

Abstract
Background
Empirical evidence investigating heterogeneous impact of retirement on mental health depending on social backgrounds is lacking, especially among older adults.
Methods
We examined the impact of changes in working status on changes in mental health using Japanese community-dwelling adults aged ≥65 years participating in the Japan Gerontological Evaluation Study between 2010 and 2013 (N = 62,438). Between-waves changes in working status (“Kept working”, “Retired”, “Started work”, or “Continuously retired”) were used to predict changes in depressive symptoms measured by the Geriatric Depression Scale. First-difference regression models were stratified by gender, controlling for changes in time-varying confounding actors including equivalised household income, marital status, instrumental activities of daily living, incidence of serious illnesses and family caregiving. We then examined the interactions between changes in working status and occupational class, changes in marital status, and post-retirement social participation.
Results
Participants who transitioned to retirement reported significantly increased depressive symptoms (β = 0.33, 95% CI: 0.21–0.45 for men, and β = 0.29, 95% CI: 0.13–0.45 for women) compared to those who kept working. Men who were continuously retired reported increased depressive symptoms (β = 0.13, 95% CI: 0.05–0.20), whereas males who started work reported decreased depressive symptoms (β = −0.20, 95% CI: -0.38–-0.02). Men from lower occupational class (compared to men from higher class) reported more increase in depressive symptoms when continuously retired (β = −0.16, 95% CI: -0.25–-0.08). Those reporting recreational social participation after retirement appeared to be less influenced by transition to retirement.
Conclusions
Retirement may increase depressive symptoms among Japanese older adults, particularly men from lower occupational class backgrounds. Encouraging recreational social participation may mitigate the adverse effects of retirement on mental health of Japanese older men.
Electronic supplementary material
The online version of this article (doi:10.1186/s12889-017-4427-0) contains supplementary material, which is available to authorized users.
Keywords: Retirement, Mental health, Social participation, Fixed-effects, Japan, Older adults
Background
Population aging is occurring worldwide and an increasing number of older adults are engaging in work in late life. Japan is experiencing the fastest rate of population ageing in the world. In Japan, the labor force participation rate among people aged 65 years or older was 21.3% in 2014, which ranked 7th among all OECD countries [1], and the population of older workers increased from 4.8 million in 2004 to 6.8 million in 2014 [2]. To maintain both the quality of life of each older individual and the financial sustainability of healthcare and long-term care systems, preventing physical and mental impairments is the key goals of public health measures for the aged [3]. Specifically, the maintenance of mental health counts as it could be strongly affected by the stressful life events that are likely to happen in older ages. Among those life events, in this study, we focused on retirement, the major events that most people experience.
Transition from work to retirement is a major life event in most people’s lives. However, there is controversy about the impact of retirement on mental health [4]. While many studies done in European countries suggest that retirement is beneficial to mental health [5–8] or has no health impact [9–11], results from some studies in Asian populations indicate the opposite, i.e. the transition to retirement is detrimental to mental health [12, 13]. These geographic differences in the association between retirement and mental health may be partly due to the differences in employment conditions and how retirements are culturally perceived by people in each region.
There are several potential mechanisms through which retirement may have adverse impact on mental health. Above and beyond the immediate reduction in income, social role theory posits that retirement results in the loss of many non-financial benefits of work, such as opportunities for health-promoting social contacts and access to social support that can buffer the adverse effects of stress [14–16]. Activity theory also posits that the transition to retirement results in reduced wellbeing for individuals for whom work provided meaning in life [17].
Moreover, the impact of retirement on mental health may not be universal and could vary between individuals depending on his/her occupational class or social situation (e.g. the presence of social support in the home environment from a marital partner) [4, 6, 18, 19]. In addition, social participation after retirement may compensate for any adverse effect of retirement stemming from loss of sense of meaning in life, which has been suggested to be linked to mental health [4, 12, 13, 20]. However, the potential impact of other types of social participation such as hobby clubs remains unknown.
In the present study, we sought to evaluate [1] the association between changes in working status and changes in depressive symptoms in a cohort of community-dwelling Japanese older adults, [2] whether the association can be mediated by changes in social contacts and social support, [3] the interaction between changes in working status and occupational class, changes in marital status, and social participation after retirement.
Methods
Data
We used data from the 2010 and 2013 waves of Japan Gerontological Evaluation Study (JAGES) project. Detailed descriptions of JAGES are available elsewhere [21, 22]. In brief, the JAGES conducted postal surveys targeting physically and cognitively independent community-dwelling older adults aged ≥65 years in Japan. The baseline survey was conducted in 2010 and we sampled 112,123 older adults residing in 31 municipalities in Japan (Response rate = 66.3%). The second survey was conducted in 2013 in which we sampled 137,736 older adults residing in 30 municipalities in Japan (Response rate = 71.1%). Twenty-four municipalities participated in both years. Sixty-two thousand four hundred thirty-eight participants responded to both surveys.
The 2013 wave of JAGES dataset consisted of five modules. The question inquiring about participants’ sense of meaning in life was measured only in one of the five modules, which was only mailed to one-fifth of the total sample. We used respondents to this module (N = 12,487) to test the interaction between retirement and two types of social participation, as well as whether a sense of meaning in life mediated this relationship. All variables used in this study were self-reported. Ethical approval of this study was obtained from the ethics review board of the University of Tokyo Medical School.
Measurement
Changes in depressive symptoms
Depressive symptoms were measured at both waves using the validated Japanese short version of the Geriatric Depression Scale (GDS-15) [23] Total scores could range from 0 to15, where higher scores indicate more depressive symptoms. GDS-15 has been commonly used as a screening tool for depression among older adults with a cutoff of 5 or above to indicate clinical depression [23, 24]. We used changes in total GDS-15 scores from 2010 to 2013 as the continuous outcome variable in this study.
Changes in working status
Information on working status (either “currently working” or “retired and not currently working”) was collected in both 2010 and 2013. Thus, no one among the subjects was considered to be partially retired. We categorized subjects as “Kept working (working/working)”, “Retired (working ➔ not working)”, “Started work (not working ➔ working)”, or “Continuously retired (not working ➔ not working)” based on patterns of changes in working status from 2010 to 2013.
Changes in social contacts and social support
We used two variables to tap changes in social contacts. First, we asked the number of friends and acquaintances the subjects met in the past month at both waves, and then, changes in the answers were modeled as a continuous variable. Second, we asked subjects “What is the relationship between you and the person you often meet?” At each wave, we focused on individuals who maintained social contacts with colleagues in the workplace. As for social support, we collected information at both waves on whether or not subjects received emotional (‘Do you have anyone who will listen to you when you have worries and complains?’) and instrumental (‘Do you have anyone who can take care of you when you are sick in bed for a few days?’) social support from their friends. Between-wave changes in perception of social supports from friends were made into a categorical variable.
Occupational class
The occupation that subjects had engaged in for the longest period of time was asked at both waves. Since it is unlikely that the longest job of older people aged 65 years or older change within 3 years (from 2010 to 2013), we treated this as a time-invariant variable. Professionals and managers were categorized as “higher occupational class”. Clerical support workers, service and sales workers, craft and related trades workers, skilled agricultural, forestry, and fishery workers, and others were categorized as “lower occupational class”.
Social participation/a sense of meaning in life
Participation in different clubs/groups was asked at both waves. We defined “social participation with roles” as participation in volunteering clubs or neighborhood councils. We defined “recreational social participation” as participation in sports organizations, hobby clubs, or older adults clubs. A sense of meaning in life was measured in 2013 by asking “Do you feel a sense of meaning in life” (yes/no).
Covariates
Changes in equivalised household income, marital status, instrumental activities of daily living, incidence of serious illnesses and family caregiving were treated as time-varying covariates. These variables are potential confounding factors, which could have influence on both retirement decision and mental health. Household income at each wave was equivalised in order to adjust for the number of members within households. Marital status of subjects at each wave was defined either “married” or “non-married (including being widowed, divorced, or single)”. Subjects’ instrumental activities of daily living (IADL) were measured using the Tokyo Metropolitan Institute of Gerontology (TMIG) Index of Competence as a broad indicator of physical health. TMIG Index of Competence was validated using the data of Japanese older community residents [25] and its total scores could range from 0 to13, where higher scores indicates more independency in daily livings. Incidence of serious illnesses and need for caregiving was assessed in 2013 by administering a checklist for events occurring in the past year.
Statistical analysis
As for missing values in some variables used in the analysis, we executed multiple imputation by chained equation method to create 100 data sets without missing value. We used the FCS statement of the MI procedure in SAS version 9.3 to create imputed data sets. Then, we excluded those who indicated depression in 2010 (GDS score of 5 or more as described below), those who never worked, and those who answered inconsistently to the question about the occupational class at the two time points. We ran all models using each data set and, using MIANALYZE procedure, we obtained the final estimates combining 100 estimates derived from 100 analyses.
We used first-difference models stratified by gender to investigate the main effects of changes in working status on changes in depressive symptoms with full-sample data (Model 1). The first-difference models tool the changes in all variables in the models, which enable to can control for all observed and unobserved time-invariant confounders (e.g. age and education) by cancelling out the estimates of time-invariant confounders. In model 2, we added variables regarding changes in social contacts and social support to test whether these changes could explain the association between changes in working status and changes in depressive symptoms. In model 3, we added an interaction term between changes in working status and occupational class. In model 4, we added an interaction term between transition to retirement and changes in marital status.
In the analysis involving a sense of meaning in life, we analyzed only one of the five sub-samples of JAGES data because it is the only module that contains information on participants’ sense of purpose in life. In model 5, we used the first-difference model again to test the main effect of changes in working status on depressive symptoms among this sub-population. In the model 6, we added the interaction term between transition to retirement and two types of social participation. Lastly, in model 7, we added sense of meaning in life as a covariate to check whether it mediated the interaction between retirement and social participation.
We stratified data by gender instead of modeling gender interaction effects to make it easy to interpret our results and prevent the problems of multicollinearity on interaction terms.
Results
Descriptive analysis showed that subjects in the full-sample dataset and the sub-sample dataset were broadly similar in terms of their background characteristics (Table 1). Nearly a quarter of male and female subjects indicated depressive symptoms at baseline.
Table 1.
Demographic Characteristics of Subjects from Full-dataset and Sub-dataset by Gender
| Full-sample | Sub-sample | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Men | Women | Men | Women | |||||||
| N = 28,868 | N = 33,569 | N = 5866 | N = 6621 | |||||||
| Mean | SD | Mean | SD | p-value | Mean | SD | Mean | SD | p-value | |
| Age in 2010 | 72.9 | 5.6 | 73.1 | 5.6 | <.0001 | 72.9 | 5.6 | 73.1 | 5.6 | 0.02 |
| GDS-15 score change (2010 → 2013) | 0.1 | 2.4 | 0.03 | 2.4 | 0.0005 | 0.1 | 2.5 | −0.01 | 2.3 | 0.02 |
| n | % | n | % | n | % | n | % | |||
| Working status in 2010 | ||||||||||
| Working status | 8095 | 30.3 | 5287 | 19.2 | <.0001 | 1687 | 31.1 | 1058 | 19.5 | <.0001 |
| Not working | 17,530 | 65.6 | 16,556 | 60 | 3510 | 64.7 | 3231 | 59.6 | ||
| Never worked | 1087 | 4.1 | 5730 | 20.8 | 232 | 4.3 | 1133 | 20.9 | ||
| Missing | 2156 | 5996 | 437 | 1199 | ||||||
| Depression in 2010 | ||||||||||
| Having depression in 2010 | 6353 | 25.5 | 6816 | 25.5 | 0.84 | 1340 | 26.4 | 1354 | 25.7 | 0.4 |
| Not having depression in 2010 | 18,602 | 74.5 | 19,878 | 74.5 | 3730 | 73.6 | 3913 | 74.3 | ||
| Missing | 3913 | 6875 | 796 | 1354 | ||||||
| Household income in 2010 (10,000 Japanese Yen) | ||||||||||
| < 300 | 12,129 | 45.6 | 15,051 | 54 | <.0001 | 2429 | 44.8 | 2921 | 53.2 | <.0001 |
| 300–600 | 9759 | 36.7 | 8427 | 30.2 | 2027 | 37.4 | 1676 | 30.5 | ||
| < 600 | 4711 | 17.7 | 4393 | 15.8 | 969 | 17.9 | 897 | 16.3 | ||
| Missing | 2269 | 5698 | 441 | 1127 | ||||||
| Marital status in 2010 | ||||||||||
| Married | 24,608 | 87.9 | 19,790 | 61.3 | <.0001 | 5007 | 88 | 3894 | 61.1 | <.0001 |
| Non-married | 3374 | 12.1 | 12,520 | 38.8 | 685 | 12 | 2484 | 39 | ||
| Missing | 886 | 1259 | 174 | 243 | ||||||
| IADL in 2010 | ||||||||||
| 13 | 9401 | 36.6 | 15,590 | 53.1 | <.0001 | 1882 | 36 | 3052 | 52.7 | <.0001 |
| 10, 12 | 12,959 | 50.4 | 11,548 | 39.3 | 2642 | 50.5 | 2313 | 40 | ||
| ≤ 9 | 3351 | 13 | 2250 | 7.7 | 710 | 13.6 | 423 | 7.3 | ||
| Missing | 3157 | 4181 | 632 | 833 | ||||||
| The number of friends subjects met in the past 1 month in 2010 | ||||||||||
| 0 | 2041 | 7.6 | 1065 | 3.5 | <.0001 | 419 | 7.7 | 198 | 3.3 | <.0001 |
| 1, 5 | 11,426 | 42.5 | 12,589 | 40.8 | 2302 | 42.3 | 2495 | 41.1 | ||
| 6- | 13,396 | 49.9 | 17,236 | 55.8 | 2728 | 50.1 | 3385 | 55.7 | ||
| Missing | 2005 | 2679 | 417 | 543 | ||||||
| Colleague as a friend who subjects met frequently in 2010 | ||||||||||
| Having colleague as a friend | 11,439 | 42.4 | 8027 | 25.4 | <.0001 | 2365 | 43.2 | 1522 | 24.4 | <.0001 |
| Not having colleague as a friend | 15,563 | 57.6 | 23,625 | 74.6 | 3116 | 56.9 | 4713 | 75.6 | ||
| Missing | 1866 | 1917 | 385 | 386 | ||||||
| Emotional social support from friends in 2010 | ||||||||||
| Having emotional social support | 7233 | 26.6 | 15,156 | 47.9 | <.0001 | 1425 | 25.7 | 2974 | 47.9 | <.0001 |
| Not having emotional social support | 19,950 | 73.4 | 16,482 | 52.1 | 4112 | 74.3 | 3234 | 52.1 | ||
| Missing | 1685 | 1931 | 329 | 413 | ||||||
| Instrumental social support from friends in 2010 | ||||||||||
| Having instrumental social support | 632 | 2.3 | 2144 | 6.8 | <.0001 | 114 | 2.1 | 400 | 6.4 | <.0001 |
| Not having instrumental social support | 26,793 | 97.7 | 29,539 | 93.2 | 5454 | 97.8 | 5844 | 93.6 | ||
| Missing | 1444 | 1886 | 298 | 377 | ||||||
| Occupational class | ||||||||||
| Higher | 9265 | 36.2 | 3031 | 12.6 | <.0001 | 1879 | 36.5 | 605 | 12.9 | <.0001 |
| Lower | 16,325 | 63.8 | 20,940 | 87.4 | 3268 | 63.5 | 4083 | 87.1 | ||
| missing | 3153 | 6394 | 698 | 1326 | ||||||
| Social participation with roles in 2013 | ||||||||||
| Participated in social activities with roles | 6536 | 26.3 | 7361 | 27.8 | 0.001 | 1292 | 25.6 | 1461 | 28 | 0.005 |
| Not participated in social activities with roles | 18,346 | 73.7 | 19,132 | 72.2 | 3764 | 74.5 | 3754 | 72 | ||
| missing | 3986 | 7076 | 810 | 1406 | ||||||
| Recreational social participation in 2013 | ||||||||||
| Participated in recreational social activities | 11,714 | 46.5 | 16,067 | 58 | <.0001 | 2367 | 46.3 | 3167 | 57.9 | <.0001 |
| Not participated in recreational social activities | 13,458 | 53.5 | 11,657 | 42.1 | 2751 | 53.8 | 2304 | 42.1 | ||
| missing | 3696 | 5845 | 748 | 1150 | ||||||
| A sense of meaning in life in 2013 | ||||||||||
| Having a sense of meaning in life in 2013 | 4666 | 86.2 | 5036 | 84.2 | 0.003 | |||||
| Not having a sense of meaning in life in 2013 | 748 | 13.8 | 945 | 15.8 | ||||||
| missing | 452 | 640 | ||||||||
GDS-15 the short version of the Geriatric Depression Scale (ranging from 0 to 15, higher score indicates more depressive symptoms). Depression in 2010 was defined by GDS-15 score of 5 or above. Non-married includes being divorced, widowed, and single. IADL Instrumental activities of daily living (ranging from 0 to 13, higher score indicates more independency in daily livings). Higher occupational class = professionals and engineering, managers. Lower occupational class = clerical support workers, service and sales workers, craft and related trades workers, skilled agricultural, forestry, and fishery workers, others. Social participation with roles = volunteering clubs, neighborhood councils. Recreational social participation = sports organizations, hobby clubs, or older adults clubs. Full-sample: subjects from all of the five modules of JAGES. Sub-sample: subjects from only one of the five modules from JAGES that includes information on a sense of meaning in life. We used t-test for age and changes in GDS score and chi-square test for other variables to calculate p-values
For men, we observed significant increases in GDS score among those who transitioned to retirement (β = 0.33, 95% CI: 0.21–0.45) and those who were continuously retired (β = 0.13, 95% CI: 0.05–0.20) compared to those who kept working (Model 1 in Table 2). For women, we observed significant increases in GDS score among those who transitioned to retirement (β = 0.29, 95% CI: 0.13–0.45) compared to those who kept working. After including changes in social contacts and social support in Model 2, significant associations observed in Model 1 were overall unchanged and remained statistically significant.
Table 2.
Multiple linear regression of Changes in GDS score on change in working status by gender (full-sample)
| Independent variables | Dependent Variable: Changes in GDS-15 score from 2010 to 2013 | |||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | |||||||
| Men | Women | Men | Women | |||||
| β coefficient (95%CI) | ||||||||
| Changes in working status (2010–2013) | ||||||||
| Kept working | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Retired | 0.33 | (0.21, 0.45) | 0.29 | (0.13,0.45) | 0.33 | (0.21,0.45) | 0.28 | (0.12,0.44) |
| Started work | −0.20 | (−0.38, −0.02) | 0.10 | (−0.13,0.33) | −0.21 | (−0.39,-0.03) | 0.10 | (−0.13,0.33) |
| Continuously retired | 0.13 | (0.05, 0.20) | 0.05 | (−0.04,0.14) | 0.10 | (0.02,0.18) | 0.05 | (−0.03,0.14) |
| Changes in Equivalized household income (10,000 JPY) | −0.0004 | (−0.0007, −0.0002) | −0.0005 | (−0.0007,-0.0002) | −0.0004 | (−0.0007,-0.0002) | −0.0004 | (−0.0007,-0.0002) |
| Changes in IADL | −0.24 | (−0.26, −0.21) | −0.28 | (−0.31,-0.25) | −0.23 | (−0.25,-0.2) | −0.26 | (−0.3,-0.23) |
| Incidence of stressful life events in the past 1 year | ||||||||
| Serious illnesses | 0.59 | (0.47, 0.70) | 0.70 | (0.54,0.87) | 0.58 | (0.46,0.7) | 0.70 | (0.53,0.87) |
| Started family caregiving | 0.54 | (0.35, 0.73) | 0.55 | (0.38,0.72) | 0.54 | (0.34,0.73) | 0.55 | (0.38,0.72) |
| Changes in marital status | ||||||||
| Married – Married | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Married - Not married | 0.48 | (0.26, 0.70) | 0.15 | (−0.02,0.32) | 0.48 | (0.26,0.7) | 0.16 | (−0.01,0.33) |
| Not married – Married | −0.04 | (−0.45, 0.36) | 0.54 | (0.13,0.95) | −0.04 | (−0.44,0.37) | 0.51 | (0.11,0.92) |
| Not married - Not married | 0.20 | (0.08,0.31) | 0.11 | (0.04,0.18) | 0.21 | (0.09,0.33) | 0.11 | (0.04,0.18) |
| The number of friends subjects met in the past 1 month | −0.02 | (−0.03,-0.01) | −0.03 | (−0.04,-0.02) | ||||
| Colleagues as a friend who subjects met frequently | ||||||||
| Continuously having colleagues as a friend | Ref. | Ref. | Ref. | Ref. | ||||
| Lost colleagues as a friend | 0.01 | (−0.09,0.11) | 0.06 | (−0.06,0.19) | ||||
| Continuously not having colleagues as a friend | 0.08 | (0.004,0.16) | −0.003 | (−0.09,0.09) | ||||
| Newly had colleagues as a friend | 0.04 | (−0.08,0.15) | −0.03 | (−0.17,0.1) | ||||
| Emotional support from friends | ||||||||
| Continuously having emotinal social support from friends | Ref. | Ref. | Ref. | Ref. | ||||
| Lost emotional social support from friends | 0.16 | (0.04,0.28) | 0.16 | (0.04,0.27) | ||||
| Continuously not having emotional social support from friends | 0.21 | (0.12,0.3) | 0.12 | (0.04,0.2) | ||||
| Newly had emotional support from friends | 0.08 | (−0.03,0.19) | −0.01 | (−0.12,0.1) | ||||
| Instrumental support from friends | ||||||||
| Continuously having instrumental social support from friends | Ref. | Ref. | Ref. | Ref. | ||||
| Lost instrumental social support from friends | 0.23 | (−0.2,0.66) | 0.19 | (−0.05,0.42) | ||||
| Continuously not having instrumental social support from friends | 0.05 | (−0.32,0.42) | 0.06 | (−0.13,0.25) | ||||
| Newly had instrumental support from friends | −0.01 | (−0.42,0.41) | −0.08 | (−0.33,0.16) | ||||
GDS-15 the short version of the Geriatric Depression Scale (ranging from 0 to 15, higher score indicates more depressive symptoms). Subjects are those who did not show depression at baseline (GDS score < 5). IADL Instrumental activities of daily living (ranging from 0 to 13, higher score indicates more independency in daily livings). Non-married includes being divorced, widowed, and single. Data of full-sample (all of the 5 sub-versions of JAGES datasets) was used for these analysis
When including interaction terms (Additional file 1 : Table S1), we did not find any statistically clear evidence on that the association between changes in working status and GDS scores were altered by occupational class (Model 3), though there were tendency that the relative increase in GDS score among men who were continuously retired were smaller among high occupational classes than lower occupational class (β = −0.08, 95% CI: -0.22–0.07) (Fig. 1). There was no significant interaction between changes in working status and occupational class among women. We observed no significant interactions between transition to retirement and changes in marital status among men and women (Model 4).
Fig. 1.
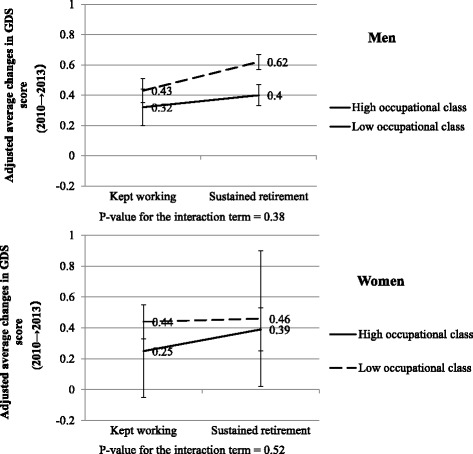
Adjusted average changes in GDS score by changes in working status and occupational class.
GDS: the short version of the geriatric depression scale (ranging from 0 to 15, higher score indicates more depressive symptoms). Adjusted for changes in time varying confounding factors including equivalised houshold income, IADL limitation, marital status, stressful life events, social relationships. Subjects are those who did not show depression at baseline (GDS score < 5). Occupational status: 1 = high (professionals and engineering, managers), 0 = low (clerical support workers, service and sales workers, craft and related trades workers, skilled agricultural, forestry, and fishery workers, others)
Analyses using the sub-dataset showed consistent results: significant increases in GDS score among men who transitioned to retirement (β = 0.40, 95% CI: 0.12–0.68) as well as men who were continuously retired (β = 0.29, 95% CI: 0.11–0.47) compared to men who kept working (Model 5 in Additional file 2: Table S2). Women who transitioned to retirement reported marginally significant increases in GDS scores (β = 0.32, 95% CI: -0.04–0.68, p = 0.09).
Although statistical evidence was weak but there was a trend among men and women that increase in depressive symptoms was less among those who participated in recreational social participation (β = −0.22, 95% CI: -0.72–0.29 for men, and β = −0.28, 95% CI: -0.92–0.37 for women) (Model 6 in Additional file 3: Table S3, Fig. 2 ). After additional adjustment for whether or not subjects have a sense of meaning in life (Model 7 in Additional file 3: Table S3), the magnitude of interaction effect between transition to retirement and recreational social participation among men considerably reduced (β = −0.05, 95% CI: -0.54–0.44), whereas it did not change among women (β = −0.27, 95% CI: -0.89–0.35). Notably, having a sense of meaning in life was strongly associated with increased depressive symptoms among men and women (β = −2.66, 95% CI: -3.00–-2.32 for men, and β = −1.84, 95% CI: -2.11-1.57 for women).
Fig. 2.
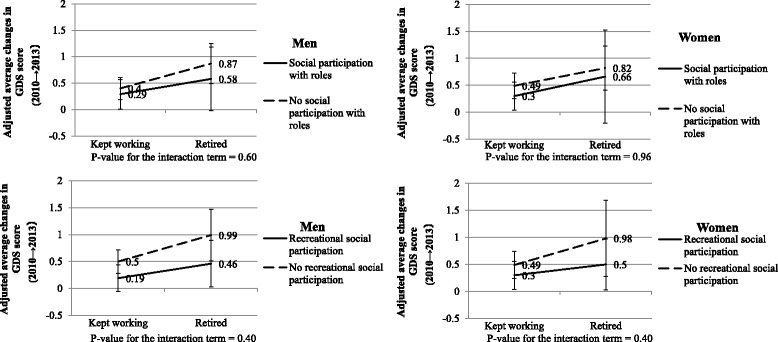
Adjusted average changes in GDS score by changes in working status and post-retirement social participation.
GDS: the short version of the geriatric depression scale (ranging from 0 to 15, higher score indicates more depressive symptoms). Adjusted for changes in time varying confounding factors including equivalised houshold income, IADL limitation, marital status, stressful life events, social relationships. Subjects are those who did not show depression at baseline (GDS score < 5). Social participation with roles includes volunteering clubs and neighborhood councils. Recreational social participation includes sports organizations, hobby clubs, and older adults clubs
Discussion
We summarize our key findings. First, the transition to retirement in both men and women and sustained retirement in men were associated with increased depressive symptoms among Japanese older adults. Second, the associations between retirement and increased depressive symptoms remained statistically significant after additionally adjusting for changes in social contacts and social support, suggesting that they did not mediate the impact of retirement on mental health at least among Japanese older adults. Third, there was a statistically non-significant trend that men from higher occupational class backgrounds appeared to be less influenced by sustained retirement, whereas we did not find such a trend among women. Fourth, we found no interaction between changes in working status and changes in marital status. Finally, there was a statistically non-significant trend that men and women who reported recreational social participation after retirement appeared to be less adversely impacted by retirement. Importantly, the magnitude of interaction effect between transition to retirement and post-retirement recreational social participation substantially reduced only among men after additionally adjusting for a sense of meaning in life. This, if causal, may suggest that having a sense of meaning in life through social participation may be crucial in mitigating the adverse impact of retirement on mental health – particularly for Japanese men.
In our data, nearly a quarter of male and female subjects indicated depressive symptoms at baseline defined by the GDS score of 5 or more. Another population-based study in Japan targeting people over the age of 64 reported that prevalence of those who scored more than 5 in GDS-15 was 23.8%, which is compatible to our data [26].
Our finding that retirement may increase depressive symptoms is inconsistent with many studies conducted in European countries [5–11], whereas a previous study in another Asian population supports our result [12, 13]. We speculate that, for Japanese workers (men especially), the loss of non-financial benefits of work outweighs the other benefits of retirement such as a relief from work-related stress overall. Interestingly, we found that changes in social contacts and social supports failed to explain the association between retirement and depressive symptoms. Although convincing evidence is lacking, the adverse effect of retirement may be attributable to a loss of other benefits of work including sense of meaning in life. Indeed, the literature suggests that many Japanese workers tend to find their purpose in life from work [27]. Retirement among Japanese workers may thus result in a loss of a sense of meaning in life.
Among Japanese workers who experienced the post-War period of rapid economic growth, employment was characterized by long hours of work as well as a shared sense of sacrifice with the goal of rebuilding the nation in the aftermath of the destruction wrought by the Second World War [28]. The participants in JAGES study -- all of whom were aged over 65 years at baseline in 2010 -- belong to this cohort. In return for their sacrifice of leisure and family life, Japanese workers of this generation were rewarded with a life-time employment guarantee. Commitment to the company thereby molded the identity of an entire generation of Japanese workers. It is in this context that we may interpret the findings of the present study. The transition to retirement for many Japanese workers entails the severing of links with work colleagues as well as loss of a sense of meaning in life. It is important to note at the same time, however, that the post-War lifetime employment guarantee has broken down in Japanese society in the aftermath of the 1991 economic bubble collapse. Our findings may therefore not apply to future generations of Japanese workers.
Our results also suggest that retirement may be more toxic among Japanese men from lower occupational class backgrounds compared to managerial/professional occupations. One explanation is that men from high SES backgrounds may have extra social roles besides work-related social roles, and therefore, may be less affected by a loss of work-related role due to retirement. Additionally, there may be some health benefits of retirement for the managerial/professional class. Indeed, mortality trends in Japan by occupational class indicate that suicide rates in these groups have risen sharply in the past two decades, possibly as a result of the pressures stemming from economic stagnation [29, 30]. It is possible that retirement can be somewhat beneficial for those workers as it relieves them of the work-related distress. The observed wide confidence intervals for the interaction terms between changes in working status and occupational class among women may be due to the small number of women who were from high-occupational background. Indeed, among female JAGES subjects in 2010, only 12.6% were categorized as high occupational class.
Our findings also indicate the trend that participation in recreational activity could mitigate the increase in depressive symptoms among Japanese retired men and women but perhaps through different mechanisms. Results from the model additionally adjusting for a sense of meaning in life suggests that recreational social participation may benefit retired Japanese men by compensating for a loss of a sense of meaning in life due to retirement. However, this was not the case for retired women. We speculate that recreational social participation for these retired women had differential meaning such as increased opportunities for informal socializing, rather than provision of a sense of meaning in life. Indeed, Takagi et al. also argued that there was a gender difference in mechanisms through which social participation enhances mental health [24]. We found no significant interaction between transition to retirement and social participation with roles including volunteerism, which was inconsistent with preceding findings [12, 13]. Participation in activities involving roles may not be completely voluntary and some participants might have been feeling a psychological distress due to “role strain”, namely a pressure to accomplish their roles [20, 31]. This may explain the non-significant interaction effect of social participation with roles and its wide variance.
Ours is, to our knowledge, the first study to evaluate the association between changes in working status and changes in depressive symptoms using data of Japanese older people. Strengths of our study include the large sample size of older adults with repeated measures of both outcomes and exposures, and the use of first-difference models to account for all time-invariant confounding factors. Nonetheless, several limitations should be noted. First, there is a possibility of reverse causation, such that workers are more likely to seek retirement when they feel depressed [32]. Although we partly addressed this issue by excluding subjects who showed depression at baseline from the analyses, future studies should specify reasons for retirement to permit causal inference. Second, unmeasured confounding factors may also exist. Even though we controlled for all observed/unobserved time-invariant confounding factors and several possible time-variant confounding factors, there may be other stressful life events or circumstances, which causes changes in working status and changes in depressive symptoms. Third, some of our measurements were admittedly crude. We used changes in received social supports from “friends” as a measurement of changes in work-related social relationships. However, it is obvious that social relationships people obtain from work are not necessarily reported as “friends”. Fourth, we evaluated social participation at the same time with our final outcome. Since we hypothesized that post-retirement social participation could mitigate the possibly adverse impact of retirement on mental health, it is ideal to measure social participation before measuring post-retirement mental health. Fifth, generalizability of our findings is limited. As the effect of retirement on mental health is presumably culture dependent, our findings may not be generalizable to other countries or future generations. Lastly, our single item measurement of “a sense of meaning in life” is not validated, and therefore, it may not successfully capture a subject’s sense of meaning in life.
Conclusions
Retirement may increase depressive symptoms among Japanese older people, possibly men with lower occupational class backgrounds in particular. An important public health implication of our study is that there is a possibility that encouraging recreational social participation may compensate for a loss of a sense of meaning in life due to retirement and mitigate the potentially adverse effects of retirement on mental health of Japanese older men.
Additional files
Regression Coefficients of Changes in Working Status and Interactions with occupational class (Model 3) and changes in marital status (Model 4) by gender (full-sample). (DOCX 17 kb)
Multiple linear regression of Changes in GDS score on changes in working status by gender (sub-sample). (DOCX 17 kb)
Regression Coefficients of Changes in Working Status and Interactions with social participation by gender (sub-sample). (DOCX 14 kb)
Acknowledgement
The authors thank other JAGES group members. We are also grateful for comments and assistance from Hideki Hashimoto, Hiroyuki Hikichi and Toru Tsuboya.
Funding
This work was supported by a Health Labour Sciences Research Grant, Comprehensive Research on Aging and Health (H28-Choju-Ippan-002, H26-Choju-Ippan-006, H25-Choju-Ippan-003, H25-KenkiWakate-015, H25-Irryo-Shitei-003(Fukko), H24-Junkanki (Shoshu)-Ippan-007, H22-Choju-Shitei-008) from the Ministry of Health, Labour and Welfare, Japan; Grants-in-Aid for Scientific Research (20,319,338, 22,390,400, 23,243,070, 23,590,786, 23,790,710, 24,140,701, 24,390,469, 24,530,698, 24,653,150, 24,683,018, 25,253,052, 25,870,881, 26,882,010, 15H01972) from the Japan Society for the Promotion of Science; grants from the National Center for Geriatrics and Gerontology, Japan (24–17, 24–23, J09KF00804); AXA Life Insurance. Co. LTD.; Japan Agency for Medical Research and Development.
Availability of data and materials
The dataset supporting the conclusions of this article is available in response to the request from the researchers admitted by the JAGES committee.
Authors’ contributions
SK: Conception and design, data analysis and interpretation, drafting the manuscript. KN: Conception and design, data interpretation, critical review of the manuscript. KK: data collection, critical review of the manuscript. KI: Conception and design, data interpretation, critical review of the manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Participants were informed that their voluntary participation in the study and returning the self-administered questionnaire via mail indicated their consent to participate in the study. The study protocol and informed consent procedure were approved by the Ethics Committee in Research of Human Subjects at Nihon Fukushi University.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- GDS-15
Short version of the Geriatric Depression Scale
- IADL
Instrumental activities of daily living
- JAGES
Japan gerontological evaluation study
- TMIG
Tokyo Metropolitan Institute of Gerontology
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1186/s12889-017-4427-0) contains supplementary material, which is available to authorized users.
Contributor Information
Koichiro Shiba, Email: shibakoichiro@gmail.com.
Naoki Kondo, Email: naoki-kondo@umin.ac.jp.
Katsunori Kondo, Email: kkondo@chiba-u.jp.
Ichiro Kawachi, Email: ckawach@aol.com.
References
- 1.OECD data. Employment: labour force participation rate.; 2014 (online). Available at: data.oecd.org/emp/labour-force-participation-rate.htm.
- 2.Ministry of Internal Affairs and Communications, Statistics Bureau. Annual report on the labour force survey.; 2014 (online). Available at: www.stat.go.jp/english/data/roudou/report/2014/index.htm.
- 3.Fukutomi E, Kimura Y, Wada T, Okumiya K, Matsubayashi K. Long-term care prevention project in Japan. Lancet (London, England) 2013;381(9861):116. doi: 10.1016/S0140-6736(13)60049-5. [DOI] [PubMed] [Google Scholar]
- 4.Banks J, Chandola T, Matthews K. International Encyclopedia of the Social & Behavioral Sciences. Amsterdam: Elsevier; 2015.
- 5.Oksanen T, Vahtera J, Westerlund H, et al. Is retirement beneficial for mental health?: antidepressant use before and after retirement. Epidemiology. 2011;22(4):553–559. doi: 10.1097/EDE.0b013e31821c41bd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mein G, Martikainen P, Hemingway H, Stansfeld S, Marmot M. Is retirement good or bad for mental and physical health functioning? Whitehall II longitudinal study of civil servants. J Epidemiol Community Health. 2003;57(1):46–49. doi: 10.1136/jech.57.1.46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jokela M, Ferrie JE, Gimeno D, et al. From midlife to early old age: health trajectories associated with retirement. Epidemiology. 2010;21(3):284–290. doi: 10.1097/EDE.0b013e3181d61f53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Westerlund H, Vahtera J, Ferrie JE, et al. Effect of retirement on major chronic conditions and fatigue: French GAZEL occupational cohort study. BMJ. 2010;341(nov23_1):c6149. doi: 10.1136/bmj.c6149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Olesen K, Rod NH, Madsen IEH, Bonde JP, Rugulies R. Does retirement reduce the risk of mental disorders? A national registry-linkage study of treatment for mental disorders before and after retirement of 245 082 Danish residents. Occup Environ Med. 2015;72(5):366–372. doi: 10.1136/oemed-2014-102228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Laaksonen M, Metsä-Simola N, Martikainen P, et al. Trajectories of mental health before and after old-age and disability retirement: a register-based study on purchases of psychotropic drugs. Scand J Work Environ Health. 2012;38(5):409–417. doi: 10.5271/sjweh.3290. [DOI] [PubMed] [Google Scholar]
- 11.Leinonen T, Lahelma E, Martikainen P. Trajectories of antidepressant medication before and after retirement: the contribution of socio-demographic factors. Eur J Epidemiol. 2013;28(5):417–426. doi: 10.1007/s10654-013-9792-0. [DOI] [PubMed] [Google Scholar]
- 12.Schwingel A, Niti MM, Tang C, Ng TP. Continued work employment and volunteerism and mental well-being of older adults: Singapore longitudinal ageing studies. Age Ageing. 2009;38(5):531–537. doi: 10.1093/ageing/afp089. [DOI] [PubMed] [Google Scholar]
- 13.Sugihara Y, Sugisawa H, Shibata H, Harada K. Productive roles, gender, and depressive symptoms: evidence from a National Longitudinal Study of late-middle-aged Japanese. J Gerontol Ser B Psychol Sci Soc Sci. 2008;63(4):P227–P234. doi: 10.1093/geronb/63.4.P227. [DOI] [PubMed] [Google Scholar]
- 14.Berkman LF, Kawachi I, Glymour MM. Social Epidemiology. 2nd ed. Oxford: Oxford University Press; 2014.
- 15.Thoits PA. Mechanisms linking social ties and support to physical and mental health. J Health Soc Behav. 2011;52(2):145–161. doi: 10.1177/0022146510395592. [DOI] [PubMed] [Google Scholar]
- 16.Mein G, Higgs P, Ferrie J, Stansfeld S. Paradigms of retirement: the importance of health and ageing in the whitehall ii study. Soc Sci Med. 1998;47(4):535–545. doi: 10.1016/S0277-9536(98)00146-4. [DOI] [PubMed] [Google Scholar]
- 17.Hao Y. Productive activities and psychological well-being among older adults. J Gerontol Ser B Psychol Sci Soc Sci. 2008;63(2):S64–S72. doi: 10.1093/geronb/63.2.S64. [DOI] [PubMed] [Google Scholar]
- 18.Wickrama KKAS, O’Neal CW, Kwag KH, Lee TK. Is working later in life good or bad for health? An investigation of multiple health outcomes. J Gerontol Ser B Psychol Sci Soc Sci. 2013;68(5):807–815. doi: 10.1093/geronb/gbt069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wang M, Shi J. Psychological research on retirement. Annu Rev Psychol. 2014;65:209–233. doi: 10.1146/annurev-psych-010213-115131. [DOI] [PubMed] [Google Scholar]
- 20.Morrow-Howell N, Hinterlong J, Rozario PA, Tang F. Effects of volunteering on the well-being of older adults. J Gerontol Ser B Psychol Sci Soc Sci. 2003;58(3):S137–S145. doi: 10.1093/geronb/58.3.S137. [DOI] [PubMed] [Google Scholar]
- 21.Tani Y, Fujiwara T, Kondo N, Noma H, Sasaki Y, Kondo K. Childhood socioeconomic status and onset of depression among Japanese older adults: the JAGES prospective cohort study. Am J Geriatr Psychiatry. 2016;24(9):717–726. doi: 10.1016/j.jagp.2016.06.001. [DOI] [PubMed] [Google Scholar]
- 22.Tani Y, Sasaki Y, Haseda M, Kondo K, Kondo N. Eating alone and depression in older men and women by cohabitation status: the JAGES longitudinal survey. Age Ageing. 2015;44(6):1019–1026. doi: 10.1093/ageing/afv145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Burke WJ, Roccaforte WH, Wengel SP. The short form of the geriatric depression scale: a comparison with the 30-item form. J Geriatr Psychiatry Neurol. 1991;4(3):173–178. doi: 10.1177/089198879100400310. [DOI] [PubMed] [Google Scholar]
- 24.Takagi D, Kondo K, Kawachi I. Social participation and mental health: moderating effects of gender, social role and rurality. BMC Public Health. 2013;13(1):701. doi: 10.1186/1471-2458-13-701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Koyano W, Shibata H, Nakazato K, Haga H, Suyama Y. Measurement of competence: reliability and validity of the TMIG Index of competence. Arch Gerontol Geriatr. 13(2):103–16. [DOI] [PubMed]
- 26.Fujisawa D, Tanaka E, Sakamoto S, Neichi K, Nakagawa A, Ono Y. The development of a brief screening instrument for depression and suicidal ideation for elderly: the depression and suicide screen. Psychiatry Clin Neurosci. 2005;59(6):634–638. doi: 10.1111/j.1440-1819.2005.01429.x. [DOI] [PubMed] [Google Scholar]
- 27.Shirai K, Iso H, Fukuda H, Toyoda Y, Takatorige T, Tatara K. Factors associated with “Ikigai” among members of a public temporary employment agency for seniors (silver human resources Centre) in Japan; gender differences. Health Qual Life Outcomes. 2006;4:12. doi: 10.1186/1477-7525-4-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Zielenziger M. Shutting out the sun: how Japan created its own Lost generation. Nan a. Talese. 2006. [Google Scholar]
- 29.Suzuki E, Kashima S, Kawachi I, Subramanian SV. Social and geographical inequalities in suicide in Japan from 1975 through 2005: a census-based longitudinal analysis. PLoS One. 2013;8(5):e63443. doi: 10.1371/journal.pone.0063443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wada K, Kondo N, Gilmour S, et al. Trends in cause specific mortality across occupations in Japanese men of working age during period of economic stagnation, 1980-2005: retrospective cohort study. BMJ. 2012;344(mar06_3):e1191. doi: 10.1136/bmj.e1191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Chandola T, Martikainen P, Bartley M, et al. Does conflict between home and work explain the effect of multiple roles on mental health? A comparative study of Finland, Japan, and the UK. Int J Epidemiol. 2004;33(4):884–893. doi: 10.1093/ije/dyh155. [DOI] [PubMed] [Google Scholar]
- 32.van Rijn RM, Robroek SJW, Brouwer S, Burdorf A. Influence of poor health on exit from paid employment: a systematic review. Occup Environ Med. 2014;71(4):295–301. doi: 10.1136/oemed-2013-101591. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Regression Coefficients of Changes in Working Status and Interactions with occupational class (Model 3) and changes in marital status (Model 4) by gender (full-sample). (DOCX 17 kb)
Multiple linear regression of Changes in GDS score on changes in working status by gender (sub-sample). (DOCX 17 kb)
Regression Coefficients of Changes in Working Status and Interactions with social participation by gender (sub-sample). (DOCX 14 kb)
Data Availability Statement
The dataset supporting the conclusions of this article is available in response to the request from the researchers admitted by the JAGES committee.