

Abstract
Purpose
To determine how adolescents and young adults (AYAs) use social media to share health information and to assess attitudes towards using social media to obtain health information and communicate with medical providers.
Methods
A cross-sectional study of AYAs, 12 years or older, attending a primary care adolescent and young adult clinic. Participants completed an anonymous survey about health-related social media use, personal health, and communication with their healthcare team.
Results
Of 244 patients approached, 204 enrolled (83.6% participation rate). Almost all (98%) had used social media within the prior month, but only 51.5% had shared health information in these networks. These participants shared about mood (76.2%), wellness (57.1%), and acute medical conditions (41.9%). Those with self-reported poor health were more likely to share health information than other groups. Privacy was the most important factor determining which platform to use. Only 25% thought social media could provide them with useful health information. Few AYAs connected with their healthcare team on social media and most did not want to use this method; texting was preferred.
Conclusions
AYAs maintain their privacy on social media regarding their health. Those with self-perceived poor health are more likely to share health information, potentially biasing online content and impairing the generalizability of social media research. AYAs do not view social media as a useful source of health information, which may limit the utility of public health messages through these platforms, and it may not be adequate for communication between patients and their healthcare team.
Keywords: social media, adolescent health, young adult, health information technology, privacy
Adolescents and young adults (AYAs) have the highest rates of social media use of any age group.1,2 Social media allows users to create, share, and exchange information and ideas in virtual networks, and it has the potential to revolutionize healthcare in a variety of ways. First, patients may benefit from social media by obtaining health information, connecting with others with similar conditions, and joining online support groups, which can enhance patient empowerment3 and may improve outcomes.4 Second, physicians may use the “digital phenotype,” or online behavior and data of their patients, to complement clinical information to obtain better diagnostic and prognostic information.5 Physicians may also leverage the popularity of social media among AYAs to enhance communication with their patients. Third, researchers can use social media to recruit patients with rare conditions,6 estimate the extent of disease outbreaks,7 and bring increased understanding of conditions via health behaviors reported online.8,9 Finally, public health departments can distribute messages for staying healthy and increase awareness of various diseases through social media.10,11
However, these potential benefits of social media rely on the type and quality of information that users voluntarily share and on their perception of the content produced in this medium. Although AYAs share a lot of personal information online—including pictures and videos, interests, relationship status, names of schools, birthdates, and email addresses12—they are conscious about maintaining privacy, control the information that others can see, and carefully manage their online reputation.12,13 How and why AYAs decide to share information about their health on social media remains an under-explored topic, yet its understanding will be essential if we are to leverage social media to improve health.
This study aims to explore the manners in which AYAs obtain and share health information on social media and to assess attitudes towards the use of social media as a method of communication between patients, physicians, and public health organizations.
Methods
We enrolled a convenience sample of English- and Spanish-speaking patients, 12 years or older, visiting the Boston Children’s Hospital Adolescent and Young Adult Clinic. Research assistants approached patients in the clinic waiting room and asked if they would like to participate in a one-time, anonymous survey about social media use. Those who agreed to participate were offered options of taking the survey on paper or online from their own wireless device, using a web link or QR code. Participants received a $5 gift card for completing the survey. Participants were recruited from January – July 2015 until the pre-specified enrollment of 200 was reached. The Boston Children’s Hospital Committee on Clinical Investigation approved this study. Consent was implied by survey completion, and parental permission was waived.
Study data were managed using REDCap electronic data capture tools hosted at Boston Children’s Hospital. Paper surveys were entered manually into REDCap by a research assistant. Ten percent of surveys were double-entered to ensure accuracy. Online surveys were directly entered by participants into REDCap.
Measures
Our questionnaire was modeled on a questionnaire for adults about social media use.14 A copy of our questionnaire is included in the online supplement. Participants were asked to select the devices they used to connect to the internet and to indicate the frequency of use of various social media platforms within the previous month. Participants were asked to rate their agreement on a 5-point Likert scale to the following phrase: “Social media can help me obtain useful health information.” Participants were asked whether they posted about various health topics on social media, which platforms they used, and why they shared this information online. Participants were asked to rate the importance of various privacy factors that affected their selection of social media sites to discuss their health. The responses “important” or “very important” were collapsed into a single category called “important” in our analyses because of the limited number of responses in some categories. Participants were asked whether they connected with someone from their healthcare team on Facebook or Twitter, and how they wished to communicate with them in the future.
Participants self-reported demographic information, including their age, gender, race, educational level, and primary language spoken at home. Participants were asked to rate their overall health as poor, fair, good, very good, or excellent, as well as to estimate their number of clinic or emergency room visits in the prior 6 months. For analysis, those reporting their health in negative or neutral terms (“poor” or “fair”) were grouped into the “poor health” group, while those reporting their health in positive terms (“good,” “very good,” or “excellent,”), were grouped into the “good health” group.
Statistics
Descriptive statistics are reported for all study variables. Age, gender, and race distributions of the survey sample were compared to administrative data describing the population of patients who visited the clinic in the calendar year 2015 using Fisher’s exact test. Associations between categorical survey variables were also assessed using Fisher’s exact test. The association between self-reported health and the number of clinic or emergency department visits within the prior 6 months was evaluated using the Wilcoxon rank-sum test. The odds of posting to social media were compared among age groups using logistic regression; pairwise differences among age groups were corrected for multiple comparisons using Tukey’s method. Analyses were conducted using SAS software version 9.3. All tests were 2-sided at the 0.05 significance level.
Results
Participants
We approached 244 patients in clinic; 204 patients agreed to participate and completed the survey, for an 83.6% participation rate. Participant characteristics are shown in Table 1. Participants who answered the survey were similar to the general clinic patient population seen in 2015 in regards to age distribution, but were more likely to be female (83.2% vs. 72.6%, p<0.001). Race could not be compared due to differences in how race was reported in the general clinic population and on our survey instrument. Participants who rated themselves as having poor health reported having had more clinic or emergency department visits within the prior 6 months, as compared to participants who rated their health as good (p=0.0040).
Table 1.
Descriptive characteristics of 204 adolescents and young adults (AYA) responding to a survey about social media use and health between January and July, 2015.
| n (%) | ||
|---|---|---|
|
| ||
| Age | 12–14 | 23 (11.3) |
|
| ||
| 15–17 | 53 (26) | |
|
| ||
| 18–21 | 80 (39.2) | |
|
| ||
| 22 or older | 48 (23.5) | |
|
| ||
| Gender | Male | 34 (16.8) |
|
| ||
| Female | 168 (83.2) | |
|
|
||
| Race/Ethnicity | Non-Hispanic White | 60 (29.4) |
|
| ||
| Non-Hispanic Black | 63 (30.9) | |
|
| ||
| Asian or Pacific Islander | 9 (4.4) | |
|
| ||
| Hispanic | 50 (24.5) | |
|
| ||
| Other | 22 (10.8) | |
|
| ||
| Schooling | Enrolled in school or college | 152 (74.5) |
|
| ||
| Elementary school | 2 (1.3) | |
|
| ||
| Middle school (grades 7–8) | 19 (12.5) | |
|
| ||
| High school (grades 9–12) | 63 (41.4) | |
|
| ||
| College | 68 (44.7) | |
|
| ||
| If not enrolled, highest level completed | 52 (25.5) | |
|
| ||
| Middle school (grades 7–8) | 3 (5.8) | |
|
| ||
| High school (grades 9–12) | 20 (38.5) | |
|
| ||
| Some college | 7 (13.5) | |
|
| ||
| College degree | 22 (42.3) | |
|
| ||
| Primary language spoken at home | English | 178 (87.3) |
|
| ||
| Spanish | 16 (7.8) | |
|
| ||
| Haitian Creole | 3 (1.5) | |
|
| ||
| Portuguese/Portuguese creole | 2 (1) | |
|
| ||
| Chinese | 2 (1) | |
|
| ||
| Other | 3 (1.5) | |
|
| ||
| Self - perceived health | Poor | 7 (3.5) |
|
| ||
| Fair | 37 (18.5) | |
|
| ||
| Good | 85 (42.5) | |
|
| ||
| Very good | 59 (28.9) | |
|
| ||
| Excellent | 16 (8) | |
|
| ||
| Number of medical visits in prior 6 months | 1 | 38 (18.8) |
|
| ||
| 2–4 | 92 (45.5) | |
|
| ||
| 5–9 | 20 (9.9) | |
|
| ||
| 10 or more | 18 (8.9) | |
Internet and Social Media Use
Virtually all participants (99%) owned and used one or more devices to connect to the internet, including smartphones (96.1%), laptop computers (67.2%), tablets (44.6%), and desktop computers (19.1%). All but four participants (n=200, 98.0%) had used at least one social media site within the prior month. The distribution and frequency of social media use according to specific platforms are shown in Figure 1. Seventeen participants (8.4%) used one social media site, 58 (28.7%) used two, 55 (27.2%) used three, 43 (21.3%) used four, 17 (8.4%) used 5, and 5 (2.5%) used six social media sites. In addition, twenty-three participants (11.3%) wrote-in that they used SnapChat, which was not included in our survey.
Figure 1.
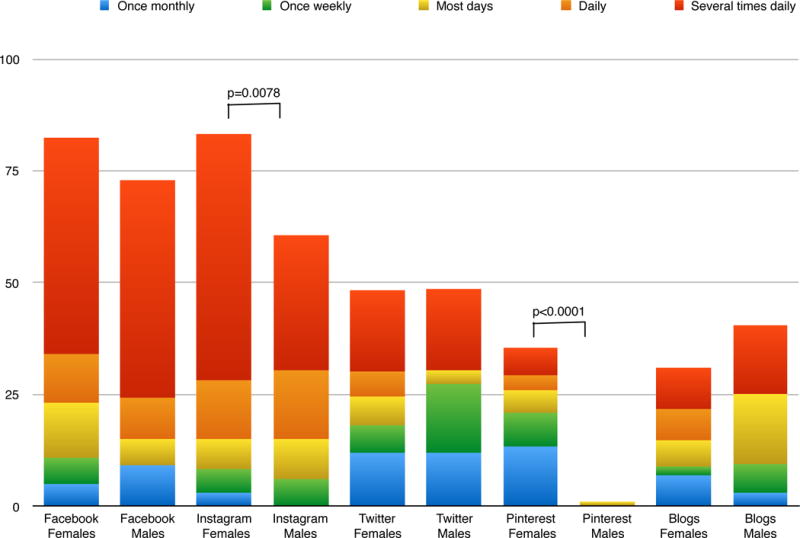
Distribution and frequency of social media use as reported by 204 adolescents and young adults responding to a survey about social media use and health between January and July, 2015.
Although Facebook, Twitter, and blog use were similarly prevalent among males and females, females were more likely than males to have used Instagram and Pinterest in the prior month (Instagram: 83.2% vs 60.6%, p=0.0078, Pinterest: 35.4% vs 3%, p=<0.0001). Participants who primarily spoke English at home were less likely than participants who spoke other languages to use Facebook (78.6% vs. 96.2%, p=0.0328). There were no other significant demographic differences in the use of other social media sites.
Posting on social media about health
One hundred and five participants (51.5%) had posted about their health on social media in the previous six months. Of these, 80 (76.2%) posted about mood, 62 (57.1%) posted about wellness and prevention, 44 (41.9%) posted about acute medical conditions, 13 (12.4%) posted about chronic medical conditions, and 10 (9.5%) posted about sexual health. Participants who shared health-related information gave a variety of reasons for doing so: 46 (43.8%) wanted to connect with others with similar conditions, 43 (41.0%) were seeking advice, 33 (31.4%) were looking for support, 28 (26.7%) wanted to share their health issue, 24 (22.9%) thought that it was fun, and 14 (13.3%) wanted to search for additional treatment options. Females reported sharing more health-related posts compared to males, a difference which approached statistical significance (55.4% vs 37.5%, p=0.0816). The 12–14 year-old age group was significantly less likely to post to social media about their health than the other age groups, (22.7% vs 56.2%, p=0.0033) despite the fact their overall social media usage did not differ (91.3% vs 97.2%, p=0.1829).
Of the 105 participants that shared health-related posts, the frequency of use of the various platforms was as follows: 61 (58.1%) posted on Facebook, 33 (31.4%) posted on Instagram, 28 (26.7%) posted on Twitter, 12 (11.4%) posted on blogs, 4 (3.8%) posted on Pinterest, and 15 (14.3%) posted on other social media sites. When asked about how they decided which site to use, the most frequently endorsed factor was privacy (the ability to control who is able to read the post), noted to be important by 76 participants (72.4%). Other important factors were the ability to share information with friends and family (n=67, 65.1%), the ability to share information with others with similar conditions (n= 54, 52.4%), the ability to remain anonymous (not having to share their real name, n= 47, 45.2%), and popularity among friends and family (n= 34, 32.7%).
Participants who rated themselves as having poor health were more likely to share health-related posts than participants who rated their health as good (67.4% vs 49.0%, p=0.0385). There were no significant differences in the topics discussed between the good and poor health groups. Participants with poor health were more likely than those with good health to post in order to share health issues (44.8% vs. 19.7%, p=0.0136), while those with good health were more likely to post because they thought it was fun (28.6% vs 6.9%, p=0.0185). There were no significant differences in other reasons for posting between the poor and good health groups.
Obtaining health information on social media
Only 51 respondents (25%) agreed or strongly agreed that social media could help them obtain useful health information, a figure that was significantly higher among those who posted to social media about their health, as compared to those who had not (n=35 of 105, 33.3%, vs. n=16 of 95, 16.8%, p=0.0092).
Connecting with the health care team
Very few participants indicated that they connected with one of their physicians, nurses, or social workers on Facebook (n=6, 2.9%) or Twitter (n=3, 1.5%). Participants were much more likely to use telephone (n=133, 65.2%), email (n=71, 34.8%), regular mail (n=25, 12.3%) or a patient portal (n=9, 4.4%) for communication. When asked how they would prefer to communicate with their primary care providers (PCPs) in the future, 108 respondents (52.9%) preferred text messaging, 47 participants (23%) an interactive clinic website or blog, 31 participants (15.2%) Facebook, and 3 participants (1.5%) Twitter. Participants were interested in these methods because they felt it would be easier to communicate (44.6%) and they would feel more connected to their provider (34.2%); allowing others to see and participate in their conversations was less commonly desired (4.5%). Notably, 75 participants (36.8%) were not interested in communicating with their PCPs with any of these methods.
Discussion
Half of AYAs surveyed in an urban adolescent clinic had shared information about their health on social media in the previous six months, most commonly regarding mood, wellness, and acute medical conditions. Participants were primarily looking to connect with others with similar conditions, seek advice, and receive support. Privacy was the most important factor in determining which social media platform to use when sharing about their health. Those who rated themselves as having poor health were more likely to share health information online; females were slightly more likely to report sharing health-related posts than males, although this was not statistically significant. One-quarter of participants thought social media could provide them with useful health information; fewer numbers were interested in connecting with their providers through these networks. These findings have important implications for patients, physicians, researchers, and public health organizations.
For patients, understanding the types of health content most commonly shared on social networks, as well as the users that typically share this information, may better allow them to evaluate the quality and applicability of user-generated health content. We found that mood was the most commonly shared health topic among AYAs—discussed by three-quarters of participants who shared health information. Prior studies have also demonstrated that users share information about mood on social networks networks.15 This is not surprising, given that psychological well-being is the most important factor related to the self-perceived health of AYAs.16 However, we build upon previous research by demonstrating that AYAs also share information about wellness and chronic medical conditions. In addition, we found that those with self-perceived poor health were more likely to share their health information online, potentially biasing user-generated health content; AYAs with self-perceived poor health were also more likely to find health information on social media useful. Thus, it is possible that negative sentiments from those with self-perceived poor health could spread to others through social media. A prior study of Facebook showed that emotional states, both positive and negative, can be transferred through this network.17 Other studies have shown that obesity18 and smoking19 also spread through social networks.
For physicians who aim to gain a better understanding of their patients through their “digital phenotype,”5 we found that only a minority of AYAs want to connect and share their online lives with members of their healthcare team. The reasons were not directly explored in our survey, although it is clear that privacy is important for these participants. AYAs already face challenges when deciding what information to share online due to “context collapse,”20 which occurs when disparate audiences view the same content. Most teens connect with friends, extended family members, siblings, and parents on social networks.12 Social media flattens these multiple audiences into one, making it difficult for AYAs to post content that will be understood and accepted by all audiences at the same time.20 Adding physicians to this mix may cause further challenges. In addition, despite the popularity of social media among AYAs, it may not improve communication between them and their physicians. We found that less than a quarter of our participants wanted to join a patient portal, and even fewer wanted to connect on social media. Instead, a system that allows private and immediate communication—text messaging—was favored by the majority of our participants.
For researchers, we demonstrate several limitations of social media use for health-related research. AYAs restrict health information shared on social media, potentially limiting the generalizations that can be obtained by analyzing online health content. A previous survey of teenagers similarly showed that only a third of adolescents discuss their personal health online.22 Further, AYAs most commonly choose to share health information in Facebook, the platform that provides the greatest privacy by restricting viewing of posts to “friends,” making it more difficult for researchers to access this content. Finally, online recruitment of study participants may be complicated by selection bias, since we found that those with self-perceived poor health are more likely to share health information than other groups.
Of interest to public health organizations, only a quarter of AYAs view social media as a useful source of health information. Our results may explain the poor engagement by the public in various social media campaigns by public health departments.10 Prior studies have shown that AYAs may not know where to find accurate health information, as they lack the ability to evaluate reliability and interpret the applicability of health information found online.23
Our study has several limitations. First, our results are based on self-reported data about social media use and health status, which may differ from actual use and status. However, a prior study showed that feelings of depression expressed on social media correlated well with symptoms of depression using a clinical scale,24 suggesting that patients share accurate health information online. Second, we had a relatively small number of males in our study, which may impair our ability to generalize male online behavior. Third, this was a single-center study in an urban population. Although our participant population was diverse, it may not be generalizable to the entire United States population. Fourth, given the rapidity of change within social media platforms, it is possible that their frequency of use may differ in the future. Nevertheless, attitudes about health information and privacy do not appear to be platform-dependent, and may remain applicable to other social networks.
In summary, despite the potential benefits of social media use to improve health, our study showed several barriers that may restrict its utility for these purposes. AYAs are protective in the types of personal information they share online—especially regarding their health—while remaining skeptical of health messages distributed through these networks. Health-related posts are more likely to be shared by those with self-reported poor health, potentially biasing online content. Furthermore, AYAs are do not want to use it to communicate with their healthcare teams. Discovering strategies to help overcome these barriers, such as improving the quality of online health content and teaching AYAs the skills to interpret this information, are essential before social media’s promise to improve health is attained.
Supplementary Material
Acknowledgments
We would like to thank all of the patients that participated in our research study. We have listed everyone who contributed significantly to this work. This work was supported by the Aerosmith Foundation. Dr. Holly Gooding is supported by the National Heart, Lung and Blood Institute—National Institutes of Health (K23HL122361-01A1).
Abbreviations
- AYA
adolescents and young adults
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interest: The authors have no conflicts of interest to disclose.
Implications and Contributions: This study found that adolescents and young adults limit health information shared on social media, do not find these platforms useful for learning about health, and do not want to connect with their physicians through these networks. These findings may limit the utility of social media initiatives to improve health.
References
- 1.Lenhart A, Page D. Teens, Social Media, and Technology Overview 2015 Pew Research Center. 2015 [Google Scholar]
- 2.Perrin A. Social Media Usage: 2005–2015. Vol. 2015. Pew Research Center; 2015. pp. 1–12. [Google Scholar]
- 3.van Uden-Kraan CF, Drossaert CHC, Taal E, Seydel ER, van de Laar MAFJ. Participation in online patient support groups endorses patients’ empowerment. Patient Education and Counseling. 2009;74(1):61–69. doi: 10.1016/j.pec.2008.07.044. [DOI] [PubMed] [Google Scholar]
- 4.Merolli M, Gray K, Martin-Sanchez F, Lopez-Campos G. Patient-Reported Outcomes and Therapeutic Affordances of Social Media: Findings From a Global Online Survey of People With Chronic Pain. J Med Internet Res. 2015;17(1):e20–e29. doi: 10.2196/jmir.3915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jain SH, Powers BW, Hawkins JB, Brownstein JS. The digital phenotype. Nat Biotechnol. 2015;33(5):462–463. doi: 10.1038/nbt.3223. [DOI] [PubMed] [Google Scholar]
- 6.Schumacher KR, Stringer KA, Donohue JE, et al. Social Media Methods for Studying Rare Diseases. 2014 Apr; doi: 10.1542/peds.2013-2966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chunara R, Andrews JR, Brownstein JS. Social and news media enable estimation of epidemiological patterns early in the 2010 Haitian cholera outbreak. Am J Trop Med Hyg. 2012;86(1):39–45. doi: 10.4269/ajtmh.2012.11-0597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.McIver DJ, Hawkins JB, Chunara R, et al. Characterizing Sleep Issues Using Twitter. J Med Internet Res. 2015;17(6):e140–19. doi: 10.2196/jmir.4476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chunara R, Bouton L, Ayers JW, Brownstein JS. Assessing the Online Social Environment for Surveillance of Obesity Prevalence. In: Pappalardo F, editor. PLoS ONE. 4. Vol. 8. 2013. pp. e61373–e61378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Thackeray R, Neiger BL, Smith AK, Van Wagenen SB. Adoption and use of social media among public health departments. BMC Public Health. 2012;12(1):242. doi: 10.1186/1471-2458-12-242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Friedman AL, Brookmeyer KA, Kachur RE, et al. An assessment of the GYT: Get Yourself Tested campaign: an integrated approach to sexually transmitted disease prevention communication. Sex Transm Dis. 2014;41(3):151–157. doi: 10.1097/OLQ. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Madden M, Lenhart A, Cortesi S, et al. Teens, social media, and privacy. Pew Research Center; 2013. [Google Scholar]
- 13.van der Velden M, Emam El K. “Not all my friends need to know”: a qualitative study of teenage patients, privacy, and social media. J Am Med Inform Assoc. 2013;20(1):16–24. doi: 10.1136/amiajnl-2012-000949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Colbert J, Yuan N, Agarwal P, Lee JL, Chretien KC, Lehmann LS. The Promise of Social Media for Health: A Nationwide Survey of Primary Care Patients on Usage Patterns and Attitudes. Society of General Internal Medicine Annual Meeting; Apr 22–25, 2015; Toronto, Canada. Abstract 20. [Google Scholar]
- 15.Moreno MA, Jelenchick LA, Egan KG, et al. Feeling bad on Facebook: depression disclosures by college students on a social networking site. Depress Anxiety. 2011;28(6):447–455. doi: 10.1002/da.20805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Piko BF. Self-perceived health among adolescents: the role of gender and psychosocial factors. Eur J Pediatr. 2006;166(7):701–708. doi: 10.1007/s00431-006-0311-0. [DOI] [PubMed] [Google Scholar]
- 17.Kramer ADI, Guillory JE, Hancock JT. Experimental evidence of massive-scale emotional contagion through social networks. Proc Natl Acad Sci USA. 2014;111(24):8788–8790. doi: 10.1073/pnas.1320040111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med. 2007;357(4):370–379. doi: 10.1056/NEJMsa066082. [DOI] [PubMed] [Google Scholar]
- 19.Christakis NA, Fowler JH. The Collective Dynamics of Smoking in a Large Social Network. New England Journal of Medicine. 2008;358(21):2249–2258. doi: 10.1056/NEJMsa0706154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Marwick AE. I tweet honestly, I tweet passionately: Twitter users, context collapse, and the imagined audience. New Media Society. 2011 doi: 10.1177/1461444810365313. [DOI] [Google Scholar]
- 21.Boyd D. It’s Complicated. Yale University Press; 2014. [Google Scholar]
- 22.Lenhart A, Smith A, Anderson M. Teens Technology Romantic Relationships. Pew Research Center. 2015 Oct;:1–77. [Google Scholar]
- 23.Wartella E, Rideout V, Zupancic H, Beau L. Teens, health, and technology, a national survey. Center on Media and Human Development; School of Communication; Northwestern University; 2015. Teens, Health, and Technology a National Survey. http://cmhd.northwestern.edu/wp-content/uploads/2015/05/1886_1_SOC_ConfReport_TeensHealthTech_051115.pdf. [Google Scholar]
- 24.Moreno MA, Christakis DA, Egan KG, et al. A pilot evaluation of associations between displayed depression references on Facebook and self-reported depression using a clinical scale. J Behav Health Serv Res. 2012;39(3):295–304. doi: 10.1007/s11414-011-9258-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.