

Abstract
There have been reports of late discharge of gallstones through operative wounds after spillage into the peritoneal cavity during laparoscopic cholecystectomy and after the development of spontaneous cholecystocutaneous fistulae. However, spontaneous discharge of gallstones from the tract of a percutaneous cholecystostomy or percutaneous drainage of a perforated gall bladder has not, to the best of our knowledge, been reported previously. We report a case in which a patient who had a percutaneous drain inserted for a perforated gall bladder discharged 34 gallstones from the tract after removal of the 7-F pigtail catheter.
Keywords: Gallstones, Gallbladder perforation, Percutaneous drainage, Spontaneous extrusion, CT
Introduction
A cholecystocutaneous fistula is a rare complication of complicated gallstone disease1 and the discharge of gallstones from a fistula tract is an even rarer event. There have been reports of late discharge of gallstones through operative wounds2,3 after spillage into the peritoneal cavity during laparoscopic cholecystectomy. A percutaneous cholecystostomy is used sometimes to drain the gall bladder in patients with acute cholecystitis in whom comorbidity precludes cholecystectomy. However, spontaneous discharge of gallstones from such a tract has, to the best of our knowledge, been unreported previously.
Case history
An 83-year-old woman was admitted with an ultrasound diagnosis of acute cholecystitis. She was treated with intravenous antibiotics (piperacillin and tazobactam) and intravenous fluids. She remained septic (white cell count 22.4 × 109 cells/mm3, C-reactive protein 380 mg/l, bilirubin 28 μol/l, alkaline phosphatase 443 iu/l, alanine transaminase 65 iu/l, lactate 1.1mmol/l) and blood culture grew Streptococcus milleri. Despite being on appropriate antibiotics, her clinical condition did not improve. Computed tomography revealed a 7 × 7cm sub-hepatic abscess containing multiple gas locules and gallstones, suspicious of a perforated gallbladder (Fig 1). As multiple cardiovascular comorbidities precluded surgery, a percutaneous 7-F pigtail drain was inserted into the sub-hepatic collection under ultrasound guidance. This drained 70 ml of pus initially. Her clinical condition improved and the pus stopped draining after 5 days. The drain was removed and she was discharged, to be readmitted after 48 hours complaining of solid matter discharging from the drain sinus tract. A gallstone was visible at the cutaneous end of the tract (Fig 2, top) and eventually a total of 34 gallstones were extruded (Fig 2, bottom). Repeat imaging showed no further collections or stones. She was ultimately discharged 4 days after readmission and continues to be well.
Figure 1.
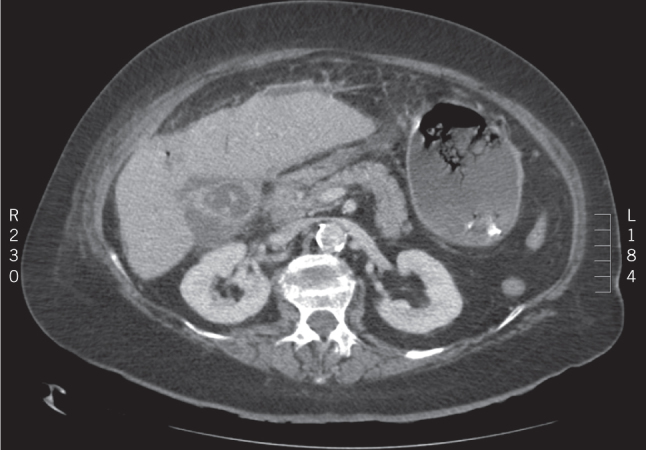
Computed tomography image showing a 7 × 7cm sub-hepatic abscess containing gallstones.
Figure 2.

A gallstone was visible at the cutaneous end of the tract (top); a total of 34 gallstones were extruded (bottom).
Discussion
Cholecystocutaneous fistula is a rare complication of neglected biliary tract disease. The increased pressure in the gallbladder because of cystic duct obstruction impairs blood flow and lymphatic drainage, causing mural necrosis and perforation. Nayman, in 1963, described a ‘burrowing abscess’ of the abdominal wall because of gallbladder inflammation leading to cutaneous fistulation.4 Gangrene of an acutely inflamed gallbladder can occur in up to 20% of patients5 and can sometimes result in transmural perforation and spillage of gallstones.6
Our patient had a perforation of her gallbladder with spillage of stones and responded well to percutaneous drainage and antibiotic therapy. Although it is unusual for peritoneocutaneous tracts to become established so early after insertion of siliconised percutaneous drains, this apparently happened in our patient, facilitating extrusion of the spilled gallstones. This spontaneous event was fortuitous, as it led to resolution of her condition, especially as surgical intervention was an extremely high-risk option. Resolution was also facilitated by the fact that the cystic duct was probably blocked, as indicated by absence of bile in the drain effluent and lack of sub-hepatic fluid collections on subsequent scans.
References
- 1.Vasanth A, Siddiqui A, O’Donnell K. Spontaneous cholecystocutaneous fistula. South Med J 2004; : 183–185. [DOI] [PubMed] [Google Scholar]
- 2.Zehetner J, Shamiyeh A, Wayand W. Lost gallstones in laparoscopic cholecystectomy: all possible complications. Am J Surg 2007; : 73–78. [DOI] [PubMed] [Google Scholar]
- 3.Woodfield JC, Rodgers M, Windsor JA. Peritoneal gallstones following laparoscopic cholecystectomy: incidence, complications, and management. Surg Endosc 2004; : 1,200–1,207. [DOI] [PubMed] [Google Scholar]
- 4.Nayman J. Empyema necessitatis of the gall-bladder. Med J Aust 1963; : 429–430. [PubMed] [Google Scholar]
- 5.Macafee DAL, Humes DJ, Bouliotis G et al. Prospective randomized trial using cost–utility analysis of early versus delayed laparoscopic cholecystectomy for acute gallbladder disease. Br J Surg 2009; : 1,031–1,040. [DOI] [PubMed] [Google Scholar]
- 6.Walton TJ, Dhingsa R, Kaye PV et al. Imaging after medically managed severe acute cholecystitis. Gut 2009; : 421, 472. [DOI] [PubMed] [Google Scholar]