

Abstract
Purpose:
The aim of this study was to analyze the effect of postcollagen crosslinking (CXL) haze on the measurement and repeatability of pachymetry and mean keratometry (Km) of four corneal topographers.
Materials and Methods:
Sixty eyes of sixty patients with progressive keratoconus who had undergone accelerated CXL (ACXL) underwent imaging with a scanning slit imaging device (Orbscan II) and three Scheimpflug imaging devices (Pentacam HR, Sirius, and Galilei). Post-ACXL haze was measured using the densitometry software on the Pentacam HR. Readings of the thinnest corneal thickness (TCT) and Km from three scans of each device were analyzed. Effect of haze on the repeatability of TCT and Km measurements was evaluated using regression models. Repeatability was assessed by coefficient of variation.
Results:
Corneal densitometry in different zones affected the repeatability of TCT measurement of Orbscan (P < 0.05) significantly but not the repeatability of TCT with Pentacam HR and Sirius (P = 0.03 and 0.05, respectively). Km values were affected by haze when measured with the Pentacam HR (P < 0.05). The repeatability of Km readings for all devices was unaffected by haze. In the anterior 0–2 mm and 2–6 mm zone, TCT (P = 0.43 and 0.45, respectively), Km values (P = 0.4 and 0.6, respectively), repeatability of TCT (P = 0.1 in both zones), and Km (P = 0.5 and 0.1, respectively) with Galilei were found to be the most reliable.
Conclusion:
Galilei measurements appear to be least affected by post-ACXL haze when compared with other devices. Hence, topography measurements in the presence of haze need to be interpreted with caution.
Key words: Crosslinking, haze, repeatability
Over the past few decades, corneal collagen crosslinking (CXL) has become popular as a treatment modality to delay the progression of keratoconus.[1] Corneal haze is a common phenomenon that occurs after this procedure. It peaks between 1 and 3 months, and though it reduces over time, it does not always reach preoperative levels.[2] This haze is evident on slit-lamp examination and confocal microscopy but can be objectively quantified and expressed in grayscale units (GSU) of 0 (optically clear cornea/no haze) to 100 (total corneal opacity) using the densitometry map on the Pentacam (Oculus, Wetzlar, Germany).[2,3]
Corneal topography plays an integral role in the management and follow-up of several corneal conditions. Corneal pachymetry is particularly useful for the evaluation of endothelial functions and corneal biomechanics, accurate measurement of intraocular pressure, in calculating the residual stromal bed before refractive surgery and in the management of keratoconus.[4,5,6] We have defined progression in our earlier studies as an increase of 0.5 diopter (D) or more in two or more keratometric values in the steep meridian between two sagittal curve maps or a decrease in corneal thickness of 10% or more at the thinnest point between two pachymetry maps on Pentacam in the preceding 6 months; hence, it becomes important to accurately measure the corneal parameters including pachymetry after crosslinking in the presence of haze.[7] Likewise, changes in the anterior surface curvature (keratometry [Km]) correlate well with changes in visual acuity and quality.[8] Both pachymetry and Km have been extensively used for documenting the progression of keratoconus as well as to evaluate the effectiveness of CXL in stabilizing the disease.[9] In vivo confocal microscopy studies after CXL have revealed the cytotoxic effects of these procedures. The disappearance of keratocytes from the anterior and intermediate stroma due to apoptosis and photonecrosis phenomena with “lacunar” or “spongy” honeycomb-like edema in the early (1–6 months) and late (after 6 months) postoperative period of conventional and accelerated procedures has been noted.[10,11] Stromal haze is also a result of these complex structural and physiological wound-healing changes in the cornea.[3] Intraobserver and interobserver repeatability of pachymetry measurements obtained by different topographers has been proved to be good and comparable to the gold standard of ultrasound pachymetry.[12,13] These measurements have been performed in normal corneas, ectasias, keratoconus, or postrefractive surgery.
Corneal haze and stromal scarring are seen in patients who have undergone refractive surgeries and keratoplasties,[14,15,16] in active and healed stages of bacterial keratitis,[17] postprimary pterygium excision,[18] corneal dystrophy,[19] keratoconus, and post-CXL.[20,21,22] The haze that occurs after CXL differs from that seen in other conditions in both appearance and course.[23] It appears then that the underlying mechanism of haze is different for each condition. This in turn can have a variable influence on the measurement of parameters of commonly used topography devices. We therefore evaluated the effect of post-CXL haze on the repeatability of measuring the thinnest corneal thickness (TCT) and mean Km in patients with keratoconus who have undergone accelerated CXL (ACXL) using a combined scanning slit and Placido disc imaging device and three Scheimpflug-based topographers.
Materials and Methods
This cross-sectional observational study was approved by the Hospital's Ethics Committee and was performed according to the tenets of the Declaration of Helsinki after obtaining a written informed consent from all patients. Patients with documented evidence of progressive keratoconus who underwent ACXL with no intraoperative or postoperative complications were included in the study. Patients with advanced keratoconus, corneal scars, active or history of allergic eye diseases, dry eye syndrome, posterior blepharitis, delayed epithelial healing following CXL, and other ocular comorbidities were excluded from the study.
One year after patients underwent ACXL, a complete ophthalmic examination including slit-lamp examination, uncorrected and corrected distance visual acuity, and subjective refraction was done. All patients underwent corneal topography with the following topographers: Orbscan II (Orbtek, Salt-Lake City, UT, USA) based on a combined scanning slit and Placido disc technology; Pentacam HR (Oculus, Wetzlar, Germany) based on the Scheimpflug principle; and Sirius (Costruzione Strumenti Oftalmici, Florence, Italy), which combines the Scheimpflug principle with the Placido disc imaging and Galilei (Ziemer, Biel, Switzerland), based on dual Scheimpflug and Placido disc imaging. All patients underwent the measurements in the same order with a break of 15 min between each topographer to avoid fatigue and lapse in concentration. Densitometry, a measure of corneal haze, was obtained from the Pentacam software, for concentric four zones: 0–2 mm, 2–6 mm, 6–10 mm, and 10–12 mm and anterior (up to 120 µ), posterior (posterior 60 µ), and central (between the anterior and posterior) zones as illustrated in Figs. 1 and 2].
Figure 1.
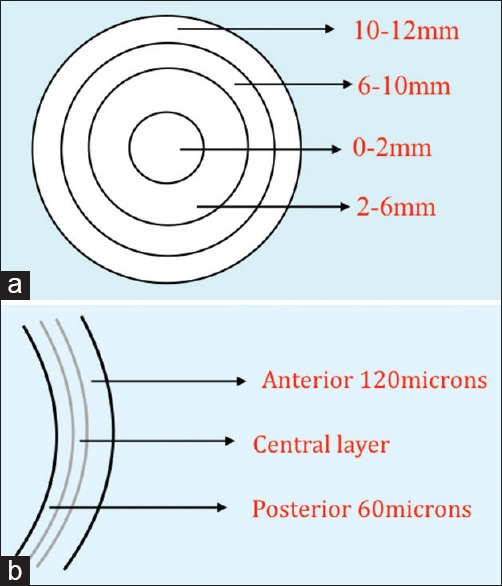
(a) Cornea divided into four zones from center to periphery. (b) Cornea divided into 3 zones from anterior to posterior
Figure 2.

Measurement of haze using the corneal densitometry software on Pentacam
A standard methodology was used to obtain measurements on each device. A central fixation light of the machine was used to align the eye to the visual axis. Patients were asked to blink completely to allow the tear film to be evenly distributed before each scan. Three good quality scans were obtained for each patient by the same examiner, and the TCT values and Km of each scan were used to assess for repeatability. Densitometric value of each zone was analyzed for its effect on the repeatability of TCT and Km.
Our definitions of repeatability were based on those adopted by the British Standards Institution and the International Standards Organization.[24,25] Independent test results were obtained using the same method, on the same subject, with the same operator, and on the same equipment with the shortest time possible between successive sets of readings to assess repeatability.[26]
Statistical analyses
Descriptive statistics included mean and standard deviation for normally distributed variables and median, First quartile, and third quartile values for nonnormally distributed variables. The effect of haze on the average of three parameter measurements was evaluated using mixed models. Three measurements of haze and three measurements of TCT and Km per eye were used for this analysis. Repeatability was assessed by coefficient of variation (CV). The CV was calculated as within-subject standard deviation/overall mean. The average measurement of haze was computed and regression models used to evaluate the effect of haze on the CV of TCT and Km measurements with the different devices. Statistical analyses were performed using Stata version 12.1 (StataCorp, College Station, TX, USA) statistical software. P ≤ 0.05 was considered statistically significant.
Results
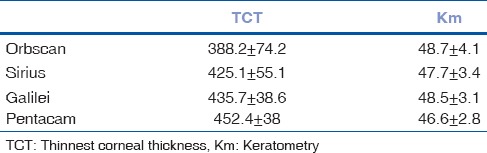
Sixty eyes of sixty patients who had undergone ACXL a year back were enrolled in the study. Among them, 27 were female patients and 33 were male patients with a mean age of 23 ± 5 years (range 15–36). There were 36 right eyes and 24 left eyes. Post-ACXL haze was measured as densitometry on the Pentacam HR in different zones of the cornea. In the anterior 0–2 mm zone, the mean densitometry measurement was 27.8 ± 7.6 GSU; in the anterior 2–6 mm zone, it was 22.3 ± 4.4 GSU; in the central 0–2 mm zone, it was 15.9 ± 3.2 GSU; and in the central 2–6 mm zone, it was found 13.2 ± 1.5 GSU. Measurements were higher in the 0–2 mm zone compared to the 2–6 mm zone and higher in the anterior zone when compared to the central zone of the cornea as shown in Table 1. The mean readings of TCT and mean keratometric values with their standard deviation using the four devices are shown in Table 2.
Table 1.
Mean densitometry values with standard deviation in different zones
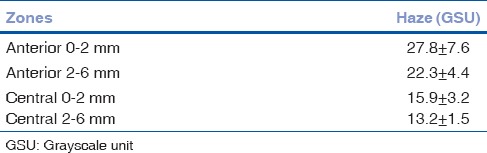
Table 2.
Mean values with standard deviation of different parameters measured with the four devices
CV of the TCT and Km measurements of the four devices is shown in Table 3. Orbscan II showed the highest variability for TCT measurements. Galilei showed the least variability compared to all other devices for TCT. The variability of Km parameters with Sirius was lower than that with the other devices. Table 4 shows the effect of haze in various zones in the cornea on parameter measurement and the repeatability of TCT for each of the four devices. TCT measurement with Orbscan was significantly affected by haze. Measurement of TCT with the other three Scheimpflug devices was independent of haze.
Table 3.
Within-subject coefficient of variation estimates (with 95% confidence intervals in brackets) of different parameter measurements with the four devices
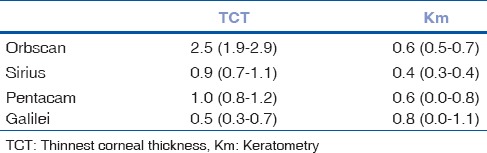
Table 4.
Effect of haze in the different zones of the cornea with 95% confidence interval in the brackets on parameter measurement and repeatability of thinnest corneal thickness measurement with the four devices
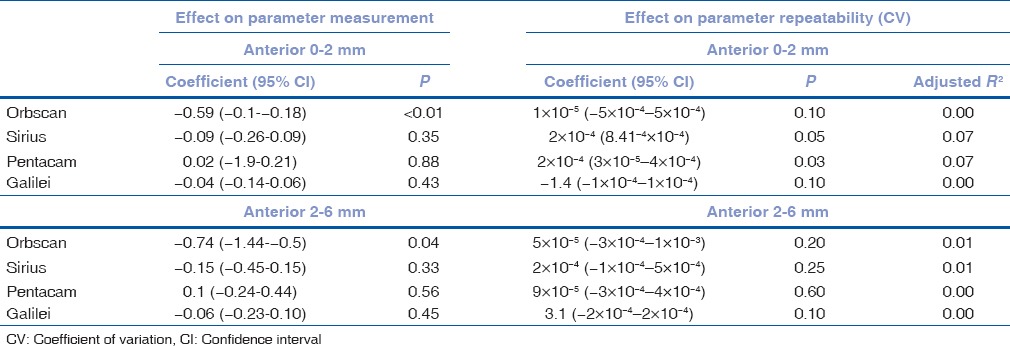
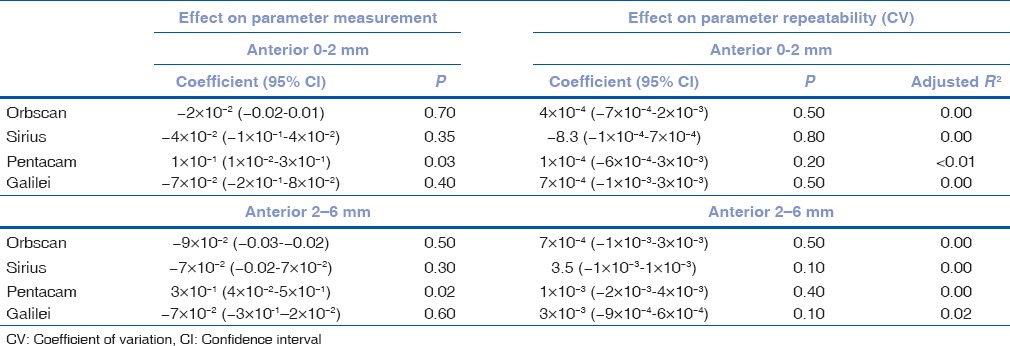
The repeatability of TCT measurements with Sirius and Pentacam was significantly affected by haze in the anterior 0–2 mm zone (P = 0.05 and 0.03), respectively. The repeatability of TCT measurements with Orbscan and Galilei was not affected by haze. Table 5 shows the effect of haze in various zones in the cornea on the measurement and repeatability of Km for each of the four devices. The Km measurement with Pentacam was significantly affected by haze (P = 0.03) while it was independent of haze for the other three devices. Haze did not affect the repeatability of Km measurements taken with any of the four devices.
Table 5.
Effect of haze in the different zones of the cornea with 95% confidence interval in the brackets on parameter measurement and repeatability of keratometry measurement with the four devices
Discussion
Keratoconus has traditionally been classified and graded based on ultrasound pachymetry and Placido disc-based imaging.[27] Ultrasound pachymetry, the gold standard for measuring corneal thickness, takes the measurement at a single point, which might not necessarily be the thinnest location.[28] It has been shown that in patients with keratoconus, Scheimpflug provides more reproducible and repeatable measurements of central thickness than those obtained with ultrasound pachymetry.[29] Topographers providing full corneal pachymetry maps are advantageous in localizing the thinnest corneal location and also for the early diagnosis of ectatic conditions. Likewise, keratometric measurements have come a long way from corneal casts, Placido disc reflection, and manual Km to automated topographers that use various imaging principles such as the Placido disc imaging, scanning slit technology, Scheimpflug photography, dual Scheimpflug imaging, and a combination of these.
Various studies have established the safety and precision of these devices for the measurement of corneal topography.[30,31] The repeatability or test–retest reliability is the variability in these measurements taken by a single person or instrument, under the same conditions within a short period, over which the underlying value can be considered to be constant. While a high repeatability of any instrument's measurement is an indication of its precision, measurements with a low repeatability should be interpreted with caution. There are several parameters that can affect repeatability, one of them being corneal clarity. Corneal haze affects the transmission of light through the cornea, resulting in backward scattering of light and can therefore influence the measurements of topographers. It is hence imperative to assess the reliability of these measurements in conditions where the corneal clarity is compromised.
Corneal haze can be a result of infections, corneal dystrophies and degenerations, and postsurgical intervention. Clinically, this can be detected and graded using a standard slit-lamp examination, albeit subjectively.[2] Quantification as densitometry on the Pentacam provides an objective and reproducible method of measuring corneal haze. The maximum effect of CXL on corneal clarity is known to occur in the anterior 300 µ of the stroma as evidenced on confocal microscopy.[3,32] In our study, haze was seen maximally in the central 0–2 mm, followed by 2–6 mm and the anterior stromal layers when compared to the rest of the cornea. This has significant implications as keratometric readings are derived from the central 3 mm area of the cornea and TCT takes into account the entire cornea including the anterior, central, and posterior zones. Therefore, both TCT and Km measurements can be affected by post-CXL haze.
The poor repeatability of Orbscan in corneas with haze has been attributed to change in the light slits traveling through the cornea and the influence of the backscatter of light. These result in variations in posterior surface data and altered pachymetric analysis.[33,34] Although an acoustic factor correction has been proposed to overcome these limitations, it has been shown that this correction works only in transparent prolate corneas and not helpful in irregular or oblate (corneal ectasia) or nontransparent corneas (haze).[35,36] Likewise, we found that the measurement of TCT with Orbscan II was affected, especially in areas where haze was significant. This suggests that in the presence of post-CXL haze, monitoring progression of keratoconus using only the Orbscan II may not be reliable. We found that the measurement of TCT with Pentacam, Sirius, and Galilei was unaffected by haze though the repeatability of Pentacam and Sirius was poor in areas where the haze was significant (central and anterior 0–2 mm). This is in contrast to previous studies, which have shown good repeatability of Scheimpflug devices in normal and keratoconic corneas.[37,38] There could be factors other than haze causing poor repeatability of the corneal measurements as shown by Hashemi et al. in their study comparing 5 devices for corneal measurements in keratoconic patients. They reported as the severity of keratoconus increases the repeatability of all devices to measure corneal parameters reduces due to measurements' errors.[39]
The measurement of Km only on the Pentacam was affected by haze when compared to other topographers. Haze in the anterior stroma up to 6 mm particularly in the central 2 mm zone had the maximum influence. It is possible that the Km readings of Orbscan, Sirius, and Galilei were unaffected by the haze due to the Placido disc component of these devices providing more accuracy while evaluating the anterior surface curvature (Km). This is in contrast to the Pentacam, which has only a single Scheimpflug imaging system. However, unlike TCT, the repeatability of Km measurement with all four topographers was unaffected by haze.
One of the limitations of the study is that the repeatability of only commonly used keratoconus indices was studied like the mean Km and TCT. Since a single operator recorded all the measurements, there is a small possibility of an observer bias. Another limitation is the lack of a control group.
In this study, we found that when evaluating patients with post-CXL haze, Galilei appears to be more reliable when assessing pachymetry and the anterior corneal surface. The pachymetry measurements of Orbscan II and the corneal curvature measurements of Pentacam were significantly affected by haze. In addition, the repeatability of pachymetry measurements of Pentacam and Sirius was significantly affected by haze. Haze did not affect the repeatability of Km measurements of any of the devices. It is important to note that the magnitude of effect of haze on either the parameter measurements or the repeatability estimates, though found statistically significant, was small in the presence of minimal haze. However, in cases with dense haze, the effect can be clinically significant and clinicians should keep this in mind while considering management decisions based on these measurements.
Conclusion
In corneas that have undergone crosslinking, response to treatment and progression of the disease must be gauged with caution, as there is increased variability in the measurement owing to corneal haze. Devices cannot be used interchangeably for measurements in postcrosslinked eyes.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135:620–7. doi: 10.1016/s0002-9394(02)02220-1. [DOI] [PubMed] [Google Scholar]
- 2.Greenstein SA, Fry KL, Bhatt J, Hersh PS. Natural history of corneal haze after collagen crosslinking for keratoconus and corneal ectasia: Scheimpflug and biomicroscopic analysis. J Cataract Refract Surg. 2010;36:2105–14. doi: 10.1016/j.jcrs.2010.06.067. [DOI] [PubMed] [Google Scholar]
- 3.Mazzotta C, Balestrazzi A, Baiocchi S, Traversi C, Caporossi A. Stromal haze after combined riboflavin-UVA corneal collagen cross-linking in keratoconus: In vivo confocal microscopic evaluation. Clin Exp Ophthalmol. 2007;35:580–2. doi: 10.1111/j.1442-9071.2007.01536.x. [DOI] [PubMed] [Google Scholar]
- 4.Chan-Ling T, Efron N, Holden BA. Diurnal variation of corneal thickness in the cat. Invest Ophthalmol Vis Sci. 1985;26:102–5. [PubMed] [Google Scholar]
- 5.Doughty MJ, Zaman ML. Human corneal thickness and its impact on intraocular pressure measures: A review and meta-analysis approach. Surv Ophthalmol. 2000;44:367–408. doi: 10.1016/s0039-6257(00)00110-7. [DOI] [PubMed] [Google Scholar]
- 6.Randleman JB, Russell B, Ward MA, Thompson KP, Stulting RD. Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology. 2003;110:267–75. doi: 10.1016/S0161-6420(02)01727-X. [DOI] [PubMed] [Google Scholar]
- 7.Shetty R, D'Souza S, Srivastava S, Ashwini R. Topography-guided custom ablation treatment for treatment of keratoconus. Indian J Ophthalmol. 2013;61:445–50. doi: 10.4103/0301-4738.116067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Belin MW, Ambrósio R. Scheimpflug imaging for keratoconus and ectatic disease. Indian J Ophthalmol. 2013;61:401–6. doi: 10.4103/0301-4738.116059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shetty R, Pahuja NK, Nuijts RM, Ajani A, Jayadev C, Sharma C, et al. Current protocols of corneal collagen cross-linking: Visual, refractive, and tomographic outcomes. Am J Ophthalmol. 2015;160:243–9. doi: 10.1016/j.ajo.2015.05.019. [DOI] [PubMed] [Google Scholar]
- 10.Mazzotta C, Traversi C, Baiocchi S, Caporossi O, Bovone C, Sparano MC, et al. Corneal healing after riboflavin ultraviolet-A collagen cross-linking determined by confocal laser scanning microscopy in vivo: Early and late modifications. Am J Ophthalmol. 2008;146:527–33. doi: 10.1016/j.ajo.2008.05.042. [DOI] [PubMed] [Google Scholar]
- 11.Touboul D, Efron N, Smadja D, Praud D, Malet F, Colin J. Corneal confocal microscopy following conventional, transepithelial, and accelerated corneal collagen cross-linking procedures for keratoconus. J Refract Surg. 2012;28:769–76. doi: 10.3928/1081597X-20121016-01. [DOI] [PubMed] [Google Scholar]
- 12.Savini G, Carbonelli M, Sbreglia A, Barboni P, Deluigi G, Hoffer KJ. Comparison of anterior segment measurements by 3 Scheimpflug tomographers and 1 Placido corneal topographer. J Cataract Refract Surg. 2011;37:1679–85. doi: 10.1016/j.jcrs.2011.03.055. [DOI] [PubMed] [Google Scholar]
- 13.Montalbán R, Piñero DP, Javaloy J, Alió JL. Intrasubject repeatability of corneal morphology measurements obtained with a new Scheimpflug photography-based system. J Cataract Refract Surg. 2012;38:971–7. doi: 10.1016/j.jcrs.2011.12.029. [DOI] [PubMed] [Google Scholar]
- 14.Fares U, Otri AM, Al-Aqaba MA, Faraj L, Dua HS. Wavefront-optimized excimer laser in situ keratomileusis for myopia and myopic astigmatism: Refractive outcomes and corneal densitometry. J Cataract Refract Surg. 2012;38:2131–8. doi: 10.1016/j.jcrs.2012.07.041. [DOI] [PubMed] [Google Scholar]
- 15.Cennamo G, Forte R, Aufiero B, La Rana A. Computerized Scheimpflug densitometry as a measure of corneal optical density after excimer laser refractive surgery in myopic eyes. J Cataract Refract Surg. 2011;37:1502–6. doi: 10.1016/j.jcrs.2011.03.037. [DOI] [PubMed] [Google Scholar]
- 16.Arnalich-Montiel F, Hernández-Verdejo JL, Oblanca N, Muñoz-Negrete FJ, De Miguel MP. Comparison of corneal haze and visual outcome in primary DSAEK versus DSAEK following failed DMEK. Graefes Arch Clin Exp Ophthalmol. 2013;251:2575–84. doi: 10.1007/s00417-013-2460-y. [DOI] [PubMed] [Google Scholar]
- 17.Otri AM, Fares U, Al-Aqaba MA, Dua HS. Corneal densitometry as an indicator of corneal health. Ophthalmology. 2012;119:501–8. doi: 10.1016/j.ophtha.2011.08.024. [DOI] [PubMed] [Google Scholar]
- 18.Kam KW, Belin MW, Young AL. Monitoring corneal densities following primary pterygium excision with adjuvant topical mitomycin-C application – An observational study of corneal scar changes. Cornea. 2015;34:530–4. doi: 10.1097/ICO.0000000000000400. [DOI] [PubMed] [Google Scholar]
- 19.Malhotra C, Jain AK, Dwivedi S, Chakma P, Rohilla V, Sachdeva K. Characteristics of pre-descemet membrane corneal dystrophy by three different imaging modalities-in vivo confocal microscopy, anterior segment optical coherence tomography, and scheimpflug corneal densitometry analysis. Cornea. 2015;34:829–32. doi: 10.1097/ICO.0000000000000454. [DOI] [PubMed] [Google Scholar]
- 20.Pircher N, Pachala M, Prager F, Pieh S, Schmidinger G. Changes in straylight and densitometry values after corneal collagen crosslinking. J Cataract Refract Surg. 2015;41:1038–43. doi: 10.1016/j.jcrs.2014.07.043. [DOI] [PubMed] [Google Scholar]
- 21.Lopes B, Ramos I, Ambrósio R., Jr Corneal densitometry in keratoconus. Cornea. 2014;33:1282–6. doi: 10.1097/ICO.0000000000000266. [DOI] [PubMed] [Google Scholar]
- 22.Anayol MA, Sekeroglu MA, Ceran BB, Dogan M, Gunaydin S, Yilmazbas P. Quantitative assessment of corneal clarity in keratoconus: A case control study of corneal densitometry. Eur J Ophthalmol. 2016;26:18–23. doi: 10.5301/ejo.5000644. [DOI] [PubMed] [Google Scholar]
- 23.Carr JD, Patel R, Hersh PS. Management of late corneal haze following photorefractive keratectomy. J Refract Surg. 1995;11(3 Suppl):S309–13. doi: 10.3928/1081-597X-19950502-25. [DOI] [PubMed] [Google Scholar]
- 24.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–10. [PubMed] [Google Scholar]
- 25.Muscat S, McKay N, Parks S, Kemp E, Keating D. Repeatability and reproducibility of corneal thickness measurements by optical coherence tomography. Invest Ophthalmol Vis Sci. 2002;43:1791–5. [PubMed] [Google Scholar]
- 26.Maldonado MJ, Nieto JC, Díez-Cuenca M, Piñero DP. Repeatability and reproducibility of posterior corneal curvature measurements by combined scanning-slit and Placido-disc topography after LASIK. Ophthalmology. 2006;113:1918–26. doi: 10.1016/j.ophtha.2006.05.053. [DOI] [PubMed] [Google Scholar]
- 27.Alió JL, Shabayek MH. Corneal higher order aberrations: A method to grade keratoconus. J Refract Surg. 2006;22:539–45. doi: 10.3928/1081-597X-20060601-05. [DOI] [PubMed] [Google Scholar]
- 28.Belin MW, Khachikian SS. New devices and clinical implications for measuring corneal thickness. Clin Exp Ophthalmol. 2006;34:729–31. doi: 10.1111/j.1442-9071.2006.01395.x. [DOI] [PubMed] [Google Scholar]
- 29.de Sanctis U, Missolungi A, Mutani B, Richiardi L, Grignolo FM. Reproducibility and repeatability of central corneal thickness measurement in keratoconus using the rotating Scheimpflug camera and ultrasound pachymetry. Am J Ophthalmol. 2007;144:712–8. doi: 10.1016/j.ajo.2007.07.021. [DOI] [PubMed] [Google Scholar]
- 30.Li Y, Shekhar R, Huang D. Corneal pachymetry mapping with high-speed optical coherence tomography. Ophthalmology. 2006;113:792–9.e2. doi: 10.1016/j.ophtha.2006.01.048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.González-Pérez J, González-Méijome JM, Rodríguez Ares MT, Parafita MA. Central corneal thickness measured with three optical devices and ultrasound pachometry. Eye Contact Lens. 2011;37:66–70. doi: 10.1097/ICL.0b013e31820c6ffc. [DOI] [PubMed] [Google Scholar]
- 32.Wollensak G, Iomdina E, Dittert DD, Herbst H. Wound healing in the rabbit cornea after corneal collagen cross-linking with riboflavin and UVA. Cornea. 2007;26:600–5. doi: 10.1097/ICO.0b013e318041f073. [DOI] [PubMed] [Google Scholar]
- 33.Boscia F, La Tegola MG, Alessio G, Sborgia C. Accuracy of Orbscan optical pachymetry in corneas with haze. J Cataract Refract Surg. 2002;28:253–8. doi: 10.1016/s0886-3350(01)01162-2. [DOI] [PubMed] [Google Scholar]
- 34.Wang Z, Chen J, Yang B. Posterior corneal surface topographic changes after laser in situ keratomileusis are related to residual corneal bed thickness. Ophthalmology. 1999;106:406–9. doi: 10.1016/S0161-6420(99)90083-0. [DOI] [PubMed] [Google Scholar]
- 35.Cheng AC, Tang E, Mohamed S, Lam DS. Correction factor in Orbscan II in the assessment of corneal pachymetry. Cornea. 2006;25:1158–61. doi: 10.1097/01.ico.0000240089.26467.dc. [DOI] [PubMed] [Google Scholar]
- 36.Chakrabarti HS, Craig JP, Brahma A, Malik TY, McGhee CN. Comparison of corneal thickness measurements using ultrasound and Orbscan slit-scanning topography in normal and post-LASIK eyes. J Cataract Refract Surg. 2001;27:1823–8. doi: 10.1016/s0886-3350(01)01089-6. [DOI] [PubMed] [Google Scholar]
- 37.Finis D, Ralla B, Karbe M, Borrelli M, Schrader S, Geerling G. Comparison of two different scheimpflug devices in the detection of keratoconus, regular astigmatism, and healthy corneas. J Ophthalmol. 2015;2015:315281. doi: 10.1155/2015/315281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Shetty R, Arora V, Jayadev C, Nuijts RM, Kumar M, Puttaiah NK, et al. Repeatability and agreement of three Scheimpflug-based imaging systems for measuring anterior segment parameters in keratoconus. Invest Ophthalmol Vis Sci. 2014;55:5263–8. doi: 10.1167/iovs.14-15055. [DOI] [PubMed] [Google Scholar]
- 39.Hashemi H, Yekta A, Khabazkhoob M. Effect of keratoconus grades on repeatability of keratometry readings: Comparison of 5 devices. J Cataract Refract Surg. 2015;41:1065–72. doi: 10.1016/j.jcrs.2014.08.043. [DOI] [PubMed] [Google Scholar]