

Abstract
The study was aimed to characterize enterococci from various clinical specimens, to determine the antimicrobial susceptibility pattern, and to explore the association between virulence factors and antimicrobial resistance. A total of 283 clinical enterococcal isolates were speciated and subjected to antimicrobial susceptibility testing. Virulence factors (hemolysin, gelatinase, and biofilm production) were detected phenotypically. Of the 283 enterococci isolated, 12 species were identified; predominant species were Enterococcus faecalis (82.33%). High-level gentamicin (HLG) and vancomycin resistance were observed among 55.57% and 6.01% of enteroccal isolates, respectively. All vancomycin-resistant enterococci (VREs) were E. faecalis and had VanA phenotype and genotype. Hemolysin, gelatinase, and biofilm production were seen in 15.90%, 12.36%, and 13.43% of enterococcal isolates, respectively. Vancomycin and HLG resistance were observed in 0.35% and 61.86% of the enterococcal isolates producing virulence factors. Isolates resistant to HLG but susceptible to vancomycin expressed more virulent factors. Further research is required to reveal the complex interplay between drug resistance and virulence factors.
Keywords: Enterococcus, vancomycin resistant, virulence factors
INTRODUCTION
Enterococci have emerged as an increasingly important cause of nosocomial infections in the last decade.[1] Enterococci from clinical sources show an alarming increase with properties of intrinsic resistance to several antibiotics.[2] Until recently, vancomycin was virtually the only drug that could be consistently relied on for the treatment of infections caused by multidrug-resistant enterococci.[3] However, emergence of vancomycin-resistant enterococci (VREs) and their increasing prevalence worldwide has made it difficult to treat serious enterococcal infections.[2] Few species such as Enterococcus gallinarum and Enterococcus casseliflavus are intrinsically resistant to vancomycin,[2] so it becomes essential to identify these species to avoid inappropriate treatment with vancomycin. Along with the emergence of multidrug resistance, the presence of several virulence factors in enterococci is an emerging concept. However, there are limited Indian studies elucidating the relationship between antimicrobial resistance and virulence factors among enterococcal isolates.
Hence, the present study was designed to investigate the profile of enterococcus species, their antimicrobial resistance pattern, associated virulence factors, and the relationship between antimicrobial resistance and virulence factors among enterococcal isolates, which is quintessential for management and prevention of these bacteria in any healthcare facility.
MICROBIOLOGY REPORT
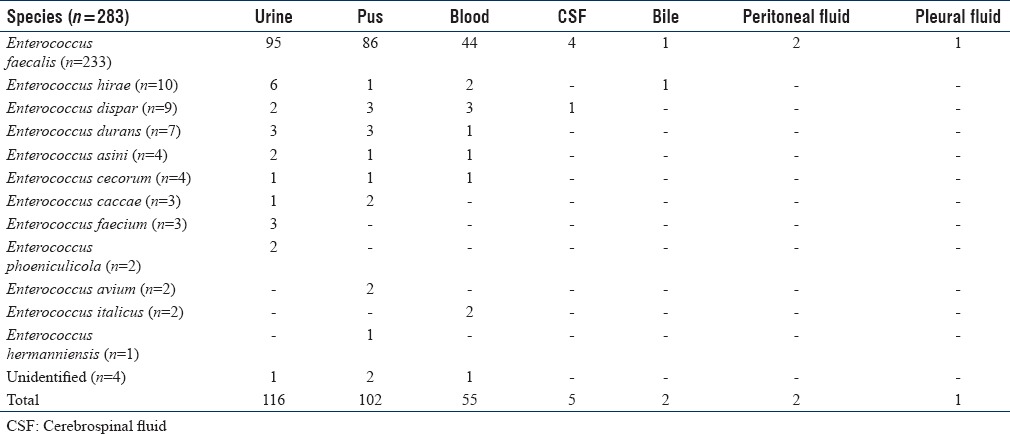
A total of 283 consecutive enterococcal isolates received from various clinical samples (blood, pus, urine and body fluid) over a period of 2 years from November 2013 to October 2015 were identified and speciated according to standard laboratory procedure as per the scheme of Facklam and Collins.[4] The clearance from the institutional ethics committee was obtained to carry out this study. The sources and the species of enterococcal isolates are summarized in Table 1. Four species could not be identified due to aberrant sugar reactions by conventional method.
Table 1.
Distribution of Enterococcus Species in Various Clinical Specimens
For studying the antimicrobial susceptibility pattern in enterococcal isolates, four methods were used (a) Kirby–Bauer disc diffusion technique,[5] (b) vancomycin screening agar method,[5] (c) minimum inhibitory concentration (MIC) testing by E strips, and (d) agar dilution method[5] for vancomycin.
For disc diffusion testing, ampicillin (10 μg), high-level gentamicin (HLG) (120 μg), erythromycin (15 μg), vancomycin (30 μg), teicoplanin (30 μg), and linezolid (15 μg) discs were used. For urine isolates, additional discs of levofloxacin (5 μg), norfloxacin (10 μg), and nitrofurantoin (300 μg) were used. Antimicrobial resistance pattern of enteroccal isolate from various clinical specimens is depicted in Table 2. On the basis of MIC of vancomycin (>64 μg/ml) and teicoplanin (>16 μg/ml), all vancomycin-resistant isolates were categorized as Van A phenotype. A total of 17 VREs were detected phenotypically as VanA.
Table 2.
Antimicrobial Resistance Pattern of Enterococci Isolates from Various Clinical Specimens

Polymerase chain reaction (PCR) was performed for detection of VanA gene among VRE isolates. Briefly, the 25 μl of PCR contained 2–4 well-isolated colonies, 2.5 μl, ×10 PCR buffer, 2 μl, 25 Mm MgCl2, 1 μl, 10 Mm dNTPs, 1 μl, 10 pm forward primer (5'GCGATATTCAAAGCTCAGCAA3') 1 μl, 10 pm reverse primer (5'TGCCGATTCAATTGCGTAGTC3'), 0.5 μl Taq DNA, and 17 μl nuclease-free water. Reaction was performed in thermocycler, and initial denaturation was done at 94°C for 4 min, followed by 30 cycles of denaturation at 94°C for 1 min, annealing at 51.70°C for 1 min, extension at 72°C for 1 min, and final extension done at 72°C for 7 min. Amplified PCR products were detected by 1.5% agarose gel electrophoresis.
All 17 VREs were detected phenotypically as VanA and were further confirmed by PCR as VanA genotype. One PCR product was sequenced. The GenBank accession number assigned to our sequence is KU 667286.
Virulence factors (hemolysin, gelatinase, and biofilm production) were detected phenotypically. Hemolysin production was detected in 5% blood agar.[6] Gelatinase activity was detected in 4% gelatin agar and clearing seen by mercuric chloride solution.[6] Biofilm formation was detected by tube method.[7] Among virulence factors tested, hemolysin was produced by 15.90%, biofilm by 13.43%, and gelatinase by 12.36% of the 283 enterococcal isolates. Relationships between enterococcal virulence and antimicrobial resistance are depicted in Table 3.
Table 3.
Relationships between Enterococcal Virulence and Antimicrobial Resistance
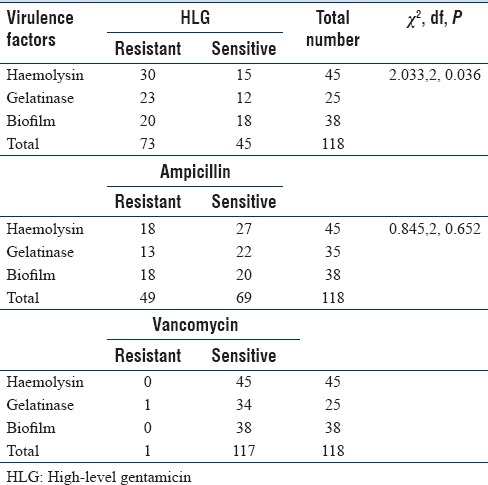
We observed that isolates resistant to HLG but susceptible to vancomycin expressed more virulence factors than vancomycin-resistant ones. This is in congruence with other studies from India.[8,9] The drug-resistant determinants in enterococcal and virulence genes are plasmid-borne with immense ability for genetic exchange both intragenically and intergenically.[10] It has been speculated that increase in one aspect of survival fitness reduces the other. Consequently acquisition of one set of plasmid may lead to loss of the other either due to incompatibility or due to fitness cost benefits.
CONCLUSION
Our study reveals the occurrence of a sizable number of HLG-resistant isolates and emergence of VRE. Linezolid demonstrated good antienterococcal activity and may be kept as the drug of choice for VRE isolates in our set up. Isolates resistant to HLG but susceptible to vancomycin expressed more virulence factors. Further research is required to reveal the complex interplay between drug resistance and virulence factors.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Fernandes SC, Dhanashree B. Drug resistance & virulence determinants in clinical isolates of Enterococcus species. Indian J Med Res. 2013;137:981–5. [PMC free article] [PubMed] [Google Scholar]
- 2.Prakash VP, Rao SR, Parija SC. Emergence of unusual species of enterococci causing infections, South India. BMC Infect Dis. 2005;5:14. doi: 10.1186/1471-2334-5-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cetinkaya Y, Falk P, Mayhall CG. Vancomycin-resistant enterococci. Clin Microbiol Rev. 2000;13:686–707. doi: 10.1128/cmr.13.4.686-707.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Facklam RR, Collins MD. Identification of Enterococcus species isolated from human infections by a conventional test scheme. J Clin Microbiol. 1989;27:731–4. doi: 10.1128/jcm.27.4.731-734.1989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.CLSI. CLSI Document M100-S22. PA: Clinical and Laboratory Standard Institute; 2012. Performance Standard for Antimicrobial Susceptibility Testing Twenty-second Informational Supplement; pp. 92–4. [Google Scholar]
- 6.Giridhara Upadhyaya PM, Umapathy BL, Ravikumar KL. Comparative study for the presence of enterococcal virulence factors gelatinase, hemolysin and biofilm among clinical and commensal isolates of Enterococcus faecalis. J Lab Physicians. 2010;2:100–4. doi: 10.4103/0974-2727.72159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mathur T, Singhal S, Khan S, Upadhyay DJ, Fatma T, Rattan A. Detection of biofilm formation among the clinical isolates of staphylococci: An evaluation of three different screening methods. Indian J Med Microbiol. 2006;24:25–9. doi: 10.4103/0255-0857.19890. [DOI] [PubMed] [Google Scholar]
- 8.Teixeira L, Carvalho M, Facklam R. Enterococcus. In: Murray P, Baron E, Jorgensen J, Landry M, Pfaller M, editors. Manual of Clinical Microbiology. 9th ed. Washington: ASM Press; 2007. pp. 434–5. [Google Scholar]
- 9.Tomita H, Pierson C, Lim SK, Clewell DB, Ike Y. Possible connection between a widely disseminated conjugative gentamicin resistance (pMG1-like) plasmid and the emergence of vancomycin resistance in Enterococcus faecium. J Clin Microbiol. 2002;40:3326–33. doi: 10.1128/JCM.40.9.3326-3333.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Banerjee T, Anupurba S. Prevalence of virulence factors and drug resistance in clinical isolates of enterococci: A study from North India. J Pathog. 2015;2015:692612. doi: 10.1155/2015/692612. [DOI] [PMC free article] [PubMed] [Google Scholar]