

Abstract
Background and aims
Prohibitions on producing, distributing and selling cannabis are loosening in various jurisdictions around the world. This paper describes the diversification of cannabis supply laws and discusses the challenges to and opportunities for learning from these changes.
Methods
We document changes in cannabis supply laws that, de jure, legalize cannabis production for medical and/or non-medical purposes (excluding industrial hemp) in Australasia, Europe, North America and South America. We also highlight challenges to evaluating these legal changes based on our experiences studying cannabis laws and policies in the United States.
Findings
As of August 2016, two countries have passed laws to legalize large-scale cannabis production for non-medical purposes at the national (Uruguay) or subnational level (four US states). At least nine other countries have passed laws to allow cannabis to be produced and distributed for medicinal purposes. Most of the changes in cannabis supply laws have occurred since 2010. The data available in most countries are inadequate for evaluating rigorously the changes in cannabis supply laws.
Conclusion
The evidence base for assessing changes in cannabis supply laws remains weak. Efforts should focus upon improving information about quantities consumed and market transactions.
Keywords: Cannabis, legalization, policy analysis
INTRODUCTION
Prohibitions on producing, distributing and selling cannabis are loosening in various jurisdictions around the world. There have been unprecedented changes since 2012, with four US states allowing for-profit companies to produce and distribute cannabis for non-medical use and Uruguay becoming the first country in the world to remove the prohibition on cannabis production. However, focusing only upon the United States and Uruguay understates significantly the amount of change that has occurred.
From decriminalization to medicalization to the oft-cited approaches implemented in the Netherlands and Spain, there have been noteworthy movements away from cannabis prohibition. In the 1970s, countries such as Italy and Uruguay eliminated the criminal penalties associated with small amounts of cannabis, some US states reduced the criminal penalties associated with cannabis possession and the Netherlands revised its Opium Act, which created the foundation for its coffeeshop model [1–4]. Cannabis depenalization and decriminalization continued to emerge in several countries during the next 40 years.
While reductions in the penalties associated with simple possession and/or use of cannabis have been evolving for some time, reductions in the penalties associated with selling cannabis are a relatively new and important phenomenon. Thus, this paper seeks to make two contributions. First, it documents the growing diversification of cannabis supply laws around the world, highlighting unique features of these policies that are sometimes ignored. Secondly, it offers ideas for improving efforts to learn from these changes in cannabis supply laws. While the promises and pitfalls of cross-national drug policy research are well known [5,6], there are also several issues that confront those who wish to monitor within-country changes to cannabis policies that should be considered. A number of these issues are discussed below.
DIVERSIFICATION OF SUPPLY LAWS AROUND THE WORLD
The prohibition of cannabis started more than 100 years ago in western countries, with many states in the United States and Europe banning its production for non-medical purposes roughly between the last quarter of the 19th century and the first quarter of the 20th century [7]. The United Nations Single Convention on Narcotic Drugs went into force in 1964, and by the end of the century most countries had prohibited the production, distribution and possession of cannabis for non-medical/non-scientific purposes (industrial hemp is a separate issue not addressed in this paper).
A number of countries and subnational jurisdictions have decriminalized cultivation of a small number of plants along with decriminalizing possession of cannabis for personal consumption [1,8]. In these jurisdictions cultivation for personal consumption is not a criminal offense, but can still be punished by an administrative sanction and/or fine. In some places multiple offenses could lead to heavier sanctions and sometimes a criminal offense. Cultivation for personal consumption does not condone or legally protect the sort of larger-scale cultivation observed in many countries that allow medical cannabis.
Table 1 presents a list of countries that legally allow cannabis production for medical and/or non-medical purposes at the national or subnational level; it does not include jurisdictions that only decriminalized cultivation for personal consumption. It also excludes countries that only allow cannabis to be produced for research purposes or industrial hemp. We specify production so as to exclude those countries that only allow pharmaceutical-grade cannabis extracts to be imported for medical purposes (the United Kingdom is the exception, as that is where the cannabis is produced for Sativex; it was approved for use there in 2010).
Table 1.
Jurisdictions passing laws to allow cannabis production and distribution for non-research purposes as of August 2016 (excludes allowances for industrial hemp or personal grows).
| Country | National? | Year passed | Comments |
|---|---|---|---|
| Non-medical | |||
| United States | No | 2012a | Four states allow for-profit companies to produce and sell cannabis (Alaska, Colorado, Oregon and Washington) to anyone aged 21 years and older; Washington, DC only allows home production and sharing. Production and possession remain illegal under federal law |
| Uruguay | Yes | 2013 | Residents aged 18 years and older must register with the government to either grow at home, join a collective or purchase cannabis from pharmacies. The latter will be produced by state-licensed companies and it is expected to be available in participating pharmacies by the end of 2016. The government will determine the price and potency of cannabis sold in pharmacies |
| Medical | |||
| United States | No | 1996a | 25 states and DC passed laws to allow cannabis flowers and other products to be produced and distributed; at least 15 other states allow physicians to recommend cannabidiol-oils, but not necessarily production. This all remains illegal under federal law. |
| Israel | Yes | Late 1990s | A medical program was developed per the 1995 recommendation of a subcommittee of the Israeli Parliament Drug Committee. Privately held companies that produce cannabis operate under a license from the Department of Health |
| Netherlands | Yes | 2000 | The Office of Medicinal Cannabis was established in 2000 and cannabis flowers were first available in pharmacies in 2003. Only five strains are currently allowed to be prescribed and they are all produced by one supplier |
| Canada | Yes | 2001 | Currently, all medical cannabis is supposed to be produced by federally licensed private companies and delivered via mail. Efforts are being made to eliminate the medical dispensaries that still operate in some jurisdictions. It was announced in August 2016 that registered patients will be allowed to grow at home |
| Chile | Yes | Late 2000s | A license to grow cannabis that was granted in 2009 was withdrawn before production, but the Supreme Court ruled in 2012 that the withdrawal was unconstitutional. In 2016, Chile is expected to harvest medical cannabis from a large, legal plantation |
| United Kingdom | Yes | 2010 | Since the 1990s GW Pharmaceuticals has produced cannabis plants in the United Kingdom to create Sativex and other cannabis-based extracts. In 2010, the United Kingdom approved Sativex to be prescribed for spasticity due to multiple sclerosis (as in many countries) |
| Czech Republic | Yes | 2013 | Domestically produced cannabis for the medical program was first delivered to the State Agency for Medical Cannabis in early 2016 (previously it had to be imported) |
| Uruguay | Yes | 2013 | Will be produced by state-licensed companies and available in pharmacies for those with a physician’s prescription |
| Jamaica | Yes | 2015 | The regulations have not been implemented, but there are plans to allow small and large- scale production of medical cannabis for residents as well as tourist and export markets |
| Colombia | Yes | 2015 | The decree signed in December 2015 permits medical cannabis under the national drug law. The new decree may be modified or superseded by an existing bill in Congress, but it currently paves the way for state-licensed commercial production, although it is unclear how much cannabis production will be permitted |
| Australia | Yes | 2016 | A law was passed at the Commonwealth level to create a regulatory framework for commercial cannabis production for medical purposes (the Tasmanian law passed in 2015 only pertained to providing cannabis for research purposes in New South Wales) |
As the Netherlands and Spain are mentioned regularly in discussions of alternative cannabis policies, readers may wonder why they are not included in Table 1. While these regimes are noteworthy—especially as they inhabit the middle ground between prohibition and commercialization (discussed below)—these countries did not pass actual laws allowing production and sales. In the Netherlands cannabis production remains illegal and enforced seriously, even though retail sales are tolerated in the coffeeshops. With regard to Spain, it: ‘criminalizes only sale, not possession or cultivation for one’s own use; drug-sharing clubs inhabit a legal gray area. …whatever legal protection the clubs have comes more from absence of enforcement than proactive legislation’ [12].
While this paper does not focus on Asia, India is a notable case that is sometimes discussed (e.g. [4]) but hard to categorize. While a law passed by the central government in 1985 prohibits the consumption of cannabis resin and flowers, it makes an exception for possessing cannabis leaves, seeds and infused products that are sometimes sold and taxed in government-authorized ‘bhang’ shops, often for religious purposes. There appears to be legal variation throughout the country, and further complicating categorization is Malhorta’s observation that: ‘Growing marijuana is illegal and punishable by up to 10 years in prison, but harvesting the leaves that grow by themselves in the wild is allowed’ [16].
As this paper is not based on a legal analysis of national and subnational drug laws for every single country, and the laws are rapidly changing, it is possible that some jurisdictions are excluded from Table 1; thus, one should consider this list as informative and not necessarily exhaustive. Our purpose is to illustrate the considerable diversity in cannabis supply laws that has emerged over the past two decades. We also want to raise awareness of important differences between them by highlighting four dimensions that can influence the size of the market that emerges in a given jurisdiction: purpose, producer, purchaser and product.
Purpose
Jurisdictions legalizing cannabis for recreational purposes, such as Uruguay and four US states, allow cannabis to be supplied for any reason. Medical marijuana jurisdictions, however, demonstrate tremendous variation in the conditions and illnesses for which cannabis can be supplied; the variation cannot be explained simply by the state of medical research. For example, physicians in California can recommend cannabis for virtually any condition or symptom they choose, while physicians in states such as Delaware and New York are only allowed to make recommendations for a very limited set of medical conditions specified in each state’s law. Jamaican law seeks to allow cannabis for sacramental, medical or scientific purposes, but the regulations have yet to be finalized [17].
Producer
An important issue in any cannabis supply policy concerns who is granted legal protection to produce and process cannabis for retail sale. Previous research in this journal highlights that several choices are available for jurisdictions considering alternatives to prohibiting marijuana supply (Fig. 1). In four US states that have legalized for recreational purposes, for-profit businesses are allowed to produce and sell cannabis. The District of Columbia legalized in 2014, but only allows home production. The situation is very different in Uruguay, where those who want legal cannabis must register with the government and choose one of three supply choices: home production, join a cooperative or purchase from participating pharmacies. The latter option is still being implemented, but the government has only licensed two companies to produce cannabis and the government will regulate the industry heavily, as well as products that can be sold, and set the price [18]. Medical markets have even greater variability in assigning producer rights, with countries such as Israel and the Netherlands assigning those rights to just a few (the Netherlands only allows one), while other jurisdictions give medical production rights to many, especially in the United States.
Figure 1.
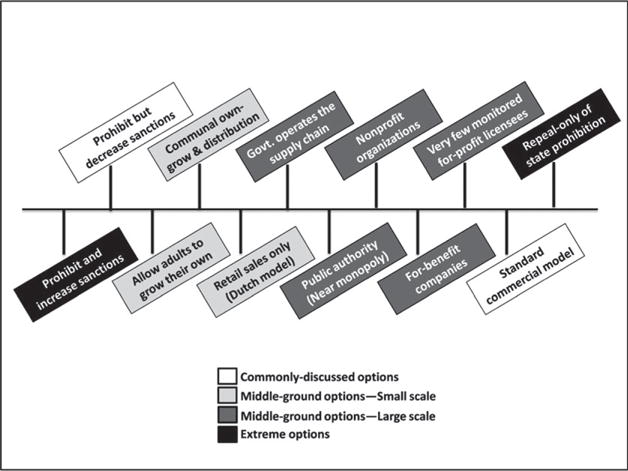
Alternatives to status quo prohibition of marijuana supply. Source: reproduced from [19]
Purchaser
In Uruguay, only residents aged 18 years or older who have registered with the government can obtain cannabis legally. To reduce the probability of diversion, non-residents are excluded from the legal market. The situation is very different in four US states where anyone from any country aged 21 years or older can purchase cannabis for any reason. All the states have thresholds for the amount of cannabis products that can be purchased at a time, and Colorado initially imposed lower thresholds for non-residents in an effort to reduce diversion to other states (that has changed). In Jamaica there is serious interest in profiting from tourists, and the current plan is to allow those who assert that they have a medical recommendation from a physician to purchase cannabis on the island, after they pay a license fee [12].
Products
While cannabis-infused brownies and teas are not uncommon in areas maintaining prohibition regimes, in many US states with legal or medical production the types of edibles and concentrated products are proliferating. In addition to several types of candies, lotions, balms and patches, the production of hash oil, sometimes in excess of 80% tetrahydrocannabinol (THC), is making it easier to produce e-cigarettes that include a hash-oil solution as well as waxes that can be dabbed (i.e. flash-vaporized). This is in stark contrast to the Dutch medical cannabis system, which only authorizes a handful of strains for medical use [20]. For now, Uruguay has decided to not allow edibles for non-medical purposes.
As indicated by the examples above, the amount of cannabis that will be supplied to a market, and hence the size of the market, will be influenced directly by decisions made by jurisdictions regarding these four dimensions as well as those discussed by others [21,22]. Ignoring these differences and their implications on the size of the market can generate misleading conclusions about the consequences of these legal changes. Researchers have demonstrated similar problems when trying to evaluate the effects of decriminalization and medical marijuana laws on consumption and consequences of use [23–25].
IMPROVING OUR ABILITY TO EVALUATE THE CONSEQUENCES OF CHANGING CANNABIS SUPPLY LAWS
Given the pace of change and tremendous variation in these laws, there is much interest in learning about their consequences. Developing reliable estimates of the impact of these policies upon the supply of cannabis is extremely difficult, as prohibition prevents systematic collection of standard supply measures (e.g. production, cost of production), making any type of research design that requires pre-policy change data infeasible. Therefore, most evaluations have focused upon prevalence and consequences associated with use. A recent paper published in this journal explained how making legal allowances for cannabis supply could have profound consequences for production costs, retail prices and consumption as well as health and social wellbeing [19]. Much will depend upon the scale of legal production, what is allowed to be produced, who is allowed to produce it, who is allowed to consume and the agencies designated to regulate.
Even when focusing upon these alternative measures, important challenges remain. For example, differences across jurisdictions in data collection and measurement can limit the inferences from comparisons, particularly when there are methodological differences in conducting general population surveys, estimating the number of problem drug users or defining cannabis-related arrests [6]. In addition, many countries have a weak data infrastructure for monitoring within-country changes.
How can interested researchers overcome some of these limitations and move policy evaluations forward in this space? We highlight three ideas for improving data collection that would assist with both cross-county and within-country analyses of these policy changes. This list is not intended to be exhaustive, but merely suggestive of steps that we think are important to take based on our experiences evaluating and projecting the consequences of changing cannabis supply laws in the United States [22,24,26]. These suggestions could improve evaluations of both supply- and demand-side policy changes.
Collect better measures about consumption
Many countries devote significant resources to obtaining self-report data about substance use via surveys of the general population and/or student populations. Much can be learned by studying who uses drugs, how often they use and how use changes over time. These data feature prominently in evaluations and drive media reports about substance use; however, a limitation to most general-population and student drug surveys is that they typically ask only about prevalence; the better ones also ask about days used in the past month.
It is critical to move beyond prevalence if we want to assess the size of a market using a demand-side approach and making projections of possible tax revenues. Information about total use days is better than prevalence, but an even better measure is total grams consumed [27]. Unfortunately, information about amount used per use day or use episode is collected rarely; in the United States the annual general population survey stopped inquiring about joints consumed per use day in 1995. There are some notable exceptions, which include pictures of unrolled joints and uncrushed buds next to prompts such as rulers and credit cards [28–32]. Even fewer surveys inquire about time of use sessions within a day, amount consumed per use session, sharing or what types of cannabis products were used (e.g. flowers, edibles, oils).
For assessing impacts associated with cannabis use, particularly health consequences, researchers should also try to understand the typical potency per dose consumed. Cannabis is not a homogeneous good; there are dozens of cannabinoids in the plant, with THC being the main cannabinoid responsible for intoxication [33]. Although problematic, at a minimum surveys should include some categorical measure about perceived potency; even better would be actual information about THC and other cannabinoids. Unless the purchase is made from dispensary or store, which requires testing and labeling, most users will not have this detailed information.
Some researchers have obtained potency information by interviewing users and then compensating them for a sample of their most recent purchase, which is then sent to a testing laboratory (e.g. [34]), but we are not aware of samples being collected for a large or representative population. Testing the potency of seized cannabis can provide some information for analysts seeking better information about what is being consumed in a particular locality (e.g. see [35]) or how cannabis policy can influence the potency of what is being consumed [36]. However, researchers cannot assume that the average potency of what is seized is the same as the average potency of what is consumed.
Most surveys do not make a distinction between medical and recreational consumption, yet consumption patterns across these two user groups need not be the same. A recent study, examining patterns of consumption between self-identified recreational and medical cannabis users in four US states where medical cannabis laws had passed, found that medical users are more likely to vaporize cannabis, consume edibles and consume in larger quantities per use episode than recreational consumers [37]. If the share of medical consumers in a given population changes over time, and these medical users consume cannabis in different amounts or forms, then changes in the composition of type of users could confound evaluations of the effects of policies on a specific type of user (e.g. recreational user). This will continue to be an important distinction as more jurisdictions make allowances for medical cannabis. It is imperative that we obtain more information about the type of cannabis products consumed by type of user as well as the amount consumed per episode per product. We must also acknowledge that some users consume for both medical and non-medical purposes.
Finally, for those interested in understanding the overall effect of cannabis legalization on public health and public safety (for both medical and recreational purposes), attention must be given to how it influences the consumption of alcohol, tobacco, prescription opiates and other drugs [7]. The literature is mixed about whether cannabis is an economic complement or substitute for alcohol [22,38]. For example, if they are they are complements and an increase in cannabis consumption increases concurrent alcohol consumption, this could have important implications for health, especially for impaired driving. While driving drunk tends to be worse than driving stoned, the bulk of the research suggests that driving under the influence of both alcohol and cannabis sharply increases the probability of a crash [39,40]. Conversely, if they are substitutes and legalization leads to a 50% increase in marijuana consumption and a 10% decrease in heavy alcohol consumption, this could be a public health ‘win’, as the economic costs of heavy alcohol use are much greater than they are for cannabis [7]. To understand this relationship, we must do more than consider whether two substances were used in the same 30-day period; we need to start asking whether the two substances are consumed during the same use occasion.
Validate self-report data
How much should we trust self-reported information about the use of an illegal drug? There is a large literature about survey respondents under-reporting stigmatized behaviors and how different survey methodologies can improve honest reporting (e.g. [41]). While cannabis users tend to be more honest than those who use the more expensive drugs, under-reporting can be severe. In the most recent validation of the US household survey, which was conducted in 2001 with those aged 12–24 years, only 61% of those testing positive for cannabis admitted to using it in the past month [42].
Unfortunately, most of these validation studies are old, based largely in the United States (e.g. see [43,44]), focus upon special populations (e.g. [42,45]) and do not address under-reporting of frequency of use [29]. Indeed, a recent cross-national comparison of drug indicators did not uncover any validation studies of general population studies in Europe [6]. The comparison, however, highlights a question from the 2003 European School Survey Project on Alcohol and Other Drugs of 15–16-year-old students, which asked: ‘If you had ever used marijuana or hashish, do you think you would have said so in this questionnaire?’. Focusing simply on those who responded ‘definitely not’, three-quarters of the countries had rates greater than 4% and one-quarter had rates greater than 8%; Croatia, Greenland, Latvia, Lithuania and Malta all reported values greater than 10%.
The lack of validation will have serious consequences for evaluating or projecting changes in cannabis laws on cannabis consumption and demand-side estimates of the size of the market. If the change in laws influences the probability that users are honest about their use, it will be difficult to determine whether a detected increase is real or an artifact of more honest reporting. To the extent that general population surveys may be used to help design and evaluate these significant policy changes, knowing whether to multiply prevalence estimates by 1.25 or 2 can have important implications for estimating tax revenues. Thus, jurisdictions should seriously consider validating the responses from a sample of their respondents.
Collect information about market transactions
Understanding the price consumers pay for cannabis in legal and illegal markets is critical for describing cannabis markets, projecting the impact of legal changes, informing implementation decisions and conducting rigorous policy evaluations. Indeed, the effect of cannabis legalization on the price for marijuana (e.g. via changes in production/distribution costs and taxes) will have important implications for consumption, government budgets and the size of the illicit market [22,26]. While price information is not typically available from suppliers, it can be obtained from consumers through survey questionnaires. For example, one could ask (as is carried out in the US National Survey on Drug Use and Health—NSDUH) how much people spent on cannabis the last time they purchased and how much cannabis they received. Collecting this type of information is critical for conducting research on the sensitivity of consumption to changes in price (what economists refer to as the price elasticity of demand). Globally, very little information is available about how a price change influences the amount of cannabis being consumed; most research tells us how changes in prices influence the prevalence of use, not the amount consumed [46,47].
Obtaining information from the consumer about how the cannabis product was obtained is important for understanding the market and diversion. The NSDUH survey has included a cannabis market module since 2002, which asks respondents about who sold them the cannabis they most recently used (‘a friend’, ‘a relative or family member’ or ‘someone I had just met or didn’t know well’) and where they made the purchase (‘inside a public building, such as a store, restaurant’, ‘inside a school building’, ‘outside on school property’, ‘inside a home, apartment, or dorm’ or ‘outside in a public area, such as a parking lot’ or ‘some other place’ [48,49] The survey should have added specific choices about medical dispensaries or collectives years ago, and if it is updated it should also include ‘state-legal outlet in the state where I live’ and ‘State-legal outlet in a state where I do not live’.
If jurisdictions allow suppliers legally, it is possible to learn about these transactions from those who are producing, selling and purchasing cannabis in a legal market. If jurisdictions require producers, processors and retailers to submit data to ‘seed-to-sale’ tracking systems, enormous amounts can be learned about the supply chain, markups and firm responses to various taxes and regulations. This would provide information about the market after the policy change, but will be inadequate for assessing the impact of changing the law to allow supply. None the less, valuable insights can be gleaned about how a particular model of supply is operating. Further, if potency testing information is also incorporated into the system, this can inform us about trends in price per unit of THC (and other cannabinoids) and price elasticity of demand after legalization. While the seed-to-sale systems in Colorado and Washington do not allow retail transactions to be linked to specific individuals, retailers who create ‘loyalty card’-type programs will be able to gain tremendous insights into consumer behaviors [50,51].
In jurisdictions where there are legal protections for purchasing cannabis, it will be critical to not only track the locations of licensees, but also when they start, and possibly stop, operating. Studies of retail-outlet density for alcohol provide useful insights and it will probably do the same for cannabis; however, this literature is often criticized, as it often only includes the license data, not the actual dates of operation.
CONCLUSION
As of August 2016, two countries have passed laws to legalize large-scale cannabis production for non-medical purposes at the national (Uruguay) or subnational level (four US states), and another country (Canada) has declared its interest in doing the same [52]. At least nine other countries have passed laws to allow cannabis to be produced and distributed for medicinal purposes. Many of these changes have occurred since 2010, and we expect other countries to follow.
It is critical that these changes in cannabis laws be evaluated rigorously, but finding appropriate control groups will prove challenging in many places. In addition, the existing data infrastructure for properly evaluating these changes is weak. This paper offers a few ideas for improving information about cannabis consumption and market transactions, but evaluations of these changes should not focus exclusively upon cannabis use. Even if relaxing supply laws increases heavy cannabis consumption, that does not mean that the policy change is a net negative; the consequences of cannabis policy change will be shaped by how it affects quantity consumed, mode of consumption and the consumption of alcohol, tobacco and other substances [7]. In addition, there are other outcomes of interest that could be considered, such as the size of the black market, the effects on government budgets, criminal justice outcomes (ranging from expenditures to the consequences of having a criminal record to police-community relations) and pleasure.
Acknowledgments
We thank Jon Caulkins, Rob MacCoun, Mafalda Paradal, Bryce Pardo, Peter Reuter, Jirka Taylor and three anonymous reviewers for their comments and suggestions. This work was supported by NIDA (R01DA03269304) and reflects only the views of the authors.
Footnotes
Declaration of interests
None.
References
- 1.MacCoun RJ, Reuter P. Drug War Heresies: Learning From Other Vices, Times, and Places. New York: Cambridge University Press; 2001. [Google Scholar]
- 2.MacCoun RJ, Reuter P. Assessing drug prohibition and its alternatives: a guide for agnostics. Ann Rev Law Soc Sci. 2011;7:61–78. [Google Scholar]
- 3.Pacula R, MacCoun R, Reuter P, Chriqui J, Kilmer B, Harris K, et al. What does it mean to decriminalize marijuana? A cross-national empirical examination. Adv Health Econ Health Serv Res. 2005;16:347–69. [PubMed] [Google Scholar]
- 4.Room R, Fischer B, Hall W, Lenton S, Reuter P. Cannabis Policy: Moving Beyond the Stalemate. Oxford: Oxford University Press; 2010. [Google Scholar]
- 5.MacCoun RJ, Saiger AJ, Kahan JP, Reuter P. Drug Policies and Problems: The Promise and Pitfalls of Cross-National Comparison. Santa Monica, CA: RAND; 1993. [Google Scholar]
- 6.Kilmer B, Reuter P, Giommoni L. What can be learned from cross-national comparisons of data on illegal drugs? Crime Justice. 2015;44:227–557. [Google Scholar]
- 7.Caulkins JP, Hawken A, Kilmer B, Kleiman M. Marijuana Legalization: What Everyone Needs To Know. New York: Oxford University Press; 2012. [Google Scholar]
- 8.Eastwood N, Fox E, Rosmarin A. A Quiet Revolution Drug Decriminalisation Across the Globe. London: 2016. Release. [Google Scholar]
- 9.Kilmer B, Kruithof K, Pardal M, Caulkins JP, Rubin J. Multinational Overview of Cannabis Production Regimes. Cambridge, UK: RAND; 2013. [Google Scholar]
- 10.BBC. Colombia fully legalises medical marijuana. Available at: http://www.bbc.com/news/world-latin-america-35165169 (accessed 16th August 2016)
- 11.Edwards J. Medicinal marijuana to be legalised in Victoria in Australian first. Available at: http://www.abc.net.au/news/2015-10-06/locally-grown-marijuana-to-be-legalised-in-vic-toria-medical/6830892 (accessed 16 August 2016)
- 12.Caulkins JP, Kilmer B, Kleiman M. Marijuana legalization: What everyone needs to know. Second. New York: Oxford University Press; 2016. [Google Scholar]
- 13.National Conference of State Legislatures. State medical marijuana laws. Available at: http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx (accessed 16 August 2016)
- 14.Reuters. Chile opens Latin America’s largest medical marijuana farm. Available at: http://www.nbcnews.com/news/latino/chile-opens-latin-america-s-largest-medical-marijuana-farm-n500301 (accessed 16 August 2016)
- 15.Státní Agentura pro Konopí pro Léčebné Použití [State Agency for Medical Cannabis] Do lékáren může zamířit první české léčebné konopí. Available at: http://www.sakl.cz/footer/archiv-novinek/do-lekaren-muze-zamirit-prvni-ceske-lecebne-konopi ((accessed 16 August 2016)
- 16.Malhorta A. Is it legal to get high on bhang in India? Wall Street Journal. 2015 Mar 6; Available at: http://blogs.wsj.com/indiarealtime/2015/03/06/is-it-legal-to-get-high-on-bhang-in-india/ (accessed 16 August 2016)
- 17.Pardo B. Jamaica and its widely praised ganja reform are at a crossroads. El Post Daily. 2016 Mar 1; Available at: http://www.samefacts.com/2016/03/drug-policy/jamaica-and-its-widely-praised-ganja-reform-are-at-a-crossroads/ (accessed 16th August 2016)
- 18.Ramsey G. With seeds planted, cannabis sales in Uruguay could start in late. 2016 Available at: http://www.wola.org/commentary/with_seeds_planted_cannabis_sales_in_uruguay_could_start_in_late_2016 (accessed 16 August 2016)
- 19.Caulkins JP, Kilmer B. Considering marijuana legalization carefully: insights for other jurisdictions from analysis for Vermont. Addiction. 2016 doi: 10.1111/add.13289. [DOI] [PubMed] [Google Scholar]
- 20.Office of Medical Cannabis. Medical Cannabis. 2016 Available at: https://www.cannabisbureau.nl/english/medicinal-cannabis (accessed 16 August 2016)
- 21.Pacula RL, Kilmer B, Wagenaar AC, Chaloupka FJ, Caulkins JP. Developing public health regulations for marijuana: lessons from alcohol and tobacco. Am J Public Health. 2014;104:1021–8. doi: 10.2105/AJPH.2013.301766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Caulkins JP, Kilmer B, Kleiman MA, MacCoun RJ, Midgette G, Oglesby P, et al. Considering Marijuana Legalization: Insights for Vermont and Other Jurisdictions. Santa Monica, CA: RAND; 2015. [Google Scholar]
- 23.Pacula RL, Sevigny EL. Natural experiments in a complex and dynamic environment: the need for a measured assessment of the evidence. J Policy Anal Manage. 2014;33:232–5. doi: 10.1002/pam.21730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pacula RL, Powell D, Heaton P, Sevigny EL. Assessing the effects of medical marijuana laws on marijuana use: the devil is in the details. J Policy Anal Manage. 2015;34:7–31. doi: 10.1002/pam.21804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Smart R. The kids aren’t alright but older adults are just fine: effects of medical marijuana market growth on substance use and abuse. Available at: http://papers.ssrn.com/sol3/papers.cfm?abstract_id=2574915 (accessed 16 August 2016)
- 26.Kilmer B, Caulkins JP, Pacula RL, MacCoun RJ, Reuter P. Altered state? Assessing How Marijuana Legalization in California Could In fluence Marijuana Consumption and Public Budgets. Santa Monica, CA: RAND; 2010. [Google Scholar]
- 27.Burns RM, Caulkins JP, Everingham SS, Kilmer B. Statistics on cannabis users skew perceptions of cannabis use. Front Psychiatry. 2013;4:138. doi: 10.3389/fpsyt.2013.00138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Korf DJ, Benschop A, Wouters M. Differential responses to cannabis potency: a typology of users based on self-reported consumption behaviour. Int J Drug Policy. 2007;18:168–76. doi: 10.1016/j.drugpo.2006.08.002. [DOI] [PubMed] [Google Scholar]
- 29.Kilmer B, Caulkins JP, Midgette G, Dahlkemper L, MacCoun RJ, Liccardo PR. Before the Grand Opening: Measuring Washington State’s Marijuana Market in the Last Year Before Legalized Commercial Sales. Santa Monica, CA: RAND; 2013. [Google Scholar]
- 30.van der Pol P, Liebregts N, de Graaf R, Korf DJ, van den Brink W, van Laar M. Predicting the transition from frequent cannabis use to cannabis dependence: a three-year prospective study. Drug Alcohol Depend. 2013;133:352–9. doi: 10.1016/j.drugalcdep.2013.06.009. [DOI] [PubMed] [Google Scholar]
- 31.van Laar M, Frijns T, Trautmann F, Lombi L. Cannabis market: user types, availability and consumption estimates. In: Trautman F, Kilmer B, Turnbull P, editors. Further Insights into Aspects of the Illicit EU Drugs Market. Luxembourg: Publications Office of the European Union; 2013. pp. 73–182. [Google Scholar]
- 32.Light MK, Orens A, Lewandowski B, Pickton T. Market Size and Demand for Marijuana in Colorado. Denver: Colorado Department of Revenue; 2014. [Google Scholar]
- 33.Hall W, Pacula RL. Cannabis Use and Dependence: Public Health and Public Policy. Melbourne: Cambridge University Press; 2003. [Google Scholar]
- 34.Lakhdar CB, Leleu H, Vaillant NG, Wolff FC. Efficiency of purchasing and selling agents in markets with quality uncertainty: the case of illicit drug transactions. Eur J Operat Res. 2013;226:646–57. [Google Scholar]
- 35.Burgdorf JR, Kilmer B, Pacula RL. Heterogeneity in the composition of marijuana seized in California. Drug Alcohol Depend. 2011;117:59–61. doi: 10.1016/j.drugalcdep.2010.11.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sevigny EL, Pacula RL, Heaton P. The effects of medical marijuana laws on potency. Int J Drug Policy. 2014;25:308–19. doi: 10.1016/j.drugpo.2014.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Pacula RL, Jacobson MJ, Maksabedian E. In the weeds: a baseline view of marijuana use among legalizing states and their neighbors. Addiction. 2016 doi: 10.1111/add.13282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Guttmannova K, Lee CM, Kilmer JR, Fleming CB, Rhew IC, Kosterman R, et al. Impacts of changing marijuana policies on alcohol use in the United States. Alcohol Clin Exp Res. 2016;40:33–46. doi: 10.1111/acer.12942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ramaekers JG, Berghaus G, van Laar M, Drummer OH. Dose related risk of motor vehicle crashes after cannabis use. Drug Alcohol Depend. 2004;73:109–19. doi: 10.1016/j.drugalcdep.2003.10.008. [DOI] [PubMed] [Google Scholar]
- 40.Hartman RL, Huestis MA. Cannabis effects on driving skills. Clin Chem. 2013;59:478–92. doi: 10.1373/clinchem.2012.194381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Turner CF, Ku L, Rogers SM, Lindberg LD, Pleck JH, Sonenstein FL. Adolescent sexual behavior, drug use, and violence: increased reporting with computer survey technology. Science. 1998;280:867–73. doi: 10.1126/science.280.5365.867. [DOI] [PubMed] [Google Scholar]
- 42.Harrison L, Martin SS, Enev T, Harrington D. Comparing Drug Testing and Self-Report of Drug Use Among Youths and Young Adults in the General Population. Rockville, MD: Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2007. [Google Scholar]
- 43.Harrison L, Hughes A. The Validity of Self-Reported Drug Use: Improving the Accuracy of Survey Estimates. Rockville, MD: National Institute on Drug Abuse; 1997. (NIH Publication No. 97-4147, NIDA Research Monograph 167). [PubMed] [Google Scholar]
- 44.Fendrich M, Johnson TP, Wislar JS, Hubbell A, Spiehler V. The utility of drug testing in epidemiological research: results from a general population survey. Addiction. 2004;99:197–208. doi: 10.1111/j.1360-0443.2003.00632.x. [DOI] [PubMed] [Google Scholar]
- 45.Hser YI, Maglione M, Boyle K. Validity of self-report of drug use among STD patients, ER patients, and arrestees. Am J Drug Alcohol Abuse. 1999;25:81–91. doi: 10.1081/ada-100101847. [DOI] [PubMed] [Google Scholar]
- 46.Gallet CA. Can price get the monkey off our back? A meta-analysis of illicit drug demand. Health Econ. 2014;23:55–68. doi: 10.1002/hec.2902. [DOI] [PubMed] [Google Scholar]
- 47.Pacula RL, Lundberg R. Why changes in price matter when thinking about marijuana policy: A review of the literature on the elasticity of demand. Public Health Rev. 2014;35:1. doi: 10.1007/BF03391701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Caulkins JP, Pacula RL. Marijuana markets: inferences from reports by the household population. J Drug Issues. 2006;36:173–200. [Google Scholar]
- 49.Davenport S, Caulkins JP. Evolution of the United States marijuana market in the decade of liberalization before full legalization. J Drug Issues. 2016 doi: 10.1177/0022042616659759. [DOI] [Google Scholar]
- 50.Caulkins JP, Cannabis policy research agenda Comments presented at New York University. 2016 Available at: https://www.youtube.com/watch?v=xRi-8RLrcHg.
- 51.Headset. What does the average cannabis consumer look like? Available at: http://headset.io/blog/what-does-the-average-cannabis-consumer-look-like (accessed 16 August 2016)
- 52.Associated Press. Canada to introduce marijuana legislation in Spring. 2017 Available at: http://www.denverpost.com/2016/04/20/canada-to-introduce-marijuana-legislation-in-spring-2017/ (accessed 16 August 2016)