

Abstract
Background: Cancer Registries (CRs) remain the gold standard for providing official epidemiological estimations. However, due to CRs’ partial population coverage, hospitalization records might represent a valuable tool to provide additional information on cancer occurrence and expenditures at national/regional level for research purposes. The Epidemiology of Cancer in Italy (EPIKIT) study group has been built up, within the framework of the Civic Observers for Health and Environment: Initiative of Responsibility and Sustainability (COHEIRS) project under the auspices of the Europe for Citizens Program, to assess population health indicators. Objective: To assess the burden of all cancers in Italian children and adults. Methods: We analyzed National Hospitalization Records from 2001 to 2011. Based on social security numbers (anonymously treated), we have excluded from our analyses all re-hospitalizations of the same patients (n = 1,878,109) over the entire 11-year period in order to minimize the overlap between prevalent and incident cancer cases. To be more conservative, only data concerning the last five years (2007–2011) have been taken into account for final analyses. The absolute number of hospitalizations and standardized hospitalization rates (SHR) were computed for each Italian province by sex and age-groups (0–19 and 20–49). Results: The EPIKIT database included a total of 4,113,169 first hospital admissions due to main diagnoses of all tumors. The annual average number of hospital admissions due to cancer in Italy has been computed in 2362 and 43,141 hospitalizations in pediatric patients (0–19 years old) and adults (20–49 years old), respectively. Women accounted for the majority of cancer cases in adults aged 20–49. As expected, the big city of Rome presented the highest average annual number of pediatric cancers (n = 392, SHR = 9.9), followed by Naples (n = 378; SHR = 9.9) and Milan (n = 212; SHR = 7.3). However, when we look at SHR, minor cities (i.e., Imperia, Isernia and others) presented values >10 per 100,000, with only 10 or 20 cases per year. Similar figures are shown also for young adults aged 20–49. Conclusions: In addition to SHR, the absolute number of incident cancer cases represents a crucial piece of information for planning adequate healthcare services and assessing social alarm phenomena. Our findings call for specific risk assessment programs at local level (involving CRs) to search for causal relations with environmental exposures.
Keywords: hospitalizations, cancer incidence, children, pediatric cancer, adult cancer, environment and health
1. Introduction
Until 1955, the word “tumor” was generically defined as “an occupational disease of chemical industry workers” in the most prestigious encyclopedic dictionaries [1]. Nowadays, cancer is generally associated with old age, and its continuous increase—observed throughout the 20th century in all industrialized countries—is generally explained as a consequence of progressive accumulation of oxidative, stochastic (random) genetic damage, along with ongoing improvement in our diagnostic capacities. From the end of the 1980s to date, cancer has involved individuals of all ages, including younger people, whose number it is difficult to estimate [2]. Cancer incidence data are essential for epidemiological purposes, as well as for planning screening campaigns and cancer primary prevention or surveillance. The implementation of Cancer Registries (CRs) represents the gold standard methodology for data collection and cancer surveillance at the local level [3].
In Italy, a network of population-based local cancer registries has been established (Italian Association of Cancer Registries, AIRTUM) in order to set high qualitative standards in data collection that result in reliable reports, with data available on the AIRTUM website. However, the AIRTUM CRs does not cover the entire Italian population, with a remarkable difference in CRs population coverage among Northern (50.2%), Central (25.5%) and Southern areas of the Country (17.9%) [4]. In the last decade, cancer incidence estimation at national level have been provided in the frame of a specific cooperation between the National Institute of Public Health (ISS), the National Cancer Institute of Milan, and the AIRTUM. They mainly adopted the Mortality-Incidence Analysis MODel (MIAMOD) statistical model, which represents a back-calculation approach to estimate the morbidity of chronic irreversible diseases from existing mortality and survival data [5,6].
Referring only to CRs when searching for epidemiological data about the overall and cancer-specific burden of tumors in general population or in well-defined subgroups (i.e., pediatric population or younger adults) might represent a limitation, due to the problem of CRs’ partial population coverage [7]. Despite possible limitations related to underestimation produced by the proportion of cancer patients that is not hospitalized, additional secondary databases such as hospital discharge records (HDR) have been proposed by researchers as potential tools to improve the ability of assessing the burden of several diseases, including cancer [8,9,10,11,12]. The accuracy of these secondary data sources has been specifically explored [13,14]. A study carried out by Penberthy et al. used both CRs and HDR for the detection of incident cancer cases [15]. In our previous studies, we have used HDR as secondary data source to specifically address the issue of breast cancer [12,16].
In this paper, we present the first analyses performed on the national hospital discharge records maintained at central level by the Ministry of Health concerning hospitalization due to main diagnosis of overall cancer, as a result of the work carried out by the Epidemiology of Cancer in Italy (EPIKIT) study group. This latter initiative has been promoted within the framework of the European Civic Observers for Health and Environment: Initiative of Responsibility and Sustainability (COHEIRS) project under the auspices of the European Union’s “Europe for Citizens” Program [17]. COHEIRS—coordinated by ALDA, the European Association of Local Democracy Agencies at the European Council in Strasbourg was implemented in Italy by the Euro Mediterranean Scientific Bio-Medical Institute (ISBEM) and International Society Doctors for the Environment (ISDE) and it has been acknowledged as one of the three best European projects of the year 2013. The aim of the COHEIRS project was to foster the implementation of the “precautionary principle” (with specific focus on health and environment assessment) stated in the Maastricht Treaty and at Article 191 of the European Union Treaty [17]. Precautionary principle should be invoked when scientific final proofs of toxicity for the environment or health are lacking, but some evidence lead to possible concerns.
Although CRs remain the gold standard methodology to collect epidemiological information on cancer incidence at local level, we attempted to estimate the burden of cancer at regional and province level for the entire nation thanks to the specific expertise developed by our study group in the treatment and analysis of HDR. These analyses could also be useful in better understanding the consistency of social alarm that have spread in certain areas of the country (i.e., the Campania region) concerning possible environmental threats to human health related to illegal activities leading to soil/air/water pollution. Our work could help in explaining the widespread perception of higher incidence of tumors in pediatric population (0–19 years old) and adults belonging to those age groups (20–49 years old) generally excluded by official screening for cancer prevention. At the same time, our work could be used by decision makers in planning healthcare services to be offered at local level in the field of oncology.
2. Materials and Methods
2.1. Database
Information concerning hospitalizations occurring in Italian hospitals are registered in Hospital Discharge Records (HDRs), which are collected in the Italian Ministry of Health’s national hospitalization database. The information is anonymous and includes the region and hospital where the patients have been hospitalized, type of hospitalization (ordinary admission or day hospital), region and province where the patient come from, local health authority (ASL) who is paying for the hospitalization costs, patient’s age, gender, main diagnosis, secondary diagnoses (comorbidities which are not the cause of the hospitalization), procedures performed, diagnosis related group (DRG) and length of the hospitalization. HDRs are kept at the central level by the Ministry of Health since the year 1999, but the national hospitalization database has been fully implemented for all Italian regions only since 2001. It is important to point out that, in the national hospitalization database, people admitted at hospitals located in different region or provinces (different from those ones where patients live), are classified according to their hometown address. Therefore, there was no possibility of misclassification of patients from one province in another. However, it was impossible to assess the time people have been living in a specific region or province.
The Italian Ministry of Health has officially provided ISDE Campania (who is part of the COHEIRS Project and promoted the EPIKIT study group) with the full database covering all hospitalizations occurred in Italy between 2001 and 2011 due to cancer diagnoses. The quality of these data is known to be very high and certified at the central level by the Ministry of Health, with completeness and reliability of records (in terms of correspondence between hospitalizations and individual social security numbers as well as in terms of absence of errors or missing data) varying from 95.6% (year 2001) and 99.8% (from year 2008), respectively, as reported in our previous studies [9,17].
Our dataset included all hospitalized patients identified based on the following International Classification of Diseases (ICD-9-CM) major diagnosis codes: 174 (breast cancer), 162 (lung cancer), 163 (pleural cancer), 161 (larynx cancer), 146 (oropharyngeal cancer), 147 (rhino-pharyngeal cancer), 148 (hypo-pharyngeal cancer), 141 (tongue cancer), 142 (salivary glands cancer), 193 (thyroid cancer), 01, 02, 03, 04, 05 (brain cancer), 188 (bladder cancer), 185 (prostatic cancer), 180 (uterine cervix cancer), 182 (uterine cancer), 183 (ovary cancer), 153 (colon cancer), 157 (pancreatic cancer), 186.0 and 186.9 (testicular cancer), 189 (kidney and urinary tract cancer), 155 (liver cancer), 200.0–200.2, 201.0–201.9, 202.0, 203.0–203.1, 203.8, 204.0, 204.2, 204.8, 204.9, 205.0, 205.1–205.3, 205.8, 205.9, 206.0–206.3, 206.8–206.9, 207, 208 (malignant tumors of lymphatic and hemopoietic system), 1510–1519 (gastric cancer), 1501–1509 (esophageal cancer), 1580–1589 (peritoneal cancer), 1560–1569 (gall-bladder and biliary tract cancer). We considered both ordinary hospitalization and day hospital regimens.
Based on social security numbers (which were treated anonymously), the Ministry of Health has enabled us to exclude all hospital re-admissions of the same patient over the entire study period, in order to minimize possible bias related to the overlapping between prevalent and incident cancer cases. To exclude hospital re-admissions from our analysis, we have considered as hospitalization “index” only the first hospital admission over the entire study period (2001–2011). Patients presenting the same social security number (treated anonymously) and the same major diagnosis were considered as the same person, and they were computed only one time. This kind of approach to minimize the overlapping between prevalent and incident cases has been already used and validated by the Environmental Protection Agency of Piemonte Region for the assessment of population health indicators [18]. After having identified first hospital admissions for the cancer diagnosis that occurred between 2001 and 2011, we removed relapses and admissions for previous cancer patients from hospitalizations taking place during the entire 11-year period. To be more conservative and exclude prevalent cancer cases and disease relapses, we have included in our final analyses only the last five years (2007–2011).
2.2. Analyses Performed and Data Treatment
The total number of records contained in the official database provided by the Ministry of Health were 5,991,278. About 24,194 records were missing information concerning the province where the hospitalized patient was living. We have excluded from our analyses all re-hospitalizations concerning the same patient (n = 1,878,109) over the entire 11-year period. As a result, the Epikit Database contains a total of 4,113,169 “first hospital admissions” due to main diagnoses of any cancer detailed in the previous paragraph. The absolute frequencies (number of hospitalizations) were computed for each Italian region (R) and province (P), by sex (S), year (y), and 10-year age groups (x):
| (1) |
The standardized hospitalization rate (H) per 100,000 inhabitants was computed by referring to the Italian population as standard of year 2001 (y) per age group (x) and sex (S):
| (2) |
| (3) |
Data were analyzed and processed using Stata (StataCorp, College Station, TX, USA) and Excel (Microsoft, Redmond, WA, USA) software. Age and sex standardized rates per region and province were calculated based on population data provided by the Italian National Institute for Statistics (ISTAT). The results of the analyses in this first paper have been studied as cumulative data (all tumors) per each Italian region and province according to sex and age groups (0–19; 20–49). Data are specifically presented per province (in tables and on maps) as absolute number of hospitalizations and standardized hospitalization rates for each of the years from 2007 to 2011.
3. Results
Table 1 and Figure 1 report the annual average standardized hospitalization rate (SHR) per region due to all cancers in people aged 0–100 years old. Table 2 and Table 3 present the overall number of new hospitalizations and the corresponding standardized hospitalization rates per 100,000 inhabitants per province due to all cancers in pediatric population aged 0–19 and adults aged 20–49 years old, respectively.
Table 1.
Overall cancer standardized hospitalization rate per region in population aged 0–100 years old (Average Annual Value).
| Region | Average Annual SHR |
|---|---|
| Piemonte | 68.84 |
| Valle d’Aosta | 87.30 |
| Lombardia | 76.64 |
| Trentino Alto Adige | 73.72 |
| Veneto | 75.19 |
| Friuli Venezia Giulia | 86.86 |
| Liguria | 84.34 |
| Emilia/Romagna | 84.00 |
| Toscana | 72.37 |
| Umbria | 76.10 |
| Marche | 76.22 |
| Lazio | 79.92 |
| Abruzzo | 67.50 |
| Molise | 74.22 |
| Campania | 77.46 |
| Puglia | 74.93 |
| Basilicata | 71.54 |
| Calabria | 65.73 |
| Sicilia | 73.71 |
| Sardegna | 80.51 |
Figure 1.
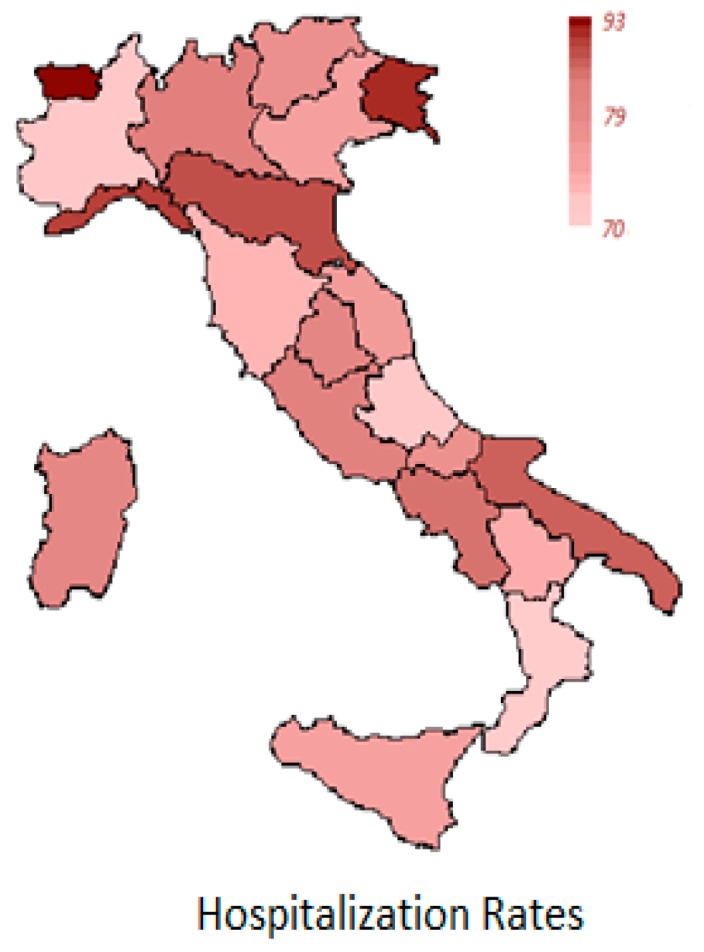
Overall regional cancer standardized hospitalization rates (SHR) per 100,000 in the population aged 0–100 years old (average annual value).
Table 2.
Standardized hospitalization rate (SHR) per 100,000 and overall number of new hospitalizations due to cancer per region and province from 2007 to 2011. Pediatric patients aged 0–19 years old.
| Region | Province | 2007 | 2008 | 2009 | 2010 | 2011 | Mean Values 2007–2011 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | SHR | n | SHR | n | SHR | n | SHR | n | SHR | n | SHR | ||
| Northern Italy | |||||||||||||
| Lombardia | Como | 38 | 6.50 | 36 | 6.15 | 32 | 5.47 | 35 | 5.98 | 45 | 7.69 | 37 | 6.36 |
| Varese | 34 | 3.98 | 54 | 6.32 | 47 | 5.50 | 55 | 6.43 | 59 | 6.90 | 50 | 5.83 | |
| Cremona | 15 | 4.44 | 15 | 4.44 | 13 | 3.85 | 17 | 5.04 | 20 | 5.93 | 16 | 4.74 | |
| Mantova | 23 | 5.86 | 16 | 4.08 | 13 | 3.31 | 26 | 6.62 | 23 | 5.86 | 20 | 5.15 | |
| Brescia | 82 | 6.22 | 65 | 4.93 | 60 | 4.55 | 91 | 6.90 | 76 | 5.77 | 75 | 5.67 | |
| Pavia | 27 | 5.69 | 28 | 5.90 | 22 | 4.64 | 37 | 7.80 | 26 | 5.48 | 28 | 5.90 | |
| Bergamo | 36 | 3.06 | 54 | 4.58 | 43 | 3.65 | 57 | 4.84 | 64 | 5.43 | 51 | 4.31 | |
| Milano | 222 | 7.64 | 215 | 7.40 | 229 | 7.88 | 239 | 8.23 | 156 | 5.37 | 212 | 7.30 | |
| Lodi | 10 | 4.46 | 14 | 6.24 | 14 | 6.24 | 18 | 8.02 | 12 | 5.35 | 14 | 6.06 | |
| Monza-Brianza | 44 | 5.18 | 44 | 5.18 | |||||||||
| Sondrio | 6 | 3.33 | 7 | 3.89 | 15 | 8.33 | 11 | 6.11 | 9 | 5.00 | 10 | 5.33 | |
| Lecco | 22 | 6.42 | 19 | 5.55 | 11 | 3.21 | 30 | 8.76 | 17 | 4.96 | 20 | 5.78 | |
| TOTAL | 515 | 5.86 | 523 | 5.95 | 499 | 5.67 | 616 | 7.01 | 551 | 6.27 | 541 | 6.15 | |
| Veneto | Rovigo | 19 | 9.60 | 13 | 6.57 | 6 | 3.03 | 10 | 5.05 | 15 | 7.58 | 13 | 6.37 |
| Venezia | 56 | 7.15 | 48 | 6.13 | 45 | 5.75 | 39 | 4.98 | 58 | 7.41 | 49 | 6.28 | |
| Vicenza | 69 | 7.48 | 54 | 5.85 | 61 | 6.61 | 59 | 6.39 | 66 | 7.15 | 62 | 6.70 | |
| Treviso | 63 | 6.81 | 63 | 6.81 | 55 | 5.94 | 70 | 7.56 | 58 | 6.27 | 62 | 6.68 | |
| Verona | 39 | 4.23 | 44 | 4.77 | 60 | 6.51 | 50 | 5.42 | 54 | 5.86 | 49 | 5.36 | |
| Padova | 52 | 5.70 | 47 | 5.15 | 56 | 6.14 | 66 | 7.24 | 51 | 5.59 | 54 | 5.96 | |
| Belluno | 8 | 4.21 | 12 | 6.31 | 3 | 1.58 | 15 | 7.89 | 8 | 4.21 | 9 | 4.84 | |
| TOTAL | 306 | 6.31 | 281 | 5.79 | 286 | 5.89 | 309 | 6.37 | 310 | 6.39 | 298 | 6.15 | |
| Emilia-Romagna | Parma | 23 | 5.89 | 27 | 6.91 | 40 | 10.24 | 41 | 10.49 | 35 | 8.96 | 33 | 8.50 |
| Rimini | 12 | 3.84 | 20 | 6.39 | 16 | 5.12 | 26 | 8.31 | 22 | 7.03 | 19 | 6.14 | |
| Bologna | 49 | 5.62 | 65 | 7.45 | 54 | 6.19 | 62 | 7.11 | 48 | 5.50 | 56 | 6.37 | |
| Forlì-Cesena | 28 | 7.68 | 22 | 6.03 | 6 | 1.64 | 21 | 5.76 | 20 | 5.48 | 19 | 5.32 | |
| Ravenna | 15 | 4.37 | 17 | 4.95 | 17 | 4.95 | 10 | 2.91 | 18 | 5.24 | 15 | 4.48 | |
| Reggio Emilia | 29 | 5.34 | 40 | 7.37 | 37 | 6.81 | 44 | 8.10 | 27 | 4.97 | 35 | 6.52 | |
| Piacenza | 17 | 6.64 | 12 | 4.69 | 26 | 10.16 | 24 | 9.38 | 12 | 4.69 | 18 | 7.11 | |
| Modena | 28 | 4.10 | 44 | 6.45 | 33 | 4.84 | 40 | 5.86 | 30 | 4.40 | 35 | 5.13 | |
| Ferrara | 24 | 8.81 | 19 | 6.97 | 17 | 6.24 | 13 | 4.77 | 7 | 2.57 | 16 | 5.87 | |
| TOTAL | 225 | 5.57 | 266 | 6.59 | 246 | 6.09 | 281 | 6.96 | 219 | 5.42 | 247 | 6.13 | |
| Piemonte | Torino | 108 | 5.22 | 124 | 5.99 | 130 | 6.28 | 143 | 6.91 | 131 | 6.33 | 127 | 6.15 |
| Alessandria | 16 | 4.60 | 26 | 7.47 | 41 | 11.78 | 30 | 8.62 | 20 | 5.75 | 27 | 7.64 | |
| Vercelli | 7 | 4.67 | 17 | 11.33 | 17 | 11.33 | 18 | 12.00 | 8 | 5.33 | 13 | 8.93 | |
| Novara | 26 | 7.55 | 28 | 8.13 | 17 | 4.93 | 16 | 4.64 | 14 | 4.06 | 20 | 5.86 | |
| Biella | 17 | 11.01 | 8 | 5.18 | 7 | 4.53 | 6 | 3.89 | 6 | 3.89 | 9 | 5.70 | |
| Asti | 10 | 5.09 | 11 | 5.60 | 13 | 6.61 | 20 | 10.17 | 7 | 3.56 | 12 | 6.21 | |
| Cuneo | 45 | 7.81 | 27 | 4.68 | 25 | 4.34 | 28 | 4.86 | 20 | 3.47 | 29 | 5.03 | |
| Verbano-Cusio-Ossola | 2 | 1.44 | 8 | 5.76 | 10 | 7.20 | 18 | 12.97 | 2 | 1.44 | 8 | 5.76 | |
| TOTAL | 231 | 5.81 | 249 | 6.26 | 260 | 6.53 | 279 | 7.01 | 208 | 5.23 | 245 | 6.17 | |
| Liguria | Imperia | 10 | 5.52 | 15 | 8.28 | 15 | 8.28 | 26 | 14.36 | 20 | 11.04 | 17 | 9.50 |
| Genova | 56 | 7.94 | 41 | 5.81 | 55 | 7.80 | 50 | 7.09 | 45 | 6.38 | 49 | 7.00 | |
| La Spezia | 8 | 4.48 | 17 | 9.52 | 16 | 8.96 | 14 | 7.84 | 10 | 5.60 | 13 | 7.28 | |
| Savona | 22 | 9.63 | 22 | 9.63 | 13 | 5.69 | 19 | 8.31 | 9 | 3.94 | 17 | 7.44 | |
| TOTAL | 96 | 7.42 | 95 | 7.34 | 99 | 7.65 | 109 | 8.43 | 84 | 6.49 | 97 | 7.47 | |
| Trentino-Alto Adige | Trento | 32 | 5.62 | 22 | 3.87 | 33 | 5.80 | 37 | 6.50 | 42 | 7.38 | 33 | 5.83 |
| Bolzano | 31 | 5.27 | 15 | 2.55 | 24 | 4.08 | 20 | 3.40 | 21 | 3.57 | 22 | 3.77 | |
| TOTAL | 63 | 5.44 | 37 | 3.20 | 57 | 4.93 | 57 | 4.92 | 63 | 5.44 | 55 | 4.79 | |
| Friuli Venezia Giulia | Udine | 24 | 5.11 | 22 | 4.69 | 42 | 8.95 | 23 | 4.90 | 31 | 6.61 | 28 | 6.05 |
| Trieste | 11 | 5.87 | 13 | 6.94 | 13 | 6.94 | 15 | 8.01 | 12 | 6.41 | 13 | 6.83 | |
| Gorizia | 6 | 4.97 | 2 | 1.66 | 11 | 9.10 | 6 | 4.97 | 6 | 4.97 | 6 | 5.13 | |
| Pordenone | 20 | 6.63 | 15 | 4.97 | 24 | 7.95 | 27 | 8.95 | 13 | 4.31 | 20 | 6.56 | |
| TOTAL | 61 | 5.65 | 52 | 4.82 | 90 | 8.34 | 71 | 6.58 | 62 | 5.75 | 67 | 6.23 | |
| Valle d’Aosta | Aosta | 10 | 8.11 | 12 | 9.73 | 4 | 3.24 | 14 | 11.36 | 10 | 8.11 | 10 | 8.11 |
| Total Northern Italy | 1446 | 5.71 | 1463 | 5.78 | 1451 | 5.73 | 1665 | 6.58 | 1445 | 5.71 | 1494 | 5.90 | |
| Central Italy | |||||||||||||
| Lazio | Roma | 433 | 10.96 | 387 | 9.80 | 408 | 10.33 | 375 | 9.49 | 357 | 9.04 | 392 | 9.92 |
| Frosinone | 42 | 8.95 | 58 | 12.36 | 55 | 11.72 | 53 | 11.29 | 42 | 8.95 | 50 | 10.65 | |
| Rieti | 19 | 13.72 | 8 | 5.78 | 16 | 11.55 | 11 | 7.94 | 12 | 8.66 | 13 | 9.53 | |
| Latina | 82 | 14.65 | 74 | 13.22 | 52 | 9.29 | 51 | 9.11 | 47 | 8.40 | 61 | 10.93 | |
| Viterbo | 42 | 14.83 | 26 | 9.18 | 18 | 6.35 | 16 | 5.65 | 21 | 7.41 | 25 | 8.68 | |
| TOTAL | 618 | 11.44 | 553 | 10.24 | 549 | 10.17 | 506 | 9.37 | 479 | 8.87 | 541 | 10.02 | |
| Toscana | Lucca | 29 | 8.44 | 19 | 5.53 | 21 | 6.11 | 17 | 4.95 | 27 | 7.85 | 23 | 6.58 |
| Grosseto | 19 | 10.37 | 9 | 4.91 | 7 | 3.82 | 12 | 6.55 | 14 | 7.64 | 12 | 6.66 | |
| Arezzo | 16 | 5.10 | 22 | 7.01 | 14 | 4.46 | 19 | 6.06 | 21 | 6.70 | 18 | 5.87 | |
| Pisa | 26 | 6.96 | 19 | 5.09 | 27 | 7.23 | 16 | 4.29 | 19 | 5.09 | 21 | 5.73 | |
| Siena | 18 | 7.58 | 17 | 7.16 | 18 | 7.58 | 6 | 2.53 | 12 | 5.06 | 14 | 5.98 | |
| Pistoia | 13 | 5.00 | 8 | 3.08 | 12 | 4.62 | 13 | 5.00 | 12 | 4.62 | 12 | 4.46 | |
| Livorno | 16 | 5.61 | 11 | 3.86 | 19 | 6.66 | 12 | 4.21 | 10 | 3.50 | 14 | 4.77 | |
| Firenze | 39 | 4.38 | 46 | 5.17 | 41 | 4.61 | 38 | 4.27 | 31 | 3.48 | 39 | 4.38 | |
| Massa-Carrara | 16 | 9.64 | 4 | 2.41 | 13 | 7.83 | 7 | 4.22 | 5 | 3.01 | 9 | 5.42 | |
| Prato | 9 | 3.73 | 15 | 6.22 | 9 | 3.73 | 6 | 2.49 | 3 | 1.24 | 8 | 3.48 | |
| TOTAL | 201 | 6.10 | 170 | 5.16 | 181 | 5.50 | 146 | 4.43 | 154 | 4.67 | 170 | 5.17 | |
| Marche | Pesaro-Urbino | 27 | 7.68 | 21 | 5.97 | 24 | 6.83 | 25 | 7.11 | 30 | 8.53 | 25 | 7.22 |
| Ascoli Piceno | 32 | 16.39 | 21 | 10.76 | 31 | 15.88 | 17 | 8.71 | 16 | 8.20 | 23 | 11.99 | |
| Ancona | 31 | 6.89 | 35 | 7.78 | 38 | 8.45 | 28 | 6.22 | 32 | 7.11 | 33 | 7.29 | |
| Macerata | 17 | 5.61 | 22 | 7.26 | 25 | 8.25 | 17 | 5.61 | 19 | 6.27 | 20 | 6.60 | |
| Fermo | 11 | 6.72 | 10 | 6.11 | 11 | 6.42 | |||||||
| TOTAL | 107 | 8.23 | 99 | 7.62 | 118 | 9.08 | 98 | 7.54 | 107 | 8.23 | 106 | 8.14 | |
| Abruzzo | Chieti | 30 | 8.32 | 43 | 11.93 | 27 | 7.49 | 29 | 8.05 | 24 | 6.66 | 31 | 8.49 |
| L’Aquila | 31 | 11.62 | 23 | 8.62 | 30 | 11.25 | 16 | 6.00 | 17 | 6.37 | 23 | 8.77 | |
| Pescara | 18 | 5.83 | 25 | 8.10 | 24 | 7.77 | 25 | 8.10 | 19 | 6.15 | 22 | 7.19 | |
| Teramo | 40 | 13.48 | 21 | 7.08 | 32 | 10.79 | 25 | 8.43 | 17 | 5.73 | 27 | 9.10 | |
| TOTAL | 119 | 9.65 | 112 | 9.09 | 113 | 9.17 | 95 | 7.71 | 77 | 6.25 | 103 | 8.37 | |
| Umbria | Terni | 27 | 13.68 | 20 | 10.13 | 13 | 6.59 | 19 | 9.63 | 16 | 8.11 | 19 | 9.63 |
| Perugia | 46 | 7.47 | 43 | 6.98 | 57 | 9.25 | 27 | 4.38 | 35 | 5.68 | 42 | 6.75 | |
| TOTAL | 73 | 8.98 | 63 | 7.74 | 70 | 8.60 | 46 | 5.65 | 51 | 6.27 | 61 | 7.45 | |
| Molise | Isernia | 14 | 18.25 | 7 | 9.12 | 10 | 13.03 | 11 | 14.34 | 8 | 10.43 | 10 | 13.03 |
| Campobasso | 17 | 7.94 | 20 | 9.34 | 32 | 14.94 | 34 | 15.87 | 18 | 8.40 | 24 | 11.30 | |
| TOTAL | 31 | 10.66 | 27 | 9.28 | 42 | 14.44 | 45 | 15.47 | 26 | 8.94 | 34 | 11.76 | |
| Total Central Italy | 1149 | 9.32 | 1024 | 8.31 | 1073 | 8.70 | 936 | 7.59 | 894 | 7.25 | 1015 | 8.23 | |
| Southern Italy | |||||||||||||
| Campania | Salerno | 143 | 12.16 | 146 | 12.42 | 109 | 9.27 | 130 | 11.06 | 120 | 10.21 | 130 | 11.02 |
| Napoli | 447 | 11.75 | 449 | 11.81 | 333 | 8.76 | 324 | 8.52 | 338 | 8.89 | 378 | 9.95 | |
| Caserta | 132 | 11.96 | 140 | 12.68 | 101 | 9.15 | 99 | 8.97 | 92 | 8.33 | 113 | 10.22 | |
| Avellino | 45 | 10.27 | 52 | 11.87 | 45 | 10.27 | 59 | 13.46 | 35 | 7.99 | 47 | 10.77 | |
| Benevento | 30 | 10.37 | 36 | 12.44 | 19 | 6.57 | 24 | 8.30 | 18 | 6.22 | 25 | 8.78 | |
| TOTAL | 797 | 11.70 | 823 | 12.09 | 607 | 8.92 | 636 | 9.34 | 603 | 8.86 | 693 | 10.18 | |
| Sicilia | Caltanissetta | 32 | 10.12 | 37 | 11.70 | 36 | 11.39 | 30 | 9.49 | 33 | 10.44 | 34 | 10.63 |
| Messina | 88 | 13.82 | 68 | 10.68 | 48 | 7.54 | 63 | 9.90 | 46 | 7.23 | 63 | 9.83 | |
| Agrigento | 46 | 9.28 | 28 | 5.65 | 34 | 6.86 | 38 | 7.67 | 35 | 7.06 | 36 | 7.30 | |
| Catania | 119 | 9.65 | 130 | 10.55 | 102 | 8.28 | 118 | 9.57 | 85 | 6.90 | 111 | 8.99 | |
| Palermo | 119 | 8.50 | 102 | 7.29 | 127 | 9.08 | 79 | 5.65 | 95 | 6.79 | 104 | 7.46 | |
| Siracusa | 26 | 6.16 | 46 | 10.89 | 26 | 6.16 | 16 | 3.79 | 27 | 6.39 | 28 | 6.68 | |
| Trapani | 33 | 7.22 | 34 | 7.43 | 52 | 11.37 | 38 | 8.31 | 25 | 5.47 | 36 | 7.96 | |
| Enna | 21 | 11.27 | 14 | 7.51 | 12 | 6.44 | 18 | 9.66 | 10 | 5.37 | 15 | 8.05 | |
| Ragusa | 36 | 10.49 | 23 | 6.70 | 23 | 6.70 | 22 | 6.41 | 14 | 4.08 | 24 | 6.88 | |
| TOTAL | 520 | 9.47 | 482 | 8.78 | 460 | 8.38 | 422 | 7.69 | 370 | 6.74 | 451 | 8.21 | |
| Puglia | Brindisi | 37 | 8.98 | 24 | 5.83 | 31 | 7.52 | 32 | 7.77 | 40 | 9.71 | 33 | 7.96 |
| Bari | 150 | 11.26 | 111 | 8.33 | 118 | 8.86 | 110 | 8.26 | 101 | 7.58 | 118 | 8.86 | |
| Foggia | 67 | 9.45 | 70 | 9.88 | 58 | 8.18 | 61 | 8.61 | 53 | 7.48 | 62 | 8.72 | |
| Barletta-Andria-Trani | 55 | 11.84 | 34 | 7.32 | 45 | 9.58 | |||||||
| Lecce | 54 | 6.68 | 52 | 6.43 | 56 | 6.93 | 49 | 6.06 | 59 | 7.30 | 54 | 6.68 | |
| Taranto | 51 | 8.22 | 41 | 6.61 | 45 | 7.26 | 34 | 5.48 | 33 | 5.32 | 41 | 6.58 | |
| TOTAL | 359 | 9.25 | 298 | 7.68 | 308 | 7.94 | 341 | 8.79 | 320 | 8.24 | 325 | 8.38 | |
| Calabria | Cosenza | 56 | 7.92 | 47 | 6.65 | 56 | 7.92 | 53 | 7.50 | 56 | 7.92 | 54 | 7.58 |
| Reggio Calabria | 54 | 8.99 | 70 | 11.65 | 45 | 7.49 | 54 | 8.99 | 46 | 7.66 | 54 | 8.96 | |
| Catanzaro | 44 | 11.93 | 35 | 9.49 | 21 | 5.69 | 50 | 13.56 | 27 | 7.32 | 35 | 9.60 | |
| Vibo Valentia | 15 | 8.43 | 9 | 5.06 | 12 | 6.74 | 18 | 10.11 | 10 | 5.62 | 13 | 7.19 | |
| Crotone | 21 | 10.46 | 13 | 6.48 | 10 | 4.98 | 18 | 8.97 | 9 | 4.48 | 14 | 7.07 | |
| TOTAL | 190 | 9.24 | 174 | 8.47 | 144 | 7.00 | 193 | 9.39 | 148 | 7.20 | 170 | 8.26 | |
| Sardegna | Oristano | 11 | 7.95 | 7 | 5.06 | 17 | 12.29 | 13 | 9.39 | 13 | 9.39 | 12 | 8.82 |
| Medio Campidano | 8 | 9.20 | 13 | 14.94 | 5 | 5.75 | 9 | 10.35 | 8 | 9.20 | 9 | 9.89 | |
| Cagliari | 40 | 8.17 | 25 | 5.11 | 40 | 8.17 | 33 | 6.74 | 44 | 8.99 | 36 | 7.44 | |
| Nuoro | 14 | 9.21 | 9 | 5.92 | 10 | 6.58 | 11 | 7.24 | 13 | 8.55 | 11 | 7.50 | |
| Ogliastra | 4 | 7.45 | 6 | 11.18 | 5 | 9.31 | 3 | 5.59 | 4 | 7.45 | 4 | 8.20 | |
| Olbia-Tempio | 9 | 6.25 | 16 | 11.11 | 14 | 9.72 | 6 | 4.17 | 10 | 6.95 | 11 | 7.64 | |
| Sassari | 27 | 9.13 | 37 | 12.51 | 23 | 7.78 | 17 | 5.75 | 12 | 4.06 | 23 | 7.85 | |
| Carbonia-Iglesias | 5 | 4.84 | 10 | 9.68 | 6 | 5.81 | 9 | 8.71 | 4 | 3.87 | 7 | 6.58 | |
| TOTAL | 118 | 8.06 | 123 | 8.41 | 120 | 8.20 | 101 | 6.90 | 108 | 7.38 | 114 | 7.79 | |
| Basilicata | Potenza | 27 | 7.35 | 23 | 6.26 | 25 | 6.81 | 29 | 7.90 | 37 | 10.08 | 28 | 7.68 |
| Matera | 20 | 9.78 | 12 | 5.87 | 10 | 4.89 | 10 | 4.89 | 11 | 5.38 | 13 | 6.16 | |
| TOTAL | 47 | 8.22 | 35 | 6.12 | 35 | 6.12 | 39 | 6.82 | 48 | 8.40 | 41 | 7.14 | |
| Total Southern Italy | 2031 | 10.02 | 1935 | 9.55 | 1674 | 8.26 | 1732 | 8.55 | 1597 | 7.88 | 1794 | 8.85 | |
Note: Regional capitals are highlighted in bold.
Table 3.
Standardized hospitalization rate (SHR) per 100,000 and overall number of new hospitalizations due to cancer per region and province from 2007 to 2011. Adults aged 20–49 years old.
| Region | Province | 2007 | 2008 | 2009 | 2010 | 2011 | Mean Values 2007–2011 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | SHR | n | SHR | n | SHR | n | SHR | n | SHR | n | SHR | ||
| Northern Italy | |||||||||||||
| Lombardia | Mantova | 291 | 71.55 | 288 | 70.81 | 276 | 67.86 | 291 | 71.55 | 324 | 79.66 | 294 | 72.29 |
| Pavia | 359 | 67.93 | 380 | 71.90 | 341 | 64.52 | 331 | 62.63 | 378 | 71.52 | 358 | 67.70 | |
| Brescia | 894 | 70.23 | 918 | 72.12 | 901 | 70.78 | 939 | 73.77 | 876 | 68.82 | 906 | 71.14 | |
| Lecco | 211 | 63.42 | 224 | 67.32 | 225 | 67.62 | 200 | 60.11 | 219 | 65.82 | 216 | 64.86 | |
| Milano | 2694 | 89.19 | 2711 | 89.76 | 2663 | 88.17 | 2434 | 80.59 | 1951 | 64.59 | 2491 | 82.46 | |
| Como | 370 | 62.42 | 414 | 69.84 | 417 | 70.35 | 356 | 60.06 | 369 | 62.25 | 385 | 64.98 | |
| Sondrio | 120 | 67.52 | 138 | 77.64 | 135 | 75.96 | 126 | 70.89 | 109 | 61.33 | 126 | 70.67 | |
| Cremona | 240 | 68.28 | 231 | 65.72 | 215 | 61.16 | 246 | 69.98 | 215 | 61.16 | 229 | 65.26 | |
| Varese | 600 | 68.94 | 640 | 73.53 | 541 | 62.16 | 555 | 63.77 | 526 | 60.43 | 572 | 65.77 | |
| Monza-Brianza | 514 | 59.90 | 514 | 59.90 | |||||||||
| Bergamo | 614 | 54.79 | 605 | 53.98 | 682 | 60.86 | 663 | 59.16 | 662 | 59.07 | 645 | 57.57 | |
| Lodi | 173 | 74.52 | 165 | 71.07 | 164 | 70.64 | 149 | 64.18 | 136 | 58.58 | 157 | 67.80 | |
| TOTAL | 6566 | 73.72 | 6714 | 75.38 | 6560 | 73.66 | 6290 | 70.62 | 6279 | 64.30 | 6482 | 71.54 | |
| Veneto | Rovigo | 139 | 59.22 | 165 | 70.30 | 186 | 79.25 | 210 | 89.48 | 185 | 78.82 | 177 | 75.41 |
| Venezia | 588 | 71.07 | 571 | 69.02 | 587 | 70.95 | 577 | 69.75 | 565 | 68.29 | 578 | 69.82 | |
| Verona | 601 | 65.53 | 627 | 68.37 | 658 | 71.75 | 595 | 64.88 | 602 | 65.64 | 617 | 67.23 | |
| Padova | 648 | 69.01 | 673 | 71.67 | 651 | 69.32 | 593 | 63.15 | 579 | 61.66 | 629 | 66.96 | |
| Treviso | 548 | 61.43 | 577 | 64.68 | 576 | 64.56 | 519 | 58.18 | 531 | 59.52 | 550 | 61.67 | |
| Belluno | 145 | 73.71 | 122 | 62.02 | 119 | 60.49 | 102 | 51.85 | 114 | 57.95 | 120 | 61.20 | |
| Vicenza | 474 | 54.12 | 517 | 59.03 | 563 | 64.28 | 543 | 62.00 | 474 | 54.12 | 514 | 58.71 | |
| TOTAL | 3143 | 64.37 | 3252 | 66.60 | 3340 | 68.40 | 3139 | 64.29 | 3050 | 62.46 | 3185 | 65.22 | |
| Emilia-Romagna | Rimini | 203 | 62.64 | 199 | 61.41 | 244 | 75.30 | 300 | 92.58 | 306 | 94.43 | 250 | 77.27 |
| Ravenna | 294 | 79.53 | 312 | 84.40 | 321 | 86.83 | 327 | 88.46 | 312 | 84.40 | 313 | 84.72 | |
| Parma | 331 | 77.79 | 347 | 81.55 | 335 | 78.73 | 341 | 80.14 | 341 | 80.14 | 339 | 79.67 | |
| Bologna | 692 | 72.99 | 762 | 80.37 | 739 | 77.94 | 742 | 78.26 | 742 | 78.26 | 735 | 77.56 | |
| Modena | 496 | 72.61 | 506 | 74.08 | 506 | 74.08 | 452 | 66.17 | 533 | 78.03 | 499 | 72.99 | |
| Ferrara | 265 | 80.76 | 262 | 79.85 | 282 | 85.94 | 290 | 88.38 | 256 | 78.02 | 271 | 82.59 | |
| Piacenza | 223 | 81.59 | 206 | 75.37 | 218 | 79.76 | 195 | 71.34 | 211 | 77.20 | 211 | 77.05 | |
| Forlì-Cesena | 253 | 65.18 | 284 | 73.17 | 255 | 65.70 | 285 | 73.43 | 297 | 76.52 | 275 | 70.80 | |
| Reggio Emilia | 392 | 74.45 | 399 | 75.78 | 392 | 74.45 | 408 | 77.49 | 380 | 72.17 | 394 | 74.87 | |
| TOTAL | 3149 | 73.81 | 3277 | 76.81 | 3292 | 77.16 | 3340 | 78.28 | 3378 | 79.17 | 3287 | 77.05 | |
| Piemonte | Alessandria | 316 | 80.79 | 337 | 86.16 | 315 | 80.53 | 306 | 78.23 | 297 | 75.93 | 314 | 80.33 |
| Vercelli | 111 | 67.41 | 118 | 71.67 | 108 | 65.59 | 107 | 64.98 | 121 | 73.49 | 113 | 68.63 | |
| Biella | 111 | 67.35 | 114 | 69.17 | 123 | 74.63 | 143 | 86.76 | 121 | 73.42 | 122 | 74.27 | |
| Novara | 249 | 68.65 | 248 | 68.38 | 289 | 79.68 | 257 | 70.86 | 262 | 72.24 | 261 | 71.96 | |
| Verbano-Cusio-Ossola | 117 | 77.38 | 108 | 71.43 | 109 | 72.09 | 100 | 66.14 | 100 | 66.14 | 107 | 70.64 | |
| Torino | 1346 | 62.31 | 1357 | 62.82 | 1383 | 64.03 | 1396 | 64.63 | 1396 | 64.63 | 1376 | 63.68 | |
| Cuneo | 307 | 54.25 | 309 | 54.60 | 342 | 60.43 | 332 | 58.67 | 341 | 60.26 | 326 | 57.64 | |
| Asti | 135 | 66.66 | 128 | 63.20 | 127 | 62.71 | 111 | 54.81 | 119 | 58.76 | 124 | 61.23 | |
| TOTAL | 2692 | 64.66 | 2719 | 65.31 | 2796 | 67.16 | 2752 | 66.11 | 2757 | 66.23 | 2743 | 65.89 | |
| Liguria | La Spezia | 175 | 86.82 | 180 | 89.30 | 160 | 79.38 | 153 | 75.90 | 165 | 81.86 | 167 | 82.65 |
| Genova | 599 | 78.90 | 679 | 89.44 | 649 | 85.49 | 545 | 71.79 | 596 | 78.51 | 614 | 80.83 | |
| Savona | 194 | 77.39 | 193 | 76.99 | 207 | 82.57 | 179 | 71.40 | 187 | 74.59 | 192 | 76.59 | |
| Imperia | 147 | 76.21 | 185 | 95.91 | 150 | 77.77 | 139 | 72.06 | 131 | 67.92 | 150 | 77.97 | |
| TOTAL | 1115 | 79.40 | 1237 | 88.09 | 1166 | 83.03 | 1016 | 72.35 | 1079 | 76.84 | 1123 | 79.94 | |
| Friuli Venezia Giulia | Udine | 381 | 74.10 | 419 | 81.49 | 404 | 78.57 | 376 | 73.13 | 397 | 77.21 | 395 | 76.90 |
| Pordenone | 232 | 74.00 | 221 | 70.49 | 193 | 61.56 | 203 | 64.75 | 238 | 75.91 | 217 | 69.34 | |
| Trieste | 169 | 81.64 | 161 | 77.77 | 159 | 76.81 | 136 | 65.70 | 148 | 71.49 | 155 | 74.68 | |
| Gorizia | 116 | 88.62 | 111 | 84.80 | 106 | 80.98 | 103 | 78.69 | 83 | 63.41 | 104 | 79.30 | |
| TOTAL | 898 | 77.04 | 912 | 78.24 | 862 | 73.95 | 818 | 70.18 | 866 | 74.29 | 871 | 74.74 | |
| Trentino-Alto Adige | Trento | 334 | 64.51 | 319 | 61.61 | 366 | 70.69 | 320 | 61.80 | 373 | 72.04 | 342 | 66.13 |
| Bolzano | 247 | 47.60 | 245 | 47.22 | 260 | 50.11 | 226 | 43.55 | 269 | 51.84 | 249 | 48.06 | |
| TOTAL | 581 | 56.05 | 564 | 54.41 | 626 | 60.39 | 546 | 52.66 | 642 | 61.93 | 592 | 57.09 | |
| Valle d’Aosta | Aosta | 88 | 70.63 | 92 | 73.84 | 78 | 62.60 | 82 | 65.81 | 73 | 58.59 | 83 | 66.29 |
| Total Northern Italy | 18,232 | 70.26 | 18,767 | 72.32 | 18,720 | 72.14 | 17,983 | 69.30 | 18,124 | 67.61 | 14,625 | 70.33 | |
| Central Italy | |||||||||||||
| Lazio | Roma | 3555 | 87.10 | 3796 | 93.00 | 3804 | 93.20 | 3576 | 87.61 | 3436 | 84.18 | 3633 | 89.02 |
| Latina | 493 | 86.45 | 473 | 82.95 | 433 | 75.93 | 481 | 84.35 | 449 | 78.74 | 466 | 81.68 | |
| Frosinone | 417 | 83.53 | 406 | 81.32 | 421 | 84.33 | 416 | 83.33 | 378 | 75.72 | 408 | 81.65 | |
| Rieti | 139 | 92.91 | 120 | 80.21 | 119 | 79.54 | 132 | 88.23 | 105 | 70.18 | 123 | 82.21 | |
| Viterbo | 230 | 73.93 | 217 | 69.75 | 251 | 80.68 | 267 | 85.83 | 191 | 61.40 | 231 | 74.32 | |
| TOTAL | 4834 | 86.14 | 5012 | 89.31 | 5028 | 89.60 | 4872 | 86.82 | 4559 | 81.24 | 4861 | 86.62 | |
| Toscana | Livorno | 266 | 83.89 | 268 | 84.52 | 271 | 85.47 | 252 | 79.48 | 229 | 72.22 | 257 | 81.12 |
| Lucca | 269 | 72.02 | 326 | 87.29 | 297 | 79.52 | 289 | 77.38 | 264 | 70.68 | 289 | 77.38 | |
| Massa-Carrara | 142 | 74.87 | 175 | 92.27 | 167 | 88.06 | 145 | 76.46 | 130 | 68.55 | 152 | 80.04 | |
| Pisa | 295 | 72.63 | 317 | 78.04 | 311 | 76.56 | 274 | 67.46 | 276 | 67.95 | 295 | 72.53 | |
| Firenze | 627 | 68.02 | 651 | 70.62 | 648 | 70.30 | 651 | 70.62 | 596 | 64.66 | 635 | 68.84 | |
| Siena | 177 | 69.87 | 182 | 71.84 | 145 | 57.24 | 165 | 65.13 | 161 | 63.55 | 166 | 65.53 | |
| Pistoia | 187 | 66.85 | 192 | 68.64 | 212 | 75.79 | 173 | 61.84 | 177 | 63.27 | 188 | 67.28 | |
| Prato | 166 | 66.79 | 137 | 55.12 | 134 | 53.91 | 167 | 67.19 | 157 | 63.16 | 152 | 61.23 | |
| Arezzo | 246 | 73.49 | 224 | 66.92 | 194 | 57.96 | 214 | 63.93 | 204 | 60.95 | 216 | 64.65 | |
| Grosseto | 162 | 79.47 | 161 | 78.98 | 160 | 78.49 | 134 | 65.73 | 124 | 60.83 | 148 | 72.70 | |
| TOTAL | 257 | 71.90 | 2633 | 74.62 | 2539 | 71.96 | 2464 | 69.83 | 2318 | 65.70 | 2042 | 70.80 | |
| Marche | Ancona | 350 | 76.05 | 399 | 86.70 | 365 | 79.31 | 369 | 80.18 | 392 | 85.18 | 375 | 81.48 |
| Pesaro-Urbino | 299 | 82.85 | 281 | 77.86 | 293 | 81.19 | 275 | 76.20 | 289 | 80.08 | 287 | 79.64 | |
| Fermo | 127 | 75.49 | 125 | 74.31 | 126 | 74.90 | |||||||
| Ascoli Piceno | 302 | 147.68 | 296 | 144.75 | 324 | 158.44 | 139 | 67.97 | 144 | 70.42 | 241 | 117.85 | |
| Macerata | 256 | 82.84 | 217 | 70.22 | 274 | 88.66 | 226 | 73.13 | 217 | 70.22 | 238 | 77.01 | |
| TOTAL | 1207 | 90.44 | 1193 | 89.39 | 1256 | 94.11 | 1136 | 75.59 | 1167 | 77.65 | 1192 | 85.44 | |
| Abruzzo | L’Aquila | 250 | 84.50 | 288 | 97.35 | 226 | 76.39 | 215 | 72.67 | 209 | 70.64 | 238 | 80.31 |
| Pescara | 212 | 67.48 | 221 | 70.34 | 214 | 68.11 | 210 | 66.84 | 217 | 69.07 | 215 | 68.37 | |
| Teramo | 225 | 72.41 | 208 | 66.94 | 219 | 70.48 | 216 | 69.51 | 213 | 68.55 | 216 | 69.58 | |
| Chieti | 254 | 66.72 | 261 | 68.56 | 253 | 66.46 | 238 | 62.52 | 238 | 62.52 | 249 | 65.36 | |
| TOTAL | 941 | 72.30 | 978 | 75.15 | 912 | 70.08 | 879 | 67.54 | 877 | 67.39 | 917 | 70.49 | |
| Umbria | Terni | 143 | 66.97 | 188 | 88.05 | 194 | 90.86 | 181 | 84.77 | 172 | 80.55 | 176 | 82.24 |
| Perugia | 419 | 65.76 | 484 | 75.96 | 492 | 77.21 | 521 | 81.77 | 478 | 75.02 | 479 | 75.14 | |
| TOTAL | 562 | 66.06 | 672 | 78.99 | 686 | 80.64 | 702 | 82.52 | 650 | 76.41 | 654 | 76.92 | |
| Molise | Campobasso | 189 | 85.28 | 200 | 90.24 | 187 | 84.38 | 190 | 85.73 | 165 | 74.45 | 186 | 84.02 |
| Isernia | 66 | 76.81 | 53 | 61.68 | 65 | 75.64 | 63 | 73.31 | 60 | 69.82 | 61 | 71.45 | |
| TOTAL | 255 | 82.91 | 253 | 82.26 | 252 | 81.94 | 253 | 82.26 | 225 | 73.16 | 248 | 80.51 | |
| Total Central Italy | 10,336 | 79.91 | 10,741 | 83.04 | 10,673 | 82.52 | 10,306 | 78.65 | 9796 | 74.76 | 10,370 | 79.78 | |
| Southern Italy | |||||||||||||
| Campania | Napoli | 2482 | 77.47 | 2353 | 73.45 | 2416 | 75.41 | 2358 | 73.60 | 2382 | 74.35 | 2398 | 74.86 |
| Caserta | 659 | 67.93 | 680 | 70.09 | 699 | 72.05 | 650 | 67.00 | 679 | 69.99 | 673 | 69.41 | |
| Salerno | 730 | 64.81 | 804 | 71.38 | 795 | 70.58 | 804 | 71.38 | 773 | 68.63 | 781 | 69.36 | |
| Avellino | 313 | 71.48 | 309 | 70.57 | 320 | 73.08 | 319 | 72.85 | 277 | 63.26 | 308 | 70.25 | |
| Benevento | 193 | 67.73 | 210 | 73.69 | 211 | 74.04 | 183 | 64.22 | 153 | 53.69 | 190 | 66.67 | |
| TOTAL | 4377 | 72.67 | 4356 | 72.32 | 4441 | 73.73 | 4314 | 71.62 | 4264 | 70.79 | 4350 | 72.23 | |
| Sicilia | Messina | 557 | 85.84 | 527 | 81.21 | 512 | 78.90 | 491 | 75.66 | 535 | 82.44 | 524 | 80.81 |
| Caltanissetta | 206 | 75.25 | 184 | 67.21 | 199 | 72.69 | 218 | 79.63 | 219 | 80.00 | 205 | 74.96 | |
| Enna | 137 | 80.20 | 123 | 72.01 | 161 | 94.25 | 126 | 73.76 | 136 | 79.62 | 137 | 79.97 | |
| Catania | 1011 | 91.17 | 918 | 82.78 | 951 | 85.76 | 874 | 78.81 | 864 | 77.91 | 924 | 83.29 | |
| Siracusa | 288 | 69.90 | 307 | 74.51 | 317 | 76.93 | 304 | 73.78 | 288 | 69.90 | 301 | 73.00 | |
| Agrigento | 312 | 69.97 | 270 | 60.55 | 266 | 59.65 | 306 | 68.62 | 299 | 67.05 | 291 | 65.17 | |
| Palermo | 854 | 67.62 | 835 | 66.11 | 824 | 65.24 | 799 | 63.26 | 803 | 63.58 | 823 | 65.16 | |
| Trapani | 265 | 62.52 | 299 | 70.54 | 264 | 62.28 | 238 | 56.15 | 244 | 57.56 | 262 | 61.81 | |
| Ragusa | 201 | 63.70 | 178 | 56.41 | 248 | 78.59 | 208 | 65.91 | 171 | 54.19 | 201 | 63.76 | |
| TOTAL | 3831 | 75.67 | 3641 | 71.92 | 3742 | 73.91 | 3564 | 70.39 | 3559 | 70.30 | 3667 | 72.44 | |
| Puglia | Lecce | 648 | 81.48 | 660 | 82.98 | 650 | 81.73 | 644 | 80.97 | 625 | 78.58 | 645 | 81.15 |
| Taranto | 465 | 77.83 | 431 | 72.14 | 427 | 71.47 | 424 | 70.97 | 457 | 76.49 | 441 | 73.78 | |
| Bari | 1180 | 91.83 | 1213 | 94.40 | 1219 | 94.87 | 926 | 72.07 | 977 | 76.04 | 1103 | 85.84 | |
| Foggia | 487 | 77.00 | 487 | 77.00 | 439 | 69.41 | 489 | 77.32 | 455 | 71.94 | 471 | 74.53 | |
| Brindisi | 300 | 74.06 | 300 | 74.06 | 298 | 73.57 | 290 | 71.59 | 281 | 69.37 | 294 | 72.53 | |
| Barletta-Andria-Trani | 248 | 59.88 | 269 | 64.95 | 259 | 62.42 | |||||||
| TOTAL | 3080 | 82.90 | 3091 | 83.20 | 3033 | 81.64 | 3021 | 81.32 | 3064 | 82.47 | 3058 | 67.41 | |
| Calabria | Cosenza | 473 | 64.64 | 513 | 70.10 | 477 | 65.18 | 514 | 70.24 | 541 | 73.93 | 504 | 68.82 |
| Catanzaro | 255 | 69.53 | 263 | 71.71 | 218 | 59.44 | 253 | 68.98 | 246 | 67.07 | 247 | 67.35 | |
| Reggio Calabria | 391 | 69.81 | 424 | 75.70 | 372 | 66.42 | 364 | 64.99 | 369 | 65.88 | 384 | 68.56 | |
| Crotone | 128 | 72.92 | 123 | 70.07 | 95 | 54.12 | 113 | 64.37 | 115 | 65.51 | 115 | 65.40 | |
| Vibo Valentia | 120 | 72.94 | 119 | 72.34 | 106 | 64.43 | 91 | 55.32 | 97 | 58.96 | 107 | 64.80 | |
| TOTAL | 1367 | 68.40 | 1442 | 72.15 | 1268 | 63.44 | 1335 | 66.79 | 1368 | 68.44 | 1356 | 67.84 | |
| Sardegna | Ogliastra | 48 | 82.63 | 37 | 63.69 | 48 | 82.63 | 46 | 79.19 | 56 | 96.40 | 47 | 80.91 |
| Carbonia-Iglesias | 141 | 110.42 | 122 | 95.54 | 112 | 87.71 | 136 | 106.51 | 107 | 83.79 | 124 | 96.79 | |
| Olbia-Tempio | 119 | 73.83 | 115 | 71.35 | 104 | 64.53 | 133 | 82.52 | 131 | 81.28 | 120 | 74.70 | |
| Sassari | 278 | 82.78 | 282 | 83.97 | 265 | 78.91 | 265 | 78.91 | 270 | 80.40 | 272 | 80.99 | |
| Cagliari | 543 | 93.15 | 533 | 91.44 | 525 | 90.06 | 540 | 92.64 | 456 | 78.23 | 519 | 89.10 | |
| Oristano | 109 | 67.53 | 109 | 67.53 | 142 | 87.98 | 135 | 83.64 | 123 | 76.20 | 124 | 76.58 | |
| Nuoro | 167 | 105.65 | 159 | 100.59 | 133 | 84.14 | 122 | 77.18 | 119 | 75.29 | 140 | 88.57 | |
| Medio Campidano | 77 | 74.78 | 85 | 82.55 | 100 | 97.11 | 87 | 84.49 | 61 | 59.24 | 82 | 79.63 | |
| TOTAL | 1482 | 87.79 | 1442 | 85.42 | 1429 | 84.65 | 1464 | 86.72 | 1323 | 78.37 | 1428 | 84.59 | |
| Basilicata | Potenza | 245 | 64.55 | 249 | 65.60 | 253 | 66.65 | 278 | 73.24 | 281 | 74.03 | 261 | 68.81 |
| Matera | 156 | 77.33 | 134 | 66.43 | 148 | 73.37 | 140 | 69.40 | 121 | 59.98 | 140 | 69.30 | |
| TOTAL | 401 | 68.99 | 383 | 65.89 | 401 | 68.98 | 418 | 71.91 | 402 | 69.15 | 401 | 68.98 | |
| Total Southern Italy | 14,538 | 76.24 | 14,355 | 75.28 | 14,314 | 75.06 | 14,116 | 74.02 | 13,980 | 73.31 | 11,467 | 74.78 | |
Regional capitals are highlighted in bold.
The average annual number of hospitalizations due to all cancers in Italy was 2362 in pediatric populations (0–19 years old) and 43,141 in adults aged 20–49 years old. Women accounted for the majority of cancer cases in young adults 20–49 (data not presented). As expected, in terms of absolute number of hospitalizations, the biggest cities of Rome, Naples, and Milan display the highest values in both the examined age groups, followed by smaller cities (number of pediatric hospitalizations > 100) such as Turin, Bari, Salerno, Caserta, Catania and Palermo. All these cities were always at the top ten places in both the examined age groups, Particularly, Rome presented the highest average annual number of pediatric cancers (n = 392, SHR = 9.9), followed by Naples (n = 378; SHR = 9.9) and Milan (n = 212; SHR = 7.3). Rome displayed also the highest number of average annual hospitalizations due to cancer in young adults aged 20–49 years old (n = 3633; SHR = 89.0), followed by Milan (n = 2491; SHR = 82.4), Naples (n = 2398; SHR = 74.8), Turin (n = 1376; SHR = 63.6), and minor cities such as Bari (n = 1103; SHR = 85.8), Catania (n = 924; SHR = 83.2), Brescia (n = 906; SHR = 71.1), Salerno (n = 781; SHR = 69.3), Bologna (n = 735; SHR = 77.5), Caserta (n = 673; SHR = 69.4), Lecce (n = 645; SHR = 81.1), Bergamo (n = 645; SHR = 57.5), Florence (n = 635; SHR = 68.8), Padova (n = 629; SHR = 66.9), Verona (n = 617; SHR = 67.2), Genova (n = 614; SHR = 80.0).
When looking only at SHR of pediatric cancers, minor cities (i.e. Imperia, Isernia and others) presented values >10 per 100,000, with only 20 cases per year. Despite huge differences in the number of hospitalizations, when looking at the SHR in pediatric patients, the highest values (≥8 per 100,000) were recorded in provinces belonging to well defined areas: Isernia, Naples, Caserta, Salerno, Avellino (region Molise and Campania); Rome, Frosinone, Rieti, Latina, Viterbo and Terni (Region Lazio and Umbria); Bari, Foggia, Barletta/Andria and Brindisi (Puglia); L’Aquila, Teramo, Chieti, Ascoli Piceno (Abruzzo and Marche); Parma (Emilia Romagna); Aosta (Val d’Aosta Region); Vercelli, and Imperia (Piemonte and Liguria); Cagliari, Oristano, Ogliastra, Medio Campidano (Sardinia); Catania, Messina, Trapani, Enna, Caltanissetta (Sicily).
Similarly, also when looking at the SHR in adult patients aged 20–49 years old, the highest values (≥75 per 100,000) were displayed in the entire Sardinia island, Liguria and Marche Region, and in the following Provinces: Milan, Alessandria, Udine, Gorizia, Ravenna, Ferrara, Rimini, Piacenza, Rovigo, Bologna and Parma (in Northern Italy); Rome, Frosinone, Rieti, Latina, L’Aquila, Lucca, Livorno, Massa-Carrara, Perugia and Terni (Central Italy); Messina, Enna, Caltanissetta, Catania, Campobasso, Bari and Lecce (in Southern Italy).
Women always presented SHR values higher than men (data not presented). Figure 2 and Figure 3 show on a map the average annual value of standardized hospitalization rate (SHR) per 100,000 inhabitants per province in pediatric population aged 0–19 and in young adults 20–49 due to all cancers.
Figure 2.

Standardized Hospitalization Rate (SHR) per 100,000 per each Italian province due to main diagnosis of cancer diagnosis of (all tumors) in pediatric population (0–19 years old).
Figure 3.

Standardized Hospitalization Rate (SHR) per 100,000 inhabitants per each Italian province due to main diagnosis of cancer (all tumors) in adults aged 20–49 years old.
4. Discussion
Our objective was to provide a preliminary tabulation of hospitalizations occurred in Italy from 2007 to 2011. The specific goal of our study was to look at the hospitalizations due to all cancers in the Italian provinces, with specific focus on youngest age groups, namely pediatric population and adults ≤50 years old, which are not covered by screening campaigns. The aim was to provide some data about the hospital admissions of cancer patients including those areas where cancer registries (CRs) have not been activated or provide only a partial population coverage. Actually, more than 50% of the Italian population is not covered by CRs and therefore no data are available on cancer incidence rates concerning all the regions, especially for Southern Italy.
Since the potential and limitations of CRs and HDR have already been addressed [8,9,10,11,12,13,14,15,16], this work might provide a first rough general picture about the burden of cancer in Italy concerning younger people, based on real official national data such as hospitalization records. We were not still able to split the database for many age groups (the analyses by smaller age groups will be presented in future publications). The decision to focus on pediatric population (0–19 years old) and young adults (20–49 years old) is closely related to the need of providing information about the possible impact of environmental threats to human health coming from the carcinogen substances officially classified by IARC (International Agency for Cancer Research, Lyon, France) [19]. Among those, special attention should be paid to fine and coarse particulate pollution, whose cardiovascular, respiratory and cancer effects on human health arise even after exposure below the legal thresholds and have been investigated in many big cities across Europe, including Rome [20,21,22]. However, it was not the aim of this study to specifically look at causal relations between tumors and environmental or personal exposures.
Recent reports of a significant increase in childhood cancer in Europe [2] and especially Italy [23] has caused concern, pushing some authors to critically reconsider this dominant model of carcinogenesis [24] and to reconsider quality, comparability and methods of analysis of data on childhood cancer [25]. Cancer has become the leading cause of death among children over the first year of age. Even after adjusting for population growth and improved detection of certain types of cancer, we have observed an increased in childhood cancer over the past 40 years. A large increase in cancer cases has been specifically documented in the first year of age, suggesting that the cancers may originate from maternal and fetal exposure to pro-carcinogenic agents, or have an epigenetic or gametic origin [2,26]. These data suggest that exposure to carcinogens from pollution could play a bigger role in causing children cancer than that played by unhealthy personal habits in adults (i.e., cigarette smoking)”.
Looking only at “rates” might be restrictive when assessing the global burden of cancer diseases and the perception by population. When examining cancer rates in the Campania Region, a big city such as Naples with about 300 new cases per year could show a SHR similar to those of smaller towns with 10–20 new cases per year. For example, the SHR in the large city of Naples was 8.89 in year 2011, which is smaller than the SHR of the smaller town of Isernia with an SHR of 10.43. However, on an absolute scale, more than 300 cases of pediatric cancer would arise in Naples in a single year, which is much higher than 8 pediatric cases per year hospitalized in Isernia. This perceived difference in the number of cancer cases in the population of Naples could contribute to public alarm and panic. Similarly, the overall 280 hospitalizations due to pediatric cancer in Milan (SHR 2011: 5.37) are not considered as a particular problem compared to the 20 cases of Teramo (SHR 2011: 5.73) when looking only at “rates”. We should also look at the problem from an ethical point of view: if we consider as “normal” that cities with a higher number of children must have more incident cancer cases, it could be questioned if we can accept in our society that “more children means more tumors”.
It is interesting to point out that public perception acts in a completely different way (no social alarm) in other areas presenting even more relevant number of pediatric hospitalizations, such as Rome and surroundings (more than 300 new cases per year on average only in the capital city). This would probably suggests that information provided to the population (i.e., the discovery of a huge number of illegal deposits or dumping sites, incineration of dangerous wastes) contribute to create panic and social alarm. Beyond the social consequences of having more children or adults suffering from cancer, we believe it is important for decision makers to have information about the absolute number of cancer cases in order to provide adequate both in-the hospital and in-home-based healthcare facilities to take care of a huge number of patients.
In this paper, we have presented our data per province and for all cancer types. Of course, we are aware that the highest observed hospitalization rates could reflect problems that are specifically attributable to the biggest cities or to single towns within the province (with the rest of the area not being responsible for the increased rates). In addition, particularly high values of SHR observed in smaller provinces might be the consequence of the higher incidence of specific tumors related to particular (environmental or professional) exposures typical of that territory. Of course, only local CRs are able to accomplish this level of characterization. This is the case of Taranto, where the local cancer registry has recorded higher incidence rates of pediatric tumors than those found out in our analyses [27]. Particular attention should be paid to the higher incidence of cancer in adults (mostly women) in the entire Sardinia Island, where the activity of CRs is still at the initial stages.
We believe that cancer hospitalization data per province presented in this study may provide a first interesting rough picture of the global problem, that can be further and deeper investigated through the use of local CRs (where and when available). We are also aware that the use of hospitalization records for epidemiological purposes present a series of limitations mainly consisting in the unavoidable “false negative cases”: cancer patients who are not hospitalized because treated at ambulatorial level and consequently not included in the national hospitalizations database. Despite hospitalization records have not been conceived as a primary epidemiological instrument but as an administrative tool, they are completed only after histological exam has allowed a final diagnosis. Therefore, the use of hospitalization records for epidemiological purposes is particularly valuable. Of course, there is the possibility of an under-estimation produced in our study by the presence of cancer patient not hospitalized, which can be detected only by CRs as gold standard methodology. However, the aim of this study was to provide a first picture of the phenomenon at national level, including also those areas not covered by CRs, which could provide detailed data once activated.
It is interesting to point out that our findings about the incidence of all pediatric cancer in Italy (with about 11,800 new cases per year over a 5-year period) are consistent with AIRTUM projections for years 2016–2020 which estimate about 11,000 new cases of cancer in the age group 0–19 in the National Association of Cancer Registries 2013 Report [28].
Data presented in this paper might represent an initial step which should encourage scientists and public bodies to assess the causes of the increasing cancer hospitalization rates in different Italian areas, with the ending of the traditional gap between Northern and Southern Italy in the field of cancer diseases. The role played by environmental pollutants [29], food and water contamination (i.e., pesticides use, toxic wastes, heavy metals, dioxins and others), nutritional, professional and other personal habits should be investigated. Finally, the higher SHR rates displayed in our study in young women (compared to men) aged 20–49 years old should be considered as a very interesting finding, as it is only partially likely to be the effect of population screening campaigns. Actually, mammographic screening campaigns involve older females aged >50 years old and only tests for the prevention of uterine cervix cancer are performed at younger age. Therefore, this latter finding could probably reflect a higher incidence of some specific female tumors (i.e., breast and thyroid cancer) as suggested by AIRTUM Reports in the younger age groups [28,30,31].
5. Conclusions
Despite the limitations due to the possible underestimation of cancer incidence, it is feasible and potentially useful to use hospitalization records as secondary data source where cancer registries do not cover an entire province or region, in order to provide preliminary information of cancer burden. As expected, the biggest Italian cities showed the highest number of hospitalizations, with well-defined areas being characterized by more pronounced SHR. In addition to the SHR, the absolute number of new cancer cases represents a crucial information for a global assessment of the problem (including healthcare, social, environmental and other evaluations) as well as for adequate planning of healthcare services by decision makers at regional level. Our results over a 5-year period are consistent with AIRTUM projections for years 2016–2020 and call for specific risk assessment programs at local level to search for causal relations with environmental and personal or professionals exposures, that should performed on cancer registries data and case-control studies as the most qualified tool for that.
Acknowledgments
This paper is a result of institutional research activities of Medicina Futura Research (IOS/Coleman Ltd., Naples, Italy) in cooperation with the Euro Mediterranean Scientific Biomedical Institute (ISBEM, Brindisi, Italy) and the International Society Doctors for the Environment (ISDE). The EPIKIT (Epidemiology of Cancer in Italy) Study Group is a result of the COHEIRS project (Civic Observers for Health and Environment: Initiative of Responsibility and Sustainibility), funded by the Europe for Citizens Program 2013–2014 to address the issue of Precautionary Principle application. The COHEIRS Project is coordinated at European Level by the Association of Local Democracy Agency (ALDA) in Strasbourg and it is implemented in Italy by ISBEM and ISDE. Authors are grateful to the ALDA General Director Antonella Valmorbida and to ALDA staff, especially to Marco Boaria, Anna Ditta and Aldo Xhani for their support in carrying out COHEIRS project, as well as to Donato Cafagna (Delegate of Italian Government for environmental affairs in Campania).
Author Contributions
All authors provided substantial contribution to the production, analysis and interpretation of the results. Prisco Piscitelli, Immacolata Marino, Andrea Falco, Matteo Rivezzi, Roberto Romano, Restituta Mazzella, Cosimo Neglia, Giulia Della Rosa, Giuseppe Pellerano, Giuseppe Militerno, Adriana Bonifacino, Gaetano Rivezzi, Roberto Romizi, Giuseppe Miserotti, Maurizio Montella, Fabrizio Bianchi, Alessandra Marinelli, Antonella De Donno, Giovanni De Filippis, Giuseppe Serravezza, Gianluca Di Tanna, Dennis Black, Valerio Gennaro, Mario Ascolese, Alessandro Distante, Ernesto Burgio, Massimo Crespi, Annamaria Colao have conceived the study together and contributed to write and prepare the manuscript before the final approval and submission. Prisco Piscitelli, Immacolata Marino, Andrea Falco, Roberto Romano, Restituta Mazzella, Cosimo Neglia, Giulia Della Rosa, Giuseppe Militerno, Gianluca Di Tanna, Valerio Gennaro, Massimo Crespi performed the statistical analyses.
Conflicts of Interest
The authors declare no conflict of interest.
References
- 1.Treccani Editors . Treccani Enciclopedic Dictionary. Treccani; Rome, Italy: 1954. [Google Scholar]
- 2.Steliarova-Foucher E., Stiller C., Kaatsch P., Berrino F., Coebergh J.W., Lacour B., Parkin M. Geographical patterns and time trends of cancer incidence and survival among children and adolescents in Europe since the 1970s (the ACCIS project): An epidemiological study. Lancet. 2004;364:2097–2105. doi: 10.1016/S0140-6736(04)17550-8. [DOI] [PubMed] [Google Scholar]
- 3.Jensen O.M., Whelan S. Planning a cancer registry. IARC Sci. Publ. 1991;95:22–28. [PubMed] [Google Scholar]
- 4.AIRT Working Group Italian cancer figures, report 2014. Epidemiol. Prev. 2014;38:1–122. [PubMed] [Google Scholar]
- 5.Verdecchia A., Capocaccia R., Egidi V., Golini A. A method for the estimation of chronic disease morbidity and trends from mortality data. Stat. Med. 1989;8:201–216. doi: 10.1002/sim.4780080207. [DOI] [PubMed] [Google Scholar]
- 6.De Angelis G., De Angelis R., Frova L., Verdecchia A. MIAMOD: A computer package to estimate chronic disease morbidity using mortality and survival data. Comput. Methods Programs Biomed. 1994;44:99–107. doi: 10.1016/0169-2607(94)90091-4. [DOI] [PubMed] [Google Scholar]
- 7.Miller M., Swan J. SEER doubles coverage by adding registries for four states. J. Natl. Cancer Inst. 2001;93:500. doi: 10.1093/jnci/93.7.500. [DOI] [PubMed] [Google Scholar]
- 8.Ellekjaer H., Holmen J., Kruger O., Terent A. Identification of incident stroke in Norway: Hospital discharge data compared with a population-based stroke register. Stroke. 1999;30:56–60. doi: 10.1161/01.STR.30.1.56. [DOI] [PubMed] [Google Scholar]
- 9.Mahonen M., Salomaa V., Brommels M., Molarius A., Miettinen H., Pyorala K., Tuomilehto J., Arstila M., Kaarsalo E., Ketonen M., et al. The validity of hospital discharge register data on coronary heart disease in Finland. Eur. J. Epidemiol. 1997;13:403–415. doi: 10.1023/A:1007306110822. [DOI] [PubMed] [Google Scholar]
- 10.Du X., Freeman J.L., Warren J.L., Nattinger A.B., Zhang D., Goodwin J.S. Accuracy and completeness of medicare claims data for surgical treatment of breast cancer. Med. Care. 2000;38:719–727. doi: 10.1097/00005650-200007000-00004. [DOI] [PubMed] [Google Scholar]
- 11.Icks A., Haastert B., Wildner M., Becker C., Meyer G. Trend of hip fracture incidence in Germany 1995–2004: A population-based study. Osteoporos. Int. 2008;19:1139–1145. doi: 10.1007/s00198-007-0534-6. [DOI] [PubMed] [Google Scholar]
- 12.Piscitelli P., Barba M., Crespi M., Di Maio M., Santoriello A., D’Aiuto M., Fucito A., Losco A., Pentimalli F., Maranta P., et al. The burden of breast cancer in Italy: Mastectomies and quadrantectomies performed between 2001 and 2008 based on nationwide hospital discharge records. J. Exp. Clin. Cancer Res. 2012;31:96. doi: 10.1186/1756-9966-31-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cooper G.S., Yuan Z., Stange K.C., Dennis L.K., Amini S.B., Rimm A.A. Agreement of medicare claims and tumor registry data for assessment of cancer-related treatment. Med. Care. 2000;38:411–421. doi: 10.1097/00005650-200004000-00008. [DOI] [PubMed] [Google Scholar]
- 14.Freeman J.L., Zhang D., Freeman D.H., Goodwin J.S. An approach to identifying incident breast cancer cases using medicare claims data. J. Clin. Epidemiol. 2000;53:605–614. doi: 10.1016/S0895-4356(99)00173-0. [DOI] [PubMed] [Google Scholar]
- 15.Penberthy L., McClish D., Pugh A., Smith W., Manning C., Retchin S. Using hospital discharge files to enhance cancer surveillance. Am. J. Epidemiol. 2003;158:27–34. doi: 10.1093/aje/kwg108. [DOI] [PubMed] [Google Scholar]
- 16.Piscitelli P., Santoriello A., Buonaguro F.M., Di Maio M., Iolascon G., Gimigliano F., Marinelli A., Distante A., Serravezza G., Sordi E., et al. Incidence of breast cancer in Italy: Mastectomies and quadrantectomies performed between 2000 and 2005. J. Exp. Clin. Cancer Res. 2009;28:86. doi: 10.1186/1756-9966-28-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Piscitelli P., Chitano G., Andreano G., Caroppo O., Andreano S., Gualtieri D., Rasinger M., Seclì M., Melissano A., De Giorgi A., et al. Dal Salento un esempio di Cittadinanza Scientifica. Epidemiol. Prev. 2013;37:3. [Google Scholar]
- 18.Piemonte EPAo: Healthcare Indicators in Piemonte Region. [(accessed on 20 April 2017)]; Available online: https://www.arpa.piemonte.it/reporting/indicatori-on_line/qualita-della-vita/salute_dimissioni-ospedaliere.
- 19.Samet J.M. The IARC monographs: Critics and controversy. Carcinogenesis. 2015;36:707–709. doi: 10.1093/carcin/bgv062. [DOI] [PubMed] [Google Scholar]
- 20.Beelen R., Raaschou-Nielsen O., Stafoggia M., Andersen Z.J., Weinmayr G., Hoffmann B., Wolf K., Samoli E., Fischer P., Nieuwenhuijsen M., et al. Effects of long-term exposure to air pollution on natural-cause mortality: An analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet. 2014;383:785–795. doi: 10.1016/S0140-6736(13)62158-3. [DOI] [PubMed] [Google Scholar]
- 21.Cesaroni G., Badaloni C., Gariazzo C., Stafoggia M., Sozzi R., Davoli M., Forastiere F. Long-term exposure to urban air pollution and mortality in a cohort of more than a million adults in Rome. Environ. Health Perspect. 2013;121:324–331. doi: 10.1289/ehp.1205862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stafoggia M., Faustini A., Rognoni M., Tessari R., Cadum E., Pacelli B., Pandolfi P., Miglio R., Mallone S., Vigotti M.A., et al. Air pollution and mortality in ten Italian cities, results of the EpiAir project. Epidemiol. Prev. 2009;33:65–76. [PubMed] [Google Scholar]
- 23.AIRTUM Report 2008—Tumors in children: Incidence, survival, temporal trends. Epidemiol. Prev. 2008;32:1–112. [Google Scholar]
- 24.Burgio E., Migliore L. Towards a systemic paradigm in carcinogenesis: Linking epigenetics and genetics. Mol. Biol. Rep. 2015;42:777–790. doi: 10.1007/s11033-014-3804-3. [DOI] [PubMed] [Google Scholar]
- 25.Steliarova-Foucher E., Kaatsch P., Lacour B., Pompe-Kirn V., Eser S., Miranda A., Danzon A., Ratiu A., Parkin D.M. Quality, comparability and methods of analysis of data on childhood cancer in Europe (1978–1997): Report from the Automated Childhood Cancer Information System project. Eur. J. Cancer. 2006;42:1915–1951. doi: 10.1016/j.ejca.2006.05.007. [DOI] [PubMed] [Google Scholar]
- 26.Greaves M. Pre-natal origins of childhood leukemia. Rev. Clin. Exp. Hematol. 2003;7:233–245. [PubMed] [Google Scholar]
- 27.Cannone G.A., Lo Monaco M.G., Carone S., Melcarne A., Tanzarella M., Bisceglia L., Ardizzone A., Minerba S., Quarta F., Coviello V., et al. Childhood cancer incidence in Apulia Region (Southern Italy), 2003–2008. Epidemiol. Prev. 2015;39:176–182. [PubMed] [Google Scholar]
- 28.AIRTUM Working Group I tumori in Italia—Rapporto 2012, I tumori dei bambini e degli adolescenti. Tumors in Italy: Pediatric cancers. Epidemiol. Prev. 2013;37:1–225. [Google Scholar]
- 29.Piscitelli P., Muscogiuri G., Colao A. Environment and health: Not only cancer. Int. J. Environ. Res. Public Health. 2016;13 doi: 10.3390/ijerph13070724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Quaglia A., Lillini R., Crocetti E., Buzzoni C., Vercelli M. Incidence and mortality trends for four major cancers in the elderly and middle-aged adults: An international comparison. Surg. Oncol. 2013;22:e31–e38. doi: 10.1016/j.suronc.2013.02.010. [DOI] [PubMed] [Google Scholar]
- 31.Michelozzi P., Schifano P. Childood cancers, risk factors and investigations models for the evaluation of spatio-temporal clusters. Epidemiol. Prev. 2016;40:28–30. doi: 10.19191/EP16.5S2.P001.096. [DOI] [PubMed] [Google Scholar]