

Abstract
STATEMENT OF THE PROBLEM:
Examinations have an important role in evaluating students’ learning outcomes and their mastery of a subject. Passing or failing an examination can have far-reaching consequences for the students. Therefore, it is not surprising that international studies consistently show that dental students report examinations and grades among the highest ranking stressors in dental schools.
PURPOSE:
The aim of this research was to measure the levels of anxiety, self-perception of preparation and expectations for success using an objective structured clinical examination (OSCE), a written examination and a preclinical preparation test, and to examine the effects of the three predictive variables on the outcomes of assessments.
MATERIALS AND METHODS:
The present research is a cross-sectional study. The population under consideration was students of Kerman Dental School in 2013. Examination anxiety was measured with Spielberger's state anxiety inventory. Preparation for the assessment (I am fully prepared = 4, I am prepared = 3, I’m not prepared = 2, I’m not fully prepared = 1) and expectation to succeed (I am quite successful = 4, I am successful = 3, I’m not successful = 2, I’m not quite successful = 1) were quantified with Likert scale. The questionnaire was completed during an OSCE, a written examination, a preclinical crown and bridge preparation test and a nonexamination situation.
RESULTS:
The study population consisted of 138 4th, 5th, and 6th year Kerman dental students (65 males and 73 females). The results showed that all the assessment methods induced a significant increase in state anxiety compared to baseline levels with the highest anxiety levels reported during an OSCE (62.4 ± 8.1, P = 0.04) and a written examination (48.8 ± 9.2, P = 0.04). The preparation levels in females were significantly higher than those in males in OSCE (P = 0.03) and written (P = 0.04).
CONCLUSION:
State anxiety was high in all the three assessment methods. OSCE induced more anxiety than other assessment formats. However, anxiety was not predictive of performance outcomes in contrast to preparation and expectation to succeed, which were good predictors of the outcome scores. Also, this study showed that despite a better answer to the assessment of (I prepared myself well for the test), the students showed high levels of state anxiety.
Keywords: Anxiety, clinical assessment, objective structured clinical examination
Introduction
Clinical instruction is one of the basic and important pillars in medical group education. Clinical instruction prepares the students to achieve clinical experience with patients and their problems in the hospital setting. That is why it is difficult to judge and evaluate their clinical skills.[1] Examinations have an important role in evaluating students’ learning outcomes and their mastery of a subject. Passing or failing an examination might have profound consequences for the students’ careers. Therefore, it is not surprising that international studies consistently show that dental students believe examinations and grades are the most important stressors in dental schools.[2,3,4,5,6]
Unfortunately, at present there are objections to the methods employed to give clinical examinations, such as the large number of participants, short time for evaluation, and absence of a distinct evaluation method.[7] One of the measurement tools is objective structured clinical examination (OSCE), introduced for the first time in 1975 by Dr. Ronald Harden.[8] Harden and Glason believed that OSCE provides a chance to evaluate different skills in different situations.[8] Several dental schools have incorporated the OSCE in their curricula since 1994 and it has been evaluated since then.[9,10,11]
Nowadays, OSCE is one of the best examination techniques, which can easily evaluate basic and professional skills of students and also determine goals of education in different fields, including recognition, sentimentalization, and psychic-dynamic aspects, by showing students’ abilities in different stations, eliminating the effects of intermediate variables.[12,13] Over the years, OSCE has been used with real patients to evaluate clinical skills of students before and after graduation. For example, during 1993‒1994 only 38 out of 126 medical schools in the US used OSCE. However, in 2003‒2004, 121 out of 126 institutions used OSCE to evaluate students.[14] Studies by Gerrow et al. showed that OSCE and written examinations yielded similar results and equal mean grades.[15] Another research study by Brown in 1999 showed that OSCE is superior to other routine evaluation methods.[16] However, other researchers have shown that the big menace to OSCE reliability is its specificity,[17,18,19] affecting each student's turnover at each station. To solve this problem there should be several stations to be able to evaluate each student's abilities. Different patients, time of each station, gender, ethics, the effect of each student's shift, student's anxiety and fatigue and the learning environment influence this exam.[18,19,20] In addition, there are some reasons why an OSCE is more stressful than written and clinical assessments.[2] Whether, studies showed that it would be valuable to dental educators to understand more fully those aspects of academic performance affected by stress. In their education, students are expected to acquire a science knowledge base, develop clinical competencies, and integrate these contextually in clinical decision-making scenarios. One or more of these three learning domains may be sensitive to the effects of stress, but this has yet to be determined.[4,6,7,21,22,23,24]
Whether an OSCE causes more stress in dental students is unknown, although there are anecdotal reports that some dental students suffer from shaking hands, quivering voices and/or increased blood pressures during OSCE. State anxiety is defined as an unpleasant arousal in the face of threatening demands or dangers. A high level of test anxiety might interfere with optimal learning. This has also been reported for students with the highest level of self-reported stress, who tend to achieve lower grades than students with lower stress levels. Perception of higher levels of stress after the examination was marginally associated with poorer marks for that examination.[5]
Clinical evaluation is one of the difficult problems in Iran, and lack of specific standards and distinct goals in clinical fields that are specified, reachable, measurable, classifiable and organized affects the learning processes of students.
There are many research studies on OSCE all over the world, but based on evidence there are only limited studies on the anxiety of OSCE compared to other dental examinations. Besides, a few dental studies have been conducted with a small sample. Also, any study has been done in Iran. Therefore, the aim of the current study was to examine whether the level of anxiety of dental students of Kerman Dental School induced by OSCE is higher than that by a written examination and a preclinical endodontic and crown preparation examination.
Materials and Methods
This study was approved by the Ethics Committee of Kerman University of Medical Sciences (No. K.90.84). In this descriptive and cross-sectional study, census sampling was applied. Population consisted of 4th, 5th, and 6th year dental students of Kerman Dental School in 2013 year (January 2013–December 2013). All students in 4th, 5th, and 6th were included in the study, in fact, a census sampling was applied that similar to other studies and sample size was adequate. The students were under no obligation to participate in this research and their participation was voluntary (written consent). The students were invited to provide their registration number, so they put their number above the anxiety questionnaire (attached form). Anxiety was measured with the Spielberger's State-Trait Anxiety Inventory questionnaire, which is a widely used and well-validated tool for measuring state and trait anxiety (Cronbach's alpha = 0.84). Demographic data included age and gender and all the exams were real.
The questionnaire consists of 20 statements (e.g., “I am tense”), to which the respondents indicate their level of agreement on a 4-point scale regarding how they feel at a given moment (1 = not at all, 2 = somewhat, 3 = moderately so, 4 = very much so). The potential scores range from 20 to 80, with high scores representing high levels of anxiety. The questionnaire was distributed to participating dental students in four test situations (the OSCE, a written test, a preclinical crown and bridge preparation test, a basic life support test), who were asked to complete the form before and after the exam by students under study. This research was carried out under real exam situations and about 10 min completed the questionnaire. Preparation for the assessment (I am fully prepared = 4, I am prepared = 3, I’m not prepared = 2, I’m not fully prepared = 1) and expectation to succeed (I am quite successful = 4, I am successful = 3, I’m not successful = 2, I’m not quite successful = 1) were quantified with Likert scale.
This research was carried out under real exam situations:
The OSCE consisted of 10 stations, 1.5 min each, and assessed the clinical competence at pediatric dental courses. Since two points could be obtained for each station, the score range was 0‒20
In a written test on oral medicine the students were required to answer 20 short essay-type questions within maximally 60 min. The score range for this examination was 0‒20
Preclinical tests on crown and bridge preparation lasted 45 min and an endodontic test consisted of access, cleaning and shaping and obturation of molar teeth in maximally 2 h. For both tests the score range was 0‒20
A basic life support course was given in 30 min to obtain blood pressure, pulse rate and also clinical knowledge and skill in emergency care such as oral and dental examinations in a model. The students did not have to prepare. As the students knew beforehand that the course did not include an assessment, the obtained values were considered to represent nonassessment baseline anxiety levels (control group).
In this study, the Pearson correlation test, Mann–Whitney U-test and Kruskal–Wallis test were used. The collected data using SPSS version 13.0 (SPSS Inc.: Chicago, IL) are analyzed and P < 0.05 was considered statistically significant.
Results
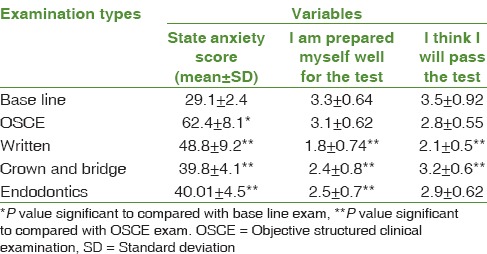
The study population consisted of 138 4th and 5th year dental students (65 males [47.1%] and 73 females [52.9%]). Mean age was 22.1 ± 4.9 years, ranging from 22 to 37. Table 1 shows state anxiety scores in all examination types before and after examination. The results showed that all the assessment methods induced a significant increase in state anxiety compared to baseline levels with the highest anxiety levels reported during an OSCE and a written examination (P = 0.01). The students reported better preparation for the OSCE and crown and bridge preparation and endodontic (preclinical, modeling) than for the oral medicine examination (written). Their expectation to pass the test was also significantly higher for crown and bridge preparation and endodontic treatment tests than for the OSCE and oral medicine tests (P = 0.01). Among all this, the written oral medicine examination yielded the lowest grades regarding the questions asked to indicate their preparation for the assessment (I prepared myself well for the test) and their expectation to succeed (I think I will pass the test) [Table 2].
Table 1.
State anxiety at all types of assessment method before and after examination

Table 2.
Correlations between level of preparation, expectation to succeed, state of anxiety and type of examination
To survey the relationship between state anxiety and the scores obtained in the exam, the students were classified into three groups according to the level of their anxiety, including high anxiety level (high), with a range of 65‒80; moderate anxiety level (intermediate), with a range of 40‒64.99; and low anxiety (low), with a range of 20‒39.99.[3]
State anxiety during the OSCE showed an association with the level of preparation, with individuals with high anxiety levels reporting better preparation; however, the scores obtained on the OSCE did not correlate with the state anxiety during the OSCE. The level of state anxiety during a written examination showed a positive correlation with the score obtained, with students with higher anxiety levels having better grades. In addition, students with higher anxiety levels during crown and bridge preparation and preclinical endodontic examination reported more preparation and achieved better scores. There was a positive correlation between preparation and the expectation to succeed. For all the four types of assessment, the level of preparation exhibited a positive correlation with the expectation to succeed. Students who reported a high level of preparation expressed more expectations to succeed and obtained better results.
Table 3 shows the relationships between the students’ anxiety levels, and their scores. This study showed that students with higher levels of anxiety during an OSCE and a written examination obtained better scores, exhibiting a positive correlation between these two items during a written exam. Furthermore, students who reported a high level of preparation and expectation to succeed on OSCE and a written examination showed higher levels of anxiety. State anxiety during the preclinical crown and bridge preparation and endodontic examinations exhibited a positive correlation with the scores obtained. State anxiety correlated with the level of preparation for these tests.
Table 3.
Correlations between state of anxiety score, level of preparation, expectation to pass the test and score obtained during different examinations
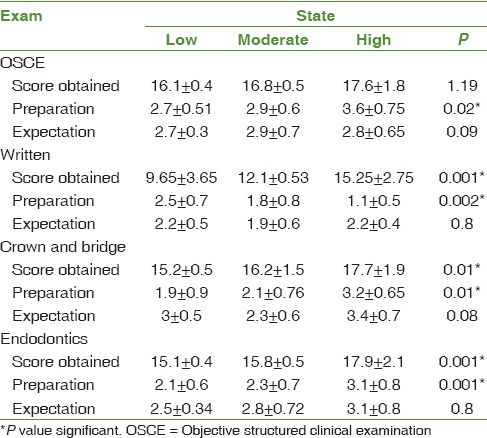
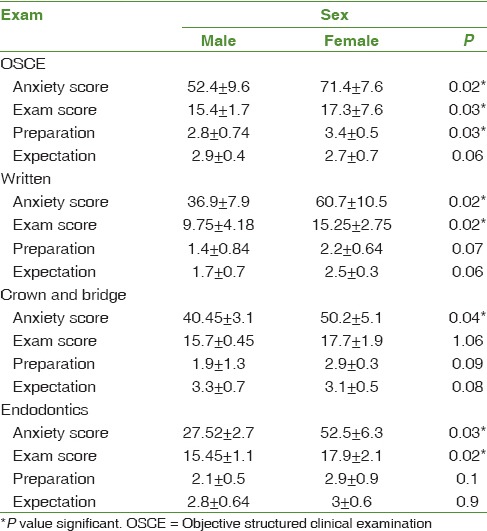
Table 4 shows the effect of gender on state anxiety, and the scores obtained. Females had higher levels of anxiety during all types of assessment, indicating a positive correlation between gender and state anxiety. The average grades of female students at all types of examinations were significantly higher than those of male students. Such a gender effect was found for the scores of the OSCE, written and endodontic exams. Levels of preparation for the examinations were higher in females. Preparation level was correlated with gender during the OSCE and written examination; also expectation to pass the test was higher in females during the OSCE and written examination but no significant relationship was found. Also, this study shows that age doesn’t significant relationship with anxiety score (P = 0.12). Although, preparation level was correlated with younger students during the written examination, expectation to pass the test was higher in younger students during the written examination but no significant relationship was found (P = 0.31).
Table 4.
Correlations between state of anxiety score, level of preparation, expectation to pass the test and score obtained during different examinations according to gender
Discussion
Examination and assessment procedures are potentially anxiety-provoking and stressful for dental students.[4,6,7,21,22,23,24] The current study explored the state anxiety of dental students during four different types of examinations. This study showed that in the control condition, the dental students reported state anxiety levels comparable to baseline population norms.[25,26]
OSCE and written examination evoked an increased level of state anxiety compared to a preclinical crown and bridge preparation and endodontic examinations, consistent with previously reported state anxiety levels of dental students by Marshall and Jones.[26] The observation that the dental students find the OSCE much more stressful than a written examination is consistent with studies of Marshall and Jones, Furlong et al., Brosnan et al. and Brand and Schoonheim-Klein.[3,26,27,28] A possible explanation is that a written examination is undertaken in relative anonymity, whereas the constant monitoring and observation during an OSCE may increase anxiety levels. Also in a written examination there is no time limit for each question and students can spend their time on any question and if they do not know the answer of one question, they can think about it at the end of the exam. However, during an OSCE usually each station has its own time which cannot be extended and if the students are not able to answer one station they do not have time to think about it. It has been demonstrated that students in a timed examination do not perform as well as their counterparts without time limits.[11,29] However, Schoonheim-Klein et al. showed that more time per station did not improve students’ performance.[30]
This study showed that despite a better answer to the assessment of (I prepared myself well for the test), the students showed high levels of state anxiety, consistent with others study.[2,4]
The written examination is a traditional method of assessment in the academic environment. Selection of our dental school was not based on performance on written tests because students are familiar with this assessment format since their 1st year in high school. This examination consisted of short essays, multiple choice questions, blanks or even true-or-false questions. This study showed that students had higher levels of anxiety during a written examination compared to preclinical crown and bridge preparation and endodontic examination, which might be attributed to the topic of the examination. The topic of the examination can induce more stress and high state anxiety levels than the type of the examination.[27] Marshall and Jones showed that topics and kinds of questions had more significant effects on the level of state anxiety than the type of the examination.[26]
The written examination showed lower anxiety levels compared to an OSCE. A possible explanation is that students are familiar with this assessment. It has been demonstrated that more experience might reduce stress levels and this is another reason to explain lower anxiety levels with written examinations. However, studies by Troncon on medical students showed that the percentage of students who were highly stressed with OSCE did not decrease with increasing experience.[31] It is a matter of controversy whether stress is functional and results in better learning, or dysfunctional and compromises learning as a result of poor performance.[32,33]
In our study, we found a significant and positive relationship between state anxiety levels during a written examination and two preclinical modeling examinations and the scores were obtained for this type of assessment. Previous studies by Brand and Schoonheim-Klein[3] showed that students with high levels of anxiety during the written examination did well on examinations and there was a positive relationship between these two. In addition, for the other two types of modeling examinations no relationship was found between state anxiety and the outcomes. Some studies have reported a weak and negative relationship between state anxiety of dental students and their grades. Studies by Westerman et al. on 1st year dental students showed a statistically significant and negative relationship between state anxiety and exam grades. During a written test in pediatric dentistry, a near-significant negative correlation between stress levels and test scores was observed.[34] In three recent studies by Reteguiz, Anderson and Stickley and Chapell et al. on medical trainees, anxiety scores were not significantly correlated with performance scores.[35,36,37]
Usually there is an inverse correlation between anxiety levels and test scores. High levels of anxiety resulted in lower test scores and low levels of anxiety gave rise to better test scores. Undoubtedly, high levels of anxiety compromise performance because anxiety can impair intellectual functions temporarily and a panic-stricken individual cannot use the whole functions of the wisdom; therefore, they cannot properly learn the examination material.[38]
The Yerkes–Dodson law indicates that some degree of state anxiety enhances performance, but only up to a certain point. High levels of anxiety may retard performance, resulting in an inverse relationship between state anxiety and performance.[39]
The level of preparation for the OSCE and other two preclinical modeling examinations was significantly related to the scores obtained. Studies by Mavis and Brand and Schoonheim-Klein[3,40] on dental and medical students showed a positive relationship between preparation levels and scores obtained.
Female students showed higher levels of preparation than male students, and there was also a positive relationship between the preparation level and OSCE and written examinations, with no relative relationship in this field.
In a previous study by Schoonheim-Klein et al., female dental students outperformed their male counterparts in a summative periodontal OSCE.[30] In the UK, female medical students also performed better in a summative OSCE.[4,7,41,42] However, in a study by Mavis and Brand and Schoonheim-Klein on a formative OSCE, no significant differences in OSCE performance were found between males and females.[3,40]
This study showed that female dental students perceive examinations and grades more stressful than males. The level of anxiety was also positively related to gender differences; in addition, women had better grades in all types of examinations, with test scores and gender in OSCE, written and endodontic examinations being positively related, consistent with studies by Grandy et al. and Al-Omari et al. studied.[4,21] It appears female dental students had higher levels of anxiety and preparation during exams compared to males; however, other studies failed to support this finding.
A possible explanation for these conflicting results may be the fact that cultural and social differences between studies might have an influence on potential gender differences in perceived stress. The type of test station may also be an important factor for gender-related differences in OSCE performance.[43] For example, in a study by Schoonheim-Klein et al., female students outperformed male students only significantly in specific areas.[30]
This study has some limitations. As the dental students were recruited on a voluntary basis, not all students participated in each test condition, and only a number of students completed all four test situations. It has been suggested that high anxious students may be less willing to participate in this type of studies. Although we cannot exclude this possibility, gender and/or examination grades of the nonparticipating or anonymously participating students did not differ significantly from the students that provided their registration number. Another potential limitation is that test anxiety levels were measured at a test station of the OSCE, which induces the possibility of changes in anxiety level during the examination, for example, a student who answered the questionnaire after performing a few stations may differ in perceived stress from a student that had finished most or all of the stations. Also, it recommended that this study be conducted with more sample and different years.
Conclusion
In summary, this study demonstrated that state anxiety was higher in dental students during four assessment methods: OSCE, written examination, preclinical crown and bridge preparation and endodontic. OSCE induced more anxiety than other assessment formats. The students reported better preparation for the OSCE and crown and bridge preparation and endodontic than for the oral medicine examination. Individuals with high anxiety levels reported better preparation; however, the scores obtained on the OSCE did not correlate with the state anxiety during the OSCE.
Financial support and sponsorship
Research Deputy, Kerman University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This study was supported by Kerman University of Medical Sciences. The authors would like to thank the Research Deputy for their financial support.
References
- 1.Katharine AM, Boursicot L, Trudie E. Using borderline methods to compare passing standards for OSCEs at graduation across three medical schools. Med Educ. 2007;41:1024–31. doi: 10.1111/j.1365-2923.2007.02857.x. [DOI] [PubMed] [Google Scholar]
- 2.Zeller A, Handschin D, Gyr N, Martina B, Battegay E. Blood pressure and heart rate of students undergoing a medical licensing examination. Blood Press. 2004;13:20–4. doi: 10.1080/08037050310025645. [DOI] [PubMed] [Google Scholar]
- 3.Brand HS, Schoonheim-Klein M. Is the OSCE more stressful? Examination anxiety and its consequences in different assessment methods in dental education. Eur J Dent Educ. 2009;13:147–53. doi: 10.1111/j.1600-0579.2008.00554.x. [DOI] [PubMed] [Google Scholar]
- 4.Al-Omari WM. Perceived sources of stress within a dental educational environment. J Contemp Dent Pract. 2005;6:64–74. [PubMed] [Google Scholar]
- 5.Muirhead V, Locker D. Canadian dental students’ perceptions of stress. J Can Dent Assoc. 2007;73:323. [PubMed] [Google Scholar]
- 6.Naidu RS, Adams JS, Simeon D, Persad S. Sources of stress and psychological disturbance among dental students in the West Indies. J Dent Educ. 2002;66:1021–30. [PubMed] [Google Scholar]
- 7.Ng V, Koh D, Mok BY, Chia SE, Lim LP. Salivary biomarkers associated with academic assessment stress among dental undergraduates. J Dent Educ. 2003;67:1091–4. [PubMed] [Google Scholar]
- 8.Rushforth HE. Objective structured clinical examination (OSCE): Review of literature and implications for nursing education. Nurse Educ Today. 2007;27:481–90. doi: 10.1016/j.nedt.2006.08.009. [DOI] [PubMed] [Google Scholar]
- 9.Kim J, Neilipovitz D, Cardinal P, Chiu M, Clinch J. A pilot study using high-fidelity simulation to formally evaluate performance in the resuscitation of critically ill patients: The university of Ottawa critical care medicine, high-fidelity simulation, and crisis resource management I study. Crit Care Med. 2006;34:2167–74. doi: 10.1097/01.CCM.0000229877.45125.CC. [DOI] [PubMed] [Google Scholar]
- 10.Barman A. Critiques on the objective structured clinical examination. Ann Acad Med Singapore. 2005;34:478–82. [PubMed] [Google Scholar]
- 11.Zartman RR, McWhorter AG, Seale NS, Boone WJ. Using OSCE-based evaluation: Curricular impact over time. J Dent Educ. 2002;66:1323–30. [PubMed] [Google Scholar]
- 12.Mossey PA, Newton JP, Stirrups DR. Scope of the OSCE in the assessment of clinical skills in dentistry. Br Dent J. 2001;190:323–6. doi: 10.1038/sj.bdj.4800961. [DOI] [PubMed] [Google Scholar]
- 13.Lie D, May W, Richter-Lagha R, Forest C, Banzali Y, Lohenry K. Adapting the McMaster-Ottawa scale and developing behavioral anchors for assessing performance in an interprofessional team observed structured clinical encounter. Med Educ Online. 2015;20:26691. doi: 10.3402/meo.v20.26691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Casey PM, Goepfert AR, Espey EL, Hammoud MM, Kaczmarczyk JM, Katz NT, et al. To the point: Reviews in medical education – The objective structured clinical examination. Am J Obstet Gynecol. 2009;200:25–34. doi: 10.1016/j.ajog.2008.09.878. [DOI] [PubMed] [Google Scholar]
- 15.Gerrow JD, Murphy HJ, Boyd MA, Scott DA. Concurrent validity of written and OSCE components of the Canadian dental certification examinations. J Dent Educ. 2003;67:896–901. [PubMed] [Google Scholar]
- 16.Graham R, Zubiaurre Bitzer LA, Anderson OR. Reliability and predictive validity of a comprehensive preclinical OSCE in dental education. J Dent Educ. 2013;77:161–7. [PubMed] [Google Scholar]
- 17.Simon SR, Bui A, Day S, Berti D, Volkan K. The relationship between second-year medical students’ OSCE scores and USMLE Step 2 scores. J Eval Clin Pract. 2007;13:901–5. doi: 10.1111/j.1365-2753.2006.00768.x. [DOI] [PubMed] [Google Scholar]
- 18.Cannick GF, Horowitz AM, Garr DR, Reed SG, Neville BW, Day TA, et al. Use of the OSCE to evaluate brief communication skills training for dental students. J Dent Educ. 2007;71:1203–9. [PMC free article] [PubMed] [Google Scholar]
- 19.Hannah A, Millichamp CJ, Ayers KM. A communication skills course for undergraduate dental students. J Dent Educ. 2004;68:970–7. [PubMed] [Google Scholar]
- 20.Hottel TL, Hardigan PC. Improvement in the interpersonal communication skills of dental students. J Dent Educ. 2005;69:281–4. [PubMed] [Google Scholar]
- 21.Grandy T, Westerman G, ErskineCombs C, Turner C. Perceptions of stress among third-year dental students. J Dent Educ. 1989;53:718–721. [PubMed] [Google Scholar]
- 22.Yan X, Yi Z, Wang X, Jinno Y, Zhang X, Koyano K, et al. Different study conditions between dental students in China and Japan. Int J Clin Exp Med. 2015;8:11396–403. [PMC free article] [PubMed] [Google Scholar]
- 23.Babar MG, Hasan SS, Ooi YJ, Ahmed SI, Wong PS, Ahmad SF, et al. Perceived sources of stress among Malaysian dental students. Int J Med Educ. 2015;6:56–61. doi: 10.5116/ijme.5521.3b2d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Breines JG, McInnis CM, Kuras YI, Thoma MV, Gianferante D, Hanlin L, et al. Self-compassionate young adults show lower salivary alpha-amylase responses to repeated psychosocial stress. Self Identity. 2015;14:390–402. doi: 10.1080/15298868.2015.1005659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Julian LJ. Measures of Anxiety. Arthritis Care Res (Hoboken) 2011;63:10. doi: 10.1002/acr.20561. 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Marshall G, Jones N. A pilot study into anxiety induced by various assessment methods. Radiography. 2003;9:185–91. [Google Scholar]
- 27.Furlong E, Fox P, Lavin M, Collins R. Oncology nursing students’ views of a modified OSCE. Eur J Oncol Nurs. 2005;9:351–9. doi: 10.1016/j.ejon.2005.03.001. [DOI] [PubMed] [Google Scholar]
- 28.Brosnan M, Evans W, Brosnan E, Brown G. Implementing objective structured clinical skills evaluation (OSCE) in nurse registration programmes in a centre in Ireland: A utilisation focused evaluation. Nurse Educ Today. 2006;26:115–22. doi: 10.1016/j.nedt.2005.08.003. [DOI] [PubMed] [Google Scholar]
- 29.LeBlanc VR, Bandiera GW. The effects of examination stress on the performance of emergency medicine residents. Med Educ. 2007;41:556–64. doi: 10.1111/j.1365-2923.2007.02765.x. [DOI] [PubMed] [Google Scholar]
- 30.Schoonheim-Klein M, Hoogstraten J, Habets L, Aartman I, Van der Vleuten C, Manogue M, et al. Language background and OSCE performance: A study of potential bias. Eur J Dent Educ. 2007;11:222–9. doi: 10.1111/j.1600-0579.2007.00459.x. [DOI] [PubMed] [Google Scholar]
- 31.Troncon LE. Clinical skills assessment: Limitations to the introduction of an “OSCE” (Objective Structured Clinical Examination) in a traditional Brazilian medical school. Sao Paulo Med J. 2004;122:12–7. doi: 10.1590/S1516-31802004000100004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sanders AE, Lushington K. Effect of perceived stress on student performance in dental school. J Dent Educ. 2002;66:75–81. [PubMed] [Google Scholar]
- 33.Keil RM. Coping and stress: A conceptual analysis. J Adv Nurs. 2004;45:659–65. doi: 10.1046/j.1365-2648.2003.02955.x. [DOI] [PubMed] [Google Scholar]
- 34.Westerman GH, Grandy TG, Ocanto RA, Erskine CG. Perceived sources of stress in the dental school environment. J Dent Educ. 1993;57:225–31. 34. [PubMed] [Google Scholar]
- 35.Reteguiz JA. Relationship between anxiety and standardized patient test performance in the medicine clerkship. J Gen Intern Med. 2006;21:415–8. doi: 10.1111/j.1525-1497.2006.00419.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Anderson M, Stickley T. Finding reality: The use of objective structured clinical examination (OSCE) in the assessment of mental health nursing students interpersonal skills. Nurse Educ Pract. 2002;2:160–8. doi: 10.1054/nepr.2002.0067. [DOI] [PubMed] [Google Scholar]
- 37.Chapell MS, Blanding B, Silverstein ME. Test anxiety and academic performance in undergraduate and graduate students. J Educ Psychol. 2005;97:268–74. [Google Scholar]
- 38.Divaris K, Barlow PJ, Chendea SA, Cheong WS, Dounis A, Dragan IF, et al. The academic environment: The students’ perspective. Eur J Dent Educ. 2008;12 Suppl 1:120–30. doi: 10.1111/j.1600-0579.2007.00494.x. [DOI] [PubMed] [Google Scholar]
- 39.Marylène Gagné M, Deci E. Self-determination theory and work motivation. J Organ Behav. 2005;4:331–62. [Google Scholar]
- 40.Mavis BE. Does studying for an objective structured clinical examination make a difference? Med Educ. 2000;34:808–12. doi: 10.1046/j.1365-2923.2000.00687.x. [DOI] [PubMed] [Google Scholar]
- 41.41 Haq I, Higham J, Morris R, Dacre J. Effect of ethnicity and gender on performance in undergraduate medical examinations. Med Educ. 2005;39:1126–8. doi: 10.1111/j.1365-2929.2005.02319.x. [DOI] [PubMed] [Google Scholar]
- 42.Wiskin CM, Allan TF, Skelton JR. Gender as a variable in the assessment of final year degree-level communication skills. Med Educ. 2004;38:129–37. doi: 10.1111/j.1365-2923.2004.01746.x. [DOI] [PubMed] [Google Scholar]
- 43.Cecchini JJ, Friedman N. First-year dental students: Relationship between stress and performance. Int J Psychosom. 1987;34:17–9. [PubMed] [Google Scholar]