

Introduction
Colorectal cancer is one of the most common cancers in industrialized nations. Its incidence has increased significantly over the last 30 years and it represents the second most common cancer-related cause of death. The extent of lymph node and haematogenous spread correlates with local depth of invasion. For haematogenous spread, the liver is the primary target organ, followed by the lungs and bone. Singular haematogenous spread to the kidneys is rare. We report the very unusual case of a woman 8 years after surgical treatment for colon cancer who presented with a renal tumour that turned out to be a colon cancer metastasis that had grown into the kidney via ureteral spread.
Case report
An 81-year-old woman was referred for surgical treatment after a CT scan had shown a renal tumour (16 cm × 12 cm × 8 cm) in a non-functioning left kidney (Figure 1). Eight years previously, the patient had undergone a left hemicolectomy and partial cystectomy for a colorectal carcinoma of the sigmoid colon (pT3 pN1 L0 V1 R0 cM0). Despite a lymph node positive situation at the time the patient had refused adjuvant treatment and did not undergo follow-up.
Figure 1.

CT scan showing large left inhomogeneous renal mass (16 cm × 12 cm × 8 cm, HU 10–15).
The now diagnosed renal tumour had been seen on a CT scan performed when the patient presented with acute symptoms of an ileus. The ileus was successfully managed conservatively. Physical examination was normal, clinical chemistry likewise including the carcinoembryonic antigen (CEA) level. The CT findings reported by radiology suggested a large, primary renal tumour consistent with a locally advanced renal cell carcinoma.
The patient was referred to urology and underwent surgery for the kidney tumour of presumably renal origin. Macroscopically, the tumour was solid, clearly delineated and its appearance consistent with a renal transitional cell carcinoma so that intraoperatively surgery was extended to include complete ureterectomy in addition to radical nephrectomy. The postoperative course was uneventful.
However, histology showed the renal tumour to be the metastasis of a tubular adenocarcinoma (G2) of colonic origin, with several smaller metastases detected in the left ureter (Figure 2). The tumour tissue was positive for CK20 and negative for CK7, with PAS-positive intracytoplasmic inclusions. Surgical margins were negative. Endoscopic examinations of the urinary bladder and the colon were normal.
Figure 2.
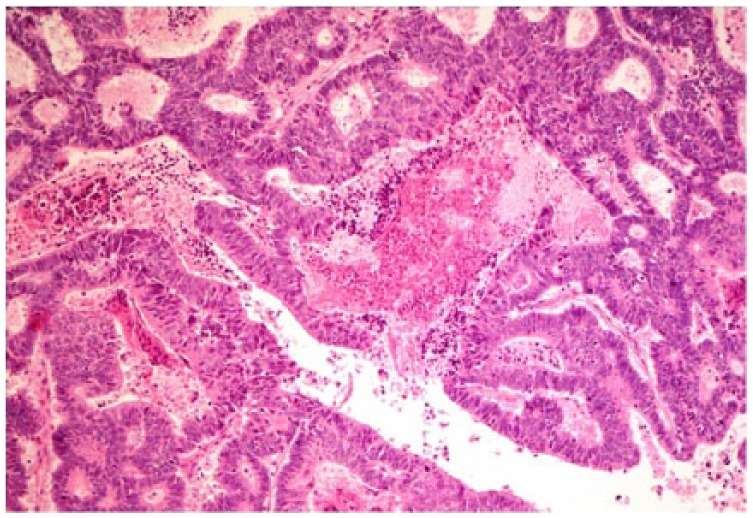
Cribriform adenocarcinoma with focal necrosis consistent with a metastasis of known colorectal cancer. Haematoxylin and eosin; original magnification 100×.
One year later the patient presented with bleeding from the colostomy and left leg oedema. Coloscopy showed a partially necrotic tumour 10 cm from the stoma and on CT scan a large retroperitoneal tumour mass was seen, surrounding the left pelvic vascular axis with thrombotic occlusion of the external iliac vein, infiltration of the psoas muscle and adherence to the small bowel. The patient did not want any further treatment.
Comment
This case shows the highly unusual finding of an adenocarcinoma of the sigmoid colon that had infiltrated the urinary bladder at the time of primary surgical treatment recurring 8 years later with spread by continuity via the ureter into the left kidney. This has hitherto not been described in the literature.
Metastases to the kidney are a rare entity. Based on autopsy studies, the incidence of renal metastases of solid organ tumours amounts to 3–15%.1–4 These arise from the lungs (19.8–23.3%), the breast (12.3%), stomach (11.1–15.1%), colon (22.2%) and malignant melanoma (14.8%),5 and less frequently from the cervix, gallbladder, urinary bladder, prostate, thyroid, hypopharynx, ovary, testis and the contralateral kidney.3 In the majority of cases, solitary renal metastases from colorectal carcinoma are asymptomatic and detected on surveillance imaging or as a result of increased CEA levels.6 Survival appears to be longer in patients who are treated by surgery. Surgical intervention in carefully selected patients with oligometastatic disease and good performance status should therefore be considered.7,8 However, systemic chemotherapy is the treatment of choice for metastatic colorectal carcinoma and nephrectomy is not commonly used in the management of renal metastases from colorectal cancer.6,8,9
The metastatic pathway in such cases is usually by haematogenous spread. Therefore, this case is quite remarkable and very rare as the spread occurred by direct intraureteric growth.
In conclusion, isolated renal metastases of colorectal carcinoma have rarely been reported in the literature (<20 cases) and no case has been reported so far illustrating intraureteric spread to the kidney.
Footnotes
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement: The authors declare that there is no conflict of interest.
Contributor Information
Désirée Louise Dräger, Department of Urology, University of Rostock, Ernst-Heydemann-Str. 6, 18057 Rostock, Germany.
Chris Protzel, Department of Urology, University of Rostock, Germany.
Andreas Erbersdobler, Institute of Pathology, University of Rostock, Germany.
Oliver Hakenberg, Department of Urology, University of Rostock, Germany.
References
- 1. Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma; analysis of 1000 autopsied cases. Cancer 1950; 3: 74–85. [DOI] [PubMed] [Google Scholar]
- 2. Bracken RB, Chica G, Johnson DE, et al. Secondary renal neoplasms: an autopsy study. South Med J 1979; 72: 806–807. [DOI] [PubMed] [Google Scholar]
- 3. Mayer RJ. Infiltrative and metastatic disease of the kidney. In Rieselbach RE, Garnick MB. (eds) Cancer and the kidney. Philadelphia: Lea & Febiger, 1982, p. 707. [Google Scholar]
- 4. Sánchez-Ortiz RF, Madsen LT, Bermejo CE, et al. A renal mass in the setting of a nonrenal malignancy: when is a renal tumor biopsy appropriate? Cancer 2004; 101: 2195–2201. [DOI] [PubMed] [Google Scholar]
- 5. Wagle DG, Moore RH, Murphy GP. Secondary carcinomas of the kidney. J Urol 1975; 114: 30–32. [DOI] [PubMed] [Google Scholar]
- 6. Dulskas A, Bagurskas P, Sinkevicius Z, et al. Sigmoid adenocarcinoma with metastases to the kidney: report of a rare case and review of the literature. Oncol Lett 2015; 10(2): 1191–1193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Zhou C, Urbauer DL, Fellman BM, et al. Metastases to the kidney: a comprehensive analysis of 151 patients from a tertiary referral centre. BJU Int 2016; 117(5): 775–782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Melichar B, Morávek P, Ferko A, et al. Metastatic colorectal carcinoma and kidney tumors: a report of four cases. Tumori 2010; 96(3): 483–486. [DOI] [PubMed] [Google Scholar]
- 9. Dagnoni C, Granero LCS, Rovere RK. Sigmoid adenocarcinoma with renal metastasis. Clin Pract 2011; 1: e88. [DOI] [PMC free article] [PubMed] [Google Scholar]