

Abstract
Background:
Breast cancer is the most frequently diagnosed malignancy and the leading cause of cancer death among women worldwide. In Morocco, there have been few recent descriptive studies on female breast cancer. The aim of this study was to describe the latest available incidence and mortality rates of breast cancer among Moroccan women and to compare them with rates in other regional and Western countries.
Methods:
For this descriptive study, Moroccan incidence data were obtained from the most recent reports of the cancer registries of Casablanca and Rabat. Information on breast cancer incidence for different countries were obtained primarily from publicly available cancer registries and Cancer Incidence in Five Continents, Volume X. Mortality data were extracted from the GLOBOCAN 2012 published by the International Agency for Research on Cancer.
Results:
The age-standardized incidence (World) rate of breast cancer in Moroccan women increased from 35.0 to 39.0 per 100,000 women between 2004 and 2008, showing an annual increase of 2.85 %. The highest incidence rates were registered in the age groups of 45-49, 50-54 and 55-59 years (106.1, 108.2 and 108.5 respectively). Sixty-nine percent of female breast cancer cases were diagnosed at stages II and III. In 2012, the estimated number of women who died of breast cancer in Morocco was 2,878. The crude, age-standardized (World) mortality rates were 17.3 and 18.0 per 100,000, respectively.
Conclusion:
Although the incidence of female breast cancer in Morocco is lower than in Western countries, evidence shows that the rate is rising. This increase of breast cancer incidence has been observed in parallel with changes in reproductive behavior and adoption of a Western lifestyle. Prevention policies need to be implemented.
Keywords: Breast cancer, incidence, mortality, Morocco
Introduction
Breast cancer is the most frequently diagnosed cancer and the leading cause of cancer death among women worldwide, with an estimated 1.7 million cases and 521 900 deaths in 2012. Breast cancer alone accounts for 25% of all cancer cases and 15% of all cancer deaths among females (Torre et al., 2015). Less developed countries account for about 55.6% of all breast cancer cases and 62.1% of deaths (Ferlay et al., 2013). Breast cancer incidence rates vary considerably across geographic regions (Ghoncheh et al., 2016). Overall, the rates are high in Northern America, Australia, New Zealand, and Northern and Western Europe; and lowest in most of Africa and Asia (Torre et al., 2015).
Although, the incidence of breast cancer in the North Africa region is lower than that in Western countries (approximately 1.5–2 times lower among females aged less than 50, and 3–4 times lower among females aged more than 50), the breast cancer picture in Northern Africa is changing (Corbex et al., 2014).
Morocco is a country with a population estimated at 33.8 million people in 2014, and a life expectancy at birth of 74.8 years in 2010 (High Commission for Planning, Morocco, 2016). According to the United Nations human development index (HDI), Morocco’s HDI value for 2014 was 0.62, which places the country in the medium human development category (The United Nations Development program, 2015).
Morocco is a country in epidemiological transition, marked by a double burden due to the coexistence of infection and chronic diseases (Nejmi and Boutayeb, 2016), and the breast cancer is increasingly becoming an important public health concern (Slaoui et al., 2014). The incidence rate of this disease has risen in the past years, likely due to changes in the pattern of breast cancer risk factors caused by adoption of a Western lifestyle.
It is noteworthy that there are few recent descriptive studies on the incidence and mortality of breast cancer among Moroccan women. The aim of this study was to describe the latest available incidence and mortality rates of breast cancer among Moroccan women and to compare them to the rates of regional and Western countries.
Materials and Methods
This descriptive study was carried out based on existing incidence and mortality data.
Moroccan incidence data
In Morocco, two population-based registries are the principal sources of reliable cancer morbidity data: The first one, the population-based cancer registry of Casablanca, covering around 12 % of the Moroccan population. It provides incidence of all types of cancer from 2004 onwards among the population of the Greater Casablanca. The second one, the population-based cancer registry of Rabat, covering around 2.1 % of the Moroccan population, it reports all new cancer cases from 2005 onwards among residents in Rabat.
We obtained breast cancer incidence data from the most recent reports of these two cancer registries, corresponding to the periods: 2004 (Cancer Registry of Casablanca, 2004), 2005–2007 (Cancer Registry of Casablanca, 2005-2007) for the cancer registry of Casablanca and 2005 (Cancer Registry of Rabat, 2005), 2006–2008 (Cancer Registry of Rabat, 2006-2008) for the cancer registry of Rabat.
International incidence data
Information on breast cancer incidence for different countries was obtained primarily from publicly available cancer registries and the Cancer Incidence in Five Continents, Volume X (Forman et al., 2014).
Mortality data
In Morocco, there are no official published data about breast cancer mortality. In this study, breast cancer mortality estimates for the year 2012, were extracted from the GLOBOCAN 2012 published by the International Agency for Research on Cancer (IARC) (Ferlay et al., 2013).
Results
Breast cancer was the first leading cancer incidence in Moroccan women, accounting for 34.4% of all new cancer cases in females (Figure 1, Figure 2). Overall, the age-standardized incidence (World) rate of breast cancer increased from 35.0 to 39.0 per 100,000 women between 2004 and 2008, showing an annual increase of 2.85 % (Table 1). The age-standardized incidence (World) of breast cancer in Morocco was higher than that in neighboring countries (Figure 3)
Figure 1.
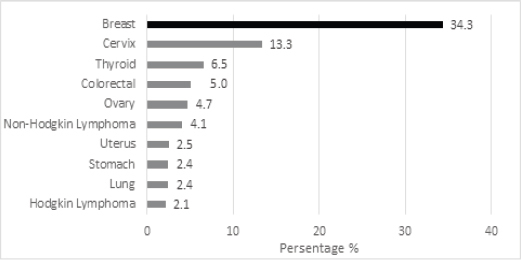
Ten Most Common Cancers among Moroccan Women, According to the Cancer Registry of Casablanca 2005-2007
Figure 2.
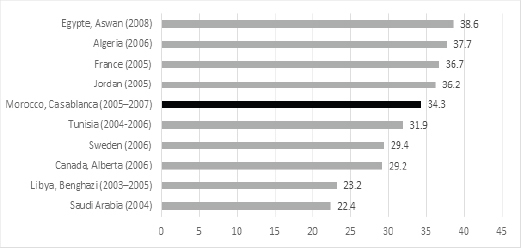
Breast Cancer as Proportion of All Reported Cancers in Females in Morocco Compared to Other Countries.
Table 1.
Numbers, Crude and Age-Standardized Incidence Rates of Female Breast Cancer in Morocco, 2004–2008
| 2004 | 2005 | 2006 | 2007 | 2008 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Casablanca | Rabat | Casablanca | Rabat | Casablanca | Rabat | Casablanca | Rabat | Casablanca | Rabat | |
| Cases | 662.0 | - | 666.0 | 127.0 | 690.0 | 158.0 | 763.0 | 182.0 | - | 151.0 |
| Crude rate | 36.1 | - | 35.9 | 38.8 | 36.3 | 47.9 | 39.9 | 54.7 | - | 45.1 |
| ASR (M) | - | - | 30.4 | 30.6 | 31.5 | 37.8 | 34.6 | 43.2 | - | 35.2 |
| ASR (W) | 35.0 | - | 35.1 | 35.8 | 35.4 | 43.1 | 38.6 | 48.1 | - | 39.0 |
CR, Crude rate per 100,000; ASR (M), Age standardized rate (Morocco population) per 100,000; ASR (W), Age standardized incidence rate (World population) per 100,000; Data from, The cancer registries of Casablanca and Rabat
Figure 3.
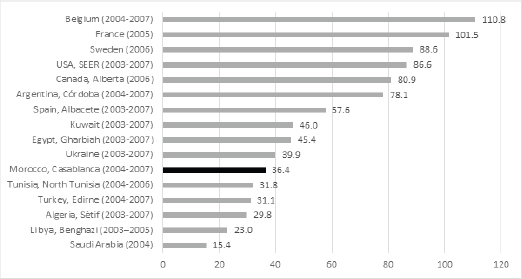
Age-Standardized Incidence (World Population) Rate for Female Breast Cancer in Morocco Compared to Other Countries.
Data from: (Cancer Registry of Saudi Arabia, 2004; El Mistiri et al., 2015; Cancer Registry of Canada- Alberta, 2006; Cancer Incidence in Sweden, 2006; Cancer Registry of Tunisia, 2004-2006; Cancer Registry of Casablanca, 2005–2007; Cancer Incidence in Jordan 2005; Bélot et al., 2008; Cancer Registry of Algeria; 2006; Cancer Registry of Egypt- Aswan, 2008)
Data from: (Forman et al., 2014; Cancer Registry of Saudi Arabia, 2004; El Mistiri et al., 2015; Cancer Registry of Tunisia, 2004-2006; Cancer Registry of Casablanca, 2004, 2005–2007; Cancer Registry of Canada- Alberta, 2006; Cancer Incidence in Sweden, 2006; Bélot et al., 2008).
Between 2005 and 2007, the highest incidence rates were registered in the age groups of 45–49, 50–54 and 55–59 years (106.1, 108.2 and 108.5 respectively). Thereafter, the incidence rates decline to 86.5, 85.9, and 53.2 for the age groups of 65–69, 70–74 and 75+ years respectively (Table 2, Figure 4).
Table 2.
Age-Specific Incidence Rate for Breast Cancer in Moroccan Women (2005-2007) According to the Cancer Registry of Casablanca
| Age range | Incidence rates |
|---|---|
| 20-24 | 0.5 |
| 25-29 | 6.8 |
| 30-34 | 18.1 |
| 35-39 | 52.8 |
| 40-44 | 96.8 |
| 45-49 | 106.1 |
| 50-54 | 108.2 |
| 55-59 | 108.5 |
| 60-64 | 103.2 |
| 65-69 | 86.5 |
| 70-74 | 85.9 |
| 75+ | 53.2 |
Figure 4.
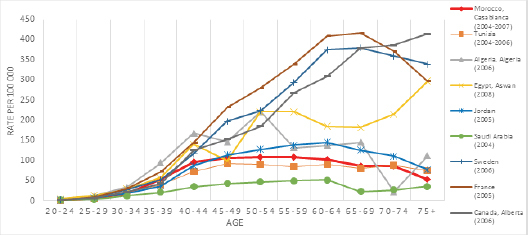
Age-Specific Incidence Rate for Female Breast Cancer in Morocco (Cancer Registry of Casablanca 2005-2007) Compared to Other Countries.
For distribution of female breast cancer by stage and according to the Rabat cancer registry (2006-2008), 13.5% of female breast cancer were diagnosed at stages I, 44.6% at stages II, 24.4% at stages III and 4.5% at stages IV (13.0% not defined).
In 2012, the estimated number of women who died of breast cancer in Morocco was 2878. The crude, age-standardized (World) mortalities were 17.3 and 18.0 per 100,000, respectively (Table 3).
Table 3.
Breast Cancer Mortality Per 100,000 Estimated by Globocan 2012
| Country | Cases | Crude Rate | ASR (W) |
|---|---|---|---|
| Morocco | 2,878 | 17.3 | 18.0 |
| Algeria | 2,839 | 15.7 | 17.5 |
| Tunisia | 624 | 11.6 | 10.8 |
| Libya | 223 | 6.9 | 8.4 |
| Egypt | 7,161 | 17.1 | 19.2 |
| Jordan | 426 | 13.6 | 21.8 |
| Kuwait | 103 | 8.8 | 17.3 |
| Lebanon | 599 | 27.3 | 24 |
| Saudi Arabia | 795 | 6.2 | 9.1 |
| China | 47,984 | 7.3 | 5.4 |
| Spain | 6,075 | 25.7 | 11.8 |
| Belgium | 2,523 | 45.9 | 20.3 |
| France | 11,933 | 36.7 | 16.4 |
| Sweden | 1,450 | 30.5 | 13.4 |
| Canada | 4,924 | 28.2 | 13.9 |
| United States of America | 43,909 | 27.5 | 14.9 |
Data from: Ferlay et al., 2013
Discussion
This study provides incidence and mortality rates of breast cancer among Moroccan women, based on the latest available data.
Breast cancer was the leading tumor in Moroccan women accounting for 34.3% of all female cancers registered between the years 2005 and 2007. This proportion was approximately similar to that in Tunisia, and was higher than those in Libya and Saudi Arabia (Figure 2).
The age-standardized incidence (World) of breast cancer in Morocco (36.4) was higher than that in neighboring countries such as Algeria (29.8), Tunisia (31.8) and Libya (23.0), but was lower than those of some western countries such as France (101.5), USA (86.6) and Canada (80.9) (Fig. 3). This disparity in incidence rates may be due to differences in the distribution of the prevalence of risk factors associated with breast cancer, as well as the availability of early detection in these countries.
Between 2004 and 2008, the incidence of breast cancer in Morocco increased by 2.8% per year. It was close to that reported by central Tunisia registry (2.2% per year) for the period 1993–2006. But such an increase is higher than the one observed in France (1.2% per year) in the period of 1990–1999 before screening was implemented (Corbex et al., 2014).
Several studies suggest that the increasing incidence trend in low- and middle income countries is largely due to increases in risk factors associated with economic development and urbanization, including obesity, adaptation of a Western-type diet, physical inactivity, delayed childbearing and/or having fewer children, earlier age at menarche, and shorter duration of breastfeeding (Boyle and Howell, 2010; DeSantis et al., 2015; Porter, 2008).
During the past several decades, Morocco, like most developing countries, has witnessed sociodemographic changes, cultural and economic transformation. This transformation has also brought many lifestyle changes, such as an increase in the age of marriage and first pregnancy, a decrease in the duration of breastfeeding and fertility, an increase in the prevalence of overweight and obesity, an increase in the prevalence of oral contraceptive use and changes in dietary habits. For example, the mean age at marriage of Moroccan women increased from 18.5 years in 1987 (Ministry of health, Morocco, 1989) to 26.3 years in 2011 (Ministry of health, Morocco, 2011), the total fertility rate (number of children per woman) decreased from 5.9 births per woman in 1980 (Ministry of health, Morocco, 1989) to 2.6 births per woman in 2011 (Ministry of health, Morocco, 2011), the average duration of breastfeeding decreased from 17.5 months in 1980 (Ministry of health, Morocco, 1989) to 16.3 months in 2011 (Ministry of health, Morocco, 2011), the prevalence of overweight among Moroccan women increased from 29.0% in 1999 to 47.8% in 2000 (Toselli et al., 2014) and the prevalence of oral contraceptive use increased from 22.9% in 1987 (Ministry of health, Morocco, 1989) to 48.4% in 2011 (Ministry of health, Morocco, 2011).
Few epidemiological studies have explored risk factors for breast cancer in Moroccan women. A case–control study developed in the region of Rabat reported that early menarche, late menopause, oral contraceptive and family history of breast cancer were likely associated with breast cancer risks (Laamiri et al., 2015). Another study conducted in the region of Oujda found an inverse relationship between breastfeeding and breast cancer (Maamri et al., 2012). Further studies are required to explore the risk factors of breast cancer among Moroccan women.
Other possible contributing factors to the observed change in breast cancer incidence in Morocco are improved access and availability of healthcare facilities as well as increased awareness regarding breast cancer.
An organized screening, which usually results in a temporary increase in incidence rates, is not implicated in the increase of breast cancer incidence in Morocco between 2004 and 2008. It started after this period (2010). However, the absence of organized screening program in this period may explain partly the incidence difference between Morocco and other countries. According to a World Health Organization study conducted on Moroccan population in 2003, only 2.1% of women aged 40 years or older had a clinical breast examination (or screening mammogram) in their life (Ministry of health, Morocco, 2007).
Regarding the age specific incidence pattern, the lowest rates of incidence of female breast cancer were seen in the age group 20-29 years and the highest in the age group 50-60 years. This situation was similar in Egypt but it was different from that in some Western countries such as France and Canada (the highest incidence rates of female breast cancer were registered in women above 60 years) (Fig. 4). The difference observed in age specific incidence between Moroccan and Western women may be partly related to the age distribution of populations in those countries. In addition, comparisons between women in high-income countries and middle-income countries should be carefully age-matched (Harford, 2011). Other studies suggest that the variation in genetic marker distribution between North African and Western populations may be involved (Boder et al., 2011).
Overall, like Arab populations (Chouchane et al., 2013; Najjar and Easson, 2010), the average age at presentation of breast cancer in Moroccan women is earlier than in Western countries. Retrospective studies focused on breast cancer in young Moroccan women, reported that 8.0% (Abahssain et al., 2010), 18.6 (Znati et al., 2014), 25.4 % (Boufettal et al., 2010) of the cases were aged 35 years or younger.
There is evidence suggesting that cancer stage is considered the most important factor in determining the prognosis of most cancers (Jazayeri et al., 2015), and women with early-stage breast cancers are expected to have excellent survival rates (Iqbal et al., 2015). Unfortunately a very high proportion of cases in developing countries including Morocco are detected in late stages (Amadou et al., 2014; Kim et al., 2015; Mathew et al., 2016; Schlichting et al., 2015). This is in contrast to that in Western countries, for example in the United States about 80 % of breast cancer cases are diagnosed at an early stage (Mobley and Kuo, 2015). Several reasons are given for the advanced stage at presentation in developing countries, such as the stigma of breast cancer and the societal implications associated with its treatments especially for mastectomy, availability and quality of primary health care services and the lack of access to mammography (Iqbal et al., 2015; Shulman et al., 2010).
Regarding mortality data, in 2012, the breast cancer mortality rate for Moroccan women (18.0 per 100,000) was similar to that in some countries with a middle income, e.g. Algeria (17.5 per 100,000), Egypt (19.2 per 100,000), and Jordan (21.8 per 100,000), but was higher than the world average which was 12.9 per 100,000. Early breast cancer detection, breast cancer diagnosis and management, as well as improved treatments may explain some of the international differences in breast cancer mortality. Furthermore, there are ongoing efforts to understand the genetic and biologic differences that might affect disease outcomes in lower-resource countries (Porter, 2009).
The Moroccan Ministry of Health and the Lalla Salma Foundation for Cancer Prevention and Treatment, launched on March 24, 2010 the National Cancer Prevention and Control Plan (NCPCP), in order to reduce the morbidity and mortality from cancer and to improve the quality of life for patients. Since the implementation of the NCPCP, national–scale operations of breast cancer screening have been regularly carried out everywhere throughout the Kingdom, and early diagnosis services for breast cancer are already available in all reference centers of reproductive health. The target population for breast cancer screening in Morocco is women aged from 45 to 69 years, or women with a family history of breast cancer (grandmother, mother, aunt, sister) (Lalla Salma Foundation for Cancer Prevention and Treatment, 2011). Further studies are needed to explore the impact of this program on breast cancer incidence and mortality in Moroccan women.
In conclusion, although the incidence of female breast cancer in Morocco is lower than Western countries, evidence shows that breast cancer in Moroccan women is rising. This increase of breast cancer incidence has been observed in parallel with reproductive behavior changes and adoption of a Western lifestyle. Further studies are recommended to explore the determinants of breast cancer in Moroccan women. In addition, information regarding survival and mortality of breast cancer need to be collected to guide decision makers to improve breast cancer management in Morocco.
Acknowledgements
The authors thank Dr. K. Alami for English editing.
Statement conflict of Interest
The authors declare that they have no competing interests.
References
- Abahssain H, Lalya I, El M’rabet FZ, et al. Breast cancer in moroccan young women: a retrospective study. BMC Res Notes. 2010;3:286. doi: 10.1186/1756-0500-3-286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amadou A, Torres-Mejía G, Hainaut P, Romieu I. Breast cancer in Latin America: global burden, patterns, and risk factors. Salud Publica Mex. 2014;56:547–54. doi: 10.21149/spm.v56i5.7379. [DOI] [PubMed] [Google Scholar]
- Belot A, Velten M, Grosclaude P, et al. Estimation nationale de l’incidence et de la mortalitépar cancer en France entre 1980 et 2005 (Institut de veille sanitaire Saint-Maurice (France) 2008 [Google Scholar]
- Boder JME, Elmabrouk Abdalla FB, Elfageih K, et al. Breast cancer patients in Libya: Comparison with European and central African patients. Oncol Lett. 2011;2:323–30. doi: 10.3892/ol.2011.245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boufettal H, Noun M, Samouh N. Breast cancer in young patient in Morrocco. Cancer Radiother. 2010;14:698–703. doi: 10.1016/j.canrad.2010.04.007. [DOI] [PubMed] [Google Scholar]
- Boyle P, Howell A. The globalisation of breast cancer. Breast Cancer Res. 2010;12:7. doi: 10.1186/bcr2736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cancer Registry of Tunisia. Registre Des Cancers Nord-Tunisie. Données 2004 –2006. Ministère de la Sante Publique 2012. 2004-2006. Available from: http://www.insp.rns.tn/doc/cancer/cancer17.pdf .
- Cancer Registry of Casablanca. Registre des cancers du grand Casablanca, Rapport 2004. 2004. Available from: http://www.contrelecancer.ma/
- Cancer Registry of Saudi Arabia. Cancer Incidence Report Saudi Arabia 2004. Ministry of Health, Saudi Cancer Registry; April 2008. 2004 [Google Scholar]
- Cancer Registry of Rabat. Incidence des cancers àRabat 2005. Ministère de la Santédu Maroc. 2005:2009. [Google Scholar]
- Cancer Incidence in Jordan. Ministry of Health Non-Communicable Diseases, Directorate Jordan Cancer Registry. 2005. Available from: www.moh.gov.jo .
- Cancer Registry of Casablanca. Registre des cancers du grand Casablanca, Rapport 2005–2007. 2005–2007 Available from: http://www.contrelecancer.ma/ [Google Scholar]
- Cancer Registry of Canada-Alberta. 2006 Annual Report of Cancer Statistics; Juin 2009. 2006. Available from: http://www.albertahealthservices.ca/assets/healthinfo/poph/hi-poph-surv-cancer-alta-cancer-registry-2006.pdf .
- Cancer Incidence in Sweden. The National Board of Health and Welfare. Centre for Epidemiology. 2006. [December 19 2007]. Available from: http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/9325/2007-42-16_20074216.pdf .
- Cancer Registry of Algeria. Registre des Tumeurs d’Alger Année 2006. Ministère de la santéet de la population, Institut national de sante publique. 2006. Available from: http://www.sante.dz/insp/registre-tumeurs-alger-2006.pdf .
- Cancer Registry of Rabat. Incidence des cancers àRabat 2006–2008. Ministère de la Santédu Maroc; juin 2012. 2006–2008 [Google Scholar]
- Cancer Registry of Egypt- Aswan. Egypt Cancer Profile Aswan 2008. Ministry of Health; May 2010. 2008. Available from: http://cancerregistry.gov.eg/
- Chouchane L, Boussen H, Sastry KSR. Breast cancer in Arab populations: molecular characteristics and disease management implications. Lancet Oncol. 2013;14:417–24. doi: 10.1016/S1470-2045(13)70165-7. [DOI] [PubMed] [Google Scholar]
- Corbex M, Bouzbid S, Boffetta Features of breast cancer in developing countries, examples from North-Africa. Eur J Cancer. 2014;50:1808–18. doi: 10.1016/j.ejca.2014.03.016. [DOI] [PubMed] [Google Scholar]
- DeSantis CE, Bray F, Ferlay J, et al. International variation in female breast cancer incidence and mortality rates. Cancer Epidemiol Biomarkers Prev. 2015;24:1495–1506. doi: 10.1158/1055-9965.EPI-15-0535. [DOI] [PubMed] [Google Scholar]
- El Mistiri M, Salati M, Marcheselli L, el al. Cancer incidence, mortality, and survival in Eastern Libya: updated report from the Benghazi Cancer Registry. Ann Epidemiol. 2015;25:564–68. doi: 10.1016/j.annepidem.2015.03.012. [DOI] [PubMed] [Google Scholar]
- Forman D, Bray F, Brewster DH, et al., editors. Cancer Incidence in Five Continents. IARC; 2014. [Google Scholar]
- Ghoncheh M, Pournamdar Z, Salehiniya H. Incidence and mortality and epidemiology of breast cancer in the world. Asian Pac J Cancer Prev. 2016;17:43–6. doi: 10.7314/apjcp.2016.17.s3.43. [DOI] [PubMed] [Google Scholar]
- High Commission for Planning, Morocco. Recensement Général de la Population et de l’Habitat 2014. 2016. [Accessed October 2016]. Available from: http://www.hcp.ma/
- Harford JB. Breast-cancer early detection in low-income and middle-income countries: do what you can versus one size fits all. Lancet Oncol. 2011;12:306–12. doi: 10.1016/S1470-2045(10)70273-4. [DOI] [PubMed] [Google Scholar]
- Iqbal J, Ginsburg O, Rochon PA, Sun P, Narod SA. Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA. 2015;313:165–73. doi: 10.1001/jama.2014.17322. [DOI] [PubMed] [Google Scholar]
- Jazayeri SB, Saadat S, Ramezani R, Kaviani A. Incidence of primary breast cancer in Iran: Ten-year national cancer registry data report. Cancer Epidemiol. 2015;39:519–27. doi: 10.1016/j.canep.2015.04.016. [DOI] [PubMed] [Google Scholar]
- Kim Y, Yoo KY, Goodman MT. Differences in incidence, mortality and survival of breast cancer by regions and countries in Asia and contributing factors. Asian Pac J Cancer Prev. 2015;16:2857–70. doi: 10.7314/apjcp.2015.16.7.2857. [DOI] [PubMed] [Google Scholar]
- Lalla Salma Foundation for Cancer Prevention and Treatment. “Guide de détection précoce des cancers du sein et du col de l’utérus au Maroc”, Rabat. 2011:2011. [Google Scholar]
- Laamiri FZ, Bouayad A, Hasswane N, et al. Risk factors for breast cancer of different age groups: Moroccan data? Open J Obstet Gynecol. 2015;5:79. [Google Scholar]
- Maamri A, El Hfid M, Chafi A, Boutayeb A. Cervix and breast cancers in Oujda city in Eastern Morocco: Determinants and risk factors. Open J Prev Med. 2012;2:9–15. [Google Scholar]
- Mathew A, George PS, Arjunan A, et al. Temporal trends and future prediction of breast cancer incidence across age groups in Trivandrum, south India. Asian Pac J Cancer Prev. 2016;17:2895–99. [PubMed] [Google Scholar]
- Ministry of health. Morocco‟Direction de la Planification et des Ressources Financières, Division de la Planification et des Etudes, Service des Etudes et de l’Information Sanitaire, ed. [Accessed on October 2016];Rapport de l’Enquête Nationale sur la Population et la SantéFamiliale, la féconditéet la santéde la population au Maroc. 1987 1989 Available from: https://dhsprogram.com/pubs/pdf/SR163/SR163.pdf . [Google Scholar]
- Ministry of health. Morocco‟Direction de la Planification et des Ressources Financière, Service des Etudes et de l’Information Sanitaire. [Accessed October 2016];Enquête sur la Santéet la Réactivitédu Système de SantéMaroc. 2003 2007 Available from: http://www.sante.gov.ma/Publications/Etudes_enquete/Documents/ESRSSM2003.pdf . [Google Scholar]
- Ministry of health. Morocco‟Direction de la Planification et des Ressources Financières, Division de la Planification et des Etudes, Service des Etudes et de l’Information Sanitaire. Rapport de l’Enquête Nationale sur la Population et la SantéFamiliale ENPSF 2011. 2011. [Accessed on October 2016]. Available from: http://www.sante.gov.ma/Documents/Enqu%C3%AAte%20.pdf .
- Mobley LR, Kuo TM. United States health policies and late-stage breast and colorectal cancer diagnosis: why such disparities by age? Health Econ Rev. 2015;5:58. doi: 10.1186/s13561-015-0058-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Najjar H, Easson A. Age at diagnosis of breast cancer in Arab nations. Int J Surg. 2010;8:448–52. doi: 10.1016/j.ijsu.2010.05.012. [DOI] [PubMed] [Google Scholar]
- Nejmi M, Boutayeb S. Cancer trends and risk factors in Morocco. In cancer care in countries and societies in Transition, (Springer) 2016:25–45. [Google Scholar]
- Porter P. “Westernizing” women’s risks? Breast cancer in lower-income countries. N Engl J Med. 2008;358:213–16. doi: 10.1056/NEJMp0708307. [DOI] [PubMed] [Google Scholar]
- Porter PL. Global trends in breast cancer incidence and mortality. Salud Publica Mex. 2009;51:141–46. doi: 10.1590/s0036-36342009000800003. [DOI] [PubMed] [Google Scholar]
- Schlichting JA, Soliman AS, Schairer C, et al. Breast cancer by age at diagnosis in the Gharbiah, Egypt, population-based registry compared to the United States Surveillance, Epidemiology, and End Results Program 2004-2008. Biomed Res Int. 2015;2015:381574. doi: 10.1155/2015/381574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shulman LN, Willett W, Sievers A, Knaul FM. Breast cancer in developing countries: opportunities for improved survival. J Oncol. 2010;29:595167. doi: 10.1155/2010/595167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slaoui M, Razine R, Ibrahimi A, et al. Breast cancer in Morocco: a literature review. Asian Pac J Cancer Prev. 2014;15:1067–74. doi: 10.7314/apjcp.2014.15.3.1067. [DOI] [PubMed] [Google Scholar]
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics 2012. CA Cancer J Clin. 2015;65:87–108. doi: 10.3322/caac.21262. [DOI] [PubMed] [Google Scholar]
- Toselli S, Gualdi-Russo E, Boulos D. Prevalence of overweight and obesity in adults from North Africa. Eur J Public Health. 2014;24:31–9. doi: 10.1093/eurpub/cku103. [DOI] [PubMed] [Google Scholar]
- The United Nations Development program. The 2015 Human Development Report USA. 2015. [Accessed October 2016]. Available from: http://hdr.undp.org/sites/default/files/2015_human_development_report.pdf .
- Znati K, Bennis S, Abbass F, Akasbi Y. Breast cancer in young patient in Morocco. Gynecol Obstet Fertil. 2014;42:149–54. doi: 10.1016/j.gyobfe.2011.08.014. [DOI] [PubMed] [Google Scholar]