

Abstract
Thyroid tuberculosis (TT) is a very rare condition, even in countries where tuberculosis is endemic. However, the prevalence of tuberculosis has increased worldwide and thyroid involvement can be a primary manifestation of the disease. We present the case of a 43-year-old patient with this diagnosis and perform a review of the related literature. After searching for similar case reports in Western Europe since 2010 we identified six cases in four countries. TT should be considered in the differential diagnosis of a thyroid nodule. Fine-needle aspiration cytology and polymerase chain reaction are useful tools as preoperative diagnosis. Typical caseous necrotic granulomas are the hallmark in biopsy.
INTRODUCTION
Tuberculosis is a disease that initially affects the lungs in most of the cases, but it can involve any organ, whether as primary disease, or secondary to hematogenous or lymphatic dissemination. Primary thyroid tuberculosis (TT) is an extremely rare condition, even in countries where tuberculosis is endemic, which is probably explained by a high resistance of the thyroid gland to infectious processes [1, 2].
CASE REPORT
A 43-year-old Ecuadorian woman, living in Spain for 20 years, was referred to our clinic after the incidental finding of a left thyroid nodule on a cervical CT scan during the study of asymptomatic, self-reported cervical and inguinal adenopathies, which were already reported as benign 2 years prior to evaluation. She reported no trips to endemic countries. There were no clinical findings of thyroid dysfunction or due to glandular compression; neither had she experienced fever or cervical pain. A palpable goiter or thyroid nodule was absent, and no lymph nodes were identified on physical examination. Routine analysis and thyroid function tests were normal. Cervical ultrasonography showed an isoechoic solid-cystic left thyroid nodule with 17 mm in its largest dimension (Fig. 1). There were no suspicious adenopathies described on ultrasound. Fine-needle aspiration cytology (FNAC) was performed, obtaining a colloid material that showed multinucleated giant cells (MGCs) and a follicular proliferation pattern with inconclusive cytological alterations (follicular lesion of undetermined significance: Bethesda Category 3).
Figure 1:
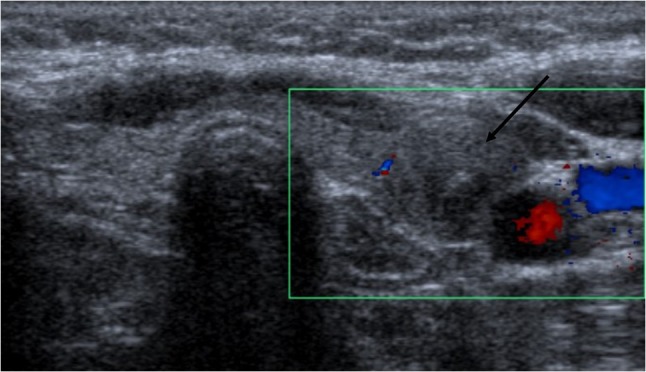
Left thyroid nodule, isoechoic, solid-cystic aspect, regular margins, well-defined borders, hypoechogenic halo present and peripheral vascularity (arrow).
Due to the possibility of malignancy, cultures for Mycobacterium tuberculosis and fast-acid bacilli stains were not performed in the FNAC material. Therefore, a left hemithyroidectomy and further histological study were performed, finding MGC and caseous necrotic granulomas (Fig. 2). Immunohistochemistry techniques for calcitonin, chromogranin and synaptophysin were negative. Native BRAF gene was not mutated. Ziehl–Neelsen stain (ZNS), periodic acid-Schiff (PAS) and silver methenamine stains did not detect pathogen agents, and cultures for Mycobacteria (MB) were negative. Amyloid substance with Congo red stain was not found. Finally, polymerase chain reaction (PCR) for M. tuberculosis was performed in the removed tissue, which was positive.
Figure 2:

Caseous necrotic granuloma (pink area, wide arrow) surrounded by a lymphocytic infiltrate and MGCs.
Additional study using chest X-ray, urine analysis and chest-abdominal CT was normal, except for multiple, unspecific lymph nodes that were found in external and common iliac chains, and in periaortic retroperitoneal chains. The cytologic study of the iliac lymph nodes was benign and no granulomas were observed. Gallium 67 scintigraphy with abdominal SPECT-CT was also normal. Serological screening tests for HIV, Syphilis, Hepatitis B and C were negative.
Treatment with isoniazid (300 mg), rifampicin (600 mg), ethambutol (1200 mg) and pyrazinamide (1500 mg) was initiated for 2 months, followed by a consolidation phase with isoniazid and rifampicin, at same doses, for 4 months. After 6 months of follow-up, our patient remains asymptomatic with a normal blood cell count, normal C-reactive protein levels, normal thyroid function and unremarkable features on neck ultrasound.
DISCUSSION
Tuberculosis is considered a public-health problem despite the measures implemented for its prevention [2], with the prevalence ranging from 0.1% to 0.6% [3]. Since 1863, when Bruns et al. reported the first case of TT, few cases were described, most of them in post-mortem studies [2]. It is unknown why thyroid gland is rarely affected, although it is well known the gland resistance to infections. The latter might be related to different mechanisms, such as the bactericidal property of the colloid, the increased vascular supply and oxygenation of the gland, and its high iodine concentration [4, 5].
TT is more prevalent in middle-aged women [6]. The involvement can be primary (the most frequent) or secondary after the spread of bacilli from an adjacent focus or by seeding the gland during hematogenous dissemination [2, 3]. Five different clinical presentations have been described (i) goiter with caseation, (ii) cold abscess formation, (iii) acute abscess, (iv) miliary tuberculosis and (v) chronic fibrosing tuberculosis [2, 7].
After a systematic medical review in the PUBMED platform of TT cases reported in western countries since 2010, we found three cases in Spain [5–7], all of them with a primary involvement, one case in France in the context of a miliary tuberculosis [4], one case in the UK [1] and one in Portugal [8] (Table 1). Overall, most of the patients were asymptomatic at the time of diagnosis, although cervical pain, increased glandular volume and fever of unknown origin may also be uncommon presentations [2, 3]. Thyroid function was normal in most of the cases, although we found three cases with hypo- or hyperthyroidism [1, 2, 8].
Table 1:
TT in Western Europe since 2010
| Author | Gender (age) | Nationality (country) | Primary or secondary | Clinical presentation | Other symptoms | Thyroid function | Diagnosis | Lymph nodes involvement | Treatment |
|---|---|---|---|---|---|---|---|---|---|
| Ortiz-Flores et al. | Female (43) | Ecuadorian (Spain) | Primary | Thyroid nodule Inguinal adenopathies |
Asymptomatic | Normal | PCR in thyroid tissue | Lymphadenitis | ATD |
| Cuesta-Hernández et al. [5] | Male (19) | South American (Spain) | Primary | Cold abscess Cervical adenopathies |
Dysphagia Weight loss Fever |
Hypothyroidism | PCR in FNAC material | Lymph nodes cytology not reported | ATD and surgical drainage |
| Peteiro-González et al. [6] | Female (58) | Not reported (Spain) | Primary with lymphatic dissemination | Goiter with caseation Cervical adenopathies |
Asymptomatic | Normal | Culture in adenopathy material | Cultures positive for MT | ATD |
| Ponce-Villar et al. [7] | Male (57) | Bolivian (Spain) | Primary | Acute abscess Cervical adenopathies |
Cervical pain Weight loss |
Normal | Culture of abscess material | Lymph nodes cytology not reported | Surgical drainage and ATD |
| Luiz et al. [8] | Male (45) | Indian (Portugal) | Primary with lymphatic dissemination | Goiter and caseation Cold abscess Cervical adenopathies |
Hemoptysis Weight loss Neck swelling |
Hypothyroidism | Culture of abscess material | Cultures positive for MT | ATD |
| Lourtet-Hascoet et al. [4] | Male (43) | Thai (France) | Secondary | Thyroid nodule Multiple adenopathies Previous primary pulmonary tuberculosis |
Cough Weight loss |
Normal | PCR in FNAC material | Cultures positive for MT | ATD |
| Raman et al. [1] | Male (38) | Indian (UK) | Primary | Goiter with caseation | Fever Neck swelling |
Hyperthyroidism | AFB stains and cultures of FNAC material | Not involved | ATD |
MT, Mycobacterium tuberculosis; AFB, Acid fast bacilli; ATD, anti-tuberculosis drugs.
Ultrasound findings are unspecific, showing a diffuse or multinodular goiter, and in some cases nodules can mimic a carcinoma [2]. FNAC is a useful diagnostic tool as it provides material for bacteriologic and cytological analysis [9]. The presence of MGC, caseous necrotic granulomas are typical of this disease [8]. Many authors suggest that MB confirmation techniques must be performed, either using ZNS, specific cultures for MB, or PCR for M. tuberculosis, with the latter being a reliable diagnostic method [2, 10]. If FNAC is non-diagnostic, a post-thyroidectomy biopsy should be considered; in this case, the presence of MGC, lymphocytic infiltration and typical granulomas will confirm the diagnosis [3, 8].
Anti-tuberculosis drugs are considered the main treatment option and its duration will depend on whether the infection is primary or secondary [8]. The role of surgery is very limited for this condition, as surgical drainage is only indicated in case of a large abscess [2]. In our patient, hemithyroidectomy was initially performed due to the possibility of malignancy.
CONFLICT OF INTEREST STATEMENT
None declared.
ETHICAL APPROVAL
We obtained patient informed consent for the presentation of this case.
GUARANTOR
A.O.F. is the guarantor of this manuscript.
FUNDING
None.
REFERENCES
- 1. Raman L, Murray J, Banka R. Primary tuberculosis of the thyroid gland: an unexpected cause of thyrotoxicosis. BMJ Case Rep 2014;2014 doi:10.1136/bcr-2013-202792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Bulbuloglu E, Ciralik H, Okur E, Ozdemir G, Ezberci F, Cetinkaya A, et al. Tuberculosis of the thyroid gland: Review of the literature. World J Surg 2006;30:149–55. doi:10.1007/s00268-005-0139-1. [DOI] [PubMed] [Google Scholar]
- 3. Ozekinci S, Mizrak B, Saruhan G, Senturk S. Histopathologic diagnosis of thyroid tuberculosis. Thyroid 2009;19:983–6. doi:10.1089/thy.2009.0189. [DOI] [PubMed] [Google Scholar]
- 4. Lourtet-Hascoet J, Le Grusse J, Fontaine S, Caron P. Thyroid tuberculosis: a new case and review of the literature. Ann Endocrinol (Paris) 2015. Oct;76:635–7. doi:10.1016/j.ando.2015.07.934. [DOI] [PubMed] [Google Scholar]
- 5. Cuesta-Hernández M, Gómez-Hoyos E, Agrela-Rojas E, Téllez-Molina MJ, Díaz-Pérez JA. Tuberculosis tiroidea: causa excepcional de bocio compresivo. Endocrinol Nutr 2013;60:e11–3. doi:10.1016/j.endonu.2012.10.005. [DOI] [PubMed] [Google Scholar]
- 6. Peteiro-González D, Cabezas-Agrícola JM, Cameselle-Teijeiro J, Mínguez I, Casanueva FF. Tuberculosis tiroidea primaria. Endocrinol Nutr 2010. Feb;57:82–3. doi:10.1016/j.endonu.2010.01.002. [DOI] [PubMed] [Google Scholar]
- 7. Ponce-Villar U, Planells-Roig M, Coret-Franco A, Peiró-Monzo F, Caro-Pérez F. Presentation of primary thyroid tuberculosis as a sub-acute thyroid abscess. A case report. Semergen 2015;41:e58–60. doi:10.1016/j.semerg.2014.04.001. [DOI] [PubMed] [Google Scholar]
- 8. Luiz HV, Pereira BD, Silva TN, Veloza A, Matos C, Portugal J, et al. Thyroid tuberculosis with abnormal thyroid function - case report and review of the literature. Endocr Pract 2013;19:e44–9. doi:10.4158/EP12276.CR. [DOI] [PubMed] [Google Scholar]
- 9. Mondal A, Patra DK. Efficacy of fine needle aspiration cytology in the diagnosis of tuberculosis of the thyroid gland: a study of 18 cases. J Laryngol Otol 1995;109:36–8. [DOI] [PubMed] [Google Scholar]
- 10. Gupta N, Sharma K, Barwad A, Sharma M, Rajwanshi A, Sharma A, et al. Thyroid tuberculosis – role of PCR in diagnosis of a rare entity. Cytopathology 2011;22:392–6. doi:10.1111/j.1365-2303.2010.00830.x. [DOI] [PubMed] [Google Scholar]