

Abstract
Background:
Remnant preservation may confer important advantages in the anterior cruciate ligament (ACL)–reconstructed knee. However, the presence of a large remnant may obscure visualization and impair the ability to correctly place tunnels during surgery.
Purpose:
To determine whether tunnel placement during anatomic ACL reconstruction using the single anteromedial bundle biological augmentation (SAMBBA) technique is consistent and precise when a large native remnant is preserved.
Study Design:
Case series; Level of evidence, 4.
Methods:
Included in this study were 99 patients undergoing an ACL reconstruction during which at least 50% of the native ACL was preserved. The femoral tunnel was created using an outside-in specific guide. The tibial tunnel was positioned in the anteromedial region of the ACL footprint, and the remnant was carefully preserved while drilling and passing the semitendinosus graft through it. Postoperatively, 3-dimensional computed tomography (3D CT) was used to evaluate tunnel placement. The mean tunnel locations were calculated and the standard deviation was used to evaluate precision of positioning. Inter- and intrareader agreement were determined to assess reliability of evaluation of tunnel position.
Results:
The center of the femoral tunnel was positioned at a mean 19.4% (SD, 2%) of the depth of the notch and a mean 23.1% (SD, 3.5%) of the lateral wall height. The center of the tibial tunnel was positioned at a mean 36.3% (SD, 3.8%) of the anteroposterior length of the tibial plateau and at a mean 47.0% (SD, 2.7%) of the mediolateral width. The small standard deviations demonstrate that this technique allows precise tunnel placement. The tunnel positions achieved were consistent with previous anatomic studies of femoral and tibial anteromedial bundle insertion. Intra- and interobserver reliability were high.
Conclusion:
Three-dimensional CT evaluation demonstrated that despite the presence of a large remnant, placement of femoral and tibial tunnels for anatomic ACL reconstruction using the SAMBBA technique is consistent and precise.
Keywords: anatomic ACL reconstruction, ACL tunnel position, remnant preservation, 3D CT scan
Over the past 20 years, knowledge regarding the anterior cruciate ligament (ACL) has evolved considerably. Anatomically, the identification of 2 bundles45 has allowed for a more detailed description of the femoral and tibial insertions.30 As a result of this improved understanding, recent interest has focused on reconstruction techniques that allow better replication of the anatomy of the native ACL and its function.31,44,48 This is important because it is clear that graft malposition influences knee kinematics18,26,46,47,49 and postoperative clinical outcomes.16,33,47 Suboptimal tunnel placement predisposes to early graft failure and can result in a lack of mobility and/or persistent instability.33,43 Accurate placement is guided by several studies that have characterized insertion points and intraoperative landmarks for anatomic ACL reconstruction.3,8,31 Despite this, numerous authors have reported that incorrect tunnel placement is not infrequent, and even with training and experience, surgeons may still have difficulty in correctly positioning tunnels intraoperatively.15,25,32,37
There is concern that the risk of tunnel malposition may be higher if remnant preservation is attempted. The presence of a remnant, particularly if large, can obscure a complete view of the anatomy of the notch.12,31,38 Preservation of the ACL remnant during reconstruction is considered important, as it may confer improved knee stability.2,4,25,26,27,35 It is postulated that a greater intrinsic potential for healing,28 better graft vascularization,26,28 and preservation of proprioceptive nerve fibers21 can result in reduced rates of graft rupture1,3,12,16–18,33,34,40 and improved proprioceptive function.20,27 In addition, it is reported that the presence of the ACL remnant can serve as an important and reliable intraoperative landmark for tunnel positioning, but in contrast, it may also make overall visualization more difficult.31
The aim of this study was therefore to evaluate whether consistent tunnel positioning was achieved in a series of patients undergoing remnant-preserving ACL reconstructions. The hypothesis was that the preservation of a large remnant does not prevent consistent and precise tunnel positioning when using outside-in femoral tunnel drilling, anteromedial (AM) viewing, and the single anteromedial bundle biological augmentation (SAMBBA) technique.34
Methods
This study received institutional review board approval, and all participants gave valid consent to participate. No financial incentives were provided. All patients diagnosed with ACL rupture at a single institution between September 2014 and March 2016 were considered for study eligibility. Those with previous ipsilateral knee ligament surgery or concomitant multiligament injury were excluded. ACL rupture was confirmed by magnetic resonance imaging and clinical examination (including positive Lachman, anterior drawer, and pivot-shift tests, and anterior laxity greater than 4 mm as measured by Rolimeter [Aircast Europe Ltd]). Surgery was indicated in patients with disability and/or incapacity to resume their previous level of activity because of instability symptoms. The senior author (F.B.) performed all surgical reconstructions.
The final eligibility criterion for the study was based on an assessment of the remnant size as visualized intraoperatively. The aim was to avoid skewing the study results by including small remnants that were unlikely to have the potential to affect visualization and therefore tunnel position. Large remnants were defined by their coverage of greater than 50% of the ACL graft at the end of surgery. This was evaluated while viewing through the AM portal with the knee at 90° of flexion. The 50% cutoff was defined by the bisection of the central axis of the ACL graft by a line projected from the central axis of the native posterior cruciate ligament (Figure 1).1
Figure 1.
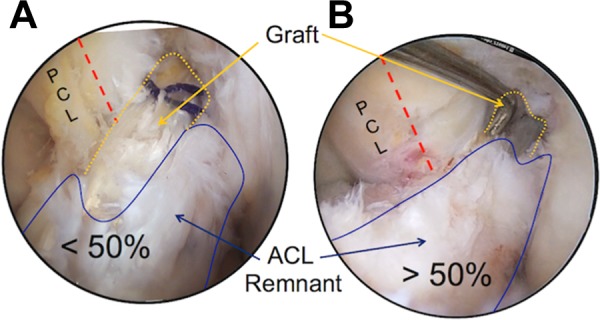
(A) Graft coverage inferior to 50%, in which the anterior cruciate ligament (ACL) remnant does not cover the graft up to of the crossing line with the posterior cruciate ligament (PCL) central fiber. (B) More than 50% of graft coverage, with the ACL remnant covering the graft far beyond the PCL central fiber. Arthroscopic view, left knees, 90° of flexion. Blue line, ACL remnant; orange dotted line, graft; red dashed line, PCL central fiber.
The SAMBBA Technique
The SAMBBA technique has been published previously34 and was used in this series of patients, with a minor modification resulting from surgeon preference. This modification involved drilling a full femoral tunnel and performing femoral fixation with a screw rather than using a socket and suspensory fixation. There were no other modifications to the published technique that is summarized here.
The semitendinosus tendon was harvested with an open-ended stripper, allowing the tibial insertion to be preserved, thereby improving fixation and vascularity of the graft. The tendon was either tripled or quadrupled to ensure a graft diameter of at least 8 mm.
Femoral tunnel drilling was performed with the knee held at 90° of flexion to allow better visualization. The objective was to center the graft in the AM bundle area. A specific outside-in guide (Footprint Femoral ACL guide, Arthrex) was introduced through the anterolateral portal. The camera was introduced through the AM portal in order to achieve optimum visualization of the lateral wall of the notch. The semilunar target of the guide was then positioned in the AM bundle area, with the limit of the ring just distal to the notch outlet and just superior to the inferior cartilaginous limit (Figure 2). This allowed positioning of a guide wire and subsequent drilling with a diameter corresponding to the graft size.
Figure 2.
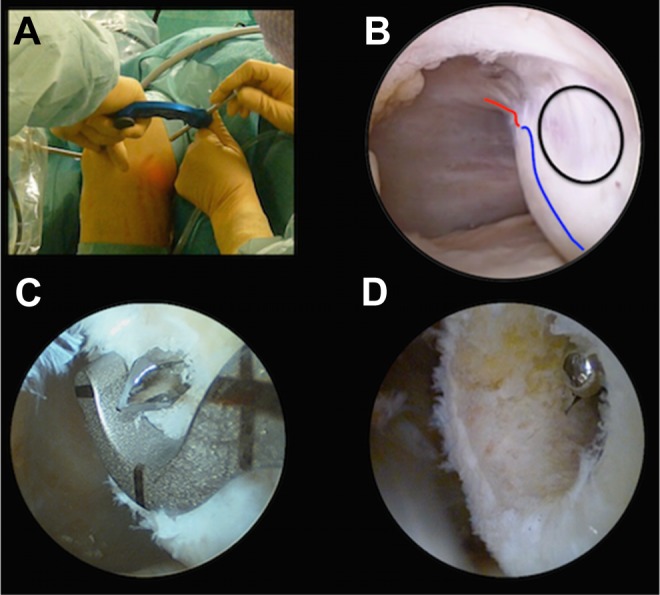
Left knee arthroscopy with anteromedial (AM) viewing. (A) External view showing positioning of specific outside-in femoral guide through the anterolateral portal. (B) Arthroscopic landmark with the camera through the AM portal: black line, ring target of the guide; red line, notch outlet; blue line, anterior-inferior cartilaginous limit. (C) Femoral anterior cruciate ligament footprint guide and emerging drill pin. (D) Femoral tunnel.
The tibial tunnel was drilled in a standard fashion with a guide close to the medial tibial spine and anterior to the posterolateral bundle tibial insertion (Figure 3). The tibial guide was positioned so that the guide wire either split or stayed within the center of the ACL tibial stump and the tunnel entrance was located approximately 1 cm medial to the tibial tuberosity. Drilling was performed in accordance with the SAMBBA technique, which allows preservation of the residual stump and graft passage within it.34 The graft was routed from the preserved hamstring tibial insertion through the tibial tunnel to the femoral tunnel using a suture loop. Tibial fixation was performed using a resorbable interference screw of the same diameter as the tunnel and 25 mm in length. The graft was fixed at 20° of flexion. A resorbable interference screw of the same diameter as the tunnel and 25 mm in length was inserted in the femoral tunnel in an “outside-in” manner through the lateral incision.
Figure 3.
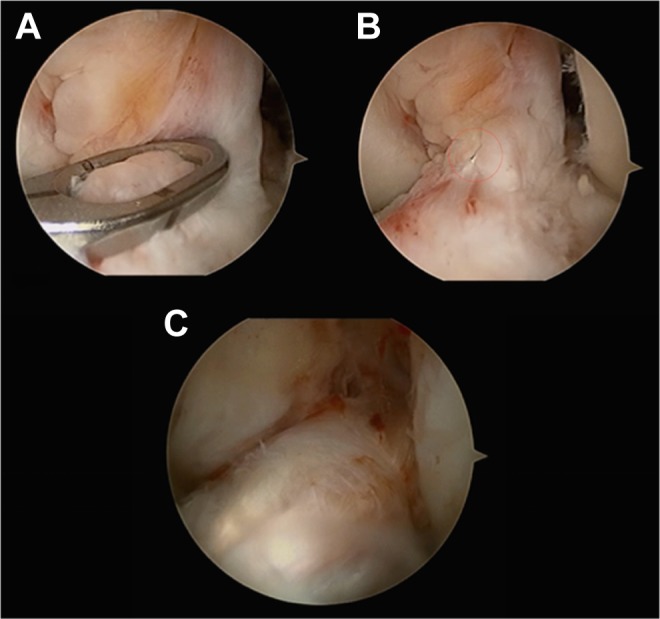
Left knee arthroscopy with anterolateral viewing and the tibial guide placed via the anteromedial portal. (A) Tibial tunnel guide wire positioning: ring target positioned on the tibial stump in the anteromedial anterior cruciate ligament area. (B) Sequential tunnel drilling (6-, 7-, and 8-mm drills). (C) Graft routed from tibia to femur through the stump.
Three-Dimensional Computed Tomography Scan Evaluation
All patients underwent computed tomography (CT) scan with a slice thickness of 0.6 mm within 1 week of surgery. The volume-rendering 3-dimensional (3D) image of the knee was reconstructed to evaluate tunnel position.13,17 In order to evaluate the femoral tunnel, the scan was oriented in a true lateral view by superimposition of the posterior curvature of the condyles in the transparency mode. The Blumensaat line was then marked. Using the 3D mode, the medial condyle was progressively digitally subtracted until the roof of the notch was superimposed on the previously marked radiologic Blumensaat line (Figure 4).
Figure 4.
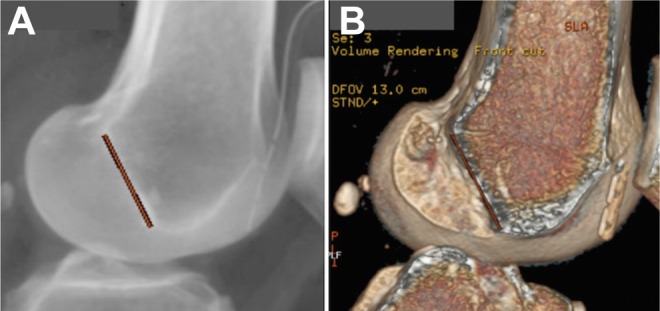
(A) Three-dimensional computed tomography scanner transparency mode: superimposition of the posterior curvature of medial and lateral condyles and marking of the Blumensaat line. (B) The medial condyle is progressively removed in order to obtain superimposition of the roof of the notch with the previously marked Blumensaat line.
The position of the femoral tunnel was evaluated using the Bernard and Hertel quadrant method.5,10,23 The anterior limit of the quadrant was adjusted on the marked Blumensaat line. The position of the femoral tunnel was determined as a percentage of the depth of the notch and as a percentage of the height of the notch. The position of the tibial tunnel was evaluated on an axial view with the sides of the gird tangential to the posterior edges and confined to the other borders of the tibial plateau (Figure 5). The location of the tibial tunnel was determined as a percentage of the anteroposterior length and the mediolateral width of the tibial plateau (Figure 5).
Figure 5.
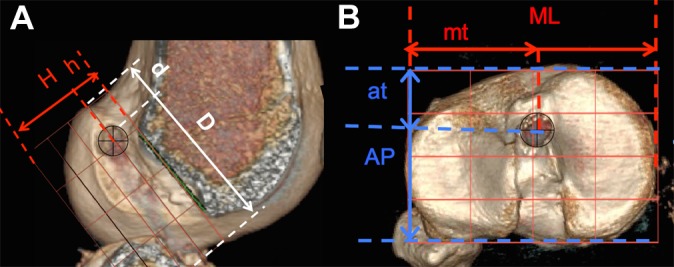
(A) Position of the center of the femoral tunnel (quadrant method). (B) Position of the center of the tibial tunnel. at/AP, position of the tibial tunnel relative to the anteroposterior length; d/D, position of the femoral tunnel relative to the depth of the Blumensaat line; h/H, position of the femoral tunnel relative to the lateral wall height; mt/mL, position of the tibial tunnel relative to the mediolateral width of the tibial plateau.
All measurements were performed with the use of ImageJ software (National Institutes of Health). Two independent evaluators performed the inter- and intraobserver reliability tests. A time period of 3 weeks elapsed between test and retest measurements. All observer-dependent steps in the analysis, including co-registration of the 3D CT models to the base models, establishment of the center of the tunnel apertures, and measurement and calculation of the position of all tibial and femoral bone tunnels, were repeated at retest. The inter- and intraobserver reliability test were performed on the first 35 cases only.
Statistical Analysis
All calculations were made using SPSS software (version 20.0, IBM Corp), with parameters set to describe 95% confidence intervals and significance reported at P < .05. Descriptive data (mean, range, proportions) were determined for the entire cohort. Data for the location of the femoral and tibial tunnels are presented as the mean position (±SD). The intraclass correlation coefficient (ICC) was measured to assess inter- and intrareader agreement for determining reliability among observers. The ICC was interpreted according to the recommendations of Landis and Koch.19
Results
A total of 227 patients underwent ACL reconstruction during the study period. Ninety-nine patients were eligible for inclusion on the basis of more than 50% of graft coverage by the remnant at the end of the surgery. There were 58 male and 41 female patients, the mean age of the study population was 28 (±4) years, and the mean time from injury to surgery was 5.8 (±4.4) months.
Intra- and interobserver reliabilities were excellent (Table 1).
TABLE 1.
Inter- and Intraobserver ICCa
| Measure | Intraobserver ICC (95% CI) | Interobserver ICC (95% CI) | |
|---|---|---|---|
| Femur | d/D | 0.97 (0.95-0.98) | 0.95 (0.91-0.97) |
| h/H | 0.96 (0.94-0.98) | 0.91 (0.81-0.96) | |
| Tibia | mt/ML | 0.87 (0.82-0.90) | 0.84 (0.77-0.93) |
| at/AP | 0.90 (0.87-0.91) | 0.83 (0.82-0.94) |
aIntraclass correlation coefficient (ICC), 95% confidence interval, and 5% significance level, where statistical relationships would be considered significant, satisfactory (0.4-0.75), and excellent (≥0.75). at/AP, position of the tibial tunnel relative to the anteroposterior length; d/D, position of the femoral tunnel relative to the depth of the Blumensaat line; h/H, position of the femoral tunnel relative to the lateral wall height; mt/mL, position of the tibial tunnel relative to the mediolateral width of the tibial plateau.
Femoral Measurements
According to the quadrant method, the center of the mean position of the femoral tunnel was at 19.4% (±2%) of the depth of the notch and 23.1% (±3.5%) of the lateral wall height. All the femoral tunnels were continuous, and no posterior cortical blowout was observed in any patients.
Tibial Measurements
On the tibia, the mean location of the tunnel was at 36.3% (±3.8%) of the anteroposterior length and 47.0% (±2.7%) from medial to lateral (Figure 6).
Figure 6.
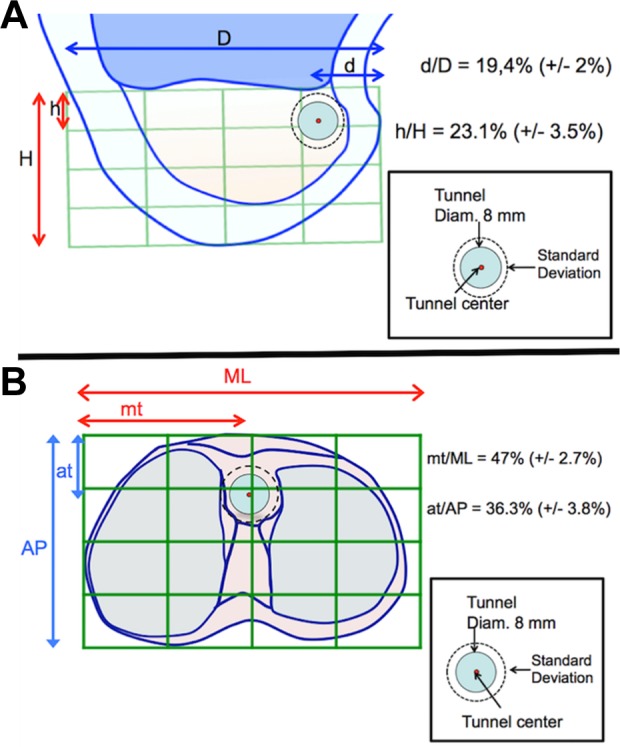
Schematic representation of the location of the 99 (A) femoral and (B) tibial tunnel placements. at/AP, position of the tibial tunnel relative to the anteroposterior length; d/D, position of the femoral tunnel relative to the depth of the Blumensaat line; h/H, position of the femoral tunnel relative to the lateral wall height; mt/mL, position of the tibial tunnel relative to the mediolateral width of the tibial plateau.
Mean location of the femoral and tibial tunnels were comparable to the ACL AM bundle location reported in anatomic studies. Table 2 shows the position of tunnels reported in previous studies.7,14,24,29,39,41,49
TABLE 2.
Overview of Anatomic Studiesa
| First Author (Year) | Methods of Measurement | Femoral AM Bundle | Tibial AM Bundle | n | ||
|---|---|---|---|---|---|---|
| d/D | h/H | at/AP | mt/ML | |||
| Zantop49 (2008) | Standard lateral radiographs | 18.5 | 22.3 | 36 | — | 20 |
| Colombet7 (2006) | Standard lateral radiographs | 26.4 | 25.3 | 36 | — | 7 |
| Lorenz24 (2009) | Standard lateral radiographs | 21 | 22 | 41 | 52 | 12 |
| Iriuchishima14 (2010) | Standard lateral radiographs | 15 | 26 | 31 | 49 | 15 |
| Pietrini29 (2011) | Standard lateral radiographs | 21.6 | 14.2 | 44.2 | 36.3 | 12 |
| Takahashi39 (2006) | Standard lateral radiographs | 31.9 | 26.9 | — | 44.2 | 20 |
| Tsukada41 (2008) | 3D CT | 21.7 | 33.2 | 37.6 | 46.5 | 36 |
| Current study | 3D CT, 2-dimensional quadrant method in standard lateral position | 19.3 | 23.1 | 36.3 | 47 | 99 |
aAll values except those in the last column are percentages. Results presented for sagittal projections of the femur and tibia plus frontal projection of the tibia. at/AP, position of the tibial tunnel relative to the anteroposterior length; d/D, position of the femoral tunnel relative to the depth of the Blumensaat line; h/H, position of the femoral tunnel relative to the lateral wall height; mt/mL, position of the tibial tunnel relative to the mediolateral width of the tibial plateau. Dashes (—) indicate no data available.
Discussion
The principal finding of our study was that outside-in femoral tunnel drilling results in consistent and accurate tunnel placement when using the SAMBBA technique. The study also demonstrates that the presence of a large tibial ACL stump does not prevent correct placement of either tibial or femoral tunnels.
For anatomic ACL reconstruction, correct tunnel placement is necessary in order to obtain consistently excellent clinical results.26,47–49 Knowledge of the ACL attachment areas and their positions relative to reproducible landmarks is a prerequisite for accurate tunnel placement, particularly at the femoral site where small changes in tunnel position have significant effects on ACL graft-length change patterns during knee motion.50 However, there is limited knowledge about the ability to reliably and precisely place tunnels with an outside-in technique if a large ACL remnant is preserved.
This study obtained high-resolution images using a 3D CT scanner to demonstrate femoral and tibial tunnel placement. The advantage of a tomographic evaluation is that it is possible to correct the rotation of the knee and obtain exact reconstructions in the axial, frontal, and sagittal planes.10,13,17 Furthermore, anatomic details can be found more exactly than they could in radiographic images as used by other authors.7,29,41 The literature has described different methods3,6,9 for the description and evaluation of the femoral and tibial insertion sites. However, in this study the modified quadrant method of Bernard and Hertel5 and Staubli and Rauschning36 was used because it is widely accepted and easy to implement.
In the current study, the mean location of the center of the femoral tunnel was 19.4% of the depth of the Blumensaat line and 23.1% of the height of the femoral condyle. The mean location of the center of the tibial tunnel was 36.3% of the anteroposterior diameter of the tibial plateau and 47.0% of the mediolateral width. These results are broadly comparable to those of other studies (Table 2). An explanation for the variations seen between different studies is that various methodologies have been used to define the deep to shallow and condylar height dimensions. An example of this is that in the current study, the deep margin was defined by a grid placed on the deepest part of the articular cartilage on an oriented CT image. In contrast, both Tsukada et al41 and Colombet et al7 used the “over the top position,” which is an anatomically different point. Furthermore, there is a lack of precise agreement between positions determined on imaging and in anatomic specimens. Colombet et al7 compared their clinical measurements in a cadaveric study against CT and found that the deep-superficial measurement had a high interobserver variability (SD, >2 mm) between the 2 methodologies, again offering an explanation for the range of values reported in different studies. This heterogeneity between studies precludes a direct comparison between reports from different authors, but it is reasonable to state that data from the current study are not anomalous compared with other published data for either the tibial or femoral tunnels.11,22,44 Furthermore, the small standard deviations reported in the current study (Figure 6) demonstrate that this technique is consistent, reproducible, and allows precise localization of tunnels. This suggests that remnant preservation does not compromise correct tunnel placement. Instead, the remnant provides a good landmark of the native anatomy, which facilitates an understanding of the correct location of tunnel placement for anatomic reconstruction. A systematic review by van Eck et al42 revealed that 81% of surgeons used this landmark routinely.
This study is subject to certain limitations. The main limitations are that all reconstructions were performed at a single center by a single surgeon who has considerable experience with remnant preservation during ACL reconstruction and that a control group was not included. The external validity of this study’s findings to surgeons who are less experienced with ACL reconstruction or remnant preservation surgery is not known, and additional data from other centers/surgeons are required to further validate this technique. Another limitation is related to the CT measurements. The time interval between repeat measurements was approximately 3 weeks. As such, it is possible that observers were able to recall previously recorded measurements, and this may have artificially inflated the reliability estimates; however, given the nature of the measurements and volume of patients, we believe that this was unlikely. A final limitation is that this study did not have a control group, and no patients with remnants smaller than 50% were included. As a result, it is unknown whether the presence of a large tibial ACL stump had any influence on tunnel position; thus, further comparative study is required. However, it is clear that large remnants did not preclude correct tunnel placement. This is reflected in the small standard deviations reported for mean tibial and femoral tunnel positions, which demonstrate that tunnels were consistently placed in a precise manner.
Conclusion
Three-dimensional CT evaluation demonstrates that despite the presence of a large remnant, placement of femoral and tibial tunnels for anatomic ACL reconstruction using the SAMBBA technique is consistent and precise.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S.-C. receives royalties from, is a paid consultant for, receives research support from, and has made presentations for Arthrex. M.T. is a paid consultant for, receives research support from, and has made presentations for Arthrex.
Ethical approval for this study was provided by the Centre Orthopédique Santy, Lyon, France.
References
- 1. Adachi N, Ochi M, Takazawa K, et al. Morphologic evaluation of remnant anterior cruciate ligament bundles after injury with three-dimensional computed tomography. Knee Surg Sports Traumatol Arthrosc. 2016;24:148–153. [DOI] [PubMed] [Google Scholar]
- 2. Adachi N, Ochi M, Uchio Y, Sumen Y. Anterior cruciate ligament augmentation under arthroscopy. A minimum 2-year follow-up in 40 patients. Arch Orthop Trauma Surg. 2000;120:128–133. [DOI] [PubMed] [Google Scholar]
- 3. Amis AA, Jakob RP. Anterior cruciate ligament graft positioning, tensioning and twisting. Knee Surg Sports Traumatol Arthrosc. 1998;6(suppl 1):S2–S12. [DOI] [PubMed] [Google Scholar]
- 4. Barrack RL, Buckley SL, Bruckner JD, Kneisl JS, Alexander AH. Partial versus complete acute anterior cruciate ligament tears. The results of nonoperative treatment. J Bone Joint Surg Br. 1990;72:622–624. [DOI] [PubMed] [Google Scholar]
- 5. Bernard M, Hertel P. Intraoperative and postoperative insertion control of anterior cruciate ligament-plasty. A radiologic measuring method (quadrant method). Unfallchirurg. 1996;99:332–340. [PubMed] [Google Scholar]
- 6. Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg. 1997;10:14–21. [PubMed] [Google Scholar]
- 7. Colombet P, Robinson J, Christel P, et al. Morphology of anterior cruciate ligament attachments for anatomic reconstruction: a cadaveric dissection and radiographic study. Arthroscopy. 2006;22:984–992. [DOI] [PubMed] [Google Scholar]
- 8. Diamantopoulos AP, Lorbach O, Paessler HH. Anterior cruciate ligament revision reconstruction: results in 107 patients. Am J Sports Med. 2008;36:851–860. [DOI] [PubMed] [Google Scholar]
- 9. Edwards A, Bull AM, Amis AA. The attachments of the anteromedial and posterolateral fibre bundles of the anterior cruciate ligament. Part 2: femoral attachment. Knee Surg Sports Traumatol Arthrosc. 2008;16:29–36. [DOI] [PubMed] [Google Scholar]
- 10. Fernandes TL, Martins NM, Watai Fde A, Albuquerque C, Jr, Pedrinelli A, Hernandez AJ. 3D computer tomography for measurement of femoral position in ACL reconstruction. Acta Ortop Bras. 2015;23:11–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Forsythe B, Kopf S, Wong AK, et al. The location of femoral and tibial tunnels in anatomic double-bundle anterior cruciate ligament reconstruction analyzed by three-dimensional computed tomography models. J Bone Joint Surg Am. 2010;92:1418–1426. [DOI] [PubMed] [Google Scholar]
- 12. Inderhaug E, Larsen A, Strand T, Waaler PA, Solheim E. The effect of feedback from post-operative 3D CT on placement of femoral tunnels in single-bundle anatomic ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2016;24:154–160. [DOI] [PubMed] [Google Scholar]
- 13. Inoue M, Tokuyasu S, Kuwahara S, et al. Tunnel location in transparent 3-dimensional CT in anatomic double-bundle anterior cruciate ligament reconstruction with the trans-tibial tunnel technique. Knee Surg Sports Traumatol Arthrosc. 2010;18:1176–1183. [DOI] [PubMed] [Google Scholar]
- 14. Iriuchishima T, Ingham SJ, Tajima G, et al. Evaluation of the tunnel placement in the anatomical double-bundle ACL reconstruction: a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2010;18:1226–1231. [DOI] [PubMed] [Google Scholar]
- 15. Jackson DW, Gasser SI. Tibial tunnel placement in ACL reconstruction. Arthroscopy. 1994;10:124–131. [DOI] [PubMed] [Google Scholar]
- 16. Khalfayan EE, Sharkey PF, Alexander AH, Bruckner JD, Bynum EB. The relationship between tunnel placement and clinical results after anterior cruciate ligament reconstruction. Am J Sports Med. 1996;24:335–341. [DOI] [PubMed] [Google Scholar]
- 17. Kim JG, Chang MH, Lim HC, et al. An in vivo 3D computed tomographic analysis of femoral tunnel geometry and aperture morphology between rigid and flexible systems in double-bundle anterior cruciate ligament reconstruction using the transportal technique. Arthroscopy. 2015;31:1318–1329. [DOI] [PubMed] [Google Scholar]
- 18. Koga H, Muneta T, Yagishita K, et al. Effect of femoral tunnel position on graft tension curves and knee stability in anatomic double-bundle anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2014;22:2811–2820. [DOI] [PubMed] [Google Scholar]
- 19. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–174. [PubMed] [Google Scholar]
- 20. Lee BI, Kwon SW, Kim JB, Choi HS, Min KD. Comparison of clinical results according to amount of preserved remnant in arthroscopic anterior cruciate ligament reconstruction using quadrupled hamstring graft. Arthroscopy. 2008;24:560–568. [DOI] [PubMed] [Google Scholar]
- 21. Lee BI, Min KD, Choi HS, et al. Immunohistochemical study of mechanoreceptors in the tibial remnant of the ruptured anterior cruciate ligament in human knees. Knee Surg Sports Traumatol Arthrosc. 2009;17:1095–1101. [DOI] [PubMed] [Google Scholar]
- 22. Lee SR, Jang HW, Lee DW, Nam SW, Ha JK, Kim JG. Evaluation of femoral tunnel positioning using 3-dimensional computed tomography and radiographs after single bundle anterior cruciate ligament reconstruction with modified transtibial technique. Clin Orthop Surg. 2013;5:188–194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Lertwanich P, Martins CA, Asai S, Ingham SJ, Smolinski P, Fu FH. Anterior cruciate ligament tunnel position measurement reliability on 3-dimensional reconstructed computed tomography. Arthroscopy. 2011;27:391–398. [DOI] [PubMed] [Google Scholar]
- 24. Lorenz S, Elser F, Mitterer M, Obst T, Imhoff AB. Radiologic evaluation of the insertion sites of the 2 functional bundles of the anterior cruciate ligament using 3-dimensional computed tomography. Am J Sports Med. 2009;37:2368–2376. [DOI] [PubMed] [Google Scholar]
- 25. Morgan CD, Kalman VR, Grawl DM. Definitive landmarks for reproducible tibial tunnel placement in anterior cruciate ligament reconstruction. Arthroscopy. 1995;11:275–288. [DOI] [PubMed] [Google Scholar]
- 26. Musahl V, Plakseychuk A, VanScyoc A, et al. Varying femoral tunnels between the anatomical footprint and isometric positions: effect on kinematics of the anterior cruciate ligament-reconstructed knee. Am J Sports Med. 2005;33:712–718. [DOI] [PubMed] [Google Scholar]
- 27. Ochi M, Adachi N, Uchio Y, et al. A minimum 2-year follow-up after selective anteromedial or posterolateral bundle anterior cruciate ligament reconstruction. Arthroscopy. 2009;25:117–122. [DOI] [PubMed] [Google Scholar]
- 28. Ochi M, Iwasa J, Uchio Y, Adachi N, Kawasaki K. Induction of somatosensory evoked potentials by mechanical stimulation in reconstructed anterior cruciate ligaments. J Bone Joint Surg Br. 2002;84:761–766. [DOI] [PubMed] [Google Scholar]
- 29. Pietrini SD, Ziegler CG, Anderson CJ, et al. Radiographic landmarks for tunnel positioning in double-bundle ACL reconstructions. Knee Surg Sports Traumatol Arthrosc. 2011;19:792–800. [DOI] [PubMed] [Google Scholar]
- 30. Purnell ML, Larson AI, Clancy W. Anterior cruciate ligament insertions on the tibia and femur and their relationships to critical bony landmarks using high-resolution volume-rendering computed tomography. Am J Sports Med. 2008;36:2083–2090. [DOI] [PubMed] [Google Scholar]
- 31. Rayan F, Nanjayan SK, Quah C, Ramoutar D, Konan S, Haddad FS. Review of evolution of tunnel position in anterior cruciate ligament reconstruction. World J Orthop. 2015;6:252–262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Sinha S, Naik AK, Meena D, Jain VK, Arya RK. Creation of femoral tunnel by outside-in technique for ACL reconstruction: an analysis. Arch Orthop Trauma Surg. 2014;134:1709–1716. [DOI] [PubMed] [Google Scholar]
- 33. Sommer C, Friederich NF, Muller W. Improperly placed anterior cruciate ligament grafts: correlation between radiological parameters and clinical results. Knee Surg Sports Traumatol Arthrosc. 2000;8:207–213. [DOI] [PubMed] [Google Scholar]
- 34. Sonnery-Cottet B, Freychet B, Murphy CG, Pupim BH, Thaunat M. Anterior cruciate ligament reconstruction and preservation: the single-anteromedial bundle biological augmentation (SAMBBA) technique. Arthrosc Tech. 2014;3:e689–e693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Sonnery-Cottet B, Lavoie F, Ogassawara R, Scussiato RG, Kidder JF, Chambat P. Selective anteromedial bundle reconstruction in partial ACL tears: a series of 36 patients with mean 24 months follow-up. Knee Surg Sports Traumatol Arthrosc. 2010;18:47–51. [DOI] [PubMed] [Google Scholar]
- 36. Staubli HU, Rauschning W. Tibial attachment area of the anterior cruciate ligament in the extended knee position. Anatomy and cryosections in vitro complemented by magnetic resonance arthrography in vivo. Knee Surg Sports Traumatol Arthrosc. 1994;2:138–146. [DOI] [PubMed] [Google Scholar]
- 37. Sudhahar TA, Glasgow MM, Donell ST. Comparison of expected vs. actual tunnel position in anterior cruciate ligament reconstruction. Knee. 2004;11:15–18. [DOI] [PubMed] [Google Scholar]
- 38. Sutter EG, Anderson JA, Garrett WE., Jr Direct visualization of existing footprint and outside-in drilling of the femoral tunnel in anterior cruciate ligament reconstruction in the knee. Arthrosc Tech. 2015;4:e107–e113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Takahashi M, Doi M, Abe M, Suzuki D, Nagano A. Anatomical study of the femoral and tibial insertions of the anteromedial and posterolateral bundles of human anterior cruciate ligament. Am J Sports Med. 2006;34:787–792. [DOI] [PubMed] [Google Scholar]
- 40. Takazawa Y, Ikeda H, Kawasaki T, et al. ACL reconstruction preserving the ACL remnant achieves good clinical outcomes and can reduce subsequent graft rupture. Orthop J Sports Med. 2013;1:2325967113505076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Tsukada H, Ishibashi Y, Tsuda E, Fukuda A, Toh S. Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints. J Orthop Sci. 2008;13:122–129.18392916 [Google Scholar]
- 42. van Eck CF, Schreiber VM, Mejia HA, et al. “Anatomic” anterior cruciate ligament reconstruction: a systematic review of surgical techniques and reporting of surgical data. Arthroscopy. 2010;26(suppl 9):S2–S12. [DOI] [PubMed] [Google Scholar]
- 43. Xu H, Zhang C, Zhang Q, et al. A systematic review of anterior cruciate ligament femoral footprint location evaluated by quadrant method for single-bundle and double-bundle anatomic reconstruction. Arthroscopy. 2016;32:1724–1734. [DOI] [PubMed] [Google Scholar]
- 44. Yamamoto Y, Hsu WH, Woo SL, Van Scyoc AH, Takakura Y, Debski RE. Knee stability and graft function after anterior cruciate ligament reconstruction: a comparison of a lateral and an anatomical femoral tunnel placement. Am J Sports Med. 2004;32:1825–1832. [DOI] [PubMed] [Google Scholar]
- 45. Yasuda K, Kondo E, Ichiyama H, et al. Anatomic reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament using hamstring tendon grafts. Arthroscopy. 2004;20:1015–1025. [DOI] [PubMed] [Google Scholar]
- 46. Zantop T, Diermann N, Schumacher T, Schanz S, Fu FH, Petersen W. Anatomical and nonanatomical double-bundle anterior cruciate ligament reconstruction: importance of femoral tunnel location on knee kinematics. Am J Sports Med. 2008;36:678–685. [DOI] [PubMed] [Google Scholar]
- 47. Zantop T, Herbort M, Raschke MJ, Fu FH, Petersen W. The role of the anteromedial and posterolateral bundles of the anterior cruciate ligament in anterior tibial translation and internal rotation. Am J Sports Med. 2007;35:223–227. [DOI] [PubMed] [Google Scholar]
- 48. Zantop T, Petersen W. Double bundle revision of a malplaced single bundle vertical ACL reconstruction: ACL revision surgery using a two femoral tunnel technique. Arch Orthop Trauma Surg. 2008;128:1287–1294. [DOI] [PubMed] [Google Scholar]
- 49. Zantop T, Wellmann M, Fu FH, Petersen W. Tunnel positioning of anteromedial and posterolateral bundles in anatomic anterior cruciate ligament reconstruction: anatomic and radiographic findings. Am J Sports Med. 2008;36:65–72. [DOI] [PubMed] [Google Scholar]
- 50. Zavras TD, Race A, Amis AA. The effect of femoral attachment location on anterior cruciate ligament reconstruction: graft tension patterns and restoration of normal anterior-posterior laxity patterns. Knee Surg Sports Traumatol Arthrosc. 2005;13:92–100. [DOI] [PubMed] [Google Scholar]