

Abstract
CONTEXT:
Type 2 diabetes is the modern epidemic wherein patient care needs multiple approaches, education, and self-awareness being one of them. There are some knowledge, attitude, and practice (KAP) studies from India but very few relating it with disease control.
AIMS:
We tried to study KAP of treated type 2 diabetics and its correlation with glycemic control.
SETTINGS AND DESIGN:
Cross-sectional KAP study.
SUBJECTS AND METHODS:
We formulated KAP questionnaires in the form of KAP - 10 points for each and total 30. We recruited 200 type 2 diabetics (96 males, 104 females) treated by MD physicians with known current glycemic status. They were asked KAP questionnaires one to one by a direct interview in local language and results were associated with various factors and glycemic control.
RESULTS:
KAP score on was average 19 out of 30 in type 2 diabetics having mean age 58 years, mean duration 9 years. KAP score was unaffected by gender, occupation, duration of disease but significantly affected by current age, and education level. Only 40% patients had good glycemic control who scored better KAP than poor glycemic. There was positive correlation between KAP score and glycemic control, with significance for only glycosylated hemoglobin and not fasting blood sugar, postprandial blood sugar.
CONCLUSIONS:
Physician treated type 2 diabetics of our region had moderate KAP score, affected by age, education which suggested to affect glycemic control. Lacunae in knowledge regarding incurability of disease, attitudes toward complication, self-care, and good practices like walking, enriching knowledge need improvement so as an optimum glycemic control.
Keywords: Attitude, glycemic control, knowledge, practice, type 2 diabetes
Introduction
Prevalence of type 2 diabetes is on the global rise, more so in developing countries like India due to rapid urbanization.[1] Education is likely to be effective if we know the characteristics of the patients, and we should have ample data on the population's knowledge, attitude, and practice (KAP) of diabetes.[2] Self-care, awareness, and education is lacking in our diabetics than those from the Western world[2] and the majority are treated pharmacologically.[3] A lot is spent behind diagnosis and treatment of the diseases[4] but priceless advices regarding does and don’ts are not given or at times neglected by the patient himself. Indian KAP studies in type 2 diabetics have highlighted limited knowledge of treatment duration, complications and dietary modification,[5] unsatisfactory attitude and practices toward prevention and control of diabetes,[6] deficient self-care,[7] and poor disease awareness as a cause of the high prevalence of disease.[8] Few interventional studies are also known suggesting the positive outcome of patient education in terms of foot care,[9] self-care practices,[10] and better KAP score.[11] Most epidemiological studies have not correlated KAP-level with current glycemic status. We aimed to assess KAP of type 2 diabetics to quantify awareness of those who are actually suffering from it and to correlate the same with current disease control to test the hypothesis that health literacy has a positive impact on disease control and better prognosis for type 2 diabetes a life-long companion of the patient.
Subjects and Methods
Study type and subjects
We conducted cross-sectional observational KAP study under the guidance of Physiology Department of our Government Medical College. Two hundred under treatment type 2 diabetes patients (96 males and 104 females) attending private clinics or a Teaching Government Hospital with known glycemic control were enrolled. Prior permission of Department of Physiology was followed by approval of Institutional Review Board of our college. Permission from the physicians and written consent from subjects undergoing study were taken, and patients were informed about indirect benefit and aim of this study.
Selection criteria
We included type 2 diabetics of either sex, ready for written consent and subjects who can answer the questions of KAP study. We excluded subjects not ready for written consent, giving incomplete KAP or not having a recent report of disease control. The initial assessment was done in the form of personal details, disease history, drug history, personal history, laboratory investigations, and any other significant detail.
Glycemic control definition
We defined normative parameters for standard blood glucose control for study as per American Diabetes Association guidelines 2014.[12] Glycemic control was defined as glycosylated hemoglobin (HbA1C) <7 mg/dL, fasting blood sugar (FBS) <130 mg/dL, and postprandial blood sugar (PP2BS) <180 mg/dL.
Knowledge, attitude, and practice questions to be used
We made predesigned, prevalidated questionnaires containing 30 questions in local language.
Ten each was allotted to assess KAP of diabetics, all being direct questions and the total score was 30.
Statistical analysis
Results of KAP study were expressed as the frequency distribution of respondent's KAP in the true sense. All calculations were accomplished by using GraphPad InStat 3 software (demo version free software of GraphPad Software, Inc., California, USA). We calculated the statistical significance difference in the mean distribution of various parameters among various subgroups by Student's t-test for parametric distribution and by Mann–Whitney U-test for nonparametric distribution. Correlation between various variables was assessed for significance using Pearson's correlation test. The difference was considered statistically significant with P < 0.05.
Results
Patient characteristics and clinical profile of study group
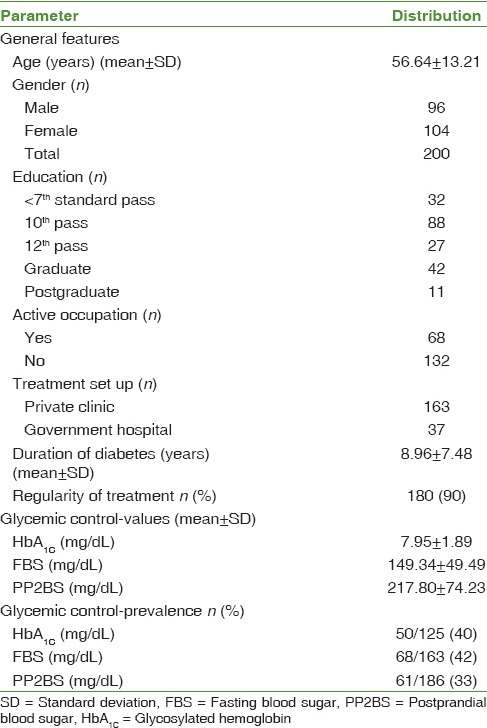
We included 200 type 2 diabetics giving complete answers of KAP form to analyze KAP regarding the disease among the outdoor patients. As shown in Table 1 mean age was 56.64 years, with equal representation of either sex or education below 10th in 140 (70%) cases, only 34% being involved in the active occupation. All 200 subjects were treated by MD physicians, predominantly private practitioners. Mean duration of disease was 9 years and all but 10% took regular treatment. Average HbA1C (7.95 ± 1.89), FBS (149.34 ± 49.49), and PP2BS (217.80 ± 74.23) were on the higher side and as per standard therapeutic guidelines, glycemic control was present only in 40%, 42%, and 33%, respectively, for these three parameters [Table 1].
Table 1.
Baseline data of type 2 diabetics under study (n=200)
Knowledge regarding type 2 diabetes
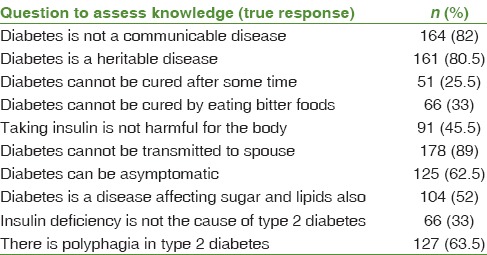
The mode of transmission of disease was misbelieved by 18% as communicable, 19.5% as noninheritable, and 11% as vertically transmissible. There were cases believing that it could be totally cured (74.5%) and cured by bitter food (67%), the prevalence of both being surprisingly high. Regarding symptomology, asymptomatic nature was known by only 62.5% and nearly same proportion (63.5%) was aware of polyphagia as a symptom of type 2 diabetes. Less than half (48%) respondents were thinking that their disease affects only sugar and not lipids. Only one-third type 2 diabetics knew that insulin is not deficient in the type of diabetes mellitus (DM) they had, and 45.5% did not agree on insulin being not harmful [Table 2].
Table 2.
Frequency distribution of respondents’ knowledge regarding type 2 diabetes
Attitude toward type 2 diabetes
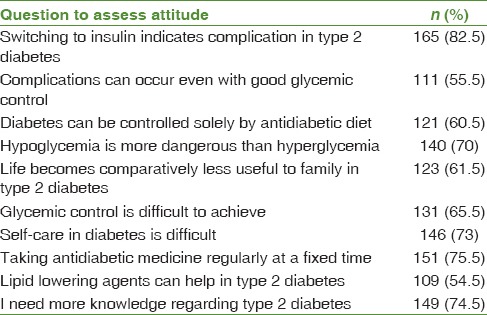
On inquiring about the time course of disease, 82.5% rightly understood that switching to insulin indicates complication, 70% were aware about hypoglycemia being more dangerous than hyperglycemia, and 55.5% had the bad attitude that there can be complications despite good glycemic control. 60.5% respondents were having faith only in diet control apart from treatment for glycemic control, which thought to be difficult to achieve by 65.5%. 61.5% were of the opinion that life becomes less useful after disease for family, and only 27% were confident about self care. Nearly, 75% were taking medication at fixed time, and lipid lowering was thought to be useful in type 2 diabetes by only half. Yet, 3 out of 4 agreed that they need enrichment about their knowledge of the disease [Table 3].
Table 3.
Frequency distribution of respondents’ attitude regarding type 2 diabetes
Practices of type 2 diabetics
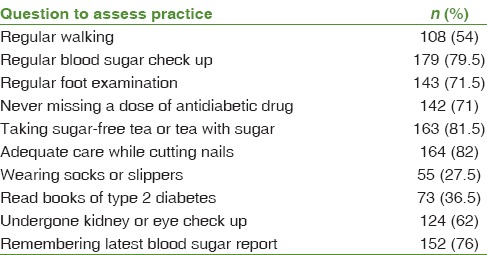
Good practices like avoiding sugar in tea, regular foot examination, and care while nail cutting were prevalent fairly good. But only half had a practice of regular walking and foot care in the form of wearing socks (27.5%), and habit of reading a book related to diabetes (36.5%) were prevailing with a low percentage. Good number of subjects had a checkup for retinopathy or nephropathy for once at least. Though 79.5% subjects were having regular glycemic control report done, just 76% remembered their last report [Table 4].
Table 4.
Frequency distribution of respondents’ practices regarding type 2 diabetes
Effect of characteristic features and glycemic control on knowledge, attitude, and practice score
In general total KAP score was 19 out of 30, but it was unaffected by gender, active occupation, duration of diabetes, and age at onset of diabetes. However, subjects with age more than or equal to 60 years had significantly higher KAP score than those with < 60 years. Similarly, subjects having education beyond standard 10 had significantly higher KAP score than those below or up to standard 10 [Table 5]. KAP scores correlated negatively with all three parameters of glucose triad but were significant only for HbA1C and not for fasting, as well as PP2BS [Table 6]. Comparison of the effect of strict glycemic control revealed that KAP score was better in those having good control than those without it, wherein statistical significance was evident for correlation with attitude and total KAP score with respect to nearly all three measures of glycemic control [Table 7].
Table 5.
Factors associated with KAP score in the study group (n=200)
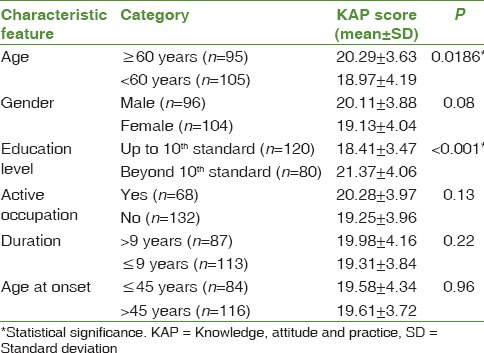
Table 6.
Correlation between current glycemic control values and KAP score
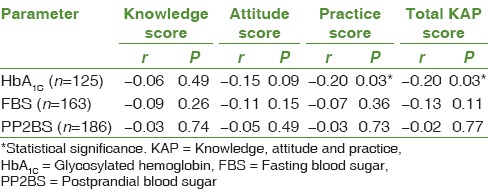
Table 7.
Quantitative comparison of KAP score among groups of respondent type 2 diabetics based on glycemic control status defined by guidelines of ADA 2014

Discussion
Type 2 diabetes is a chronic disease making patient compliance the most important factor to fight against it.[13] Patient compliance can be effectively increased by self-awareness helping adopt healthy diet and lifestyle, regular glycemic checkups, and periodic screening.[13] A previous KAP study done in our region on outdoor type 2 diabetics attending government hospitals showed poor KAP and inadequacy of time allotted by doctors.[2] By including patients from government and predominantly private set up we tried to explore it further, correlating it with disease duration and gender also. We included more questions to inquire their KAP and tried to correlate them with a current glycemic status that was taken as a mean to judge the adequacy of disease control.
We found fairly good knowledge among type 2 diabetics regarding mode of transmission but still few were unaware about it, in line with previous studies.[2,6,8,14,15] Better score can be attributable to the fact that majority were treated by physicians at private set-ups like the patients of richer countries,[16,17] comparatively good educational status with nearly 84% having passed secondary school exam, and higher average duration of disease (9 years) in the study group.[2,18] Nearly, 3 out of 4 surprisingly believed that it can be cured and that too by eating bitter things, alike a previous study done in our region[2] and another Indian study.[15] Such misbelieves must be removed by patient education as it may lead to noncompliance to treatment in years to come looking at the chronicity of disease, in a country like India where nearly 85–90% type 2 diabetics are noncomplaint.[19] Nearly, 40% were unaware about asymptomatic nature and polyphagia was not known to them despite having the disease for on average 9 years. The highest lacunae in knowledge was with regard to insulin and type 2 diabetes, where nearly half were not aware about insulin level in their type of diabetes misinterpreting insulin injection as harmful for the body. The same was observation regarding insulin among other type 2 diabetics as documented in a recent study.[13] This highlights ignorance of subjects regarding symptomology and modes of treatment, which may affect disease control adversely. The goals of management for patients with diabetes include optimization of blood glucose control, prevention of immediate complications, and prevention of long-term complications.[20] All treatment factors, diet, drugs, and exercise, have to be carefully managed on a daily basis by patients themselves. Patients must also be able to recognize when they need professional help. Successful self-management depends heavily on initial education about the interaction of all the treatment factors and ongoing support and reinforcement. Education of patients with diabetes is considered a fundamental aspect of diabetes care.[21] It is the health literacy that matters more than mere awareness that an incurable disease is present.
Attitude regarding regularity for hypoglycemic drug, usefulness of hypolipidemic drug, and switching on to insulin in complications were positive in majority but still considerable number of type 2 diabetics believed that complications can occur despite good glycemic control, that too being understood as difficult to achieve and many relied upon only diet control in addition to medicines. These may be the cause why glycemic control was substandard in our case group having majority of patients affording private consultancy and counseling for same should be done. Nearly, three-fifth cases believed that life become less useful for family and this could be the reason for lesser involvement of cases in active occupations. Same is reflected as an adverse outcome that only 27% type 2 diabetics were self care confident which is lower than other studies.[2,14] Moreover, it is also true that patient education improves self care practices of type 2 diabetics.[9,10] Patients who are regularly involved in self-care practices have achieved better glycemic control.[22] A recent study has reviewed that employment and diabetes need to be given due care and subjects should be motivated to live an active life that ultimately benefits them for better prognosis.[23] Still the most encouraging thing is that 3 out of 4 respondents agreed upon felt need for further knowledge regarding diabetes. A recent phenomenology qualitative research done regarding physical, mental, social, and spiritual attitudes of type 2 diabetics has identified a number of key themes that may be useful in upgrading awareness of the experience and attitudes of type 2 diabetics.[24] Our results need consideration in designing and publicizing educational initiatives aimed for promoting patient management specific to our population.
Evaluation of practice part revealed that good practices like routine glycemic checkup, remembering recent report, avoiding sugar in tea, foot care practices, and checkups for complications were prevailing good. But walking that benefits diabetics in multiple ways[25] was neglected by most and just one-third subjects had read books or literature regarding diabetes. Subjects must be motivated for exercise that can improve their physical and mental makeup that ultimately benefits them. In line with conclusion of Kishore et al., subjects need to be made aware of the asymptomatic phase of DM and its long-term complications while, at the same time, they should be sensitized about the importance of taking regular treatment and management.[26] Good practices can simply lessen the burden of complications like diabetic foot which are end-results of negligence toward primary prevention by patients themselves. Diabetic group education, though in effect and have been effective in the Western world,[27] is still not popularized in our country and can help to further raise the KAP and disease control.
Males and females were not much different in their KAP score contradictory to other studies which found better KAP in males than females where subjects belonged to lower socioeconomic class and females had low literacy, as well as health literacy.[2,28,29] KAP score improved with age like other studies[2,23] significantly even if we excluded newly diagnosed patients,[7] mean duration being 9 years. Education was a significant factor affecting KAP score in line with the previous study.[28] Literacy itself affects health literacy that gives better self-awareness, better compliance, and better outcome.[30] Shah et al.[2] mentioned in his previous study that type 2 diabetics of our region believes in self-care and are ready to change but sometimes they are not given adequate time by the physicians. Physicians should rather encourage type 2 diabetics to participate in diabetes education and argue that patients can profit even if actual treatment and examination results are promising.[27] Of all significant correlates of KAP, education is the only modifiable risk factor. Fortunately, literacy is now made fundamental right in India and can potentially help in the management of type 2 diabetes effectively as inferred by Al-Maskari et al.[31]
Type 2 diabetics with better glycemic control had higher knowledge score, attitude score, practice score, and total KAP score than those with poor control. Rather reciprocally lesser KAP affects the fulfillment of required norms for the management of diabetes, absence of which worsens hyperglycemia. This unchecked and asymptomatic hyperglycemia, lack of awareness about either complications[32] and prevention of same by good glycemic control,[33] imposes risk for various complications. Correlation of KAP was significant with HbA1C, and not for FBS and PP2BS, which are less reliable for ultimate measure of disease control. A study has shown that patient's knowledge of recent HbA1C helps in better management.[34] A study done in UAE revealed that knowledge, practice, and attitude scores in type 2 diabetics were all statistically significantly positively, but rather weakly, associated, but none of them was significantly correlated with HbA1C, contradictory to us.[31] Indians in general and people of our region have substandard glucose control,[35] and it can be due to inadequate awareness about the same owing to poor knowledge, bad attitude, and poor practices.[2] Sheer number, lack of awareness, and suboptimum disease control make T2DM worse scenario for India.[36] Reinforcement of the same can serve as effective and cheap primary prevention if applied adequately. Better education leads to better self-care that ends in better glycemic, hence the disease control.[22] Patient education programs are thus the need of this hour and must be insinuated depending upon population characteristics of a particular region.
Our study was limited by moderate sample size, homogeneity of subjects, recall bias of patients, subjective, observational nature of study and unavailability of all reports of glycemic control in each subject. Yet, it revealed the KAP status of type 2 diabetics in our region ranking among top five in the country, poor glycemic control and contribution of low KAP score. It suggests need for patient education and awareness to minimize the aftermaths of this disease that cannot be cured. Prevention is always better than cure, and good KAP leads to better disease control as per this study and many complications can be primarily prevented by patients’ health literacy, a cost-effective tool.
Conclusions
In type 2 diabetics treated by private MD physicians, predominantly from private set-up, we found moderate KAP score and 40% prevalence of strict glycemic control. Good glycemics scored better than poor glycemics, where glucose triad correlated positively with KAP but significant only for HbA1C. Lacunae in knowledge regarding nature and incurability of disease, attitudes toward complication, self-care and usefulness of life, and good practices like walking and enriching knowledge regarding type 2 diabetes need improvement so as a strict glycemic control.
Financial support and sponsorship
This study was selected, approved and funded by Indian Council of Medical Research under short-term studentship program 2014.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We are thankful to Department of Physiology, Government Medical College, Bhavnagar, Gujarat, India for allowing us to conduct this study. We are also thankful to Dr. Rahul Shridhrani, Dr. Panna Kamdar, Dr. Pradeep Joshi, and other MD physicians for allowing this study. We acknowledge the support of Indian Council of Medical Research for selecting, approving and funding this project under short-term studentship program 2014.
References
- 1.Cheema A, Adeloye D, Sidhu S, Sridhar D, Chan KY. Urbanization and prevalence of type 2 diabetes in Southern Asia: A systematic analysis. J Glob Health. 2014;4:010404. doi: 10.7189/jogh.04.010404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shah VN, Kamdar PK, Shah N. Assessing the knowledge, attitudes and practice of type 2 diabetes among patients of Saurashtra region, Gujarat. Int J Diabetes Dev Ctries. 2009;29:118–22. doi: 10.4103/0973-3930.54288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.American Diabetes Association. Standards of medical care in diabetes-2010. Diabetes Care. 2010;33(Suppl 1):S11–61. doi: 10.2337/dc10-S011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ramachandran A, Ramachandran S, Snehalatha C, Augustine C, Murugesan N, Viswanathan V, et al. Increasing expenditure on health care incurred by diabetic subjects in a developing country: A study from India. Diabetes Care. 2007;30:252–6. doi: 10.2337/dc06-0144. [DOI] [PubMed] [Google Scholar]
- 5.Bawa MS, Patil AR. Study to assess awareness, attitude, practices & risk factors amongst type 2 diabetes patients attending rural health training center in Maharashtra. Int J Health Sci Res. 2014;4:21–5. [Google Scholar]
- 6.Satyanarayana TB, Mahendrappa SK. A cross sectional study of knowledge, attitude and practice among patients with type 2 diabetes mellitus at a tertiary care hospital. J Evol Med Dent Sci. 2014;3:5317–21. [Google Scholar]
- 7.Raithatha SJ, Shankar SU, Dinesh K. Self-care practices among diabetic patients in Anand District of Gujarat. ISRN Family Med 2014. 2014:743791. doi: 10.1155/2014/743791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kide S, Rangari A, Shiral R, Mane N, Yadav P, Ambulkar K, et al. Knowledge and awareness of diabetes amongst diabetes patients in Wardha region. Int J Diabetes Dev Ctries. 2014;34(4):232–232. [Google Scholar]
- 9.Saurabh S, Sarkar S, Selvaraj K, Kar SS, Kumar SG, Roy G. Effectiveness of foot care education among people with type 2 diabetes in rural Puducherry, India. Indian J Endocrinol Metab. 2014;18:106–10. doi: 10.4103/2230-8210.126587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Gujrathi A, Dhakne S, Almale B, Mahale M, Vankudre A, Gosavi S. Impact of community based diabetic patient education on glycaemic status, life style and self care practices among type 2 diabetes patients in an urban slum of Mumbai, India. Int J Interdiscip Multidiscip Stud. 2014;1:279–87. [Google Scholar]
- 11.Malathy R, Narmadha MP, Ramesh S, Alvin JM, Babu ND. Effect of a diabetes counseling programm on knowledge, attitude and practice among diabetic patients in Erode district of South India. Pharm Pract. 2011;3:65–72. doi: 10.4103/0975-1483.76422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.American Diabetes Association. Standards of medical care in diabetes-2014. Diabetes Care. 2014;37(Suppl 1):S14–80. doi: 10.2337/dc14-S014. [DOI] [PubMed] [Google Scholar]
- 13.Baruah MP, Pathak A, Kalra S, Das AK, Zargar AH, Bajaj S, et al. A revisit to prevailing care and challenges of managing diabetes in India: Focus on regional disparities. Indian J Endocrinol Metab. 2014;18:254–63. doi: 10.4103/2230-8210.131113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lakshman RL, Nuthi S, Valsangkar S. An assessment of knowledge and self care practice amongst diabetics in an urban area. MRIMS J Health Sci. 2014;2:11–4. [Google Scholar]
- 15.Rujul D, Vadgama P, Parth D. Effect of awareness of diabetes on clinical outcomes of diabetes: An observational study at a private hospital in Gujarat. Natl J Med Res. 2012;2:493–6. [Google Scholar]
- 16.Al Bimani ZS, Khan SA, David P. Evaluation of T2DM related knowledge and practices of Omani patients. Saudi Pharm J. 2015;23:22–7. doi: 10.1016/j.jsps.2013.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wang H, Song Z, Ba Y, Zhu L, Wen Y. Nutritional and eating education improves knowledge and practice of patients with type 2 diabetes concerning dietary intake and blood glucose control in an outlying city of China. Public Health Nutr. 2014;17:2351–8. doi: 10.1017/S1368980013002735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Perera DP, De Silva RE, Perera WL. Knowledge of diabetes among type 2 diabetes patients attending a primary health care clinic in Sri Lanka. East Mediterr Health J. 2013;19:644–8. [PubMed] [Google Scholar]
- 19.Lahiri SK, Haldar D, Chowdhury SP, Sarkar GN, Bhadury S, Datta UK. Junctures to the therapeutic goal of diabetes mellitus: Experience in a tertiary care hospital of Kolkata. J Midlife Health. 2011;2:31–6. doi: 10.4103/0976-7800.83271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Piette JD, Glasgow R. Education and home glucose monitoring. In: Gerstein HC, Haynes RB, editors. Evidenced-Based Diabetes Care. Vol. 1. London: BC Decker; pp. 207–51. [Google Scholar]
- 21.NICE. Guidance on the Use of Patient-Education Models for Diabetes. Technology Appraisal 60. London: National Institute for Clinical Excellence; 2003. [Google Scholar]
- 22.Padma K, Bele SD, Bodhare TN, Valsangkar S. Evaluation of knowledge and self care practices in diabetic patients and their role in disease management. Natl Med J India. 2012;3:3–6. [Google Scholar]
- 23.American Diabetes Association. Diabetes and employment. Diabetes Care. 2011;34(Suppl 1):S82–6. doi: 10.2337/dc11-S082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Abolghasemi R, Sedaghat M. The patient's attitude toward type 2 diabetes mellitus, a qualitative study. J Relig Health. 2015;54:1191–205. doi: 10.1007/s10943-014-9848-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Di Loreto C, Fanelli C, Lucidi P, Murdolo G, De Cicco A, Parlanti N, et al. Make your diabetic patients walk: Long-term impact of different amounts of physical activity on type 2 diabetes. Diabetes Care. 2005;28:1295–302. doi: 10.2337/diacare.28.6.1295. [DOI] [PubMed] [Google Scholar]
- 26.Kishore J, Kohli C, Gupta N, Kumar N, Sharma P. Awareness, practices and treatment seeking behavior of type 2 diabetes mellitus patients in Delhi. Ann Med Health Sci Res. 2015;5:266–73. doi: 10.4103/2141-9248.160184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Schäfer I, Pawels M, Küver C, Pohontsch NJ, Scherer M, van den Bussche H, et al. Strategies for improving participation in diabetes education. A qualitative study. PLoS One. 2014;9:e95035. doi: 10.1371/journal.pone.0095035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.George H, Rakesh P, Krishna M, Alex R, Abraham VJ, George K, et al. Foot care knowledge and practices and the prevalence of peripheral neuropathy among people with diabetes attending a secondary care rural hospital in Southern India. J Family Med Prim Care. 2013;2:27–32. doi: 10.4103/2249-4863.109938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sandhu K, Sachdeva R. Food habits, lifestyle, knowledge, attitude and practices of male diabetic subjects as influenced by nutrition counseling. Asian J Dairy Foods Res. 2013;32:220–7. [Google Scholar]
- 30.Adams RJ. Improving health outcomes with better patient understanding and education. Risk Manag Healthc Policy. 2010;3:61–72. doi: 10.2147/RMHP.S7500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Al-Maskari F, El-Sadig M, Al-Kaabi JM, Afandi B, Nagelkerke N, Yeatts KB. Knowledge, attitude and practices of diabetic patients in the United Arab Emirates. PLoS One. 2013;8:e52857. doi: 10.1371/journal.pone.0052857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mohan D, Raj D, Shanthirani CS, Datta M, Unwin NC, Kapur A, et al. Awareness and knowledge of diabetes in Chennai – The Chennai Urban Rural Epidemiology Study [CURES-9] J Assoc Physicians India. 2005;53:283–7. [PubMed] [Google Scholar]
- 33.Mehrotra R, Bajaj S, Kumar D, Singh KJ. Influence of education and occupation on knowledge about diabetes control. Natl Med J India. 2000;13:293–6. [PubMed] [Google Scholar]
- 34.Heisler M, Piette JD, Spencer M, Kieffer E, Vijan S. The relationship between knowledge of recent HbA1c values and diabetes care understanding and self-management. Diabetes Care. 2005;28:816–22. doi: 10.2337/diacare.28.4.816. [DOI] [PubMed] [Google Scholar]
- 35.Solanki JD, Makwana AH, Mehta HB, Gokhale PA, Shah CJ. A study of prevalence and association of risk factors for diabetic vasculopathy in an urban area of Gujarat. J Family Med Prim Care. 2013;2:360–4. doi: 10.4103/2249-4863.123906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Joshi SR, Das AK, Vijay VJ, Mohan V. Challenges in diabetes care in India: Sheer numbers, lack of awareness and inadequate control. J Assoc Physicians India. 2008;56:443–50. [PubMed] [Google Scholar]