

Abstract
Background
According to the projections of the World Health Organization, 15% of all disabilities will be associated with mental illnesses by 2020. One of the mental disorders with the largest social impacts due to high personal and family costs is psychosis. Among the most effective psychological approaches to treat schizophrenia and other psychotic disorders at the world level is cognitive behavioral therapy. Recently, cognitive behavioral therapy has introduced several tools and strategies that promote psychological processes based on acceptance and mindfulness. A large number of studies support the effectiveness of mindfulness in dealing with various mental health problems, including psychosis. This study is aimed at determining the efficiency of a mindfulness-based program in increasing cognitive function and psychological well-being in patients with a first episode of schizophrenia and a high risk mental state (those at risk of developing an episode of psychosis).
Methods and design
This is an experimentally designed, multi-center randomized controlled trial, with a 3-month follow-up period. The study participants will be 48 patients diagnosed with schizophrenia (first episode) and 48 with a high-risk mental state, from Santiago, Chile, aged between 15 and 35 years. Participants will be submitted to a mindfulness-based intervention (MBI), which will involve taking part in eight mindfulness workshops adapted for people with psychosis. Workshops will last approximately 1.5 hours and take place once a week, over 8 weeks. The primary outcome will be the cognitive function through Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) and the secondary outcome will be psychological well-being measured by self-reporting questionnaires.
Discussion
The outcomes of this trial will add empirical evidence to the benefits and feasibility of MBIs for the psychotherapeutic treatment of patients with schizophrenia and high-risk mental states in reducing cognitive impairment in attention, working memory, and social cognition, as well as increasing the psychological well-being by empowering the patients’ personal resources in the management of their own symptoms and psychotic experiences.
Trial registration
ISRCTN registration number ISRCTN24327446. Registered on 12 September 2016.
Electronic supplementary material
The online version of this article (doi:10.1186/s13063-017-1967-7) contains supplementary material, which is available to authorized users.
Keywords: Mindfulness, Schizophrenia, High-risk mental state, Cognitive functions, Psychological well-being
Background
According to projections of the World Health Organization, 15% of all human disabilities will be associated with mental illnesses by 2020 [1]. One of the mental disorders with the largest social impacts due to high personal and family costs is psychosis, particularly schizophrenia [2]. At present, national and international clinical guidelines suggest favoring an intervention approach that aims to minimize the time an individual is without treatment and to continue treatment during all the phases of the illness. This has led several countries to modify their public policies towards an early intervention of the disorder. Evidence suggests a better prognosis for patients with a lower duration of untreated psychosis [3, 4].
Early intervention not only focuses on the first psychotic episode but also in premorbid states, characterized by subclinical signs and symptoms and with specific features, including delusional beliefs, attenuated hallucinations, and disorganized speech with intact reality testing but of sufficient severity and/or frequency that it is not discounted or ignored. Additionally, symptoms should have worsened in the past year with sufficient clinical discomfort for the affected patients or their relatives to pursue specialized help. Such attenuated symptoms have been characterized as a high-risk mental state for psychosis, collected by DSM-5 to be studied as an Attenuated Psychosis Symptom Syndrome [5]. While not all individuals who experience a high-risk mental state derive into a psychosis, all those with schizophrenia showed a high-risk premorbid state. Therefore, it is extremely relevant to determine the factors that effectively predict a transition towards psychosis [6].
Several countries, including the United Kingdom, Australia, or Canada, to name a few, have included early intervention as a core approach to address schizophrenia. In Chile, its treatment has been a public policy priority. As a matter of fact, first-episode schizophrenia is the first mental health condition included in the Explicit Health Care Guarantees. Clinical guidelines suggest an integral approach, i.e., one that considers the psychosocial and pharmacological dimensions. Among the psychosocial interventions with the best results in addressing schizophrenia and other psychotic disorders at the world level is cognitive behavioral therapy. Recently, cognitive behavioral therapy has introduced several tools and strategies that promote psychological processes based on acceptance and mindfulness [7].
Mindfulness-based interventions (MBIs)
Mindfulness is a research area in psychology that has experienced the greatest development in recent years. These interventions include acceptance and commitment therapy (ACT), mindfulness-based cognitive therapy, mindfulness-based stress reduction therapy, or dialectical behavior therapy. This set of procedures shares the basic notion that, in order to achieve adequate psychological functioning, individuals should change the way in which they relate to their symptoms instead of eliminating them [8]. Recently, these interventions have been grouped under the label of third wave cognitive behavioral therapies [9]. ACT and MBIs are among the third wave therapies used efficiently in psychosis.
Mindfulness can be understood as a specific form of meditation that seeks to increase different psychological functions by means of a synergic effort between attention regulation, self-awareness and emotional regulation, thereby increasing psychological resilience and self-regulation [10]. Mindfulness has been defined as, “Paying attention in a particular way: on purpose, in the present moment, and non-judgmentally” [11]. It has also been conceptualized as a theoretical construction, as a practice and as a psychological process [12]. Training in mindfulness from a Western and academic standpoint has been developed and disseminated through standardized group programs lasting from 8 to 10 weeks and in clinical and health contexts [8, 13].
Such approaches rely on broad empirical support. In fact, recent meta-analyses suggest that mindfulness is an effective intervention for the treatment of several mental health disorders, including depression and anxiety [14, 15]. However, one recent meta-analysis revealed that ACTs and MBIs show promising results in the management of positive and negative symptoms of psychosis [16].
Specifically, the first study of mindfulness in psychosis was conducted in the United Kingdom with patients who suffered stress-induced hallucinations. Patients attended to six mindfulness sessions. The outcomes of this non-controlled study revealed an increase of mindfulness skills in the management of stress-causing thoughts and images. Additionally, the perception regarding the psychological well-being of patients had improved [17]. On the other hand, Chadwick et al. [17] suggested a series of changes to the MBIs when used in psychotic patients in order to ensure the procedure’s feasibility in this population group. Subsequently, Chadwick et al. [18] performed the first controlled study assessing mindfulness skills and overall patient functioning. Both measures improved in the expected direction and showed significant outcomes in intra-group comparisons, but did not do better than the control group. The second controlled clinical trial was conducted in Spain with a small sample of psychotic patients [19], and revealed that, when patients increased their acceptance rates, they also had a less stressing relationship with their thoughts and emotions, in addition to improvements in overall functioning; however, only the first outcome was statistically significant compared to the control group. Another more solid study in terms of the number of participants (N = 98) and the introduction of follow-up measures (18 months) was performed by Lee and Chien [20]. The outcomes of their study revealed that patients showed improved levels of illness insights and overall functioning, and a reduction in symptom severity and in the number and length of hospitalizations. All of these indicators were statistically significant compared to the control group (usual treatment). Recent studies have confirmed the results mentioned above [21, 22]. Other non-controlled studies have proven the feasibility of using mindfulness in patients with psychosis [23–25].
On the other hand, several qualitative studies have revealed that practicing mindfulness results in a less stressful relationship between patients and their symptoms, with greater flexibility and control over them. This change has a direct impact on the way in which a person relates both to others and to themselves, increasing their confidence and the sense of self-agency. In other words, a person gains an active role in the way they face their symptoms and life, strengthening a self-image that is not only centered around the absence or presence of psychotic symptoms but on their personal resources as the main focus of recovery [26–28].
Considering all the research in this area, i.e., more than 20 studies including randomized, non-controlled, qualitative, and single case clinical trials [29], two aspects can be pinpointed concerning the use of mindfulness in psychosis. Firstly, that mindfulness reduces the stress associated to psychotic symptoms and thereby promotes patient recovery and, secondly, its implementation in clinical centers is both safe and viable.
The relevance of the mindfulness study in cognitive functions and psychological well-being
Mindfulness and cognitive functions
Cognitive impairments have been described as a core element of schizophrenia; indeed, 90% of patients have difficulties in this area [30, 31]. What is relevant is that these impairments are found before the onset of schizophrenia, which suggests that they are not a consequence of the illness but rather a vulnerability factor for schizophrenia [32] and a functionality predictor in patients [33]. Cognitive functions subject to the greatest decline in the transition from a high-risk mental state to a first psychotic episode are working memory [34], attention [35], and social cognition [36]. For instance, working memory has been defined as the most solid indicator in the transition between a high-risk mental state and schizophrenia. On the other hand, improvements in attention could be a remission indicator in high-risk people with schizophrenia [35], while the reduction of social cognition skills have been related to the length and severity of symptoms [37].
The control of attention in mindfulness is one of the pillars to achieve improved psychological flexibility and therefore greater response options facing adverse stimuli. In fact, expert meditators score higher in attention tests than non-meditators or beginners [38]. On the other hand, working memory has been related to other cognitive domains that are impaired in schizophrenia, such as attention and planning [39], and other executive functions, including inhibitory control and mental flexibility [40]. As background information, while mindfulness has a major impact on working memory [41, 42], this impact depends on the time devoted to meditation, being greater in people who meditate regularly compared to beginners [42, 43]. Similarly, working memory has been related to social cognition [44]. For instance, the cognitive training of working memory improves social perception in patients with schizophrenia [45].
Mindfulness and its impact on psychological well-being
Psychological well-being is a key area in the current conception of health [1]. In other words, it is not only the absence or reduction of symptoms that matters in the treatment of severe mental disorders such as schizophrenia [46]. The concept of mental health recovery notes that people should lead a purposeful and meaningful life, regardless of whether they have a mental disorder. However, a review study concluded that only a very small amount of interventions have proven effective in improving the psychological well-being of patients with schizophrenia [47]. Numerous studies, however, emphasize the favorable impacts of mindfulness, among them a reduction of symptoms and, above all, the development of a more favorable way of relating to own experience, with greater presence and acceptance, thereby promoting the sense of self-empowerment and improving a broader self-image not exclusively focused on the presence or absence of symptoms [21, 28]. In this sense, focusing attention on own feelings and managing them is related to improved emotional intelligence, also a very important aspect in the social sphere [48, 49]. An increase in the aspects mentioned above is among the main findings of qualitative research concerning mindfulness in psychosis [31]. It should be noted that this project understands psychological well-being from two perspectives. The first refers to a positive dimension which aims at increasing positive emotions and more flexible psychological states (mindfulness), while the second refers to a symptomatic sphere where a less aversive relationship with private events is expected and thus a reduction in psychological discomfort [46].
The purpose of this study is to determine how efficient MBIs can be in increasing cognitive functions and psychological well-being in patients with a first episode of schizophrenia and patients in a high-risk mental state, and thus define the scope of mindfulness to increase these areas of functioning. The specific goals are to (1) determine how efficient a mindfulness intervention can be in increasing attention, working memory, and social cognition rates, compared with the control group; (2) establish which spheres of psychological well-being increase (positive dimension) and which decrease (symptomatic dimension) with mindfulness training, compared to the control group; (3) determine whether the expected outcomes (increased cognitive functions and psychological well-being) are still present 3 months after the intervention has finalized, and additionally establish whether impacts are greater in participants who continue practicing mindfulness compared to those who fail to continue the practice; and (4) describe, on the one side, the subjective experience of patients regarding the feasibility of implementing such an intervention in a local context and, on the other, the benefits of mindfulness for patients compared to other psychosocial interventions in the context of mental health public policies in Chile.
The hypotheses are as follows. (1) MBIs will increase executive functions. Specifically, a statistically significant increase is expected in attention, working memory, and social cognition rates compared to the control group. (2) Subjective psychological well-being rates will increase significantly in the mindfulness group compared to the control group. (3) The outcomes in the areas described will persist 3 months after; however, impacts will be greater on people who continue practicing mindfulness compared to those who do not.
The questions that guide the qualitative goals are as follows. (1) What were the benefits and shortcomings found during the workshop? (2) Do patients continue with this practice and mainstream the outcomes into other areas of their lives? (3) What differences and similarities are perceived by patients between mindfulness and traditional psychosocial interventions?
Methods and design
This is a multi-center randomized controlled trial (RCT) with two parallel arms and 1:1 allocation. A mixed analysis approach will be used. To assess the RCT’s effectiveness, a quantitative method will be used, while a qualitative approach will help understand subjective change processes considering cultural traits.
Participants
Patients will be recruited from six clinical centers from three different cities in Chile; four in Santiago, one in Valdivia, and one in Osorno. Ninety six people are expected to take part in the study, of which 48 will be patients diagnosed with a first episode of schizophrenia (divided into 24 trial and 24 controls) based on the following criteria: patients with a psychotic episode without a prior diagnostic of schizophrenia, patients diagnosed with schizophrenia for the first time, and/or patients who persist with the schizophrenia diagnosis after the first episode. Additionally considered is the participation of 48 patients under a high-risk mental state (divided into 24 trial and 24 controls) who meet the criteria of an Attenuated Psychosis Symptom Syndrome, including delusional beliefs, attenuated hallucinations, and disorganized speech with intact reality testing but of sufficient severity and/or frequency that it is not discounted or ignored [5]. Sample size was estimated considering a previous RCT for people with schizophrenia on both the MBI [20] and a cognitive remediation program [50]. The sample size was calculated by using the statistical program G*Power [51]. The sample required to detect statistically significant differences in the cognitive functioning for a two-tailed test of the proportions with an effect size of 0.80, an alpha of 0.05, and a power of 0.90 is 2 × 39. With an estimated 15–20% drop-out over 3 months, we decided to include 96 persons in the trial, 48 allocated in each intervention arm. The inclusion criteria are (1) patients diagnosed with a first episode of schizophrenia or in high-risk of psychosis, as applicable; (2) aged between 15 and 35 years; and (3) clinical stability defined by medical and psychometric criteria (e.g., PAANS). Exclusion criteria are (1) risk of suicide; (2) severe intellectual disability (mental retardation); (3) medical illness inconsistent with the intervention; and (4) substance abuse or dependence in the past 6 months. Figures 1 and 2 summarize the process of randomization, group allocation, and assessment. The SPIRIT checklist is available in Additional file 1.
Fig. 1.
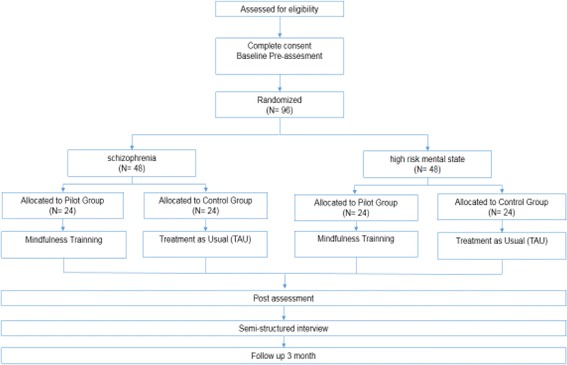
This figure illustrates the process of randomization, allocation assessment, and follow-up throughout the study
Fig. 2.
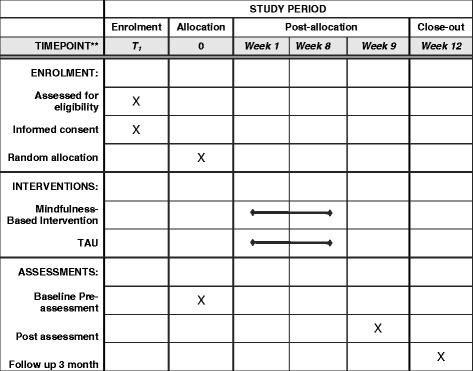
Schedule of enrollment, intervention, and assessments for the mindfulness-based intervention
Procedure
Participants, as defined above, will be randomly allocated (a simple randomized sampling will be used) to the trial or control group. Randomization to either trial or treatment as usual will be conducted by independent researchers using a stratified block randomization procedure with a computer-generated allocation sequence. Health experts who will implement the MBIs will be blind to this procedure and will not carry out the assessment.
Intervention group
Participants will be provided with the MBI, plus treatment as usual, divided into 24 patients diagnosed with a first episode of schizophrenia and 24 patients in a high-risk mental state (groups do not include both profiles). This means that both groups will be submitted to eight sessions of mindfulness workshops adapted for patients with psychosis [17]. The proposed duration for each session is 1 hour and a half, once a week. The intervention will take place in the facilities of each participating clinical center and led by a mindfulness coach with specific training in the target audience. The main project researcher will supervise and train each coach in the application of mindfulness in psychosis. The workshop includes take-home exercises. Additionally, every participant will get a pen drive or CD with guided mindfulness practice audios and a booklet with the contents of each session. Groups will be composed of up to eight members and two workshops have been planned by every participating institution.
Control group
Participants will receive standard care for this illness (treatment as usual), in other words, pharmacology and psychosocial intervention under clinical guidelines (e.g., social skills workshop).
The assessment, application of neuropsychological tests (Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) Battery), and self-reporting questionnaires will take place (1) before the workshop; (2) after the workshop; and (3) at follow-up 3 months after completing the workshop. Additionally, 4 weeks after completing the workshop, participants will be submitted to semi-structured interviews. The number of interviews will be defined based on the saturation of the concepts found in the qualitative methodology. Each interview will last approximately 20 minutes and will be performed by a member of the research team.
Measuring instruments
Primary outcome
The primary outcome will be the cognitive function through MATRICS. This battery assesses seven functioning areas, namely speed of processing, attention/vigilance, working memory, verbal learning, visual learning, reasoning and problem solving, and social cognition. The assessment takes place through seven tests.
Secondary outcomes
Psychological well-being/positive dimension (increase)
The following instruments will be used to assess the psychological well-being in its positive dimension:
Psychological well-being scale [52, 53], which includes 39 items grouped in six subscales: self-acceptance, positive relations with others, autonomy, environmental mastery, purpose in life, and personal growth. Respondents answer in the Likert scale format with a range from 1 to 6 (1 = strong disagreement and 6 = strong agreement). This scale has been broadly studied to assess psychological well-being. The version validated in Chile and published by Véliz-Burgos will be used [54].
Self-esteem scale by Rosenberg. This is a 10-item scale broadly used in research. It is a uni-dimensional instrument answered with a Likert scale of four options, ranging from “strongly agree” to “strongly disagree”. The Chilean version showed adequate psychometric properties [55].
Five Facet Mindfulness Questionnaire [56], which is a self-reporting questionnaire that describes mindfulness operationally as a multidimensional construction, built on the following five facets: observing, describing, acting with awareness, non-judging of experiences, and non-reactivity to experience. The questionnaire uses a Likert scale ranging from 1 (never or very rarely true) to 5 (very often or always true). It presents adequate psychometric properties in the Chilean population [57].
Psychological well-being/symptomatology dimension (reduction)
The following instruments will be used to measure the symptomatic dimensions of psychological well-being:
Positive and Negative Affect Schedule (PANAS) [58], which is a 20-item scale including by 10 items that assess positive affect and 10 items that assess negative affect. Items are formed by words that describe different feelings and emotions. The Chilean version published by Dufey and Fernández will be used [59].
Penn State Worry Questionnaire (PSWQ-11) [60], which is a measure of worry phenomena designed to assess the general trends when experiencing worry. It is composed by 16 items to which participants respond in a 5-score Likert scale, ranging from 1 “not at all typical of me” to 5 “very typical of me”. The Spanish version of Sandin, Chorot, Valiente and Lostao will be used, which has shown to have adequate psychometric properties [61].
Depression, Anxiety and Stress Scale (DASS-21) [62]. This is a self-applied scale that assesses general symptoms in three dimensions. Seven items are related to depression symptoms, seven to anxiety symptoms, and seven to stress. The scale has been validated in Chile with good psychometric properties [63].
Data analysis
A mixed qualitative and quantitative analysis method will be used. Qualitative information will be collected by means of semi-structured interviews and assessed with the Grounded Theory. This data analysis approach is widely used in social sciences and was previously applied for the analysis of the subjective experience of patients with psychosis [26]. This methodology will analyze the patients’ subjective experience regarding the feasibility and contribution of this type of intervention in a local context. At the quantitative level, the hypothesis will be contrasted though a mixed designed ANOVA in order to consider both the impacts of the intervention (inter subjects) and time (intra-subject; pre, post, and follow-up measurements) in every variable assessed. The analysis will help prove the hypotheses regarding the efficiency of this intervention in both patient groups. If statistically significant differences are found between the trial and control groups at the beginning of the intervention, corrections will be conducted using an ANCOVA.
Ethics
The research protocol follows the indications of the Singapore Statement on Research Integrity and has been approved by two ethics committees, namely Pontificia Universidad Católica de Chile and Universidad de Chile.
Discussion
Schizophrenia is a chronic and severe mental health disorder. In Chile, it is a public health priority subject to integral treatment indications (pharmacological and psychosocial). There is abundant empirical evidence suggesting that MBIs are feasible and beneficial interventions for patients with schizophrenia. MBIs promote a more flexible relationship with the psychotic symptoms, with impacts on the patients self-awareness and own resources and not only on the shortcomings and limitations of having a chronic mental illness [7, 16, 29]. However, one of the elusive areas in targeting these psychotherapeutic treatments are cognitive impairments [7], while an adequate cognitive functioning has clear impacts on the psychological well-being of patients [64].
All the scientific evidence points to the need to study the relationship suggested in this project, i.e., to determine the impact of mindfulness on cognitive functions and the psychological well-being in people with schizophrenia. However, it is also worthwhile to include people with a high-risk mental state since this could provide insights in several areas, including (1) proving the efficacy of the MBI intervention for this group; (2) comparing the outcomes with those of patients with a first episode of schizophrenia (i.e., determine the scope of mindfulness according to the pathology level); and (3) allow subjective assessment of the mindfulness benefits according to patient experience when facing a reduction in psychological discomfort.
Thus, this study aims, on the one hand, to discuss different aspects that have not yet been addressed in the literature concerning MBIs applied in psychosis and, on the other, to confirm previous findings in other social and cultural contexts so as to improve the ecological soundness of this intervention [28]. In addition, the insights provided by self-reporting studies need to be improved through more accurate measurements such as neuropsychological tests.
Should the hypotheses suggested in this study be proven, this would add empirical evidence about the benefits and feasibility of MBIs for the psychotherapeutic treatment of patients with schizophrenia as well as of those with a high-risk mental state in reducing cognitive impairments in attention, working memory, and social cognition. The results would also increase the psychological well-being by empowering patients’ personal resources in the management of their own symptoms and psychotic experiences.
Trial status
The research is presently in the sample recruitment phase and the workshops are expected to begin on November 15, 2016.
Additional files
SPIRIT checklist. (DOC 121 kb)
Acknowledgements
We thank the Chilean National Fund for Scientific and Technological Development, FONDECYT (project N° 11150846) for funding this project.
Funding
This project is funded by the Chilean National Fund for Scientific and Technological Development, FONDECYT (project N° 11150846), and supported by FONDECYT N° 11140464 P.I. Gaspar PA and the Fund for Innovation and Competitiveness (FIC) of the Chilean Ministry of Economy, Development, and Tourism, through the Millennium Scientific Initiative, grant no. IS130005.
Availability of data and materials
Not applicable.
Authors’ contributions
AIL conceived the original idea of the study and was involved in drafting the manuscript, managing and advising the project. PAG participated in design and feedback for the final version. AP, MJV, AM, and PAG provided support in coordinating the project with the clinical centers. RM is clinical coordinator. CS is clinical coordinator and helped to draft the manuscript. GV and BPH made substantial contributions to the conception of the study. MD, JL, EK, and CV will act as monitors and will be running workshops. All authors read and approved the final manuscript.
Authors’ information
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Full ethical approval was obtained from the local Ethics Committees.
1. Scientific Ethical Committee for Social Sciences, Arts and Humanities. Approval Minutes No. 21, November 18, 2015. Pontificia Universidad Católica de Chile. The ethics committee also approved letter of Informer Assent and Consent Informer.
2. Scientific and Research Ethics Committee of the Clinical Hospital of University of Chile. Approval Minutes No. 32, June 29, 2016. University of Chile.
This study protocol is in compliance with the Helsinki Declaration. In addition, informed and written consent will be obtained from the participants.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- ACT
Acceptance and commitment therapy
- MATRICS
Measurement and Treatment Research to Improve Cognition in Schizophrenia
- MBI
Mindfulness-based intervention
- RCT
Randomized controlled trial
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1186/s13063-017-1967-7) contains supplementary material, which is available to authorized users.
Contributor Information
Álvaro I. Langer, Email: alvaro.langer@uach.cl
Carlos Schmidt, Email: vicenteschmidt@gmail.com.
Rocío Mayol, Email: rociomayolt@gmail.com.
Marcela Díaz, Email: marcedipro@gmail.com.
Javiera Lecaros, Email: javieralecarosb@gmail.com.
Edwin Krogh, Email: edwinkrogh@gmail.com.
Aída Pardow, Email: apardow@redgesam.cl.
Carolina Vergara, Email: carolivergara@gmail.com.
Guillermo Vergara, Email: gvergara@redgesam.cl.
Bernardita Pérez-Herrera, Email: bernardita.perez.herrera@gmail.com.
María José Villar, Email: cotevillar@gmail.com.
Alejandro Maturana, Email: almaturana@vtr.net.
Pablo A. Gaspar, Email: pablo.gaspar@gmail.com
References
- 1.World Health Organization . Promoting Mental Health. Concepts, Emerging Evidence, Practice. Geneva: WHO; 2004. [Google Scholar]
- 2.Mortensen PB, Pedersen CB, Westergaard T, Wohlfahrt J, Ewald H, Mors O, Andersen PK, Melbye M. Effects of family history and place and season of birth on the risk of schizophrenia. N Engl J Med. 2009;340:603–8. doi: 10.1056/NEJM199902253400803. [DOI] [PubMed] [Google Scholar]
- 3.Boonstra N, Klaassen R, Sytema S, Marshall M, De Haan L, Wunderink L, Wiersma D. Duration of untreated psychosis and negative symptoms--a systematic review and meta-analysis of individual patient data. Schizophr Res. 2012;142:12–9. doi: 10.1016/j.schres.2012.08.017. [DOI] [PubMed] [Google Scholar]
- 4.Marshall M, Lewis S, Lockwood A, Drake R, Jones P, Croudace T. Association between duration of untreated psychosis and outcome in cohorts of first-episode patients: a systematic review. Arch Gen Psychatry. 2005;62:975–83. doi: 10.1001/archpsyc.62.9.975. [DOI] [PubMed] [Google Scholar]
- 5.American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5. Washington: APA; 2013. [Google Scholar]
- 6.Fusar-Poli P, Borgwardt S, Bechdolf A, Addington J, Riecher-Rössler A, Schultze-Lutter F, et al. The psychosis high-risk state: a comprehensive state-of-the-art review. JAMA Psychiatry. 2013;70:107–20. doi: 10.1001/jamapsychiatry.2013.269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gaudiano BA. Incorporating Acceptance and Mindfulness into the Treatment of Psychosis: Current Trends and Future Directions. Oxford: Oxford Press; 2015. [Google Scholar]
- 8.Segal Z, Williams J, Teasdale J. Mindfulness Based Cognitive Therapy for Depression. New York: Guilford Press; 2002. [Google Scholar]
- 9.Hayes SC. Acceptance and commitment therapy, relational frame theory and the third wave of behavioral and cognitive therapies. Behav Ther. 2004;35:639–65. doi: 10.1016/S0005-7894(04)80013-3. [DOI] [PubMed] [Google Scholar]
- 10.Tang Y, Hölzel BK, Posner MI. The neuroscience of mindfulness meditation. Neuroscience Scie. 2015;16:213–25. doi: 10.1038/nrn3916. [DOI] [PubMed] [Google Scholar]
- 11.Kabat-Zinn J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life. New York: Hyperion; 1994. [Google Scholar]
- 12.Germer C, Siegel R, Fulton P. Mindfulness and Psychotherapy. New York: Guilford Press; 2005. [Google Scholar]
- 13.Kabat-Zinn J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain and Illness. New York: Hyperion; 1990. [Google Scholar]
- 14.Fjorback LO, Arendt M, Ornbøl E, Fink P, Walach H. Mindfulness-based stress reduction and mindfulness-based cognitive therapy: a systematic review of randomized controlled trials. Acta Psychiatr Scand. 2011;124:102–19. doi: 10.1111/j.1600-0447.2011.01704.x. [DOI] [PubMed] [Google Scholar]
- 15.Hofmann SG, Sawyer AT, Witt AA, Oh D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. J Consult Clin Psychol. 2010;78:169–83. doi: 10.1037/a0018555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Khoury B, Lecomte T, Gaudiano BA, Paquin K. Mindfulness interventions for psychosis: A meta-analysis. Schizophr Res. 2013;150:176–84. doi: 10.1016/j.schres.2013.07.055. [DOI] [PubMed] [Google Scholar]
- 17.Chadwick P, Taylor KN, Abba N. Mindfulness groups for people with psychosis. Behav Cogn Psychother. 2005;33:351–9. doi: 10.1017/S1352465805002158. [DOI] [Google Scholar]
- 18.Chadwick P, Hughes S, Russell D, Russell I, Dagnan D. Mindfulness groups for distressing voices and paranoia: A replication and randomized feasibility trial. Behav Cogn Psychother. 2009;37:403–12. doi: 10.1017/S1352465809990166. [DOI] [PubMed] [Google Scholar]
- 19.Langer ÁI, Cangas AJ, Salcedo E, Fuentes B. Applying mindfulness therapy in a group of psychotic individuals: A controlled study. Behav Cogn Psychother. 2012;40:105–9. doi: 10.1017/S1352465811000464. [DOI] [PubMed] [Google Scholar]
- 20.Chien WT, Lee IY. The Mindfulness-based psychoeducation program for Chinese patients with schizophrenia. Psychiatr Serv. 2013;64:376–9. doi: 10.1176/appi.ps.002092012. [DOI] [PubMed] [Google Scholar]
- 21.Chadwick P, Strauss C, Jones A-M, Kingdon D, Ellett L, Dannahy L, et al. Group mindfulness-based intervention for distressing voices: A pragmatic randomised controlled trial. Schizopher Res. 2016;175:168–73. doi: 10.1016/j.schres.2016.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.López-Navarro E, Del Canto C, Belber M, Mayol A, Fernández-Alonso O, Lluis J, et al. Mindfulness improves psychological quality of life in community-based patients with severe mental health problems: A pilot randomized clinical trial. Schizophr Res. 2015;168:530–6. doi: 10.1016/j.schres.2015.08.016. [DOI] [PubMed] [Google Scholar]
- 23.Dannahy L, Hayward M, Strauss C, Turton W, Harding E, Chadwick P. Group person-based cognitive therapy for distressing voices: Pilot data from nine groups. J Behav Ther Exp Psy. 2011;42:111–6. doi: 10.1016/j.jbtep.2010.07.006. [DOI] [PubMed] [Google Scholar]
- 24.Johnson DP, Penn DL, Fredrickson BL, Kring AM, Meyer PS, Catalino LI, Brantley MA. Pilot study of loving-kindness meditation for the negative symptoms of schizophrenia. Schizophr Res. 2011;129:137–40. doi: 10.1016/j.schres.2011.02.015. [DOI] [PubMed] [Google Scholar]
- 25.Van der Valk R, van de Waerdt S, Meijer CJ, van den Hout I, de Haan L. Feasibility of mindfulness-based therapy in patients recovering from a first psychotic episode: A pilot study. Early Interv Psychia. 2013;7:64–70. doi: 10.1111/j.1751-7893.2012.00356.x. [DOI] [PubMed] [Google Scholar]
- 26.Abba N, Chadwick P, Stevenson C. Responding mindfully to distressing psychosis: A grounded theory analysis. Psychother Res. 2008;18:77–87. doi: 10.1080/10503300701367992. [DOI] [PubMed] [Google Scholar]
- 27.Ashcroft K, Barrow F, Lee R, MacKinnon K. Mindfulness groups for early psychosis: A qualitative study. Psychol Psychother. 2012;85:327–34. doi: 10.1111/j.2044-8341.2011.02031.x. [DOI] [PubMed] [Google Scholar]
- 28.May K, Strauss C, Coyle A, Hayward M. Person-based cognitive therapy groups for distressing voices: A thematic analysis of participant experiences of the therapy. Psychosis. 2014;6:16–26. doi: 10.1080/17522439.2012.708775. [DOI] [Google Scholar]
- 29.Langer AI, Carmona-Torres JA, Van Gordon W, Shonin EY. Mindfulness-Based Interventions in Psychosis (MBIp): State of the Art and Future Developments. In: Shonin E, Van Gordon W, Griffiths MD, editors. Mindfulness and Other Buddhist-Derived Approaches in Mental Health and Addiction, Advances in Mental Health and Addiction Series. Switzerland: Springer; 2016. pp. 211–23. [Google Scholar]
- 30.Kelleher I, Clarke MC, Rawdon C, Murphy J, Cannon M. Neurocognition in the extended psychosis phenotype: performance of a community sample of adolescents with psychotic symptoms on the MATRICS neurocognitive battery. Schizophr Bull. 2013;39:1018–26. doi: 10.1093/schbul/sbs086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Palmer BW, Heaton RK, Paulsen JS, Kuck J, Braff D, Harris MJ, Zisook S, Jeste DV. Is it possible to be schizophrenic yet neuropsychologically normal? Neuropsychology. 1997;11:437–46. doi: 10.1037/0894-4105.11.3.437. [DOI] [PubMed] [Google Scholar]
- 32.Bowie CR, Harvey PD. Cognitive deficits and functional outcome in schizophrenia. Neuropsychiatric Dis Treat. 2008;2:531–6. doi: 10.2147/nedt.2006.2.4.531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Green MF, Kern RS, Braff DL, Mintz J. Neurocognitive deficits and functional outcome in schizophrenia: Are we measuring the “right stuff”? Schizophr Bull. 2000;26:119–36. doi: 10.1093/oxfordjournals.schbul.a033430. [DOI] [PubMed] [Google Scholar]
- 34.Giuliano AJ, Li H, Mesholam-Gately RI, Sorenson SM, Woodberry KA, Seidman LJ. Neurocognition in the psychosis risk syndrome: a quantitative and qualitative. Review Curr Pharm Des. 2012;18:399–415. doi: 10.2174/138161212799316019. [DOI] [PubMed] [Google Scholar]
- 35.Lee J, Kern RS, Harvey PO, Horan WP, Kee KS, Ochsner K, et al. An intact social cognitive process in schizophrenia: situational context effects on perception of facial affect. Schizophr Bull. 2013;39:640–7. doi: 10.1093/schbul/sbs063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Langdon R, Connors MH, Connaughton E. Social cognition and social judgment in schizophrenia. Schizophr Res Cognition. 2014;1:171–4. doi: 10.1016/j.scog.2014.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Luedtke B, Kukla M, Renard SB, Lysaker P. Metacognitive functioning and social cognition as predictors of accuracy of self-appraisals of vocational function in schizophrenia. Schizophr Res. 2012;137:260–1. doi: 10.1016/j.schres.2012.02.006. [DOI] [PubMed] [Google Scholar]
- 38.Tang YY, Ma Y, Wang J, Fan Y, Feng S, Lu Q, et al. Short-term meditation training improves attention and self-regulation. Proc Natl Acad Sci U S A. 2007;104:17152–6. doi: 10.1073/pnas.0707678104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Silver H, Feldman P, Bilker W, Gur RC. Working memory deficit as a core neuropsychological dysfunction in Schizophrenia. Am J Psychiatry. 2003;160:1809–16. doi: 10.1176/appi.ajp.160.10.1809. [DOI] [PubMed] [Google Scholar]
- 40.McCabe DP, Roediger HL, McDaniel MA, Balota DA, Hambrick DZ. The relationship between working memory capacity and executive functioning: evidence for a common executive attention construct. Neuropsychology. 2010;24:222–43. doi: 10.1037/a0017619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Chambers R, Lo BCY, Allen NB. The impact of intensive mindfulness training on attentional control, cognitive style, and affect. Cogn Ther Res. 2008;32:303–22. doi: 10.1007/s10608-007-9119-0. [DOI] [Google Scholar]
- 42.Jha AP, Stanley EA, Kiyonaga A, Wong L, Gelfand L. Examining the protective effects of mindfulness training on working memory capacity and affective experience. Emotion. 2010;10:54–64. doi: 10.1037/a0018438. [DOI] [PubMed] [Google Scholar]
- 43.Zeidan F, Johnson SK, Diamond BJ, David Z, Goolkasian P. Mindfulness training improves cognition: Evidence of brief mental training. Conscious Cogn. 2010;19:597–605. doi: 10.1016/j.concog.2010.03.014. [DOI] [PubMed] [Google Scholar]
- 44.Vauth R, Rüsch N, Wirtz M, Corrigan PW. Does social cognition influence the relation between neurocognitive deficits and vocational functioning in schizophrenia? Psychiatry Res. 2004;128:155–65. doi: 10.1016/j.psychres.2004.05.018. [DOI] [PubMed] [Google Scholar]
- 45.Corrigan PW, Hirschbeck JN, Wolfe M. Memory and vigilance training to improve social perception in schizophrenia. Schizophr Res. 1995;17:257–65. doi: 10.1016/0920-9964(95)00008-9. [DOI] [PubMed] [Google Scholar]
- 46.Slade M. Mental illness and well-being: the central importance of positive psychology and recovery approaches. BMC Health Serv Res. 2010;10:26. doi: 10.1186/1472-6963-10-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Schrank B, Brownell T, Jakaite Z, Larkin C, Pesola F, Riches S, Tylee A, Slade M. Evaluation of a positive psychotherapy group intervention for people with psychosis: pilot randomized controlled trial. Epidemiol Psychiatr Sci. 2016;25:235–46. doi: 10.1017/S2045796015000141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.De la Fuente M, Franco C, Salvador M. Efectos de un programa de meditación (mindfulness) en la medida de la alexitimia y las habilidades sociales. Psicothema. 2010;22:369–75. [PubMed] [Google Scholar]
- 49.Extremera N, Fernández-Berrocal P. El uso de las medidas de habilidad en el ámbito de la inteligencia emocional. Boletín de Psicología. 2004;80:59–77. [Google Scholar]
- 50.Fisher M, Holland C, Merzenich MM, Vinogradov S. Using neuroplasticity-based auditory training to improve verbal memory in schizophrenia. Am J Psychiatry. 2009;166:805–11. doi: 10.1176/appi.ajp.2009.08050757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–91. doi: 10.3758/BF03193146. [DOI] [PubMed] [Google Scholar]
- 52.Ryff CD. Happiness Is Everything, or Is It? Explorations on the Meaning of Psychological Well-Being. J Pers Soc Psychol. 1989;57:1069–81. doi: 10.1037/0022-3514.57.6.1069. [DOI] [Google Scholar]
- 53.Van Dierendonck D. The Construct Validity of Ryff's Scales of Psychological Well-Being and Its Extension With Spiritual Well-Being. Pers Individ Differ. 2004;36:629–43. doi: 10.1016/S0191-8869(03)00122-3. [DOI] [Google Scholar]
- 54.Véliz BA. Propiedades psicométricas de la escala de bienestar psicológico y su estructura factorial en universitarios Chilenos. Psicoperspectivas. 2012;11(2):143–63. [Google Scholar]
- 55.Rojas-Barahona C, Zegers B, Förster C. La escala de autoestima de Rosenberg: Validación para Chile en una muestra de jóvenes adultos, adultos y adultos mayores. Rev Med Chile. 2009;137:791–800. doi: 10.4067/S0034-98872009000600009. [DOI] [PubMed] [Google Scholar]
- 56.Baer R, Smith G, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment. 2006;13:27–45. doi: 10.1177/1073191105283504. [DOI] [PubMed] [Google Scholar]
- 57.Schmidt C, Vinet E. Atención Plena: Validación del Five Facet Mindfulness Questionnaire (FFMQ) en estudiantes universitarios Chilenos. Ter Psicol. 2015;33:93–101. doi: 10.4067/S0718-48082015000200004. [DOI] [Google Scholar]
- 58.Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J Pers Soc Psychol. 1988;54:1063–70. doi: 10.1037/0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- 59.Dufey M, Fernández AM. Validez y confiabilidad del Positive Affect and Negative Affect Schedule (PANAS) en estudiantes universitarios Chilenos. RIDEP. 2012;1:157–73. [Google Scholar]
- 60.Meyer TJ, Miller ML, Metzger RL, Borkovec TD. Development and validation of the Penn State Worry Questionnaire. Behav Res Ther. 1990;28:487–95. doi: 10.1016/0005-7967(90)90135-6. [DOI] [PubMed] [Google Scholar]
- 61.Sandin B, Chorot P, Valiente RM, Lostao L. Validación Española del Cuestionario de Preocupación PSWQ: Estructura factorial y propiedades psicométricas. Rev Psicopatol Psicol Clin. 2009;14:107–22. [Google Scholar]
- 62.Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behav Res Ther. 1995;33:335–43. doi: 10.1016/0005-7967(94)00075-U. [DOI] [PubMed] [Google Scholar]
- 63.Antúnez Z, Vinet E. Escalas de Depresión, Ansiedad y Estrés (DASS – 21): validación de la versión abreviada en estudiantes universitarios Chilenos. Ter Psicol. 2012;30:49–55. doi: 10.4067/S0718-48082012000300005. [DOI] [Google Scholar]
- 64.Lysaker PH, Dimaggio G. Metacognitive capacities for reflection in schizophrenia: implications for developing treatments. Schizophr Bull. 2014;40:487–91. doi: 10.1093/schbul/sbu038. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
SPIRIT checklist. (DOC 121 kb)
Data Availability Statement
Not applicable.