

Abstract
Kidney stone imaging is an important diagnostic tool and initial step in deciding which therapeutic options to use for the management of kidney stones. Guidelines provided by the American College of Radiology, American Urological Association, and European Association of Urology differ regarding the optimal initial imaging modality to use to evaluate patients with suspected obstructive nephrolithiasis. Noncontrast CT of the abdomen and pelvis consistently provides the most accurate diagnosis but also exposes patients to ionizing radiation. Traditionally, ultrasonography has a lower sensitivity and specificity than CT, but does not require use of radiation. However, when these imaging modalities were compared in a randomized controlled trial they were found to have equivalent diagnostic accuracy within the emergency department. Both modalities have advantages and disadvantages. Kidney, ureter, bladder (KUB) plain film radiography is most helpful in evaluating for interval stone growth in patients with known stone disease, and is less useful in the setting of acute stones. MRI provides the possibility of 3D imaging without exposure to radiation, but it is costly and currently stones are difficult to visualize. Further developments are expected to enhance each imaging modality for the evaluation and treatment of kidney stones in the near future. A proposed algorithm for imaging patients with acute stones in light of the current guidelines and a randomized controlled trial could aid clinicians.
Clinicians in a range of medical specialties will encounter patients with kidney stones. As many as one in 11 Americans develop nephrolithiasis, and over the past 15 years the prevalence has increased by almost 70%1,2. The number of imaging studies ordered to evaluate for kidney stones is also increasing: from 1992 to 2009 the use of CT for imaging patients with kidney stones tripled3. Imaging of patients presenting with suspected kidney stones facilitates diagnosis and provides the first step in management by establishing the size and location of stones4.
Choosing the correct imaging modality for kidney stones involves many factors including the clinical setting, patient body habitus, cost, and tolerance of ionizing radiation. Multiple imaging modalities are available, but widespread clinical use is currently limited to CT, ultrasonography, and kidney ureter bladder (KUB) plain film radiography. In this Review, we will outline the basics of each imaging modality, its sensitivity and specificity, advantages, disadvantages and costs. We also consider clinical guideline recommendations from the three main bodies providing guidance regarding stone imaging: the American Urological Association (AUA), European Association of Urology (EAU), and the American College of Radiology (ACR), and areas of best use. We also discuss areas of emerging investigation, as imaging is a key research priority in urinary stone disease5. Additionally, we consider a large randomized controlled trial conducted in 2014 comparing CT and ultrasonography within the emergency department setting for the evaluation of acute renal colic6.
Information gained from imaging
Patients presenting to the emergency department with flank pain and haematuria are likely to undergo abdominal imaging as part of a workup for kidney stones, but diagnosis and location of the stone can often be anticipated without imaging based on the patient’s history and physical examination. Stone formation can be quite complex and differ between various stone compositions7; however, stones are largely asymptomatic when they are growing in the renal calyces. Passage into the ureter obstructs the flow of urine, leading to upstream dilatation of the ureter and renal pelvis. This obstruction generally results in colic-type pain as ureteral peristalsis increases8. Nausea and vomiting are often associated with these severe bouts of pain. Classically, a stone obstructs proximally near the ureteropelvic junction where the renal pelvis narrows to the calibre of the ureter. Obstruction at this point causes pain radiating to the flank. The stone encounters two additional points of narrowing as it moves distally, firstly where the ureter crosses the iliac vessels, and secondly at the bladder, referred to as the ureterovesical junction. Obstruction of the iliac vessels causes pain radiating down into the groin or lower abdomen. Stones lodged at the ureterovesical junction tend to cause pain that radiates into the scrotum or labia, inner thigh, or urethra and often create urinary frequency, urgency, and dysuria, as the stone irritates the bladder. Upon presentation to the emergency department the majority of patients have stones located at the ureteropelvic junction or ureterovesical junction9. Passing stones might also cause abrasions to the mucosal lining of the ureter, resulting in visible or microscopic haematuria.
The emergency department is a common setting for the initial presentation of patients with obstructing stones. Such a diagnosis might be suspected without imaging; however practitioners must entertain a wide differential diagnosis for patients with severe abdominal and/or flank pain3. Imaging modalities with high sensitivity provide the clinician with confidence that symptoms are caused by an alternative pathology when no stones are visualized. Alternatively, imaging modalities with high specificity demonstrate that a patient’s symptoms are related to stones when they are visualized. Measurements of sensitivity and specificity can vary widely throughout the literature based on several factors, including the method used as the reference standard to determine true-positive and true-negative values, and the population of patients being examined.
In addition to diagnosis, initial imaging is the first step in disease management. Determination of stone size and location from imaging enables risk stratification regarding spontaneous stone passage without surgical intervention10. However, the likelihood of stone passage is multifactorial and the probability of spontaneous passage decreases with increased stone size and improves with a more distal location in the ureter11. As a stone moves through the ureter the patient’s pain may vary, or even resolve completely despite continued obstruction from the stone. This phenomenon makes symptom resolution a poor marker of stone passage, and persistence of the asymptomatic obstruction can lead to permanent loss of renal function, or even kidney failure. Thus, when a stone is suspected of having passed, but the patient has not witnessed the actual stone, imaging is necessary to definitively confirm the passage of the stone4. Serial imaging can be used to follow the progress of a passing stone, and might also be used by the urologist and/or nephrologist as they monitor nonobstructing stones for growth.
Broadly, the available imaging modalities include CT, ultrasonography, KUB radiography, and MRI. The sensitivity, specificity, dose of ionizing radiation, and relative costs vary between modalities (TABLE 1). An algorithm is also proposed for imaging patients with suspected stones in the emergency department setting (FIG. 1).
Table 1.
Comparison of different imaging modalities for kidney stones
| Imaging modality | Sensitivity* (%) | Specificity* (%) | Radiation exposure (mSv)25 | Cost multiple relative to that of KUB25 |
|---|---|---|---|---|
| CT | 95 (REF 12) | 98 (REF 12) | 10.0 | 10 |
| Low-dose CT | 95 (REF 12) | 97 (REF 12) | ~3.0 | 10 |
| Ultrasonography | 84 (REF 25) | 53 (REF 25) | None | 5 |
| KUB | 57 (REF 25) | 76 (REF 25) | 0.7 | 1 |
| MRI | 82 (REF 25) | 98 (REF 25) | None | 30 |
KUB, kidney, ureters, and bladder plain film.
Published sensitivity and specificity vary widely in the literature for some modalities; therefore, these values are derived from values published by the American College of Radiography and American Urological Association, which have obtained them from pooled data analysis
Figure 1. A proposed algorithm for imaging patients with acute stone disease in the emergency department.
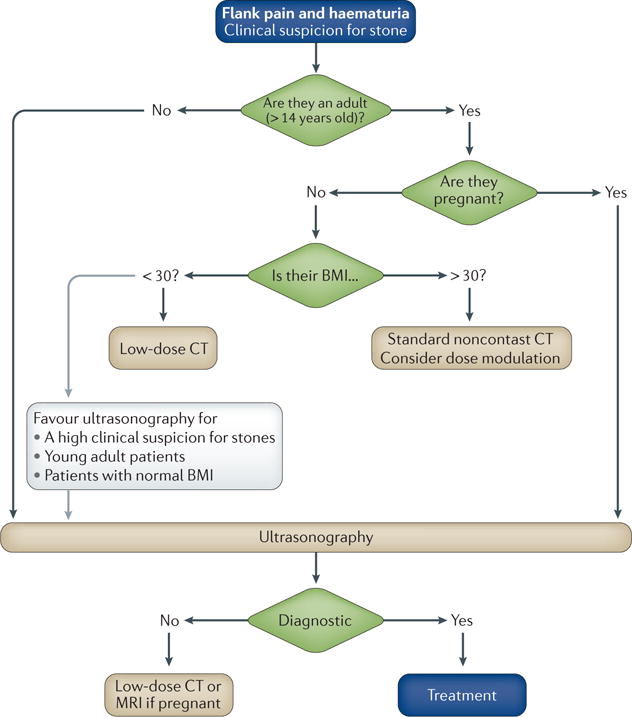
Initial stratification is based on age; American Urological Association (AUA) guidelines delineate patients <14 years old as paediatric patients. Adult patients are stratified based on whether they are pregnant and BMI. Ultrasonography should also be considered first in adult patients, especially those with a normal BMI and adults in whom a reasonable suspicion of stone disease exists. In such cases the sensitivity and specificity will be sufficiently high to augment the patient’s pretest probability of having a kidney stone without considerably increasing the risk of missing a alternative diagnosis. low-dose CT, noncontrast CT with <3 mSv of radiation exposure.
Noncontrast CT
CT broadly refers to many types of imaging scans with differing amounts of contrast or even none at all, and variable image timing depending on the clinical question to be answered. In patients with nephrolithiasis, noncontrast CT or CT-KUB radiography are most often used. CT exploits the different degrees to which body tissues absorb radiation. Multiple data points are obtained by rotating a radiation source and contralateral detector around the patient, these data are processed by a computer into 3D images. As kidney stones have a markedly different composition compared with renal parenchyma and urine, they absorb considerably more radiation and are easily identifiable without the need for contrast (FIG. 2). CT generates a 3D image of the stone and the surrounding anatomy, which can be reconstructed into multiple viewing planes. The sensitivity of CT for detecting kidney stones is the highest of all the available modalities and reasonable estimates suggest it is ~95%12. Few large stones are missed using CT but small stones (<3 mm) might slip between the imaged tissue planes and not be detected13. The ACR estimates the specificity of CT to be 98% when a patient presents with acute flank pain suspicious of an obstructing stone. Almost all stones can be visualized using CT with the exception of some stones that are caused by the precipitation of protease-inhibitor medications in the urine14.
Figure 2. A coronal demonstration of bilateral 8 mm nephrolithiasis on noncontrast CT.
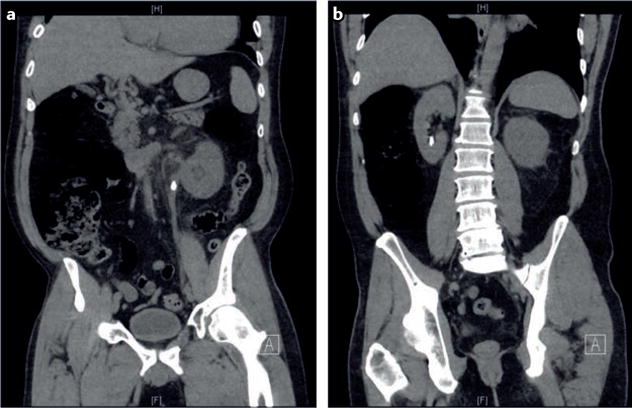
These stones are clearly visible using this imaging modality. Additional anatomical detail can be obtained by reconstructing the images in an axial plane. a | This coronal CT image clearly demonstrates a left-sided obstructing stone. b | Posterior coronal CT view of panel a demonstrating a lower-pole nonobstructing stone. An excellent level of anatomical detail can be seen here and can be further increased by reconstructing the image in an axial plane.
The detailed anatomical images that are obtained, which enable evaluation of other potential causes of the patient’s presenting symptoms, is an additional advantage of CT (FIG. 2). In the emergent setting, the differential diagnosis for flank pain with haematuria includes trauma; renal, ureteral and bladder masses; renal papillary necrosis; pyelonephritis; nephropathy; congenital ureteral obstruction; urinary tract infection; bladder stones; large retroperitoneal masses; aortic dissections; arterial-venous malformation; thrombosis; diverticulitis with fistula; endometriosis; and large ovarian and uterine masses in which haematuria can mistakenly be thought to come from a vaginal source. The differential diagnosis for patients with abdominal pain without haematuria is even more extensive.
CT imaging can also provide information regarding the composition of stones. Attenuation describes the density of objects encountered by photons passing from the radiation source to the detector. The Hounsfield unit (HU) is a measurement of attenuation. In this scale, water is given the value of 0 HU, air is −1,000 HU, and dense bone is 1,000 HU. The Hounsfield units of a stone can indicate its type, as different stone compositions absorb differing amounts of radiation. Uric acid stones are typically 200–400 HU, whereas calcium oxalate stones are ~600–1,200 HU15. CT attenuation can also be used to predict responsiveness to shockwave lithotripsy, as increased attenuation correlates with an increase in the number of shocks required and with reduced success rates16,17. Attenuation is complicated by the need for proper technique; for example, averaging attenuation over a voxel that is larger than a stone can reduce the Hounsfield units measured for a stone. This reduction might result in misinterpretion of a dense, hard stone that would be inappropriate for shockwave lithotripsy as being less dense18,19. This issue can be mitigated by using dual-energy CT scanners, which enable imaging of patients’ tissues at two different voltages, facilitating comparison of results from two separate detectors. These scanners also enable tissue evaluation at varied energy levels, and further improve the accuracy of determinations of stone composition19–22.
Finally, the accuracy of CT is an important characteristic when imaging patients that are obese23. The accuracy of CT is generally better than that of ultrasonography, as imaging obese patients using ultrasonography is difficult; however no definitive study has been conducted that compares the two modalities for imaging kidney stones in obese patients. The difficulty in imaging obese patients has been definitively demonstrated by imaging of patients with cholelithiasis, for which CT was shown to be more sensitive and specific than ultrasonography24. Standard CT is the imaging modality of choice for patients with a BMI >30 according to the ACR, AUA and EAU12,25,26. Going forward, the obesity of patients will be an important consideration given the imaging needs of the obese population and the increasing prevalence of stones, which is rising in parallel with obesity rates24.
Limitations of CT include cost and radiation exposure. Multiple variables such as charges, costs and reimbursement, as well as the many stakeholders including hospital systems, insurance companies and the patient often complicate discussions concerning costs. However, the cost of performing a CT scan is approximately double that of performing a renal ultrasonography scan based on a review of Medicare data6, and around one-third of the cost of an MRI25. Low-dose CT is similar in cost to traditional CT25. In the STONE trial by Melnikow and colleagues27, ultrasonography was estimated to be approximately half the cost of CT; however, the overall cost of the visit to the Emergency Department was similar regardless of the type of imaging modality used. Despite this observation, cost remains an important factor differentiating CT from ultrasonography, but radiation exposure is an equally important consideration.
A standard CT scan exposes patients to an effective dose of ionizing radiation of ~10 mSv25. Such a radiation dose might not be trivial; malignancies have been documented after a dose of 100 mSv, and the dose is additive over a person’s lifetime28. This fact is particularly important in patients with kidney stones, who tend to be young (stone formers tend to have their first stone between the ages of 20 years and 40 years; however, stones can manifest at any age), and often have multiple recurrent stone events over their lifetime27. Patients can also present many times to the emergency department with the same stone when stones remain symptomatic5. Clinicians have called for reductions in the amount of radiation used in medical imaging and CT is an important source of radiation exposure29. In addition to radiation exposure, these CT scans often have incidental findings, which might or might not be clinically important but often lead to further analysis or invasive testing.
Low-dose CT is a method of reducing radiation exposure by lowering the tube current to the radiation source. A traditional noncontrast CT might use a tube current of 100 mAs, whereas in low-dose CT the tube current decreases to ~30 mAs or lower30. Alternatively, low-dose protocols might use an automated current modulator, which adjusts the tube current based on tissue attenuation. Low-dose CT has been defined as <3 mSv of ionizing radiation. In comparison with standard CT, the sensitivity of low-dose CT is excellent, at 99% with a specificity of 94%, based on conclusions of a metaanalysis involving 1,061 patients31. A low-dose CT provides similar information to that provided by standard CT and the protocol can be used in a similar setting. Data regarding stone size and location are still accurate, and Hounsfield units can still predict stone composition with the same relative units for calcium stones32.
However, image quality and accuracy tends to decrease with reduced tube current30. Decreased image resolution can limit the ability to evaluate patients with non-stone-related pathologies and those with stones <3 mm33. Notably, the difference between standard and low-dose CT is not binary: as the power of the radiation source decreases so does the radiation exposure. The ability to produce ultralow-dose CT, which results in <1 mSv exposure, is possible and can be used for patients with known stone disease to evaluate changes in stone volume. Conversely, the radiation level used in the protocol of a low-dose or ultralow-dose CT can be increased to account for patient adiposity34. Currently, the AUA, EAU, and ACR do not recommend low-dose CT scans for patients with a BMI >30 as they are believed to be ineffective12,25,26. Discussion of a clinical suspicion of stones and concerns regarding radiation exposure with the performing radiologist might be helpful. Often CT settings and the area of imaging can be optimized for the patient’s body habitus and the specific clinical question. Dose modulation will probably continue to be refined in the future.
Overall, CT is a highly sensitive and specific technique for imaging stones in patients presenting with renal colic, which is useful in the emergent setting for diagnosis and in the surgical setting owing to the superior anatomical detail obtained, therefore, assisting surgical decision making. The greatest limitations are cost and radiation exposure, which can be somewhat overcome by using low-dose protocols. The ACR and AUA both recommend CT as the first-line investigation for adult patients presenting with symptoms suggestive of obstructive nephrolithiasis. The EAU recommends that CT be used to confirm a stone diagnosis for cases in which ultrasonography is equivocal26. When considering low-dose protocols, one should be mindful of a patient’s age, BMI, and degree of clinical suspicion of stones in order to choose the optimal imaging option25,26.
Ultrasonography
Ultrasonography is a low-cost imaging modality that does not rely on ionizing radiation and is becoming the primary alternative to CT outside the USA; however clinicians in the USA are now also moving towards this technique. Images obtained using ultrasonograhpy are produced when a transducer delivers short bursts of acoustic energy to the patient. This energy propagates through tissue as waves, partially reflecting back to the source when passing between tissues of different densities and/or acoustic impedances. A receiver detects the reflected waves, enabling images to be generated based on wave travel times and amplitude. The standard grayscale image is referred to as B-mode or brightness mode ultrasonography and in B-mode stones appear bright sometimes with a dark distal shadow. In B-mode, harmonic mode can also be used in which the transmitted signal is lower frequency than the received signal in an effort to improve resolution and decrease clutter. Colour is sometimes displayed on top of the image generated in B-mode (harmonic or not), which reflects the strength or frequency of Doppler signal in Doppler ultrasonography. The Doppler ultrasound signal is particularly sensitive to motion such as fluid flow in a ureteral jet, but the presence of stones can create an artefact in Doppler ultrasonographic imaging that results in colour in the image at the location of the stone.
Like CT, B-mode ultrasonography makes use of physical differences between stones and surrounding tissues to detect the stones. Relative to soft tissues, stones strongly reflect ultrasonic waves and appear as bright echogenic structures in the ultrasonographic image. Ultrasonic waves are unable to penetrate through stones, leaving a nonechogenic shadow beyond the stone in the image. Ultrasonography can also be used to detect surrogate markers of obstructing stones such as hydronephrosis35, and a lack of a ureteral jet using Doppler ultrasonography36.
A wide range of sensitivities and specificities for ultrasonography have been reported, probably owing to variations in technique, body habitus, patient population and reference standards. Imaging stones in the renal pelvis and in the ureter also present different challenges as it is difficult to image the length of an undilated ureter owing to interference by bowel gas and increased penetration depth. A pooled review of the literature demonstrates a sensitivity and specificity of 45% and 94%, respectively, for detection of ureteral calculi and 45% and 88%, respectively, for renal calculi37. Sensitivity is reduced for stones <3 mm, which might not produce a shadow, and stones can be missed in a decompressed system owing to the difficulty in distinguishing echogenic stones from echogenic central sinus fat in the kidney37. Sensitivity can be improved by combining ultrasonography with KUB radiography. Again, wide variations exist but estimates of sensitivity and specificity for these combined studies range from 58% to 100% and 37% to 100%, respectively25. Clinical frustration exists with regards to the variability in the accuracy of ultrasonography reported in the literature and differing guideline statements. The ACR and AUA recommend CT evaluation as a first-line investigation of patients with suspected kidney stones, whereas the EAU recommends ultrasonography12,25,26.
In this setting, Smith-Bindman et al.28 have published the STONE trial. This study randomized patients with suspected obstructive nephrolithiasis to evaluation with CT, ultrasonography performed at the bedside or ultrasonography performed in the radiology department. Overall, 2,759 patients were randomized to one of the three arms and then assessed over 180 days to evaluate the accuracy of stone diagnosis, based on patient reports of stone passage or surgical intervention. One primary outcome was to evaluate the risk of a failure to diagnose high-risk conditions such as an abdominal aortic aneurysm with rupture, pneumonia, sepsis, appendicitis with rupture, diverticulitis with abscess, bowel ischemia or perforation, renal infarction, renal stone with abscess, pyelonephritis with urosepsis, ovarian torsion or aortic dissection. Notably, obese patients were excluded from this study, and providers were allowed to order additional testing as indicated (including a CT scan if desired) after the initial imaging study.
Overall, no significant differences were reported in sensitivity (~85%), specificity (~50%), or complications between the three arms at the time of discharge from the emergency department6. However, several important considerations exist when evaluating the data. A follow-up CT scan was performed in 41% of patients in the group that received ultrasonography at the bedside and in 27% of patients imaged with ultrasonography in the radiology department. Thus, many of the patients included in the ultrasonography groups received diagnostic benefit from the additional CT scan. Additionally, the sensitivity and specificity for the CT group in this study were 86% and 53%, respectively. These values are dramatically lower than the expected sensitivity and specificity of >95%, in fact, these values are among the lowest for CT scans reported in the literature. Concern also exists that ultrasonography might be adequate for acute management in the emergency department, but inadequate for patients that need surgery and a treatment provider is likely to require a CT before surgical intervention. As a result of this study and these limitations, the first-line imaging modality for evaluating the clinical suspicion of obstructive nephrolithiasis is a controversial topic. However, clear advantages of ultrasonography exist, including availability, cost and lack of exposure to ionizing radiation. Ultrasonography is unique in that it is the only portable imaging modality for evaluation of nephrolithiasis allowing practitioners to evaluate patients at the bedside. Ultrasonography has also traditionally been considered to cost about half as much as a standard CT, although the entire cost of the encounter might be similar for both modalities according to the STONE trial data38.
The effects of ionizing radiation accumulate throughout a patient’s life, therefore, exposure must be as low as reasonably achievable, especially in paediatric patients (<14 years old) or those who are pregnant to prevent cumulative exposure to levels of radiation that are able to induce malignancies28. In pregnant patients concern also exists regarding the potential teratogenic effects of radiation on the developing fetus39. Ultrasonography does not use ionizing radiation, for this reason the AUA, EAU and ACR recommend that ultrasonography be the first-line imaging modality in young and pregnant patients12,25,26. Ultrasonography also has increased accuracy in children owing to their small body size meaning that the distance between the ultrasonography probe and anatomy of interest is reduced37. In pregnant women, signs of obstruction such as a lack of ureteral jets can be used as a surrogate marker of an obstructing stone36.
Imaging guidelines differ between the AUA, ACR and EAU. Currently the EAU is the only oversight body that recommends ultrasonography as a first-line evaluation for patients with suspected obstructing nephrolithiasis26. However, this recommendation might change as future guideline committees evaluate data from the STONE trial. Our research group is currently working on several approaches to improve ultrasonography for kidney stone management. This research includes the use of stone shadow, twinkling artefact and stone-specific imaging. Currently, care should be taken when measuring stone size using ultrasonography. The width of the ultrasound beam, and, therefore, resolution, are similar to the size of some small stones, which might result in an overestimation of true stone size. In one study, up to 50% of kidney stones <5 mm in size were measured as ≥ 5 mm37. Our group has measured the shadow behind the stone, effectively measuring where waves are absent, rather than the waves variably bouncing off the front surface of the stone40. Measuring stone shadow improves the measurement accuracy of ex vivo stones estimating stone size when using ultrasonography to values similar to those of CT (FIG. 3).
Figure 3. Comparison of stone size estimates by B-mode ultrasonography and CT.
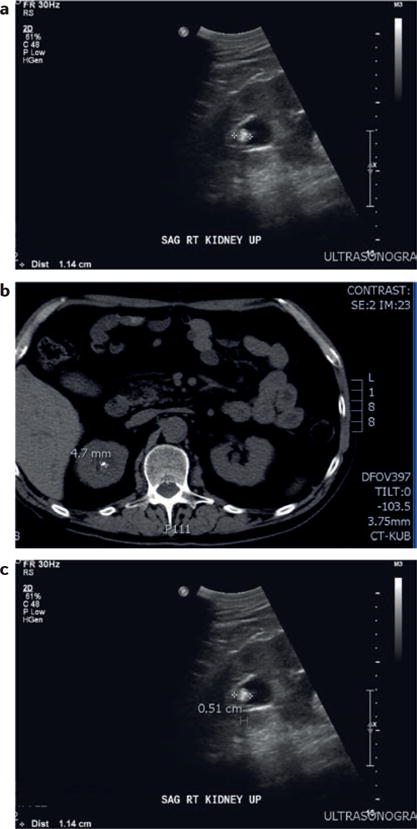
a | B-mode ultrasonographic stone sizing on a longitudinal view of the kidney. b | CT scan image with an estimate of stone size, which is about half of the estimated size according to ultrasonography. c | Measurement of the stone shadow using B-mode ultrasonography provides a much closer estimate to that estimated using CT imaging.
Use of the twinkling artefact assists in identifying stones and can improve the specificity of ultrasonography by differentiating stones from other echogenic structures37,41. B-mode and Doppler ultrasonography can be used to induce a twinkling artefact (FIG. 4). The twinkling artefact is the appearance of a mosaic of colours in a Doppler ultrasound image42,43. The twinkling artefact improves stone identification and specificity (FIG. 4).
Figure 4. Comparison of ultrasonography in B-mode or the novel ‘S-mode’ in humans.
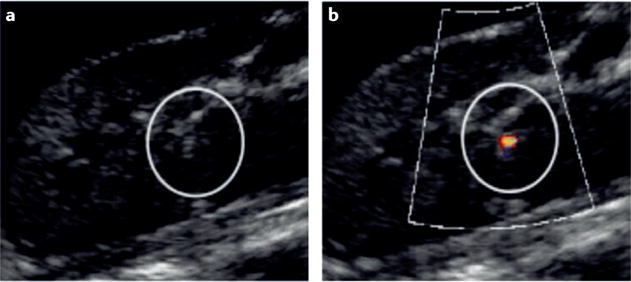
a | Conventional B-mode and b | novel S-mode. S-Mode combines enhanced B-mode and enhanced Doppler detection based on the twinkling artefact to make the stone particularly evident in the image. The bright opaque green on the bright white stone increases the contrast:background ratio, enabling easy of identification of the stone41.
Taking this research even further, our group is working on a stone-specific mode for ultrasonography termed ‘S-mode’ to harness the inherent differences between stones and their surrounding tissues42,44. Ultrasonographic greyscale imaging is currently optimized for visualization and differentiation of soft tissues. An unintended consequence of this configuration is the reduction in visualization and resolution of kidney stones. For example, spatial compounding, which is the averaging of images captured from multiple angles, is commonly present on commercial ultrasonography equipment. This technique reduces speckles on the image as it smooths and averages the contrast between tissues. However, this averaging can reduce the echogenicity of a stone making it appear larger than it actually is, reducing detectability and overestimating the size. Furthermore, transmit beam shape and frequency can be changed to increase the accuracy of stone detection and sizing, such as can be achieved with harmonic imaging40. Our basic science research has indicated that the twinkling artefact is probably caused by microbubbles present on the surface of the stone45. In S-mode, the Doppler ultrasonography transmit signal is optimized to excite these microbubbles, and receiver signal processing is tuned to detect the bubbles’ response. This optimization makes twinkling a design feature rather than an artefact. Some of these techniques can be implemented with current ultrasonography systems; however, others require modification of the processing systems by the manufacturing company, which would not be technically difficult.
These ultrasonography techniques continue to evolve, but a previous version of S-mode ultrasonography performed better than conventional ultrasonography in humans, with a sensitivity of 80%, specificity of 90%, a positive predictive value of 76% and a negative predictive value of 92%46. In the future, minimizing the system settings available to the operator and increasing automated stone detection and sizing are possibilities, and should reduce the user variability of ultrasonographic imaging.
In summary, ultrasonography is currently less sensitive and specific than CT imaging for detecting and sizing of stones, but has good diagnostic ability, and can reliably enable detection of hydronephrosis. This technique is recommended as the first-line imaging modality for patients that are pregnant and paediatric patients (<14 years old). An initial ultrasonography procedure might save some patients the expense and radiation exposure of a CT scan, and nondiagnostic ultrasonography can be followed by an alternative imaging modality, as is recommended in the EAU guidelines. Ultrasonography currently has some limitations, but efforts are underway to improve its effectiveness for kidney stone imaging. Moving forward, use of point-of-care ultrasonography is rapidly increasing, which will probably increase operator experience and confidence with this modality47,48. Research efforts should continue, with a focus on improving stone visualization; increasing sensitivity, specificity and stone sizing; and decreasing user variability.
Kidney, ureter, bladder radiography
KUB plain film radiography and fluoroscopy use a single energy source to produce photons, which pass through tissues in an anterior-to-posterior orientation encountering a contralateral receiver. This technique uses the same fundamental concepts as CT but in a single plane. Historically, KUB radiography has been used to conduct an intravenous pyelogram, which enabled evaluation of the presence of hydronephrosis and obstruction. This modality was largely replaced with the introduction of CT as an imaging technique49. Currently, the sensitivity and specificity of standard KUB radiography is estimated to be 57% and 76%, respectively25. Advantages of KUB radiography include relatively low ionizing radiation exposure compared with CT (0.15 mSv) and low cost (~10% of ultrasonography)50. If stones can be visualized using KUB radiography, they are also likely to be visible under fluoroscopy, which can be used as a guide during shockwave lithotripsy or ureteroscopy. However, as this imaging modality only views stones at one angle, accuracy is decreased yielding reduced sensitivity and specificity and, therefore, limiting its utility. Many stone types can be visualized using KUB radiography; however cystine and struvite stones often are poorly visible on KUB radiography, and uric acid and matrix stones are not visible at all. To compensate for this phenomenon, ultrasonography and KUB radiography can be performed in conjunction, enabling the higher sensitivity of ultrasonography to augment the higher specificity of KUB radiography25. The AUA suggests use of this combined imaging approach for the evaluation of ureteral stone disease during stone passage or after treatment51,52 (FIGS 2,5). For example, an obstructing stone (FIG. 5a) can be observed to move after treatment (FIG. 5b). However, small stones over a bony structure, or those shadowed by bowel gas can be concealed. When evaluating for new stones, KUB radiography has a sensitivity of 37.0% for stones <5 mm, but this increases to 87.5% for stones >5 mm52. Overall, KUB radiography is cost effective compared with other modalities for monitoring stone size in stone formers who are receiving medical therapy53.
Figure 5. Two plain films of the abdomen before and after treatment for an obstructing left-ureteral stone.
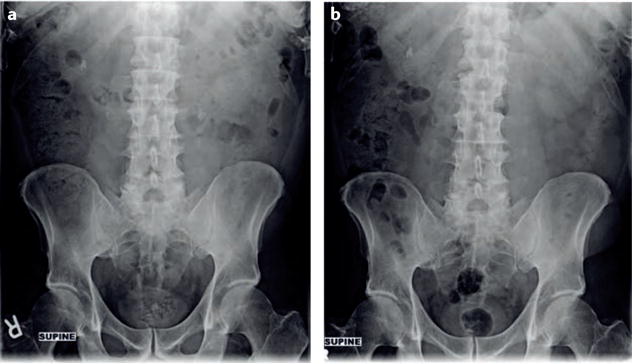
This patient also underwent CT imaging (FIG. 2). a | The left obstructing stone is clearly visible before treatment. b | After treatment the stone is no longer visible. Stones overlaying a bony structure, <5 mm or shaded by a bowel gas loop can easily be missed.
Advances in KUB radiography fuse the low-radiation dose of KUB radiography with the computational imaging capacity of CT. Digital tomosynthesis integrates KUB radiography scout films taken in an arc around the patient — somewhat akin to a CT scan — with computer integration of the image data from an opposed detector. This procedure enables visualization of stones from multiple angles rather than simply anterior to posterior, and has been used extensively in breast imaging as an alternative screening modality for mammography54–56. For patients with kidney stones, imaging at multiple angles improves sensitivity and specificity with scant increases in radiation exposure57,58. These imaging modalities are currently experimental, but they indicate that KUB radiography might remain an important technique in kidney stone imaging. Overall, KUB radiography is most helpful in evaluating a patient with known stone disease, and is less useful in the acute stone setting. However, the low sensitivity of this imaging modality is improved through pairing with ultrasonography and by technological advances such as digital tomosynthesis.
MRI
MRI functions by using a magnetic field to align the patient’s free water protons along a magnetic field axis. A radiofrequency antenna, referred to as a coil, is placed over the area to be imaged and releases pulses of energy that disrupt the alignment of the protons. When the pulses stop, protons release energy as they realign with the magnetic field — this released energy can be captured as an image. The sensitivity of MRI for stone imaging is variable, and, like ultrasonography, can be augmented by hydronephrosis59. Using standard MRI sequences, stones appear as a nonspecific signal void60; however, by adjusting the imaging sequence, stones can be identified with increased reliably61. The sensitivity of MRI, at 82%, is higher than that of ultrasonography and KUB radiography but less than that of CT, as stones are less easily visible when using MRI than they are when using CT25. Hydronephrosis is easily visible, but stones might not clearly be the cause of the obstruction. The differential diagnoses for incidentally discovered hydronephrosis includes stone disease and obstruction by a known malignancy and definitive diagnosis can require a CT scan to detect a ureteral stone (FIG. 6). When stones are visualized on MRI the modality is diagnostic, making specificity high at 98.3%22. A major advantage of MRI is the ability to provide 3D imaging without radiation. Unfortunately, the drawbacks of MRI prevent it from widespread use in stone imaging. In general, MRI costs about three times more than a CT scan and has lower accuracy and much longer image acquisition times. MRI is probably most appropriately used as an adjunctive to ultrasonography in patients that are pregnant. During pregnancy the kidneys undergo physiological dilatation, therefore, removing hydronephrosis as a surrogate marker of obstruction. MRI has been used as a diagnostic modality when stones cannot be visualized using ultrasonography but there is clinical suspicion of obstructing nephrolithiasis62. The ACR, AUA and EAU guidelines suggest that MRI be used as a second-line modality when ultrasonography is nondiagnostic in patients that are pregnant12,25,26. Low-dose CT has also been used in this population63; however the risks of radiation exposure must be discussed with the patient. In the future, ultrashort-echo-time MRI sequences might improve the sensitivity, specificity, and accuracy of stone sizing using MRI61.
Figure 6. Image sequence demonstrating coronal cuts on MRI.
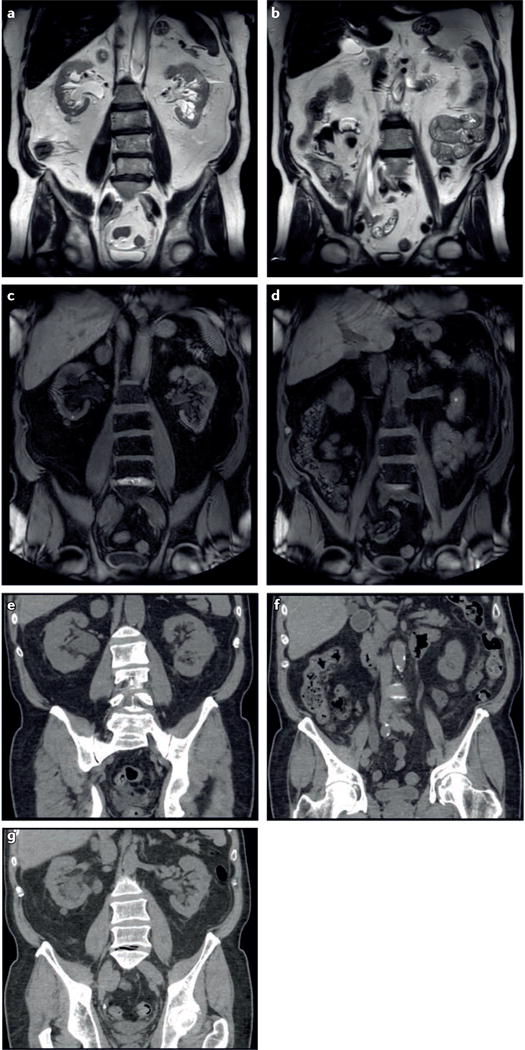
a,b | Images obtained using T2 and c,d | images obtained using T1 sequences, clearly demonstrating hydronephrosis but distal pathology is not clear. Scan performed for cancer surveillance — differential included metastasis, extrinsic ureteral compression and stones. e-g | CT images showing the hydronephrosis and hydroureter; a distal right ureteral stone is now easily visualized enabling diagnosis and considerably altering this patient’s treatment course.
Conclusions
Evaluation of patients with flank pain and haematuria depends on patient age, BMI and whether the patient is pregnant. Ultrasonography should be considered the standard-of-care, first-line imaging modality for patients <14 years of age and those who are pregnant. This modality should be considered for all patients with potential nephrolithiasis when a strong suspicion of stones exists and in thin (BMI <30) patients. CT is currently considered by the AUA and ACR to be the gold-standard modality for evaluation of patients with acute flank pain where clinical suspicion of nephrolithiasis exists. CT is also recommended by the EAU as the modality of choice after inconclusive ultrasonography. A proposed algorithm might assist in deciding on the best approach for imaging patients in the emergency department (FIG. 1). Level one evidence is now available to support the use of ultrasonography in nonobese (BMI <30) adults as a first-line modality. This finding is currently controversial, but could ultimately result in an increase in the use of ultrasonography as an initial imaging study for patients with acute stones. Regardless of the initial imaging modality, clinicians must attempt to reduce radiation exposure to as low as reasonably achievable. Some inconclusive results are to be expected when evaluating a patient using ultrasonography, and imaging with a low-dose CT in these circumstances is reasonable. In addition, advances in CT, ultrasonography, KUB radiography, and MRI technologies are continuing and are likely to improve all modalities in the future.
Key points.
Noncontrast CT is the most accurate imaging modality for kidney stones owing to high sensitivity, specificity, accurate stone sizing, and the ability to evaluate non-stone-related pathologies
Ultrasonography has a lower sensitivity and specificity than CT, but does not expose patients to ionizing radiation and is less expensive than CT
Ultrasonography has several limitations, but a randomized controlled trial demonstrated similar performance in the emergency department to that of CT for patients with suspected kidney stones
Ultrasonography is the first-line imaging modality for pregnant women and patients <14 years old
Low-dose CT has many of the same advantages of standard CT and reduces radiation exposure; however, its diagnostic accuracy is reduced in obese patients and dose modulation should be considered
In the future, improvements in CT, ultrasonography, kidney ureter bladder radiography, and MRI might improve the accuracy of imaging kidney stones
Acknowledgments
This work and Review are part of a large collaborative effort, and we appreciate the help of our many collaborators at the University of Washington Center for Industrial and Medical Ultrasound, the University of Washington Department of Urology, Washington, and the National Institute of Diabetes and Digestive and Kidney Diseases Program Project DK043881, USA. This material is the result of work supported by resources from the VA Puget Sound Health Care System, Seattle, Washington, USA. Funding was provided by National Space Biomedical Research Institute through NASA NCC 9-58, grants from the National Institute of Diabetes and Digestive and Kidney Diseases (DK043881 and DK092197), the University of Washington Applied Physics Laboratory, and the University of Washington Department of Urology.
Footnotes
Author contributions
All authors researched data, discussed content, wrote and reviewed and edited the manuscript before submission.
Competing interests statement
The authors declare no competing interests.
References
- 1.Scales CD, et al. Prevalence of kidney stones in the United States. Eur Urol. 2012;62:160–165. doi: 10.1016/j.eururo.2012.03.052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Stamatelou KK, Francis ME, Jones CA, Nyberg LM, Curhan GC. Time trends in reported prevalence of kidney stones in the United States: 1976–1994. Kidney Int. 2003;63:1817–1823. doi: 10.1046/j.1523-1755.2003.00917.x. [DOI] [PubMed] [Google Scholar]
- 3.Fwu CW, Eggers PW, Kimmel PL, Kusek JW, Kirkali Z. Emergency department visits, use of imaging, and drugs for urolithiasis have increased in the United States. Kidney Int. 2013;83:479–486. doi: 10.1038/ki.2012.419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Preminger GM, et al. 2007 guideline for the management of ureteral calculi. J Urol. 2007;178:2418–2434. doi: 10.1016/j.juro.2007.09.107. [DOI] [PubMed] [Google Scholar]
- 5.Scales CD, Jr, et al. Urinary stone disease: advancing knowledge, patient care, and population health. Clin J Am Soc Nephrol. 2016;11:1305–1312. doi: 10.2215/CJN.13251215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Smith-Bindman R, et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. N Engl J Med. 2014;371:1100–1110. doi: 10.1056/NEJMoa1404446. [DOI] [PubMed] [Google Scholar]
- 7.Miller NL, Evan AP, Lingeman JE. Pathogenesis of renal calculi. Urol Clin North Am. 2007;34:295–313. doi: 10.1016/j.ucl.2007.05.007. [DOI] [PubMed] [Google Scholar]
- 8.Hammad FT, Lammers WJ, Stephen B, Lubbad L. Propagation of the electrical impulse in reversible unilateral ureteral obstruction as determined at high electrophysiological resolution. J Urol. 2011;185:744–750. doi: 10.1016/j.juro.2010.09.078. [DOI] [PubMed] [Google Scholar]
- 9.Ordon M, Schuler TD, Ghiculete D, Pace KT, Honey RJ. Stones lodge at three sites of anatomic narrowing in the ureter: clinical fact or fiction? J Endourol. 2013;27:270–276. doi: 10.1089/end.2012.0201. [DOI] [PubMed] [Google Scholar]
- 10.Fielding JR, Silverman SG, Samuel S, Zou KH, Loughlin KR. Unenhanced helical CT of ureteral stones: a replacement for excretory urography in planning treatment. AJR Am J Roentgenol. 1998;171:1051–1053. doi: 10.2214/ajr.171.4.9762995. [DOI] [PubMed] [Google Scholar]
- 11.Coll DM, Varanelli MJ, Smith RC. Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. AJR Am J Roentgenol. 2002;178:101–103. doi: 10.2214/ajr.178.1.1780101. [DOI] [PubMed] [Google Scholar]
- 12.Coursey CA, et al. ACR Appropriateness Criteria(R) acute onset flank pain-suspicion of stone disease. Ultrasound Q. 2012;28:227–233. doi: 10.1097/RUQ.0b013e3182625974. [DOI] [PubMed] [Google Scholar]
- 13.Memarsadeghi M, et al. Unenhanced multi-detector row CT in patients suspected of having urinary stone disease: effect of section width on diagnosis. Radiology. 2005;235:530–536. doi: 10.1148/radiol.2352040448. [DOI] [PubMed] [Google Scholar]
- 14.Schwartz BF, Schenkman N, Armenakas NA, Stoller ML. Imaging characteristics of indinavir calculi. J Urol. 1999;161:1085–1087. [PubMed] [Google Scholar]
- 15.Nakada SY, et al. Determination of stone composition by noncontrast spiral computed tomography in the clinical setting. Urology. 2000;55:816–819. doi: 10.1016/s0090-4295(00)00518-5. [DOI] [PubMed] [Google Scholar]
- 16.Shah K, et al. Predicting effectiveness of extracorporeal shockwave lithotripsy by stone attenuation value. J Endourol. 2010;24:1169–1173. doi: 10.1089/end.2010.0124. [DOI] [PubMed] [Google Scholar]
- 17.Kim SC, et al. Cystine calculi: correlation of CT-visible structure, CT number, and stone morphology with fragmentation by shock wave lithotripsy. Urol Res. 2007;35:319–324. doi: 10.1007/s00240-007-0117-1. [DOI] [PubMed] [Google Scholar]
- 18.Duan X, et al. Differentiation of calcium oxalate monohydrate and calcium oxalate dihydrate stones using quantitative morphological information from micro-computerized and clinical computerized tomography. J Urol. 2013;189:2350–2356. doi: 10.1016/j.juro.2012.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Primak AN, et al. Noninvasive differentiation of uric acid versus non-uric acid kidney stones using dualenergy CT. Acad Radiol. 2007;14:1441–1447. doi: 10.1016/j.acra.2007.09.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Qu M, et al. Dual-energy dual-source CT with additional spectral filtration can improve the differentiation of non-uric acid renal stones: an ex vivo phantom study. AJR Am J Roentgenol. 2011;196:1279–1287. doi: 10.2214/AJR.10.5041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wang J, et al. Characterisation of urinary stones in the presence of iodinated contrast medium using dual-energy CT: a phantom study. Eur Radiol. 2012;22:2589–2596. doi: 10.1007/s00330-012-2532-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Coursey CA, et al. Dual-energy multidetector CT: how does it work, what can it tell us, and when can we use it in abdominopelvic imaging? Radiographics. 2010;30:1037–1055. doi: 10.1148/rg.304095175. [DOI] [PubMed] [Google Scholar]
- 23.Vujovic A, Keoghane S. Management of renal stone disease in obese patients. Nat Clin Pract Urol. 2007;4:671–676. doi: 10.1038/ncpuro0988. [DOI] [PubMed] [Google Scholar]
- 24.Neitlich T, Neitlich J. The imaging evaluation of cholelithiasis in the obese patient-ultrasound versus CT cholecystography: our experience with the bariatric surgery population. Obes Surg. 2009;19:207–210. doi: 10.1007/s11695-008-9582-z. [DOI] [PubMed] [Google Scholar]
- 25.Fulgham PF, Assimos DG, Pearle MS, Preminger GM. Clinical effectiveness protocols for imaging in the management of ureteral calculous disease: AUA technology assessment. J Urol. 2013;189:1203–1213. doi: 10.1016/j.juro.2012.10.031. [DOI] [PubMed] [Google Scholar]
- 26.Türk C, et al. EAU guidelines on interventional treatment for urolithiasis. Eur Urol. 2015;69:475–482. doi: 10.1016/j.eururo.2015.07.041. [DOI] [PubMed] [Google Scholar]
- 27.Blacklock NJ. The pattern of urolithiasis in the Royal Navy. J R Nav Med Serv. 1965;51:99–111. [PubMed] [Google Scholar]
- 28.National Research Council. Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII, Phase I, Letter Report. The National Acadamies Press; 1998. [PubMed] [Google Scholar]
- 29.Brenner DJ, Hall EJ. Computed tomography — an increasing source of radiation exposure. N Engl J Med. 2007;357:2277–2284. doi: 10.1056/NEJMra072149. [DOI] [PubMed] [Google Scholar]
- 30.Jellison FC, et al. Effect of low dose radiation computerized tomography protocols on distal ureteral calculus detection. J Urol. 2009;182:2762–2767. doi: 10.1016/j.juro.2009.08.042. [DOI] [PubMed] [Google Scholar]
- 31.Niemann T, Kollmann T, Bongartz G. Diagnostic performance of low-dose CT for the detection of urolithiasis: a meta-analysis. AJR Am J Roentgenol. 2008;191:396–401. doi: 10.2214/AJR.07.3414. [DOI] [PubMed] [Google Scholar]
- 32.Alsyouf M, et al. Comparing stone attenuation in low-and conventional-dose noncontrast computed tomography. J Endourol. 2014;28:704–707. doi: 10.1089/end.2013.0789. [DOI] [PubMed] [Google Scholar]
- 33.Poletti PA, et al. Low-dose versus standard-dose CT protocol in patients with clinically suspected renal colic. AJR Am J Roentgenol. 2007;188:927–933. doi: 10.2214/AJR.06.0793. [DOI] [PubMed] [Google Scholar]
- 34.Gervaise A, et al. Low-dose CT with automatic tube current modulation, adaptive statistical iterative reconstruction, and low tube voltage for the diagnosis of renal colic: impact of body mass index. AJR Am J Roentgenol. 2014;202:553–560. doi: 10.2214/AJR.13.11350. [DOI] [PubMed] [Google Scholar]
- 35.Erwin BC, Carroll BA, Sommer FG. Renal colic: the role of ultrasound in initial evaluation. Radiology. 1984;152:147–150. doi: 10.1148/radiology.152.1.6729105. [DOI] [PubMed] [Google Scholar]
- 36.Asrat T, Roossin MC, Miller EI. Ultrasonographic detection of ureteral jets in normal pregnancy. Am J Obstet Gynecol. 1998;178:1194–1198. doi: 10.1016/s0002-9378(98)70322-9. [DOI] [PubMed] [Google Scholar]
- 37.Ray AA, Ghiculete D, Pace KT, Honey RJ. Limitations to ultrasound in the detection and measurement of urinary tract calculi. Urology. 2010;76:295–300. doi: 10.1016/j.urology.2009.12.015. [DOI] [PubMed] [Google Scholar]
- 38.Melnikow J, et al. Cost analysis of the STONE randomized trial: can health care costs be reduced one test at a time? Med Care. 2016;54:337–342. doi: 10.1097/MLR.0000000000000487. [DOI] [PubMed] [Google Scholar]
- 39.Patel SJ, Reede DL, Katz DS, Subramaniam R, Amorosa JK. Imaging the pregnant patient for nonobstetric conditions: algorithms and radiation dose considerations. Radiographics. 2007;27:1705–1722. doi: 10.1148/rg.276075002. [DOI] [PubMed] [Google Scholar]
- 40.Dunmire B, et al. Use of the acoustic shadow width to determine kidney stone size with ultrasound. J Urol. 2016;195:171–177. doi: 10.1016/j.juro.2015.05.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Sorensen MD, et al. B-mode ultrasound versus color Doppler twinkling artifact in detecting kidney stones. J Endourol. 2013;27:149–153. doi: 10.1089/end.2012.0430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Cunitz B, et al. Improved detection of kidney stones using an optimized doppler imaging sequence. IEEE Int Ultrason Symp. 2014;2014:452–455. doi: 10.1109/ULTSYM.2014.0112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Sapozhnikov O, Lu W, Bailey MR, Kaczkowski P, Crum LA. 2aBA6 Bubbles trapped on the surface of kidney stones as a cause of the twinkling artifact in ultrasound imaging. Proc Meet Acoust. 2013;19:075033. doi: 10.1121/1.4800292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Dunmire B, et al. Tools to improve the accuracy of kidney stone sizing with ultrasound. J Endourol. 2015;29:147–152. doi: 10.1089/end.2014.0332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Khokhlova T, Li T, Sapozhnikov O, Hwang JH. The use of twinkling artifact of Doppler imaging to monitor cavitation in tissue during high intensity focused ultrasound therapy. Proc Meet Acoust. 2013;19:075034. doi: 10.1121/1.4800366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Sorensen MD, et al. Focused ultrasonic propulsion of kidney stones: review and update of preclinical technology. J Endourol. 2013;27:1183–1186. doi: 10.1089/end.2013.0315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Sanders JL, Noble VE, Raja AS, Sullivan AF, Camargo CA., Jr Access to and use of point-of-care ultrasound in the emergency department West. J Emerg Med. 2015;16:747–752. doi: 10.5811/westjem.2015.7.27216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Talley BE, et al. Variable access to immediate bedside ultrasound in the emergency department. West J Emerg Med. 2011;12:96–99. [PMC free article] [PubMed] [Google Scholar]
- 49.Worster A, Preyra I, Weaver B, Haines T. The accuracy of noncontrast helical computed tomography versus intravenous pyelography in the diagnosis of suspected acute urolithiasis: a metaanalysis. Ann Emerg Med. 2002;40:280–286. doi: 10.1067/mem.2002.126170. [DOI] [PubMed] [Google Scholar]
- 50.Thomson JM, Glocer J, Abbott C, Maling TM, Mark S. Computed tomography versus intravenous urography in diagnosis of acute flank pain from urolithiasis: a randomized study comparing imaging costs and radiation dose. Australas Radiol. 2001;45:291–297. doi: 10.1046/j.1440-1673.2001.00923.x. [DOI] [PubMed] [Google Scholar]
- 51.Johnston R, Lin A, Du J, Mark S. Comparison of kidney-ureter-bladder abdominal radiography and computed tomography scout films for identifying renal calculi. BJU Int. 2009;104:670–673. doi: 10.1111/j.1464-410X.2009.08542.x. [DOI] [PubMed] [Google Scholar]
- 52.Ege G, Akman H, Kuzucu K, Yildiz S. Can computed tomography scout radiography replace plain film in the evaluation of patients with acute urinary tract colic? Acta Radiol. 2004;45:469–473. doi: 10.1080/02841850410005264. [DOI] [PubMed] [Google Scholar]
- 53.Bishoff JT, Rastinehad AR. In: Campbell-Walsh Urology. Wein AJ, Kavoussi LR, Partin AW, Peters CA, editors. Vol. 1. Elsevier; 2016. pp. 26–62. Ch. 2. [Google Scholar]
- 54.Houssami N, Skaane P. Overview of the evidence on digital breast tomosynthesis in breast cancer detection. Breast. 2013;22:101–108. doi: 10.1016/j.breast.2013.01.017. [DOI] [PubMed] [Google Scholar]
- 55.Svahn TM, Houssami N, Sechopoulos I, Mattsson S. Review of radiation dose estimates in digital breast tomosynthesis relative to those in two-view full-field digital mammography. Breast. 2015;24:93–99. doi: 10.1016/j.breast.2014.12.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Svahn TM, Macaskill P, Houssami N. Radiologists’ interpretive efficiency and variability in true-and false-positive detection when screen-reading with tomosynthesis (3D-mammography) relative to standard mammography in population screening. Breast. 2015;24:687–693. doi: 10.1016/j.breast.2015.08.012. [DOI] [PubMed] [Google Scholar]
- 57.Neisius A, et al. Digital tomosynthesis: a new technique for imaging nephrolithiasis. Specific organ doses and effective doses compared with renal stone protocol noncontrast computed tomography. Urology. 2014;83:282–287. doi: 10.1016/j.urology.2013.10.004. [DOI] [PubMed] [Google Scholar]
- 58.Mermuys K, et al. Digital tomosynthesis in the detection of urolithiasis: diagnostic performance and dosimetry compared with digital radiography with MDCT as the reference standard. AJR Am J Roentgenol. 2010;195:161–167. doi: 10.2214/AJR.09.3075. [DOI] [PubMed] [Google Scholar]
- 59.Karabacakoglu A, Karakose S, Ince O, Cobankara OE, Karalezli G. Diagnostic value of diuretic-enhanced excretory MR urography in patients with obstructive uropathy. Eur J Radiol. 2004;52:320–327. doi: 10.1016/j.ejrad.2003.10.023. [DOI] [PubMed] [Google Scholar]
- 60.Robson MD, Gatehouse PD, Bydder M, Bydder GM. Magnetic resonance: an introduction to ultrashort TE (UTE) imaging. J Comput Assist Tomogr. 2003;27:825–846. doi: 10.1097/00004728-200311000-00001. [DOI] [PubMed] [Google Scholar]
- 61.Yassin A, et al. In vitro MR imaging of renal stones with an ultra-short echo time magnetic resonance imaging sequence. Acad Radiol. 2012;19:1566–1572. doi: 10.1016/j.acra.2012.07.008. [DOI] [PubMed] [Google Scholar]
- 62.Mullins JK, Semins MJ, Hyams ES, Bohlman ME, Matlaga BR. Half Fourier single-shot turbo spin-echo magnetic resonance urography for the evaluation of suspected renal colic in pregnancy. Urology. 2012;79:1252–1255. doi: 10.1016/j.urology.2011.12.016. [DOI] [PubMed] [Google Scholar]
- 63.White WM, et al. Low-dose computed tomography for the evaluation of flank pain in the pregnant population. J Endourol. 2007;21:1255–1260. doi: 10.1089/end.2007.0017. [DOI] [PubMed] [Google Scholar]