

Abstract
Knowledge and concern degree about work-related radiation hazards remained unknown among orthopedic surgeons. The aim of the cross-sectional study is to investigate whether the knowledge degree of work-related radiation is associated with psychological distress among orthopedic surgeons. This cross-sectional study sent electronic questionnaire via WeChat to orthopedic surgeons nationwide. Concern and knowing degree over radiation exposure was evaluated by a single self-reported question. Professional evaluation of concern degree was reflected by general psychological distress, which was assessed with the Kessler 10 scale (K10) and depressive symptoms with the Center for Epidemiologic Studies Depression Scale (CES-D). Only 43.23% (115/266) respondents knew well about radiation and a total of 78.20% (208/266) respondents considered radiation exposure as a great concern. Among those who reported concerns about radiation exposure, a total of 57.69% (120/208) respondents reported knowing little about radiation. Respondents who reported concerns over radiation exposure were significantly associated with higher scores on CES-D and K10 (P < .05). Among respondents who reported concerns over radiation exposure, those who have fewer knowledge about radiation, had higher CES-D and K10 scores than those who knew well about radiation (P < .05). Among respondents who reported no concerns over radiation exposure, those who knew little about radiation still had higher CES-D and K10 scores (P < .05). Fewer radiation knowledge tends to induce more radiation concerns associated with higher psychological distress in orthopedic surgeons. Radiation knowledge should be enhanced for surgeons who daily work with radiation-related fluoroscopy.
Keywords: bibliometric analysis, orthopedic surgeons, psychological distress, radiation concerns, radiation exposure, work health
1. Introduction
The fluoroscopically guided technique has provided effective assistance for orthopedic surgery, whose drawback appears to dramatically increase radiation exposure to surgeons as well as other medical staff.[1] Orthopedic surgeons can be exposed to primary radiation and secondary radiation from iatrogenic X-ray. Primary radiation refers to direct radiation exposure while a surgeon enters the space between x-ray generator and receptor, and secondary radiation mainly refers to scattered radiation.[2] In general, radiation exposure is accused for causing a series of physical and mental illness, with stochastic and deterministic effect.[3] The accumulated radiation exposure over time has been reported to be associated with cancer, cataracts and other diseases,[4] especially the organs sensitive to radiation (eg, gonads, bone marrow, breast, cornea).[1] Thus, radiation exposure is a great concern for orthopedic surgeons as a special group routinely applying radiation-related technique.[5,6]
Occupational health problem in hospital is came up with lately and valued as both physical and mental obstacles for all healthcare workers.[7] In an attempt to minimize sequelae of occupational exposure to ionizing radiation, the International Commission of Radiation Protection (ICRP) has published the maximum, yearly, occupational exposure limit for all sensitive organs or tissues.[8] Occupational exposure limit for eye has been already updated from 150 to 20mSv per year recommended by ICRP.[9] These recommended limits should raise the attention of all orthopedic surgeons, because they routinely used radiation-related fluoroscopy to conduct surgeries. However, knowledge and concern degree about work-related radiation hazards remained unknown among orthopedic surgeons, although many studies have indicated relatively safe radiation dosage accumulated per year in various surgeries.[10–12] Therefore, the aim of the cross-sectional study is to investigate whether the knowledge degree of work-related radiation is associated with psychological distress among orthopedic surgeons.
2. Methods
2.1. General information
The cross-sectional study was reviewed and approved by the Ethical Commission of Shanghai Tenth People's Hospital. We provided a complete description of this study to all the participants whose consent were obtained prior to the survey and the potential publications of the research. We sent electronic questionnaires to orthopedic surgeons nationwide via WeChat as well as paper questionnaires during national conference from May 2015 to Dec 2015. We recruited orthopedic surgeons include chief physicians, associate chief physicians, attending physicians, resident doctors, and graduates of orthopedics.
The inclusion criteria were (1) aged 18 years or older; (2) orthopedic surgeons including various subspecialties such as spine, traumatic orthopedics, foot and ankle, as well as joint who routinely employing radiation-related fluoroscopy; (3) physically and psychologically capable of understanding and providing consent for study participation. We excluded invalid paper questionnaires: (1) incomplete responses to required field; (2) unidentified answers to required questions; (3) evident mistakes of the replied answers; (4) others that we researchers independently confirmed invalid.
2.2. Measures
Participants were surveyed via a self-reported questionnaire which we settled with mainly a series of multiple choice questions and part fill in the blanks for this study. Demographic characteristics including gender, age, height, weight, occupational title, period of employment and subspecialty (repeatable) were obtained with questions. To evaluate knowledge and concern over radiation exposure, the participants answered the questions, “Do you concern and know about radiation exposure” and chose the most appropriate one from the following answers “know little and not concern,” “know well but not concern,” “know little but concern,” and “know well and concern.”
To further evaluate radiation concerns, participants needed to provide informations of their protection strategies (eg, leaded glasses, real-time monitor, thyroid gland shield, leaded apron, and leaded hat). General psychological distress was assessed with the Kessler 10 scale (K10), and depressive symptoms with the Center for Epidemiologic Studies Depression Scale (CES-D). K10 was presented with priority in detecting depressive disorders which also worked on anxiety.[13] CES-D is one of the most widely used self-administered instruments for depression screening.[14] Reliability and validity of all those scales have been proved and confirmed in prior studies.[13,15,16]
2.3. Statistical analysis
Inter-group comparisons of the dependent variables, including K10 and CES-D scores, were performed using an analysis of variance (ANOVA). Pearson correlations test was conducted to investigate the potential relationship between employment period and psychological assessment (K10 and CES-D). A P < .05 indicated statistical significance and all statistical analysis was performed via SPSS version 20.0 (SPSS, Inc., Chicago, IL). We also conducted a bibliometric analysis via GoPubmed to provide a macroscopic view of global publications concerning orthopedic radiation. Pearson correlation test was used to investigate the potential correlation between knowledge contributions over orthopedic radiation and gross domestic product (GDP) of a country.
3. Results
A total of 500 questionnaires were sent, and we received 277 responses but excluded 11 invalid questionnaires. There were 266 orthopedic surgeons who enrolled in this study as participants and completed the questionnaire, all of whom were males. Informations of demographic characteristics were listed in Table 1. The average age was 36.80 ± 8.12 years old, and the average employment period was 12.11 ± 8.05 years. Chief physician accounted 18.8% for the sample, whereas associate chief doctor 20.7%, attending physician 25.9%, resident doctor accounted for 9.8% and graduate students for 22.6%. Only 43.23% (115/266) respondents knew well about radiation and a total of 78.20% (208/266) respondents considered radiation exposure was a great concern. Among those who concerned about radiation exposure, a total of 57.69% (120/208) respondents reported knowing little about radiation.
Table 1.
Basic characteristics of participants specialized in orthopedics.

ANOVA results demonstrated no significant differences in CES-D or K10 between different subspecialties and work degree (P > .05). However, concern over radiation exposure significantly associated with higher scores on CES-D as well as K10 (P < .05) (Table 2). Respondents who reported knowing little about radiation also presented higher scores on CES-D and K10 (P < .05). Multiple comparisons demonstrated that among those who concerned radiation, fewer knowledge about radiation led to more radiation concern associated with higher CES-D (P = 0.049) and K10 scores (P < .001). Among respondents who reported no concerns over radiation exposure, those who knew little about radiation still had higher CES-D and K10 scores (P < .05). However, there were no correlations between employment period and psychological assessment, either K10 or CES-D (P > .05). Most participants (89.10%) took various protection strategies to minimize the radiation hazards (Fig. 1), but only 4.51% participants (12/266) wore leaded glasses to protect their eyes. Respondents who reported concerns over radiation tended to take protection strategies (P < .05).
Table 2.
K10 and CES-D among participants grouped by radiation concern and knowledge.

Figure 1.
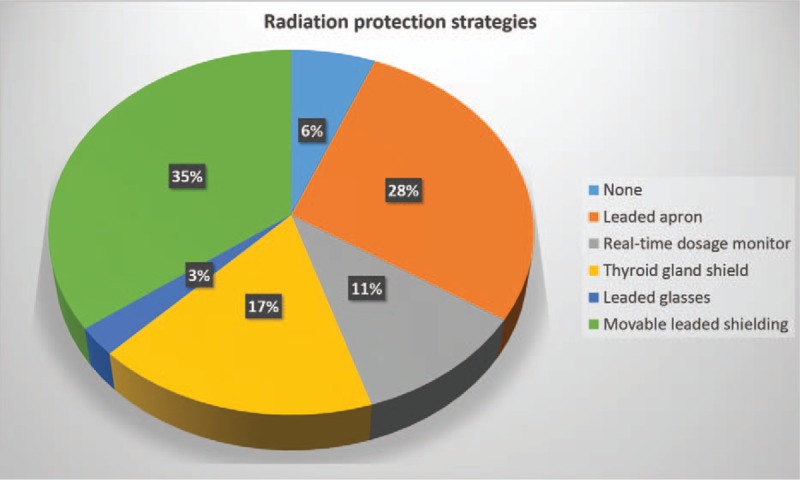
Proportional map of different radiation protection strategies in participants.
4. Discussion
Orthopedic surgeons are routinely exposed with fluoroscopic radiation but radiation knowledge varies. This was the first study to demonstrate that knowledge deficiency might lead to more radiation concerns associated with higher psychological distress in orthopedic surgeons. We also confirmed the protection deficiency of radiation hazards among orthopedic surgeons over the nation, which further confirmed their reported concerns over radiation. Thus, it is essential to enhance protection management for minimizing radiation exposure as well as providing more relevant knowledge to comfort surgeons.
As a kind of mental health problem, psychological distress is a ubiquitous phenomenon among current social life. Psychological distress is an umbrella term that encompasses stress, burnout, depression, anxiety, and other related mental health problems.[17] Inducements of psychological distress are complicate and interactive, stress is usually associated with the development of mental health problems, in which concern over a physical condition may also play a role.[18] Scholars have indicated long-term, low-dose rate radiation exposure would cause psychological stress and an increased risk of depression decades later.[19] Review to Chernobyl accident and Japan's nuclear disaster also presented significant association of radiation exposure and subsequent psychological distress.[20–24] The current study further confirmed the association of concern over radiation exposure with psychological distress. However, radiation itself causes DNA damage, increases risk of cancer, and is associated with psychological stress responses.[25] Cause of psychological distress among subjects could both be concern over radiation exposure and the radiation effect itself, which is difficult to accurately distinguish.
Protection strategies of radiation exposure to orthopedic surgeons were gradually widespread and published since Barry reported in 1984.[26] Multiple studies have introduced more advanced fluoroscopy devices to assist an orthopedic surgery, and numerous strategies protection has been proposed to minimize the radiation exposure.[27–33] Lee et al[1] indicated that following factors could reduce radiation exposure during intraoperative use of C-arm, which included distance from the patient, C-arm configuration, radio-protective equipment, rotating the surgeons’ eyes away from the patient, and avoiding direct exposure of surgeons’ hands. Yu and Khan[31] found that orthopedic surgeons can decline potential radiation risks by optimizing variables such as the use of barriers, knowledge of position, distance from the radiation source, and use of advanced image guidance navigation-assisted technology. However, the inconvenient truths were that only 4.51% participants wore leaded glasses to protect their eyes, although the eye was one of the most sensitive organs to radiation exposure[34]. Only 19.17% participants reported wearing real-time dosage monitor, although real-time dosage monitor was well validated strategy to minimize radiation exposure[35]. Only 30.45% participants reported wearing thyroid gland shield, although radiation-induced thyroid cancer has been well documented.[36]
Even among orthopedic surgeons, who should be more knowledgeable about radiation exposure than other public workers, uncertainty about radiation exposure still existed and created a significant negative effect on their mental health.[14] Indeed, we did observe a rapid increase of publication productivity concerning orthopedic radiation over the last decades, which meant more and more surgeons conducted the related research and increase their knowledge in a way. Bibliometric analysis demonstrated that only 3631 publications concerning orthopedic radiation were obtained over 5 decades, although we could observe a nearly triple increase over the last 2 decades (Fig. 2). However, the global map demonstrated that the scientific productivity of orthopedic radiation concentrated in western countries (Fig. 3). As demonstrated in Table 3, strong correlation between knowledge contributions over orthopedic radiation were strongly correlated with GDP (r2 = 0.762, P < .0001). However, we should also realize that most research activities over orthopedic radiation concentrated in developed countries. These knowledge deficiency of radiation might play a role in radiation concerns, because people tend to be afraid something they did not know well. As we observed in the current study, knowledge deficiency over radiation might contribute to the radiation concern associated with higher CES-D and K10 scores. The cumulative exposure doses to the surgeon can be maintained well within annual permissible limits.[33]
Figure 2.

Publications concerning orthopedic radiation over the past five decades.
Figure 3.

Global distributions of publications concerning orthopedic radiation.
Table 3.
Global distributions of publications concerning orthopedic radiation.

Nevertheless, this cross-sectional study is not without limitations. First of all, a presented correlation is not the cause-and-effect relationship. We could not identify whether long-term radiation exposure might induce psychological distress. Secondly, we did not investigate radiation knowledge of patients and subspecialty analysis, which we will disclose in the near future study. We need a larger sample to participate in the future study, although we have adequate data to clarify the issue we aimed to discuss in the current study.
5. Conclusions
This was the first study to demonstrate that knowledge deficiency might contribute to the radiation concerns associated with higher psychological distress in orthopedic surgeons. Radiation knowledge should be enhanced with more education and research activities for surgeons who daily work with radiation-related fluoroscopy, especially in developing countries. However, when interpreting these data, we should realize that this cross-sectional study could not define a cause-and-effect relationship for any potential associations identified in the study.
Footnotes
Abbreviations: ANOVA = analysis of variance, CES-D = Epidemiologic Studies Depression Scale, GDP = gross domestic product, ICRP = International Commission of Radiation Protection, K10 = Kessler 10 scale.
GF, YW, and CG equally contribute to the study.
The authors report no conflicts of interest.
References
- [1].Yamashita K, Higashino K, Wada K, et al. Radiation exposure to the surgeon and patient during a fluoroscopic procedure: how high is the exposure dose? A cadaveric study. Spine (Phila Pa 1976) 2016. [DOI] [PubMed] [Google Scholar]
- [2].Efstathopoulos EP, Pantos I, Andreou M, et al. Occupational radiation doses to the extremities and the eyes in interventional radiology and cardiology procedures. Br J Radiol 2011;84:70–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Ahn Y, Kim CH, Lee JH, et al. Radiation exposure to the surgeon during percutaneous endoscopic lumbar discectomy: a prospective study. Spine (Phila Pa 1976) 2013;38:617–25. [DOI] [PubMed] [Google Scholar]
- [4].Fattal P, Goldstein JA. A novel complete radiation protection system eliminates physician radiation exposure and leaded aprons. Catheter Cardiovasc Interv 2013;82:11–6. [DOI] [PubMed] [Google Scholar]
- [5].Fan G, Han R, Gu X, et al. Navigation improves the learning curve of transforamimal percutaneous endoscopic lumbar discectomy. Int Orthop 2017;41:323–32. [DOI] [PubMed] [Google Scholar]
- [6].Fan G, He S, Chen Z. Musculoskeletal pain and cancer risk of staff working with fluoroscopically guided procedures. J Am Coll Cardiol 2015;66:759–60. [DOI] [PubMed] [Google Scholar]
- [7].Goldstein JA. Orthopedic afflictions in the interventional laboratory: tales from the working wounded. J Am Coll Cardiol 2015;65:827–9. [DOI] [PubMed] [Google Scholar]
- [8].Fan G, Fu Q, Gu G, et al. Radiation exposure to surgeon in minimally invasive transforaminal lumbar interbody fusion with novel spinal locators. J Spinal Disord Tech 2015;28:E173–80. [DOI] [PubMed] [Google Scholar]
- [9].Waddell BS, Waddell WH, Godoy G, et al. Comparison of ocular radiation exposure utilizing three types of leaded glasses. Spine (Phila Pa 1976) 2016;41:E231–6. [DOI] [PubMed] [Google Scholar]
- [10].Fitousi NT, Efstathopoulos EP, Delis HB, et al. Patient and staff dosimetry in vertebroplasty. Spine (Phila Pa 1976) 2006;31:E884–9. [DOI] [PubMed] [Google Scholar]
- [11].Mroz TE, Abdullah KG, Steinmetz MP, et al. Radiation exposure to the surgeon during percutaneous pedicle screw placement. J Spinal Disord Tech 2011;24:264–7. [DOI] [PubMed] [Google Scholar]
- [12].Taher F, Hughes AP, Sama AA, et al. 2013 Young Investigator Award winner: how safe is lateral lumbar interbody fusion for the surgeon? A prospective in vivo radiation exposure study. Spine (Phila Pa 1976) 2013;38:1386–92. [DOI] [PubMed] [Google Scholar]
- [13].Furukawa TA, Kessler RC, Slade T, et al. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol Med 2003;33:357–62. [DOI] [PubMed] [Google Scholar]
- [14].Matsuoka Y, Nishi D, Nakaya N, et al. Concern over radiation exposure and psychological distress among rescue workers following the Great East Japan Earthquake. BMC Public Health 2012;12:249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Zhang Y, Ting RZ, Lam MH, et al. Measuring depression with CES-D in Chinese patients with type 2 diabetes: the validity and its comparison to PHQ-9. BMC Psychiatry 2015;15:198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Zakay D, Shub J. Concurrent duration production as a workload measure. Ergonomics 1998;41:1115–28. [DOI] [PubMed] [Google Scholar]
- [17].Facey AD, Tallentire V, Selzer RM, et al. Understanding and reducing work-related psychological distress in interns: a systematic review. Intern Med J 2015;45:995–1004. [DOI] [PubMed] [Google Scholar]
- [18].Kim S, Noh D, Park SI. Mediating effect of stress on the association between early trauma and psychological distress in Korean college students: a cross-sectional observational study. J Psychiatr Ment Health Nurs 2015;22:784–91. [DOI] [PubMed] [Google Scholar]
- [19].Yen PN, Lin IF, Chang WP, et al. Risk factors of depression after prolonged low-dose rate environmental radiation exposure. Int J Radiat Biol 2014;90:859–66. [DOI] [PubMed] [Google Scholar]
- [20].Bromet EJ, Havenaar JM. Psychological and perceived health effects of the Chernobyl disaster: a 20-year review. Health Phys 2007;93:516–21. [DOI] [PubMed] [Google Scholar]
- [21].Bromet EJ, Havenaar JM, Guey LT. A 25 year retrospective review of the psychological consequences of the Chernobyl accident. Clin Oncol (R Coll Radiol) 2011;23:297–305. [DOI] [PubMed] [Google Scholar]
- [22].Tsubokura M, Hara K, Matsumura T, et al. The immediate physical and mental health crisis in residents proximal to the evacuation zone after Japan's nuclear disaster: an observational pilot study. Disaster Med Public Health Prep 2014;8:30–6. [DOI] [PubMed] [Google Scholar]
- [23].Koscheyev VS, Leon GR, Gourine AV, et al. The psychosocial aftermath of the Chernobyl disaster in an area of relatively low contamination. Prehosp Disaster Med 1997;12:41–6. [DOI] [PubMed] [Google Scholar]
- [24].Pastel RH. Radiophobia: long-term psychological consequences of Chernobyl. Mil Med 2002;167:134–6. [PubMed] [Google Scholar]
- [25].Cwikel JG, Gidron Y, Quastel M. Low-dose environmental radiation, DNA damage, and cancer: the possible contribution of psychological factors. Psychol Health Med 2010;15:1–6. [DOI] [PubMed] [Google Scholar]
- [26].Barry TP. Radiation exposure to an orthopedic surgeon. Clin Orthop Relat Res 1984;182:160–4. [PubMed] [Google Scholar]
- [27].Huppertz A, Radmer S, Wagner M, et al. Computed tomography for preoperative planning in total hip arthroplasty: what radiologists need to know. Skeletal Radiol 2014;43:1041–51. [DOI] [PubMed] [Google Scholar]
- [28].Akins R, Abdelgawad AA, Kanlic EM. Computer navigation in orthopedic trauma: safer surgeries with less irradiation and more precision. J Surg Orthop Adv 2012;21:187–97. [DOI] [PubMed] [Google Scholar]
- [29].Hammer GP, Scheidemann-Wesp U, Samkange-Zeeb F, et al. Occupational exposure to low doses of ionizing radiation and cataract development: a systematic literature review and perspectives on future studies. Radiat Environ Biophys 2013;52:303–19. [DOI] [PubMed] [Google Scholar]
- [30].Mulconrey DS. Fluoroscopic radiation exposure in spinal surgery: in vivo evaluation for operating room personnel. J Spinal Disord Tech 2013;29:E331–5. [DOI] [PubMed] [Google Scholar]
- [31].Yu E, Khan SN. Does less invasive spine surgery result in increased radiation exposure? A systematic review. Clin Orthop Relat Res 2014;472:1738–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Cecen GS, Gulabi D, Pehlivanoglu G, et al. Radiation in the orthopedic operating theatre. Acta Orthop Traumatol Turc 2015;49:297–301. [DOI] [PubMed] [Google Scholar]
- [33].Mahajan A, Samuel S, Saran AK, et al. Occupational radiation exposure from C arm fluoroscopy during common orthopaedic surgical procedures and its prevention. J Clin Diagn Res 2015;9:rc01–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Struelens L, Schoonjans W, Schils F, et al. Extremity and eye lens dosimetry for medical staff performing vertebroplasty and kyphoplasty procedures. J Radiol Prot 2013;33:635–45. [DOI] [PubMed] [Google Scholar]
- [35].Safari MJ, Wong JH, Kadir KA, et al. Real-time eye lens dose monitoring during cerebral angiography procedures. Eur Radiol 2016;26:79–86. [DOI] [PubMed] [Google Scholar]
- [36].Nachalon Y, Katz O, Alkan U, et al. radiation-induced thyroid cancer: gender-related disease characteristics and survival. Ann Otol Rhinol Laryngol 2016;125:242–6. [DOI] [PubMed] [Google Scholar]