

Abstract
Background:
Neck pain is a major public health concern that has been extensively studied in adults but not in children and adolescents. Therefore, the purpose of this article is to explore musculoskeletal neck pain in children and adolescents, as well as to discuss its possible risk factors and complications.
Methods:
Participants were patients under 18 years of age, who had presented to the clinic (Beirut, Lebanon) in 2015, with nonspecific neck pain. They were examined and asked to evaluate and localize the pain. Neck positioning during various activities along with other complications were explored. Patients reporting pain associated with congenital or systemic diseases and fractures were excluded.
Results:
Two-hundred-and-seven children and adolescents presented with nonspecific neck pain. Musculoskeletal neck pain with spasm was diagnosed in 180 patients (N = 180). Participants did not show any findings on physical examination and radiological studies, and had no comorbidities. More females (57%) than males (43%) and more adolescents (60%) than children (40%) were affected. All the 180 participants (100%) reported flawed flexion of their back and neck while studying and/or using smartphones and tablets. Eye symptoms were reported in 21% of the cases, and parents of most participants (82%) reported a change in the psychological and social behavior of their children.
Conclusions:
Musculoskeletal neck pain is an important disease in children and adolescents with numerous risk factors contributing to its development. Increased stresses regarding the cervical spine may lead to cervical degeneration along with other developmental, medical, psychological, and social complications.
Keywords: Adolescents, children, neck flexion, neck pain, smartphones, text neck
INTRODUCTION
Neck pain is a major public health problem in modern societies.[4,14] It can originate from any structure in the neck including intervertebral discs, ligaments, muscles, facet joints, dura, and nerve roots.[3] Potential causes can be tumors, infection, inflammatory diseases, and congenital disorders. In most cases, however, no systemic illness can be detected, and the complaint is labeled as musculoskeletal neck pain.[2]
Prevalence data have shown that, in a general population, the 1-year incidence of neck pain can be as high as 40%.[1] The World Health Organization (WHO) has ranked neck pain and other musculoskeletal diseases at 4th and 10th, respectively, among all health conditions for years lived with disability.[32] These conditions were also acknowledged as the key drivers of the increase in years lived with disability over the past 20 years.[32] In addition, data from the WHO Global Burden of Disease study showed that neck pain is the 8th ranked reason for most years lived with disability for 15–19 year olds of any health condition, which is higher than well-known adolescent public health problems such as asthma, alcohol use, drug use, and road injury.[21]
Although the epidemiology, burden, and treatment of musculoskeletal pain have been extensively explored in adults, the same is not true for children. The lack of clinical research pertinent to children and adolescents has been emphasized by multiple studies.[7,15,25,26,29] Emerging evidence shows that children, especially adolescents who report persistent pain, are at an increased risk of chronic pain as adults.[5,19,23] Moreover, many musculoskeletal illnesses follow a long-term pattern of recurring exacerbations and remissions, with the most consistent predictor of a new episode being the experience of a previous episode.[30]
As the surge in prevalence of musculoskeletal conditions occurs in childhood and adolescence, it may be necessary to investigate the condition at these stages of life.[24] Understanding aspects and risk factors surrounding the initial onset provides the best opportunity to develop efficacious treatments, and is central to any efforts at primary prevention.
Therefore, the purpose of this article is to explore musculoskeletal neck pain in children and adolescents under 18 years of age, and to discuss possible risk factors and complications related to this pain.
MATERIALS AND METHODS
This study explored cases that presented to our clinic in Beirut, Lebanon, in 2015 with nonspecific neck pain. Demographic information including age, sex, level of education, use of technology, and study habits were collected from individuals and their parents.
Interviewed individuals were under 18 years of age. Those whose ages ranged between 8 and 11 years were considered children, and those whose ages ranged between 12 and 17 years were considered adolescents. Patients were asked to localize the pain on themselves and on a model provided to them. Neurological assessment was conducted to test for sensory and motor deficits. Individuals were also asked about their pertinent daily habits, studying conditions, sitting positions, and sleeping positions. Further investigation explored the use of technology such as cell phones, tablets, computers, and television; participants were asked to show their usual neck position when engaged in these activities. All interviewees underwent radiological studies by radiography to rule out scoliosis or any other pathologies at the cervical spine level. In addition, psychological and social symptoms were investigated.
For the purposes of this study, we did not include patients reporting pain associated with congenital or systemic diseases, such as scoliosis. We also excluded patients reporting pain resulting from frank injuries, such as fractures, and pain following surgical interventions. Chronic neck pain was defined as continuous neck complaints for more than 6 months.
RESULTS
In total, 207 children and adolescents presented with nonspecific neck pain. All patients reported having cervical neck pain of more than 6 months’ duration that radiates dorsally down the back and to the shoulders. None had sensory or motor deficits. Twenty-seven patients were found to have dorsolumbar scoliosis and were excluded from the study. The remaining 180 patients did not show any finding on physical examination and radiological studies, and had no comorbidities. They were diagnosed with musculoskeletal neck pain with spasm, and were the focus of our study (N = 180). Ages ranged between 8 and 17 years, with a mean age of 14 years. Demographics of the children and adolescents participating in the study are presented in Table 1.
Table 1.
Demographics of the children and adolescents participating in the study (N=180)
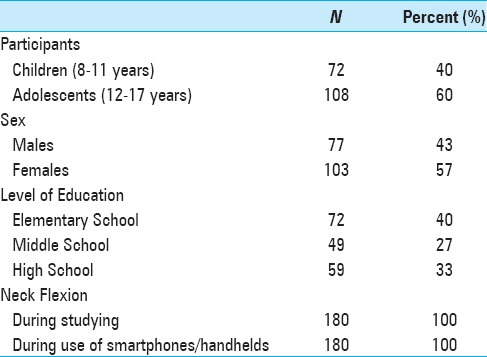
All the 180 participants (100%) reported flawed flexion of their back and neck while studying. They also admitted to using smartphones and/or tablets. When asked to demonstrate how they used these devices, all participants (100%) showed strong flexion of the neck (≥45 degrees) when engaged in the activity. Children and adolescents in our sample spent an average of 5 and 7 hours a day, respectively, on their smartphones and handheld devices. Table 2 shows the pain sites, eye symptoms, and psychological and social effects that were found in the children and adolescents.
Table 2.
Pain location, eye symptoms, and psychological and social effects in the children and adolescents participating in the study (N=180)
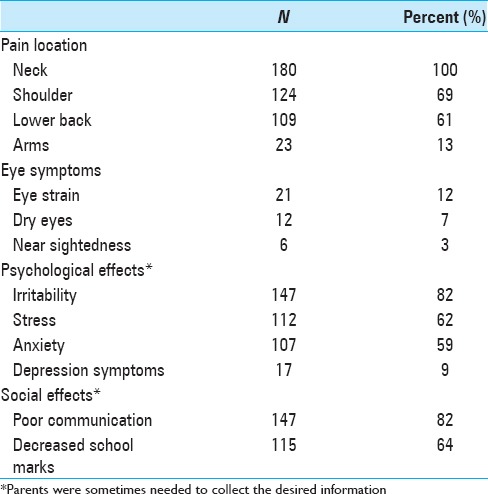
A change in behavior, defined by a change in daily habits and usual social interactions, as noticed by parents, was reported in 147 young participants (82%). They were described as having become more irritable and alienated. Parents of 115 participants (64%) reported that their grades in school have been declining.
DISCUSSION
Musculoskeletal neck pain in children and adolescents is very common. Almost 87% (180 of 207) of the children and adolescents presented in our study were diagnosed with musculoskeletal neck pain. Other studies and reviews have shown 1-year incidences of 28% and 40% for neck pain.[1,22]
All our participants reported flexing their back and neck while studying. Ariëns et al.[1] found a positive relationship between neck flexion and neck pain, suggesting an increased risk of neck pain for individuals studying with the neck at a minimum of 20° of flexion for more than 70% of the studying time. Moreover, all our participants showed strong flexion of the neck when using smartphones. “Text neck,” a 21st-century syndrome, is a term derived from the onset of cervical spinal degeneration resulting from the repeated stress of frequent forward head flexion while looking down at the screens of mobile devices and “texting” for long periods of time.[31] Text neck is becoming more common as more people, especially teens and adolescents, hunch over smartphones.[6] It is estimated that 75% of the world's population spends hours daily hunched over their handheld devices with their heads flexed forward.[19] In our sample, children and adolescents spent averages of 5 and 7 hours a day, respectively, with their heads tilted over reading and texting on their smartphones and handheld devices. Cumulatively, this is an average of 1825 and 2555 hours a year, respectively, of excess stresses seen in the cervical spine area. Hansraj adds that it is possible that a high school student may spend an extra 5000 hours in poor posture.[18]
The weight put on the spine dramatically increases when flexing the head forward at varying degrees [Figure 1]. A full-grown head weighs 4.54 to 5.44 kg in the neutral position.[18] As the head tilts forward, the forces seen by the neck surges to 12.25 kg at 15°, 18.14 kg at 30°, 22.23 kg at 45°, and 27.22 kg at 60°.[18] The frequent forward flexion causes changes in the cervical spine, curvature, supporting ligaments, tendons, and musculature, as well as the bony segments, commonly causing postural change and pain felt in the neck and other associated areas.[31]
Figure 1.

A chart depicting the stress and weight put on the neck and spine as a result of hunching over a smartphone and handheld devices at varying degrees. The neck flexion angle is the angle between the global vertical and the vector pointing from C7 to the occipitocervical joint. A full-grown head weighs 5 kg in the neutral position. As the head bends forward, the weight seen by the neck increases to 18 kg at 30° and 27 kg at 60°
The effects of forward flexion of the neck transcend pain to contribute to more associated complications. Often times, the effects of prolonged neck flexion can contribute to nearsightedness, eye strain, or dry eyes, as the eyes are forced to focus on an object placed nearby.[8] New research suggests a link between forward leaning postures that people use while texting, studying, surfing the web, emailing, and playing video games, and hyperkyphosis, which is associated with pulmonary disease and cardiovascular problems.[9] It is suggested that when someone drops their head and rounds their shoulders while looking at a smartphone or a tablet, it is harder for them to take a full breath because of the restriction to their muscles.[9] In addition, the ribs cannot move properly; thus, the heart and lungs cannot function to their full effectiveness.[9] Most times, children and adolescents do not know they could be doing serious long-term damage to their body because the short-term effects are not as noticeable. It is only in later life that the effects can seriously affect the quality of life. This increases fears that younger people, who are society's biggest users of smartphones and tablets, could be facing a future of pain and disability, or even taking years off of their life expectancy.
Emre et al.[10] indicate that computers, wireless internet, cell phones, and televisions emit an extremely low-frequency electromagnetic field. Electromagnetic radiation can cause difficulty sleeping, dizziness, headaches, tingling in the hands, ringing in the ears, eye pain, “unexplained” cardiac conditions, electrosensitivity, low immunity, attention deficit hyperactivity disorder, and autism.[20] When electrical properties are considered, the absorption of electromagnetic radiation through a child's head can be over two times greater, and absorption of the skull's bone marrow ten times greater, than in adults.[16]
Parents of most of our participants reported that their children have become more isolated and easily irritable. In addition, their grades in school have been negatively affected. Children who use more than the expert recommended 1–2 hours per day of technology, have a 60% increase in psychological disorders.[28] As mentioned previously, children and adolescents in our sample spent averages of 5 and 7 hours a day, respectively, on their smartphones and handheld devices. It is indicated that the more time students spend consuming media, and the more violent its contents are, the worse their grades in school, even when controlling for vital factors such as family, education, or immigrant background.[27] In addition, spending too many hours on handheld devices and smartphones will negatively affect children and adolescents’ communication skills, particularly with regard to face-to-face communication skills, bullying, and teasing.[17]
The lack of validated instruments to measure musculoskeletal neck pain and its consequences in children and adolescents is a limitation in similar studies. This is due to the fact that it becomes difficult to draw conclusions and compare between different samples, populations, and cultures. In addition, the method of administration is critical because self-administered instruments cannot be conducted among illiterate and young children, and the need for a parent to collect information may hinder the pain evaluation process.
Future studies should aim to find a unified instrument to measure musculoskeletal neck pain, and validation across cultures should occur. The pathways and mechanisms for the association of pain experienced in childhood and pain experienced in adulthood are unknown. It can be hypothesized that a physiological or behavioral trigger is set when a child has a particular painful experience, which predisposes them to pain as an adult. Genetic susceptibility may also underlie the experience of pain. Future studies can aim to explore these mechanisms. Moreover, there is a particular need for studies to investigate the nature of the relationships between neck pain and other adverse health risk factors.
CONCLUSIONS
Musculoskeletal neck pain is a common multifactorial disease in children and adolescents, implying that there are numerous risk factors contributing to its development. Bending the head, neck, and shoulders over cell phones and handheld devices, along with distorted neck positioning when sitting, studying, and watching television, can lead to incrementally increased stresses in the cervical spine area. These stresses may lead to early wear, tear, degeneration, and possibly surgeries. Other developmental, medical, psychological, and social complications are also of concern. While it is nearly impossible to avoid the habits and technologies that cause these issues, young individuals should make an effort to perform activities with a neutral spine and to avoid neck flexion for hours each day.[11,12,13,14] Cervical spine surgeons, pediatric neurologists, public health advocates, and social workers should run campaigns to raise awareness on musculoskeletal neck pain and its medical, psycholgical, and societal consequences, and methods of prevention and treatment.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Contributor Information
Jawad Fares, Email: jyf04@mail.aub.edu.
Mohamad Y. Fares, Email: myf04@mail.aub.edu.
Youssef Fares, Email: yfares@ul.edu.lb.
REFERENCES
- 1.Ariëns GAM, Borghouts JAJ, Koes BW. Neck pain. In: Crombie IK, Croft PR, Linton SJ, LeResche L, Korff M, editors. Epidemiology of pain. Seattle: IASP Press; 1999. pp. 235–6. [Google Scholar]
- 2.Bogduk N. Neck pain. Aust Fam Physician. 1984;13:26–30. [PubMed] [Google Scholar]
- 3.Bogduk N. Neck pain: An update. Aust Fam Physician. 1988;17:75. [PubMed] [Google Scholar]
- 4.Bouter LM, van der Wal G. Psychosocial risk factors for neck pain: A systematic review. Am J Ind Med. 2011;39:180–93. doi: 10.1002/1097-0274(200102)39:2<180::aid-ajim1005>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- 5.Brattberg G. Do pain problems in young school children persist into early adulthood? A 13-year follow-up. Eur J Pain. 2004;8:187–99. doi: 10.1016/j.ejpain.2003.08.001. [DOI] [PubMed] [Google Scholar]
- 6.Chronic Conditions Team. Text Neck: Is Smartphone Use Causing Your Neck Pain? Healthessentials. 2015. [Last accessed on 2016 Sep 01]. https://health.clevelandclinic.org/2015/03/text-neck-is-smartphone-use-causing-your-neck-pain/
- 7.Cohen E, Uleryk E, Jasuja M, Parkin PC. An absence of pediatric randomized controlled trials in general medical journals, 1985–2004. J Clin Epidemiol. 2007;60:118–23. doi: 10.1016/j.jclinepi.2006.03.015. [DOI] [PubMed] [Google Scholar]
- 8.CORRECTVISION. “The Effects of Texting on Your Eye Health,” CORRECTVISION 2015. [Last accessed on 2016 Sep 01]. http://www.correctvision.com/eye-health/effects-of-texting/
- 9.Curtis S. Texting for long periods ‘could lower life expectancy’. The Telegraph 2014. [Last accessed on 2016 Sep 01]. http://www.telegraph.co.uk/technology/mobile-phones/10721014/Texting-for-long-periods-could-lower-lifeexpectancy.html .
- 10.Emre M, Cetiner S, Zencir S, Unlukurt I, Kahraman I, Topcu Z. Oxidative stress and apoptosis in relation to exposure to magnetic field. Cell Biochem Biophys. 2011;59:71–7. doi: 10.1007/s12013-010-9113-0. [DOI] [PubMed] [Google Scholar]
- 11.Fares J, Al Tabosh H, Saadeddin Z, El Mouhayyar C, Aridi H. Stress, burnout and coping strategies in preclinical medical students. N Am J Med Sci. 2016;8:75. doi: 10.4103/1947-2714.177299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fares J, Fares Y. The role of yoga in relieving medical student anxiety and stress. N Am J Med Sci. 2016;8:202. doi: 10.4103/1947-2714.179963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fares J, Saadeddin Z, Al Tabosh H, Aridi H, El Mouhayyar C, Koleilat MK, et al. Extracurricular activities associated with stress and burnout in preclinical medical students. J Epidemiol Glob Health. 2016;6:177–85. doi: 10.1016/j.jegh.2015.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fares Y. Conseils pour une Colonne Vertebrale Saine. Beirut. 2000 [Google Scholar]
- 15.Fares Y, Fares J. Neurosurgery in Lebanon: History, Development, and Future Challenges. World Neurosurg. 2017 doi: 10.1016/j.wneu.2016.12.014. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 16.Gandhi OP, Morgan LL, de Salles AA, Han YY, Herberman RB, Davis DL. Exposure limits: The underestimation of absorbed cell phone radiation, especially in children. Electromagn Biol Med. 2012;31:34–51. doi: 10.3109/15368378.2011.622827. [DOI] [PubMed] [Google Scholar]
- 17.Graham JB. Impacts of Text Messaging on Adolescents’ Communication Skills: School Social Workers’ Perceptions. Master of Social Work Clinical Research Papers, Paper 184, St. Catherine University, St. Paul and Minneapolis, Minnesota, US. 2013 [Google Scholar]
- 18.Hansraj KK. Assessment of stresses in the cervical spine caused by posture and position of the head. Surg Technol Int. 2014;25:277–9. [PubMed] [Google Scholar]
- 19.Hestbaek L, Leboeuf-Yde C, Kyvik KO, Manniche C. The course of low back pain from adolescence to adulthood: Eight-year follow-up of 9600 twins. Spine. 2006;31:468–72. doi: 10.1097/01.brs.0000199958.04073.d9. [DOI] [PubMed] [Google Scholar]
- 20.Hossmann KA, Hermann DM. Effects of electromagnetic radiation of mobile phones on the central nervous system. Bioelectromagnetics. 2003;24:49–62. doi: 10.1002/bem.10068. [DOI] [PubMed] [Google Scholar]
- 21.Institute for Health Metrics and Evaluation – IHME. HealthData.org 2015. [Last accessed on 2016 Sep 01]. http://vizhub.healthdata.org/gbd-compare/
- 22.Jeffries LJ, Milanese SF, Grimmer-Somers KA. Epidemiology of adolescent spinal pain: A systematic overview of the research literature. Spine. 2007;32:2630–7. doi: 10.1097/BRS.0b013e318158d70b. [DOI] [PubMed] [Google Scholar]
- 23.Jones GT, Silman AJ, Power C, Macfarlane GJ. Are common symptoms in childhood associated with chronic widespread body pain in adulthood?: Results from the 1958 british birth cohort study. Arthritis Rheum. 2007;56:1669–75. doi: 10.1002/art.22587. [DOI] [PubMed] [Google Scholar]
- 24.Kamper SJ, Henschke N, Hestbaek L, Dunn KM, Williams CM. Musculoskeletal pain in children and adolescents. Braz J Phys Ther. 2016;20:275–84. doi: 10.1590/bjpt-rbf.2014.0149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McBeth J, Jones K. Epidemiology of chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. 2007;21:403–25. doi: 10.1016/j.berh.2007.03.003. [DOI] [PubMed] [Google Scholar]
- 26.Michaleff ZA, Kamper SJ, Maher CG, Evans R, Broderick C, Henschke N. Low back pain in children and adolescents: A systematic review and meta-analysis evaluating the effectiveness of conservative interventions. Eur Spine J. 2014;23:2046–58. doi: 10.1007/s00586-014-3461-1. [DOI] [PubMed] [Google Scholar]
- 27.Mössle T, Kleimann M, Rehbein F, Pfeiffer C. Media use and school achievement–boys at risk? Br J Dev Psychol. 2010;28:699–725. doi: 10.1348/026151009x475307. [DOI] [PubMed] [Google Scholar]
- 28.Page AS, Cooper AR, Griew P, Jago R. Children's screen viewing is related to psychological difficulties irrespective of physical activity. Pediatrics. 2010;126:e1011–7. doi: 10.1542/peds.2010-1154. [DOI] [PubMed] [Google Scholar]
- 29.Rodgers A. Managing chronic pain in children and adolescents. BMJ. 2002;324:1570–6. [Google Scholar]
- 30.Taylor JB, Goode AP, George SZ, Cook CE. Incidence and risk factors for first-time incident low back pain: A systematic review and meta-analysis. Spine J. 2014;14:2299–319. doi: 10.1016/j.spinee.2014.01.026. [DOI] [PubMed] [Google Scholar]
- 31.TEXT NECK®: A Global Epidemic. The Text Neck Institute. [Last accessed on 2016 Aug 29]. http://text-neck.com/
- 32.Vos T, Barber RM, Bell B, Bertozzi-Villa A, Biryukov S, Bolliger I, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:743–800. doi: 10.1016/S0140-6736(15)60692-4. [DOI] [PMC free article] [PubMed] [Google Scholar]