

Abstract
INTRODUCTION:
Each mother has the legal right to decide about her delivery, but this decision should be made based on scientific knowledge. Instructions during pregnancy help to choose the proper type of delivery. This study conducted aimed to compare two instructional methods of role playing and lecture on primigravida decision about type of delivery.
SUBJECTS AND METHODS:
In this single-blind clinical trial 67 primigravida, 34–36 week were selected using multi-stage sampling and assigned into two groups randomly. Decision-making (before, 2-week after, and at admission in maternity department) was tested by a questionnaire. In role-playing group, advantages and disadvantages of two type delivery were presented by role-playing in 90-min by three scenarios. In lecture group, it was also presented in a 90-min lecture. Data were analyzed by mean difference test, Fisher test, independent and paired t-test.
RESULTS:
Two groups showed a significant difference in terms of decision at admission to maternity department (P = 0.000). 75% of lecture group and 100% of role-playing group selected normal delivery. Postintervention knowledge score in lecture group was 18 ± 5.3 and in role-playing group 17.1 ± 4.0. Percent of change in knowledge scores in two groups was significant (P = 0.001). Participants’ attitude, before and after the intervention, in both groups was significant (P < 0.05). Mean difference of pre- and post-test in relation to two groups’ knowledge and attitude scores was not significant (P > 0.05).
CONCLUSION:
In this research, lecture was more effective in raising knowledge level, and role playing was more effective in raising decision to vaginal delivery and reducing elective caesarean section. It is therefore suggested to use both teaching methods altogether for pregnant women to decrease the rate of unnecessary cesarean.
Keywords: Attitude, decision-making, knowledge, lecture, role playing, type of delivery
Introduction
A cesarian section (CS) is a surgical procedure in which one or more incisions are made through a mother's abdomen and uterus to deliver babies. CS is conducted only when natural delivery is contraindicated to protect mother's and infant's health.[1] Nowadays, unfortunately, having a CS has become a culture for escaping pain and has influenced public health. This is when CS imposes more risk to the mother, compared to vaginal delivery, and includes complications such as endomyometritis, bleeding, thromboembolism, and mortality (in mother), and preterm labor, respiratory distress syndrome, resistant pulmonary hypertension, and damages such as injury, bruise, or other traumas in infant.[2] Although indications of CS delivery are limited, it has increasingly grown in the most countries. American College of Obstetrics and Gynecologist has estimated 15.55 CS until 2010[1] while in some Iranian cities it is reported to be 47%.[2] Although educational programs of physicians and encouraging labor trial after previous transverse cesarean has been designed for decreasing CS rate,[3] it is increasingly growing in developing countries.[4] As to the studies, 65% of CS conducted in Iran were unnecessary and optional (elective cesarean) whose causes may be due to lake of knowledge, negative attitude toward normal delivery, fetal health, prevention of urogenital lacerations, fear of pain, change in sexual relationships, persistence of spouse, insurance for expenses, and other experience.[4,5,6,7] Although each mother has the legal right to choose the type of delivery, this decision should be made based on scientific knowledge.[8] In general, decision-making is a mental process that all human beings apply it through their lives. Obviously, effective decision-making needs applying a huge amount of information, in fact, information is considered as a mean and strategic tool for decision-making. Undoubtedly, quaky of decisions depends on the accuracy of information at decision-making time. In the decision-making process, decision maker's attitude plays an important role in interpretation and evaluation of information.[9] Hence, attitude and knowledge level influence decision-making for choosing either normal delivery or CS, so special strategies should be used for improving knowledge and attitude, and help proper decision-making. Education during pregnancy helps the improvement of knowledge and attitude and making decision for proper delivery method.[4] It could be effective when conducting to a positive attitude, or toward selecting the best and safest decision about pregnancy method based on the situation.[10] Iranian researchers could decrease CS delivery rate using different instructional methods such as group decision, behavioral intent model, instructional materials, and films.[11,12,13] However, regarding high Iranian CS rate, the distance for WHO Logan, reaching to 15% cesarian until 2011, and the effect of interventions in decreasing CS rate requires more effective interventions.[13] Of the most important principles of education, is selecting the most effective instructional method on learners, active participation. Role playing is one of these methods which are considered as a method for changing the attitude and trying to assist individuals to make their complicated decisions by the help of social groups.[1,5] Of the outstanding characteristics of this method is that observers feel themselves in the scene when they watch the play and communicate with the players emotionally.[14] This method aims to clarify the situation for individuals by role playing to encourage them to discuss and express their feeling and instructions freely.[15] In this method, learning occurs much better and more effective because of high concentration and emotional involvement,[14] and learners could develop their attitudes and problem-solving skills.[16] They found it interactive, experimental, convenient, and interesting;[17] and evaluated it as more exciting, instructive, and more valuable in comparison with lecture.[18] Several studies have been conducted for finding higher learning such as the study of role-playing on students who are in learning atmosphere,[19] however regarding high level of unnecessary CS and its risk for mother and infant, the effect of knowledge deficit and improper pregnant attitude toward normal delivery and CS and importance of role playing in making complicated decisions, no study has been performed for studying the effect of role playing on pregnant women who experience special situation for making correct decision and consequent performance, because this study aimed to compare the effect of two instructional methods of role playing and lecture on the pregnants’ decision-making about the type of delivery. It is expected to familiarize the pregnant with the consequences of vaginal delivery and CS and help them in making decision for choosing the proper method of delivery and making correct attitude toward vaginal delivery to decrease unnecessary CS.
Subjects and Methods
This clinical trial was conducted on 67 primiparous women (35 in roleplay group and 32 in lecture education group) referring to the health care centers in three cities of Mashhad at Khorasan province after obtaining the approval of Ethics Committee of Mashhad University of Medical Sciences. Participants in this study were informed that participating in this study is not compulsory, and if they do not like to answer some questions they are free not to answer them and their personal information will be treated as confidential and will not be disclosed. IRCT code is IRCT2015092623370N2.
As no report has been published in relation to the effect of role play on the fear of childbirth, based on a pilot study, the sample size was calculated to be 32 in each group. Sampling was by cluster sampling conducted among the health care centers of region number three. Two centers were assigned to role play method, two to lecture, and from the remaining centers, three subcenters were assigned to role play and three to lecture method. To prevent bias in education, it was tried to conduct education in identical conditions concerning the place of education, level of noise, educational equipment, time of the day, etc., As the routine educational method in health care centers is lecture, there was no need for a control group. Inclusion criteria were: No experience of acute psychological emotions, delivery and childbirth fear score > 28, primiparous, single pregnancy, gestational age of 34–36 weeks, age of 18–35 years, no history of infertility, no indication for CS, and not having passed the educational course for delivery methods. Exclusion criteria were: Some medical condition in a pregnant woman, diagnosis of abnormal fetus/no possibility for delivery of fetus on sonography, and abnormal volume of amniotic fluid or placenta.
Knowledge and attitude (before and 2 weeks after the intervention) and decision-making (before, 2 weeks after admission and in the delivery section) were evaluated using a valid and reliable researcher-made questionnaire, to investigate pregnant women's decision, a researcher-made checklist containing one question. The knowledge questionnaire has 23 items by three response (true, false, I do not know) and the attitude questionnaire has 22 items rated on a five-point Likert's scale (strongly agree, agree, no idea, disagree, strongly). The validity of these questionnaires were confirmed by 20 gynecologists and midwives of Mashhad University of Medical Sciences and their reliability were confirmed using alpha Coronach method (α =0.83 for knowledge and α =0.94 for attitude questionnaire). The validity of the decision-making checklist before intervention, 2 weeks after intervention, and of decision-making on the mode of delivery at admission in the labor was confirmed through content validity, and their reliability was obtained by evaluators’ consensus (r = 0.974).
The two groups of lecture and role playing were divided into four subgroups after taking the pretest. The role-playing group was divided into two subgroups of 10 subjects each and another two subgroups of 9 subjects each (38 subjects). Each group was instructed in a 90-min session about the advantages and disadvantages of normal delivery and CS. In this method, the researcher with two other co-researchers played three scenarios in seven steps (for each scenario) including warm up, selecting the participant, preparing the scene, preparing observers, play, discussion and evaluation, and generalization to education about the advantages and disadvantages of normal delivery and CS.
In the warm-up stage, the researcher narrated two true stories about the individuals who were wondering about the selection of the mode of delivery due to fear of childbirth and asked the participants to voluntarily accept to play the role of a pregnant woman with the researcher and two co-researchers. Then the participants helped the researcher to prepare and process the scene (scene preparation was conducted with the needed equipment for role play in two scenarios), and the observers were asked to pay close attention to the scenarios, taking important notes, and discuss them at the end of scenario. In scenarios, the reasons for mothers’ fear of natural delivery and CS were discussed. In the first scenario, one of the participants (a pregnant woman) played the role of a woman who referred to a midwife's office to select the mode of delivery and witnessed the events occurring in the office. Then, she referred to the midwife and consulted with her about her concerns.
The midwife talked to her about the two types of delivery impractically and asked her to express her decision after the scenario about choosing the type of delivery. After choosing the type of delivery, participants discussed the pregnant woman's selection (the same researcher gave no help) and justified each other to come to a conclusion. The second scenario was about a woman with a normal delivery and the benefits and complications experienced by her. The next step was similar to the first scenario. In the third scenario, one of the co-researchers defended CS, and another defended normal delivery at judge (natural delivery and CS appeared like a human and judge is researcher). After these three scenarios, participants were asked to talk about their friends’/relatives’ experiences of the two types of delivery. Lecture group (two subgroups of 10 subjects each and two subgroups of 9 subjects each) was instructed using PowerPoint presentation, marker, and whiteboard in a 90-min session. At the end of the session, participants’ questions were answered.
Two weeks after educational course for each group (lecture and role play), knowledge, attitude, and decision-making questionnaires were completed again. They were followed at admission by phone conversation for knowing their decision.
Data were analyzed by SPSS Version 14 (SPSS Inc.: Chicago, IL) and paired t-test, independent t-test, exact Fisher test and Chi-square were used for analysis.
Results
Participants aged 24 ± 4 years old, of which 58% were housewives and 14.9% employers. Educational level of most (51.4%) was at high school. Educational level of most of their husbands was at junior high school (38.8%), and they were workers (44.3%). The two groups showed no significant difference in terms of age, educational level and job of pregnant woman and her husband, income, source of information about type of delivery, insurance, time of referring for pregnancy care, and suggestion of mother, husband, friends, relatives and gynecologist about type of delivery (P < 0.05).
Exact Fisher test was used for comparing the frequency of primiparous woman's decision-making about the type of delivery before, 2 weeks after intervention and at admission to maternity department. As to the results, no significant difference was found; however, it was significant at admission (P = 0.000) [Table 1].
Table 1.
Comparing frequency of primiparous woman's decision making about type of delivery before, two weeks after intervention and at admission to maternity department

Knowledge score about the type of delivery, showed significant increase in comparison with before the educational course in both groups of lecture and role play (P = 0.000) but mean difference of pre- and post-test in relation to two groups’ knowledge scores was not significant (P > 0.05) [Table 2].
Table 2.
Comparing average of primiparous woman's knowledge about type of delivery before, 2 weeks after intervention in two groups

Change of scores related to the knowledge about type of delivery showed that the lecture group has the most (120%) knowledge increase in comparison with role playing (90%). The result of rates difference showed a significant difference between the two groups in this term (P = 0.001) [Figure 1].
Figure 1.
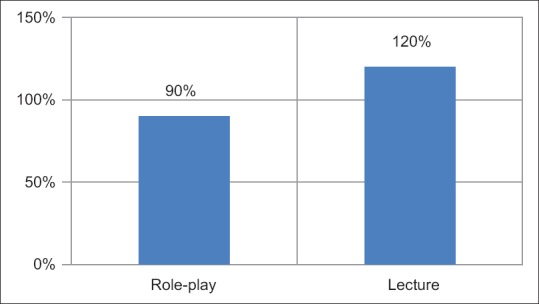
Comparison of rate of knowledge increase about type of delivery after the intervention in tow groups. Difference of proportions test: P =0.001
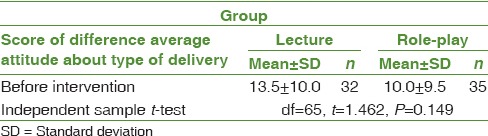
According to Table 3, there is a significant difference between the two groups in terms of attitude toward the type of delivery before and after intervention (P = 0.000), in other words, intervention could cause significant difference in attitudes of the two groups. As to the results, the two groups are different in terms of mean score of attitude toward the type of delivery before and after intervention (P = 0.034) and they were also significant before intervention (P = 0.003) [Table 3]. The mean difference of attitude toward the type of delivery before and after the intervention was studied using independent t-test and showed no significance (P = 0.149) [Table 4]. The change of score related to attitude toward the type of intervention showed that the lecture group had most (18%) attitude empowerment in comparison with roleplay group (12%); the result of ratio difference showed no significance between the two groups in this term (P = 0.173).
Table 3.
Comparing average of primiparous woman's attitude about type of delivery before, 2 weeks after intervention in two groups

Table 4.
Comparing difference average of primiparous woman's attitude about type of delivery before, 2 weeks after intervention in two groups
Discussion
In the lecture group, 25% of women probably and 40.6% absolutely selected natural delivery before intervention. Two weeks after intervention, the possibility of a decision on natural delivery was reduced by 6.2% and its absoluteness increased by 31.3%. However, at the time of admission in the labor ward, this possibility decreased by 3.2%, the absoluteness of natural delivery decreased by 12.5%, and the decision on CS increased, compared to before intervention. On the contrary, in roleplay group, 31.4% and 57.1% of women before intervention would possibly and absolutely select natural delivery, respectively. Two weeks after intervention, 11.4% decrease of probable decision and 22.9% increase to absolute decision were observed. At the time of admission in the labor ward, all possibilities for a natural delivery changed to absoluteness. Therefore, role play could change pregnant women's hesitation to decisiveness. In Fathian's study, behavioral intent model (based on this theory, people first make decision and behave based on rational and logical review of available information, and second, people consider the outcomes and results of their function before making a decision) was found to be effective in changing pregnant women's attitude toward normal delivery, in comparison with routine pregnancy care (P = 0.007). In Fathian's study, 74.3% of pregnant women of the experimental group (25.7% absolute and 48.6% probable) and 71.4% of the control group (30.0% absolute and 41.4% probable) intended to undergo normal delivery before intervention. After the intervention, normal delivery intention was 92.9% in the experimental group and 49.8% in the control group. Hence, intention to normal delivery has increased by 18.6% in the experimental group and has decreased by 21.6% in the control group.[13] This could be indicated as insufficient routine pregnancy care which has decreased by approaching to delivery time. The difference between the present study and Fathian's study is that in our study, pregnant women's decision-making was studied in three sections (before intervention, 2 weeks after intervention, and at admission) while Fathian studied it before and after intervention. At admission, many factors could affect the decision on the type of delivery. In this study, although increase in decision-making for normal delivery after intervention in role play in comparison with behavioral intent model was 11.5–18.6%, this increase led to 100% final decision for normal delivery, which remained 100% up to admission in the maternity department, while Fathian et al. did not compare the effect of behavioral intent model after intervention and at admission.[13]
In Fathian's study, the type of delivery performed in the two groups was not significant (P = 0.002); however, the elective CS in the presence and absence of midwifery problems were not studied. In the present study, although no significant difference was found in the type of performed delivery (P = 0.17), the elective CS in the lecture group was 5 times as much as in the roleplay group. The aim of education during pregnancy period was to bring about a decrease in elective cesarean by mothers, which was achieved in this study.
Role plays try to help individuals to find their own meaning in social world and seek help from social groups for making decision in difficult situations.[20,21] Methods such as role play need active involvement and development of personal communication with message, namely, personal projection. Hence, role plays, contrary to traditional methods whose concentration is change of attitude before change of behavior, focus first on behaviors, and then makes individuals modified attitude for matching them to new behaviors.[22] It could be considered as one of the causes for increasing decision-making for normal delivery, and the decrease of elective CS with no significant change in knowledge and attitude score in the roleplay group in comparison with the lecture group.
Lashgari et al. conducted a study entitled “effect of training programs of pregnant women on their delivery type selection: A single-blind, randomized control trial.” Test group used different structural methods such as film, booklet/lecture notes, visiting the maternity department, and interviewing the women who had delivery. Results showed significant different between the test and control (no education) groups in term of the type of delivery selected (P = 0.03).[13] Education could increase the decision taken toward normal delivery to 14%; however, in this study, role playing could increase the decision for normal delivery to 100%, which remained unchanged up to time of delivery. In fact, the role play method could increase the decision for normal delivery in a short time (90 min) in comparison with the study of Lashgari (180 min) and sustain the decision made. In Lashgari's study, pregnant women's decision at admission to the maternity department was not studied, so there was no data to be compared in this part.
In Kian et al.'s study entitled “the effect of education based on health belief model on selecting type of delivery,” the test group used different structural methods such as lecture, question and answer, film presentation of normal delivery and CS, and pamphlets about normal delivery and CS. The results showed a significant difference between the two groups in terms of the type of delivery selected (P = 0.001) (control group received routine pregnancy care). Health belief modelled to 96.9% selecting normal delivery and 3.1% selecting cesarean.[23] As Rahimi Kian et al. did not report the rate of normal delivery and CS before intervention, there was no data to compare with the present study. Although the educational intervention of Rahimi Kian, Fathian et al., and Lashgari et al. could increase the rate of normal delivery, none of them studied the sustainability of this decision at the beginning of labor that is the main situation for decision-making, and finally, the type of performed delivery. Of the strengths of the present study are 100% decision-making for normal delivery, sustained decision up to admission to the maternity department, and decrease in elective cesarean in the roleplay group in comparison with the lecture group.
Lecture is one of the simplest methods for increasing knowledge[24] and is considered as a main instructional method for health care professions. Many experts still believed that it would be effective if properly used.[20] It could be regarded as a good source for people who do not read magazines’, books or watch TV.[3]
In this study, the effect of role play on knowledge was less than lecture due to unknown origin; however, the probable cause could be short time of education (90 min), voluminous part of educational course, and short interval between pre- and post-test. Hence, it is recommended to compare stability of transferred knowledge of role play and lecture. As to Table 3, attitude means score 2 weeks of the two groups show significant difference before and after the intervention, however, no significant difference was found in terms of rate of changing attitude, so the two methods had similar effect on attitude level.
Attitudes acquired by deeper processing are more accessible and more resistant to change.[13] In most conducted studies on pregnants, the post-test was taken at least 4 weeks after intervention,[11,12,13] but the present study was conducted on gestational age of 34–36. Hence, a posttest was taken 2 weeks after intervention due to probability of delivery and risk of dropout. Thus, perhaps the long interval between pre- and post-test leads to more and much more sustainable attitude change in the role play in comparison with the lecture group. Fathian's study showed significant attitude is important in the experimental group compared to the control group (routine pregnancy care) based on health belief model (P < 0.001).[13] In this study, one session of lecture for increasing knowledge, one session general discussion for change of attitude and one session at the end of month for focusing on attitude and intent of pregnants toward normal delivery and one session for pregnants’ husbands were held. In the present study, just one session was held for each group, and certainly more educational session is related to holding educational sessions for husbands. Several studies focus on the role of husband on selecting the type of delivery and pregnant’ attitude.[13,15] Meanwhile, similarity of effectiveness of lecture and role play could indicate the importance of organized lecture based on standards. Hence, conducting the organized lecture for midwives and educational packages about advantages and disadvantages of normal delivery and CS to health centers with lower expresses could develop knowledge and attitudes of pregnant toward the type of delivery. Role play in contrary to traditional methods whose focuses are changing attitude before behavior, concentrates first on change of behavior, then made them modified attitudes to new behaviors.[22] Hence, it is recommended to increase sample size and pretest-posttest interval and the study attitude change, and decrease the rate of CS in roleplay group and compare with other instructional methods.
Conclusion
Of advantages of the present study is that despite low effect of lecture on knowledge development of learners in comparison with active approaches in several studies, the high level of knowledge development in pregnant was achieved. Hence, it could be concluded that a well-organized, low-cost lecture by midwives of health centers, could develop pregnant knowledge for selecting the safest type of delivery. However, as the aim of knowledge development is change of attitude and consequently changes of behavior, i.e., Application of active educational methods such as role play, accompanied with lecture method, is suggested to reduce primiparous women's decision-making for unnecessary CS.
Financial support and sponsorship
Chancellor for Research, Mashhad University of Medical Sciences, Mashhad, Iran with code of 88822.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
Special thanks to participants, co-researchers (Ms. Golzar, Ms. Karami and Ms. Mirzaee) and respected staff of Masshad Health Center Number 3. Authors thanks, Mashhad University of Medical Sciences Vice-Presidency for research for fully financial support of this study. The study is an MSc thesis.
References
- 1.Cunningham F, Leveno K, Gilstrap L, Hauth J, Wenstrom K. Williams Obstetrics. 22nd ed. New York: The McGraw-Hill Professional Publishing; 2014. p. 590. [Google Scholar]
- 2.Sharifirad G, Fathian Z. Survey of pregnant women view than vaginal and cesarean delivery based on behavioral intention model. J Illam Univ Med Sci. 2007;1:19–23. [Google Scholar]
- 3.Ewles L, Simnett I. Promoting Health: A Practical Guide. 5th ed. London: Elsevier; 2003. [Google Scholar]
- 4.Nuri T. Reasons of Cesarean Choice in Pregnant Women Refer to Rasht Health Centers. Midwifery, MSc Thesis: Tehran University of Medical Sciences; 2004. [Google Scholar]
- 5.Abedian Z, Navaee M, Jafarisani H, Ebrahimzadeh S, Arani A. Comparison of the effect of two teaching methods of role playing and lecture on primigravida women's knowledge, attitude and decision making in relation to type of delivery. J Obstet Gynecol Infertil. 2012;14:25–35. [Google Scholar]
- 6.Mohammaditabar S, Kiani A, Haidari M. Assessmen of nulliparous women tendencies to choose the type of delivery. J Babol Univ Med Sci. 2009;3:54–9. [Google Scholar]
- 7.Negahban T, Ansari A. Whether the fear of delivery can be predict the emergency caesarean among the primigravida women? J Nurs Midwifery Tehran Med Sci. 2008;14:73–81. [Google Scholar]
- 8.Amu O, Rajendran S, Bolaji II. Should doctors perform an elective caesarean section on request? Maternal choice alone should not determine method of delivery. BMJ. 1998;317:463–5. [PubMed] [Google Scholar]
- 9.Hammond JS, Keeney RL, Raiffa H. “The hidden traps in decision making”. Harvard Business Review on Decision Making. Boston: Harvard Business School Press; 2001. pp. 143–168. [Google Scholar]
- 10.Hildingsson I, Thomas JE. Women's perspectives on maternity services in Sweden: Processes, problems, and solutions. J Midwifery Womens Health. 2007;52:126–33. doi: 10.1016/j.jmwh.2006.10.023. [DOI] [PubMed] [Google Scholar]
- 11.Amidy M, Akbarzadeh K. Effect of health education on knowledge and attitudes of pregnant women in cesarean section. J Illam Univ Med Sci. 2005;13:17–26. [Google Scholar]
- 12.Lashgari M, Delavari S, Markazi Moghaddam N, Gorouhi F. Effect of training programs of pregnant women on their delivery type selection: A single blind, randomized control trial. J Tehran Army Univ Med Sci. 2005;3:679–84. [Google Scholar]
- 13.Fathian Z, Sharifirad G, Hasanzade A, Fathian Z. Study of the effects of behavioral intention model education on reducing the cesarean rate among pregnant women of Khomeyni-Shahr. J East Med. 2006;9:123–31. [Google Scholar]
- 14.Saberian M, Hajiaghajani S. The process of curriculum planning in medical science. Tehran: Salemi Publications; 2006. pp. 43–54. [Google Scholar]
- 15.Christine E. Translated by: Mahmudi Mohsen. Tehran: Bustan Tohid Publications; 1998. Teaching Skills Development Manual. A Guide for Teachers of Health Workers; p. 161. [Google Scholar]
- 16.Cacioppo J, Petty R, Kao C, Rodriguez R. Central and peripheral routes to persuasion: An individual difference perspective. J Pers Soc Psychol. 1986;51:1032–43. [Google Scholar]
- 17.Joyner B, Young L. Teaching medical students using role play: Twelve tips for successful role plays. Med Teach. 2006;28:225–9. doi: 10.1080/01421590600711252. [DOI] [PubMed] [Google Scholar]
- 18.DeNeve K, Heppner M. Role play simulations: The assessment of an active learning technique and comparisons with traditional lectures. Innov Higher Educ. 1997;21:231–46. [Google Scholar]
- 19.MacLaren J, Cohen L, Larkin K, Shelton E. Training nursing students in evidence-based techniques for cognitive-behavioral pediatric pain management.The Journal of nursing education. 2008;47:351. doi: 10.3928/01484834-20080801-05. [DOI] [PubMed] [Google Scholar]
- 20.Azizi F. Medical Education, Challenges and Prospects. Tehran: Education Deputy and Affairs of Student, Ministry of Health and Medical Education; 2003. [Google Scholar]
- 21.Joyce BR, Weil M, Calhoun E. Models of Teaching. 7th ed. Tehran: Kamale Tarbiat Publications; 2004. [Google Scholar]
- 22.Festinger L, Carlsmith JM. Cognitive consequences of forces compliance. J Abnormal and Social Psychology. 1959;58:203–10. doi: 10.1037/h0041593. [DOI] [PubMed] [Google Scholar]
- 23.Kian FR, Miralimohamadi M, Abbas M, Gazaforudi KA, Barugh NS. Effect of Health Belief Model education on chosen delivery method. J Nurs Midwifery Tehran Univ Med Sci (Hayat) 2008;14:25–32. [Google Scholar]
- 24.Yaghubian M, Yaghubi T, Salmeh F, Golmohammadi F, Safari H. Comparison of the effects of education booklet and lecture method with booklet training on the knowledge of nurses about professional rules. Iran J Med Educ. 2009;9:372–81. [Google Scholar]