

Abstract
Background:
Burnout has its focus on exhaustion and it includes persistent response to long-lasting job-related stressful events. It has a special relevance in health care area in which staff is under constant psychological, emotional, and physical stress. The results of several studies on burnout prevalence among Iranian nurses indicate its high incidence. Therefore, more accurate researches are required for better preventive interventions, and to do so, a reliable validated scale is required. One of the suitable and new tools for the measurement of burnout is Copenhagen Burnout Inventory (CBI). This study aimed to translate and investigate psychometric properties of CBI in Iranian nurses.
Materials and Methods:
In this methodological study, after the translation process, face and content validities via qualitative and quantitative methods was done. Content validation ratio, scale-level content validated index, item-level content validity index were measured. Then, construct validity was determined through factor analysis. Furthermore, internal consistency reliability and stability were assessed. The questionnaire was sent to 450 nurses who were randomly selected via quota sampling.
Results:
Face and content validity were acceptable. After translation and cultural adaptation process, exploratory factor analysis suggested a new model based on four factors and fit indices validated this model via confirmatory factor analysis. Internal consistency and stability of CBI were affirmed for each subscale separately.
Conclusions:
The four-factor Persian version of the CBI proved to enjoy acceptable psychometric properties. It can be applied to evaluate burnout in Iranian nurses or other health care providers.
Keywords: Burnout, Copenhagen Burnout Inventory, factor analysis, nurses, psychometric properties
Introduction
For the first time, the concept of burnout was presented in the literature in the 1970s by Freudenberger[1] and Maslach.[2] Burnout is described as a negative result of human service work, which is explained by emotional exhaustion, lack of energy, and work turn over. It is a situation of physical, emotional, and mental exhaustion that results from long-term involvement in work situations.[3] Burnout has three aspects personal, work-related, and client-related.[4] Burnout is a prolonged response to chronic emotional and interpersonal stressors on the job and it includes persistent response to long-lasting job-related stressful events. Burnout is a special problem in health care system, because the staffs are dealing with psychoemotional stress and physical stress.[5]
Burnout is often studied in the nurse community for several reasons. One reason is the fact that the nursing profession is susceptibility and vulnerability to high incidence of burnout. The significant role burnout plays on mental and physical wellbeing of nurses makes carrying out more accurate studies on this concept quite necessary and obvious.[6]
Based on the observations by Shaufeli and Enzman (1998), burnout influences personal, interpersonal, and organizational levels, each of which contains five types of signs: Affective, cognitive, physical, behavioral, and motivational.[7] The personal consequences include work-related musculoskeletal illnesses,[8] depression,[9] sleep disorders,[10] and other negative personal effects on mental health such as reduced self-confidence and psychosomatic disorders.[11]
In the organizational level, burnout leads to increase in sickness absence from work and society and significant effects on the performance of nurses.[12] Some studies showed that patients were less satisfied with hospitals in which nurses had higher percentages of dissatisfaction or lower confidence in management.[13,14] According to Cimiotti et al.,[15] hospitals in which burnout has been diminished by 30% had fewer infections that can save about $68 million.
Many researchers and practitioners agree that lack of adequate health care sources is one of the main problems that Iranian nurses, such as their colleagues in many other societies, are involved in health-care systems.[16] These conditions have made Iranian nurses to face an increased possibility of physical and mental stress, which can lead to burnout.[17] Many studies regarding burnout in Iranian nurses indicate its high incidence.[18] Thus, more accurate research are needed for better preventive interventions and heath care.
To put it differently, it seems vital to apply changes into the profession in order to reduce burnout in nurses; furthermore, what is more important is measuring the effectiveness of these changes, and to do so, a reliable validated scale is required. One of the suitable and new tools for the measurement of burnout is Copenhagen Burnout Inventory (CBI).[4] CBI is a valid and reliable instrument and has been used in several studies. CBI has 19 items and uses a 5-item Likert-type scale (0 means never or very low degree and 5 always or very high degree) and includes three subscales of personal burnout (6 items), work related burnout (7 items), and client related burnout (6 items).[4,19] The CBI has been translated into many languages (English, Japanese, Swedish, Finnish, French, and Slovenian) and is being used in many countries. The reliability and validity of the CBI in different cultures were reported to be sound and acceptable.[4]
However, in spite of the importance of the concept in stressful professions such as nursing, no valid and reliable instrument for assessing burnout exists in Persian language. As a result, this study was designed with the aim of translating and studying the psychometric properties of the Persian Version of “Copenhagen Burnout Inventory.”
Materials and Methods
The present study is a methodological research[20] through which the CBI instrument is translated and the new Persian version is validated among Iranian nurses. This study was carried out in three main phases between March 1st 2013 and October 31st 2014. The first phase was translation and cultural adaptation of the English version of CBI. The second phase was the qualitative face and content validation, and in the third phase, quantitative procedures were run.
Phase I: Translation and cultural adaptation
After receiving permission from the original designer of the CBI, the instrument was translated and cultural adaptation. This translation was carried out as follows: Forward translation: The English version of the instrument was translated into Persian by two translators fluent in both English and Persian. Expert panel: A bilingual (English and Persian) expert panel was brought together. The expert panel compared the two translations and the final version was prepared after applying a few changes. Back-translation: The final translation of CBI was translated back into English by two other translators, both fluent in English and Persian. Pre-testing and cognitive interviewing: Five nurses were randomly selected from the target population in order to test the tentative final version. Final version: After incorporating some slight revisions, the final Persian version of the instrument was prepared. Documentation: All the cultural adaptation procedures are observable through the proper documents.
Afterward, the translated instrument was ready to undergo validation process.
Phase II: Qualitative face and content validation of persian version of CBI
Face validity
To confirm the face validity, the final instrument was administered to thirty nurses who worked in different wards of different hospitals to express their ideas about simplicity and comprehensibility of each word and sentence. After incorporating a few comments given by the participants, the items were reworded.
Content validity
In order to assess the content validity, ten experts (two experts in clinical psychology, two psychiatric nurses, two nursing management trainers, and four nursing assistant professors, expert in development of relevant instruments) were invited to review the translated instrument qualitatively. After two weeks, all the suggestions were collected. The comments were carefully assessed and some of the items were re-worded. The validated instrument was finalized and ready to undergo the next phase. Further, we calculated content validation ratio (CVI) scale-level content validity index (SCVI) and item-level content validity index (IVCVI) for this scale. CVR of this scale was >1.5. Its ICVI was >0.85 and SCVI was approximately 0.90.
Phase III: Quantitative assessment of persian version of CBI: Assessment of reliability and construct validity using factor analysis
Factor analysis
As Severinsson reported “while the translation of questionnaires for cross-cultural research is important, methodological problems for validity may arise,” Exploratory Factor Analysis (EFA) is necessary. In other words, after cultural adaptation Confirmatory Factor Analysis (CFA) changes into EFA to explore a favorite structural model.[21] Therefore, after translation and cultural adaptation process, we conducted EFA with four factors via principal components analysis followed by a varimax rotation to test the factor constructs of all the 19 items for the P-CBI subscales. Kaiser–Meyer–Olkin (KMO) test and Bartlett's test of sphericity were also assessed to confirm sample adequacy for extraction of the factors. Then for confirming new explored model, CFA was conducted.
CFA is a structural equation modeling (SEM) method which is used to compare the goodness of fit between a hypothesized model and the data acquired from study cases. There are some fit indicators for determining the goodness of fit of the model and it is suggested that several indicators be considered.[22,23] In the present study, several indices of fit, i.e., Chi-square, root mean error of approximation (RMSEA), goodness-of fit index (GFI), comparative fit index (CFI), and adjusted goodness-of-fit index (AGFI) were calculated. The common used fit index is Chi-square. Because this index is dependent on the sample size, the ratio of Chi-square to the degree of freedom was considered where values 2–3 indicate a good fit of the model. Another important index is the RMSEA where values less than 0.08 are considered acceptable and those less than 0.05 indicate a good fit of the model.[23] Suitable values are considered to be >0.9 for CFI and GFI and >0.85 for AGFI.[24]
Reliability
Cronbach's alpha is the best method for evaluating internal consistency. The Cronbach's alpha of about 0.7 is sufficient and of >0.80 indicates high internal consistency of the instruments. The stability was measured via intra-class correlation coefficients through test-retest on 30 nurses with a 2-week interval period.[25] The internal consistency was separately measured via Cronbach's alpha twice for each subscale, first before and then after factor analysis.
Data collection
Four hundred and fifty nurses were randomly selected by quota sampling. Participants were employees in general hospitals affiliated with three major universities of medical sciences in Tehran. Collecting data was performed from May until September 2014. The aim of study was explained to the participants. Then, both demographics (age, sex, educational level, marital status, and occupational characteristics) and the CBI questionnaires were given to the participating nurses to complete.
Data analysis
Reliability of P-CBI as well as descriptive statistics for the participants variables were measured by SPSS version 22. Factor analysis was conducted via LISREL8.5.
Ethical considerations
Ethical authorization and agreement were obtained from the Research and Ethics Committees of University of Medical Sciences. Written informed consents were also acquired from all the participants who took part in the study.
Results
Quantitative phase (Factor analysis and reliability)
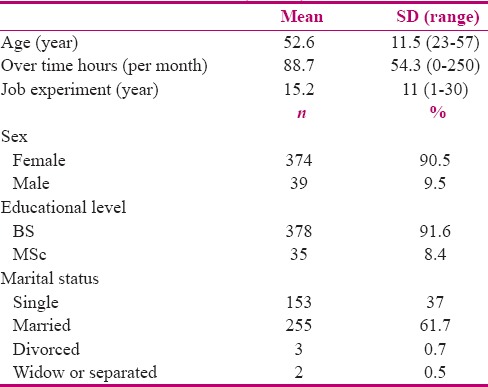
A total of 413 questionnaires were analyzed. Demographic characteristics of the participants are given in Table 1. Women accounted for 90.5% of the population, and the mean age (SD) was 52.6 (11.5) years. Most of the participants) 91.6%) had a BSc in nursing [Table 1].
Table 1.
Demographic and work characteristics of nurses (n=413)
Factor analysis
Exploratory factor analysis was done to achieve the better model. Thus, first, data was tested by the Bartlett's test of sphericity to achieve sample adequacy [Bartlett's test of sphericity;P < 0.05, χ2 = 3248.04 and KMO = 0.92].
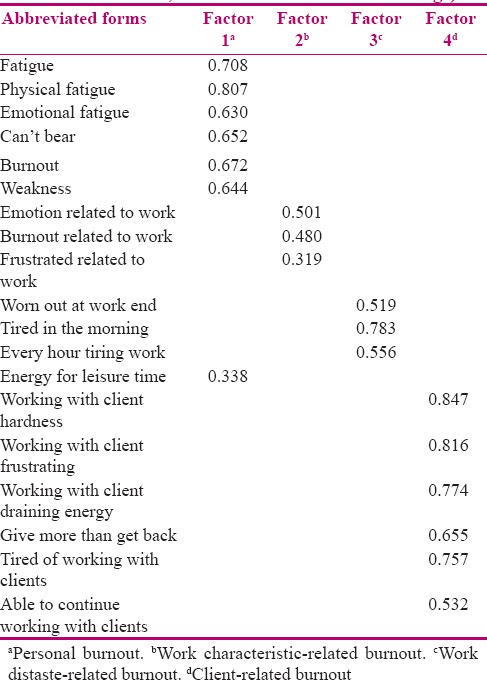
Then, several explorative factor analyses were performed among the variables to recognize the best model to fit, and as a final point a four-factor model was selected by item-to-factor loading of >0.3.
When testing the factor pattern of all the 19 CBI items, all the 6 items for the personal burnout subscale were loaded on the first factor, in addition to the item no. 13 (the last item in work burnout). 3 items of 7, 8, and 9 from the “work-related burnout” subscale loaded on the second factor; 3 items 10, 11, and 12 also from this subscale loaded on the third subscale, and finally all the 6 items for the “client-related burnout” subscale loaded on the forth factor [Table 2]. Based on the meaning of the loaded items on the second and the third factors, these factors were named work-characteristics-related burnout and work-distaste-related burnout, respectively.
Table 2.
Results of the confirmatory factor analysis of four-factor model of Copenhagen Burnout Inventory (Persian version)
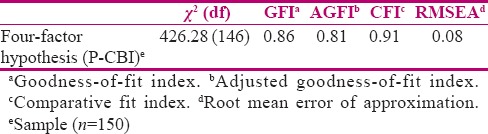
This hypothesized four-factor model (Persian version of CBI: P-CBI) was tested by CFA on another group of participants (150 nurses). Therefore, the four-factor model of P-CBI with 19 items (personal burnout: 7 items, work-characteristic-related burnout: 3 items, work-distaste-related burnout: 3 items, and client-related burnout: 6 items) is a model with the best fit indices. CFI and GFI indices are acceptable and other indices such as the ratio of Chi-square to the degree of freedom, RMSEA, AGFI, and SRMR indicate a good fit of the model [Table 3].[26]
Table 3.
Maximum correlation of each item with extracted factors (extraction method: principal component analysis, rotation method; varimax-rotated factor loadings)
Reliability
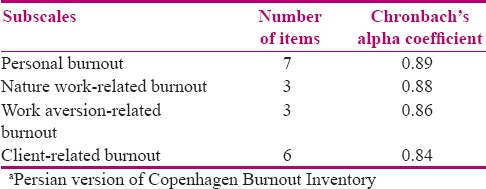
Coefficient of Cronbach's alpha for its subscales before factor analysis was 0.87–0.89 and after that 0.84–0.89 [Table 4]. The intra-class coefficient correlation for test-retest reliability for subscales of personal burnout, work-characteristics-related burnout, work-distaste, and client-related burnout were 0.95, 0.84, 0.83, and 0.90 (P < 0.001), respectively.
Table 4.
Cronbach's alpha coeffcients of total and subscales of four factors P-CBIa
Discussion
Because of the importance of the concept of burnout in nursing professionals and its role on their mental and physical health, the necessity of studying this aspect is undisputable. Professional nurses are continually challenged to stay up-to-date to supply the highest quality of patient care. However, the quality of health care depends on many factors such as their health and work ability.[27] Shimizutani et al.[28] found that an increase in the workload is related with higher scores for the client-related burnout due to the stressors arising from conflict with patients. It is also found that burnout has negative influence on the individual as well as on the organization in general.[29] For example, relationships have been shown between burnout and depression, a sense of disappointment, exhaustion, and lack of motivation,[10,29] medication use, and thoughts of suicide, job dissatisfaction, and desire to leave the job, as well as an increase in the number of sick days, absence from work, and leaving nursing profession.[10] In conclusion, nursing burnout results in unsatisfactory patient care, job dissatisfaction, lack of marital and familial agreement, reduction of self-esteem, difficulty in concentration, social isolation, fatigue, loss of libido, headache, flu, gastrointestinal problems, sleep disorders, and alcohol and drug abuse.[10,30]
Regardless of the importance of burnout in health care system, it has not been considered properly among Iranian health care workers partly due to the lack of appropriate instruments. The current study was designed in order to translate and validate the Persian version of the CBI among the population of nurses. The CBI instrument was translated as well as adapted culturally into Persian and its psychometric properties were assessed. When an instrument is translated and used in a new culture, assessing its psychometric properties is necessary because the original psychometric properties may not be applicable in the new culture.[25] In the present study, content and face validity, construct validity, as well as the reliability of this instrument were evaluated.
Based on the results, the Persian version of CBI has acceptable reliability and validity and the constructs of its two subscales (personal burnout and client-related burnout) are fairly similar to the original version[4] but work-related burnout is divided into two separate subscales. The qualitative findings of the present study during the translation process, content, and face validity were reported good and acceptable. The results obtained from factor analysis revealed that the four-factor Persian version of CBI is valid and reliable.
CFA and EFA of CBI were concluded using a sample of 413 nurses (263 samples for primary steps of EFA and 150 for the final step of CFA).
In a study designed to validate the two subscales of the Chinese version of CBI (C-CBI) for the employees in two companies in Taiwan, it was shown that item 13 had no significant correlation with the other items and work-related burnout subscale. Therefore, once more, item 13 was omitted from the Chinese version, however, this model was not confirmed, either. Both the C-CBI personal burnout and work-related burnout subscales had high internal consistency and correlated acceptably with the other measures of health, job characteristics, and perception of work; in addition, EFA extracted two factors (for 13 items).[31]
Another study was conducted among secondary school teachers in New Zealand to validate the English version of CBI. The CFA model for the three burnout subscales was acceptable as well as the internal consistency, homogeneity reliability, and criterion-related validity.[32] In another study, carried out by Molinero Ruiz et al.[33] on the psychometrics of the CBI among 479 workers in four organizations with different work groups, the items of the three subscales showed good consistency and homogeneity. Moreover, convergent validity of the Spanish version of CBI was confirmed in the 19-item scale of CBI. Nevertheless, in our view, low correlation of item 13 appears to be related to cultural characteristics because leisure time is a personal concern that EFA model (the four-factor model) may confirm. According to the EFA model in our samples, item 13 was omitted from work-related burnout subscale and then added to the personal burnout subscale.
In the present study, a new step was taken in factor analysis of this instrument, i.e., evaluation of EFA and CFA for the four-factor version of CBI, which had not been conducted so far. In addition, the findings of the current study indicated that the Persian version of CBI has a good internal consistency. The Cronbach's alpha of each subscale is evenly matched to the obtained values in the other studies especially that of the original scale.[4] The results of the test-retest revealed that the Persian version of the instrument has a good stability, which confirms the findings reported by Fong et al.[34] about the Chinese version of CBI.
Study limitations
This study has some limitations. First, the small sample size may reduce the statistical power of the study. In addition, because the participants of the study were nurses and limited number of these professional was available, we could not conduct a study with a parallel population to compare our findings.
Conclusion
It is suggested that the Persian version of CBI, in addition to the acceptable validity and reliability, has confirmed construct validity in the four-factor model. This instrument can be used by nurses and health care managers to promote their knowledge and patient care. It is notable that each subscale of P-CBI can be used as an instrument separately. Besides, P-CBI can be completed in a short time because of its simplicity and the small number of items. This study can be a basis for the future studies in the field of burnout in other groups of health care providers, teachers, and social service workers in Iran.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
This study is part of a nursing Master's program, approved by Shahid Beheshti University of Medical Sciences, Tehran, Iran. The present research was funded by the Shahid Beheshti University of Medical Sciences, Tehran, Iran. This article has been derived from a research project (grant no.: 1392-1-86-12770). The authors wish to thank all the participants, and Dr. Kristensen for allowing us to use the instrument.
References
- 1.Freudenberger HJ. Staff burnout. JSI. 1974;30:159–65. [Google Scholar]
- 2.Maslach C. Burned-out. Human Behav. 1976;5:16–22. [Google Scholar]
- 3.Schaufeli WB, Greenglass ER. Introduction to special issue on burnout and health. Psychol Health. 2001;16:501–10. doi: 10.1080/08870440108405523. [DOI] [PubMed] [Google Scholar]
- 4.Kristensen TS, Borritz M, Villadsen E, Christensen KB. The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work Stress. 2005;19:192–207. [Google Scholar]
- 5.Beckstead JW. Confirmatory factor analysis of the Maslach Burnout Inventory among Florida nurses. Int J Nurs Stud. 2002;39:785–92. doi: 10.1016/s0020-7489(02)00012-3. [DOI] [PubMed] [Google Scholar]
- 6.Institute of Medicine Committee on Quality of Health Care in America. Crossing the quality CHSM: A new health system for the 21st century. Paper presented at the National Academy Press; Washington, DC. 2001. [Google Scholar]
- 7.Mbuthia NN. University of South Africa, Unpublished thesis. 2009. An investigation into the factors that nurses working in critical care units perceive. [Google Scholar]
- 8.Jaworek M, Marek T, Karwowski W, Andrzejczak C, Genaidy AM. Burnout syndrome as a mediator for the effect of work-related factors on musculoskeletal complaints among hospital nurses. Int J Ind Ergon. 2010;40:368–75. [Google Scholar]
- 9.Ahola K, Hakanen J. Job strain, burnout, and depressive symptoms: A prospective study among dentists. J Affect Disord. 2007;104:103–10. doi: 10.1016/j.jad.2007.03.004. [DOI] [PubMed] [Google Scholar]
- 10.Vela-Bueno A, Moreno-Jiménez B, Rodríguez-Muñoz A, Olavarrieta-Bernardino S, Fernández-Mendoza J, De la Cruz-Troca JJ, et al. Insomnia and sleep quality among primary care physicians with low and high burnout levels. J Psychosom Res. 2008;64:435–42. doi: 10.1016/j.jpsychores.2007.10.014. [DOI] [PubMed] [Google Scholar]
- 11.Piko BF. Burnout, role conflict, job satisfaction and psychosocial health among Hungarian health care staff: A questionnaire survey. Int J Nurs Stud. 2006;43:311–8. doi: 10.1016/j.ijnurstu.2005.05.003. [DOI] [PubMed] [Google Scholar]
- 12.Risambessy A, Swasto B, Thoyib A, Astuti ES. The influence of transformational leadership style, motivation, burnout towards job satisfaction and employee performance. J Basic Appl Sci Res. 2012;2:8833–42. [Google Scholar]
- 13.Aiken LH, Sermeus W, Van den Heede K, Sloane DM, Busse R, McKee M, et al. Patient safety, satisfaction, and quality of hospital care: Cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ. 2012;344:e1717. doi: 10.1136/bmj.e1717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McHugh MD, Kutney-Lee A, Cimiotti JP, Sloane DM, Aiken LH. Nurses' widespread job dissatisfaction, burnout, and frustration with health benefits signal problems for patient care. Health Aff (Millwood) 2011;30:202–10. doi: 10.1377/hlthaff.2010.0100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cimiotti JP, Aiken LH, Sloane DM, Wu ES. Nurse staffing, burnout, and health care-associated infection. Am J Infect Control. 2012;40:486–90. doi: 10.1016/j.ajic.2012.02.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Anoosheh M, Ahmadi F, Faghihzadeh S, Vaismoradi M. Causes and management of nursing practice errors: A questionnaire survey of hospital nurses in Iran. Int Nurs Rev. 2008;55:288–95. doi: 10.1111/j.1466-7657.2008.00623.x. [DOI] [PubMed] [Google Scholar]
- 17.Dehghan Nayeri N, Nazari AA, Salsali M, Ahmadi F, Adib Hajbaghery M. Iranian staff nurses' views of their productivity and management factors improving and impeding it: A qualitative study. Nurs Health Sci. 2006;8:51–6. doi: 10.1111/j.1442-2018.2006.00254.x. [DOI] [PubMed] [Google Scholar]
- 18.Khodabakhsh M, Mansuri P. Analysis and comparison between frequency and depth of job-burnout aspects among male and female nurses. ZJRMS. 2011;13:40–2. [Google Scholar]
- 19.Winwood PC, Winefield AH. Comparing two measures of burnout among dentists in Australia. Int J Stress Manag. 2004;11:282–9. [Google Scholar]
- 20.LoBiondo-Wood G, Haber J. Nursing Research: Methods and Critical Appraisal for Evidence-Based Practice. Louise, MO: Mosby, Elsevier; 2010. [Google Scholar]
- 21.Severinsson E. Evaluation of the Manchester clinical supervision scale: Norwegian and Swedish versions. J Nurs Manag. 2012;20:81–9. doi: 10.1111/j.1365-2834.2011.01297.x. [DOI] [PubMed] [Google Scholar]
- 22.Brown TA. Confirmatory Factor Analysis for Applied Research. New York: The Guilford Press; 2006. [Google Scholar]
- 23.Seo DC, Torabi MR, Blair EH, Ellis NT. A cross-validation of safety climate scale using confirmatory factor analytic approach. J Safety Res. 2004;35:427–45. doi: 10.1016/j.jsr.2004.04.006. [DOI] [PubMed] [Google Scholar]
- 24.Helsen K, Van den Bussche E, Vlaeyen JW, Goubert L. Confirmatory factor analysis of the Dutch Intolerance of Uncertainty Scale: Comparison of the full and short version. J Behav Ther Exp Psychiatry. 2013;44:21–9. doi: 10.1016/j.jbtep.2012.07.004. [DOI] [PubMed] [Google Scholar]
- 25.Polit D, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Philadelphia, PA: Lippincott Williams & Wilkins; 2012. [Google Scholar]
- 26.Munro BH. Statistical Methods for Health Care Research. Philadelphia, PA: Lippincott Williams & Wilkins; 2005. [Google Scholar]
- 27.Knezevic B, Milosevic M, Golubic R, Belosevic L, Russo A, Mustajbegovic J. Work-related stress and work ability among Croatian university hospital midwives. Midwifery. 2011;27:146–53. doi: 10.1016/j.midw.2009.04.002. [DOI] [PubMed] [Google Scholar]
- 28.Shimizutani M, Odagiri Y, Ohya Y, Shimomitsu T, Kristensen TS, Maruta T, et al. Relationship of nurse burnout with personality characteristics and coping behaviors. Ind Health. 2008;46:326–35. doi: 10.2486/indhealth.46.326. [DOI] [PubMed] [Google Scholar]
- 29.Euwema MC, Kop N, Bakker AB. The behaviour of police officers in conflict situations: How burnout and reduced dominance contribute to better outcomes. Work Stress. 2004;18:23–38. [Google Scholar]
- 30.Demir A, Ulusoy M, Ulusoy M. Investigation of factors influencing burnout levels in the professional and private lives of nurses. Int J Nurs Stud. 2003;40:807–27. doi: 10.1016/s0020-7489(03)00077-4. [DOI] [PubMed] [Google Scholar]
- 31.Yeh WY, Cheng Y, Chen CJ, Hu PY, Kristensen TS. Psychometric properties of the Chinese version of Copenhagen Burnout Inventory among employees in two companies in Taiwan. Int J Behav Med. 2007;14:126–33. doi: 10.1007/BF03000183. [DOI] [PubMed] [Google Scholar]
- 32.Milfont TL, Denny S, Ameratunga S, Robinson E, Merry S. Burnout and wellbeing: Testing the Copenhagen Burnout Inventory in New Zealand teachers. Soc Indic Res. 2007;89:169–77. [Google Scholar]
- 33.Molinero Ruiz E, Basart Gómez-Quintero H, Moncada Lluis S. Validation of the Copenhagen Burnout Inventory to assess professional burnout in Spain. Rev Esp Salud Publica. 2013;87:165–79. doi: 10.4321/S1135-57272013000200006. [DOI] [PubMed] [Google Scholar]
- 34.Fong TC, Ho RT, Ng SM. Psychometric properties of the Copenhagen Burnout Inventory-Chinese version. J Psychol. 2014;148:255–66. doi: 10.1080/00223980.2013.781498. [DOI] [PubMed] [Google Scholar]