubMed] [Google Scholar]
- 14.Radzi R, Osaki T, Tsuka T, et al. Photodynamic hyperthermal therapy with indocyanine green (ICG) induces apoptosis and cell cycle arrest in B16F10 murine melanoma cells. J Vet Med Sci. 2012;74(5):545–51. doi: 10.1292/jvms.11-0464. [DOI] [PubMed] [Google Scholar]