

Abstract
Background:
One of the most common reasons of elbow and forearm pain is lateral epicondylitis diagnosed based on clinical examination. The extracorporeal shock wave therapy is applied for less invasive treatments with different dosages. This study aimed to investigate the effects of high- and low-dose ESW in treating the lateral epicondylitis.
Materials and Methods:
This clinical trial was done in Al Zahra medical center on 40 patients who were selected randomly and divided into two groups. After VAS, the first group was treated by Duolith SD1 shock wave, energy of 0.25 mj/mm2, 1000 shocks; the second was treated by focus with the energy of 0.10 mj/mm2, 1000 shocks per session for 15 minutes with weekly intervals in three sessions. The patients were also treated with drugs (NSAIDs) and the visual analog scale (VAS) was reassessed 1 week after the last session and 12 weeks after finishing the treatment.
Results:
The mean of pain intensity during study was decreased in the two groups but reduction of pain intensity in the low-dose groups was higher than the high-dose groups (P = 0.001). Changes in other parameters including wrist extension test, middle finger extension test and PG was also similar.
Conclusion:
Extra corporeal shockwave therapy can be effective in treating lateral epicondylitis, but its effects usually appear in after 2 or 3 months and using the low dose of this treating method has more desirable therapeutic effects.
Keywords: Lateral epicondilitis, musculocutaneus diseases, shock wave
Introduction
Lateral epicondylitis is one of the most common causes of forearm and elbow pain in adults. In 1883, this disease was known as tennis elbow due to the more prevalence in tennis players.[1] It can be seen usually in people over 35 with the age peak of 40–50 years. It is more common in men among tennis players, but in general population it has the same prevalence in both sexes.[2] In most cases, the location of muscle’s origin of extensor carpi radialis brevis is involved, but it is not much common to involve the muscles of extensor digitrom communis, extensor carpi radialis longus and extensor carpi ulnaris.
Usually it begins gradually and is more related to the repeated activities in upper extremities especially the extensor muscles of wrist that includes for example supination and pronation.[3] These patients complain about the pain of outer forearm or the proximal and distal areas. They generally don’t complain about of paresthesia and numbness; in test, the painful point is on the outer epicondyle.[3] We can confirm the diagnosis with the tests such as wrist extension and long finger extension, but sometimes this disease is mistaken with entrapment of posterior interosseous of radial nerve; however, this problem is less prevalent and the area of pain is in 3–4 cm distal to the outer epicondyle.[3]
Treatments include avoiding aggravating activities, edible analgesics, physical modalities, braces, exercises such as eccentric strengthening wrist extensor, corticosteroid injection or autologous blood or PRP, surgery with the method of tenotomy under the ultrasounds guides and extracorporal shock wave therapy (ESWT) which are used for patients resistant to treatment.[3,4]
ESWT are a class of mechanical waves which are produced by the use of piezoelectric and electromagnetic technology. Shock wave modalities can generate rapidly rising acoustic waves with high-peak pressure amplitudes and the majority of energy flux is concentrated on a small focus. Its biological mechanisms for treating tendinopathies comprise destroying sensory unmyelinated nerve fibers and eliciting neovascularization in degenerative tissues.[5,6]
Entering mechanical impact of these waves in target area causes to increase the permeability in cell membrane and neovascularization in created small cavities by pulses in the tissue. The result of this process is the reduction in sensitivity of pain receivers and improvement of dying tissues. In the form of focused shock wave, the waves have short wavelength and high penetration depth and energy. Generated waves concentrate in a focal point away from the applicator’s surface and import the highest energy in that point, therefore, it is used to treat different areas in the body (deep and superficial) such as pains of lateral epicondylitis and classifying tendons.[7,8,9]
In radial form, the waves have long wavelength and low penetration depth and the most energy is imported to the body in the area of applicator surface. Thus, it is used for treating the body surface area.
Unlike ultrasound device applied in physiotherapy in which tissues are heated by extended high frequencies, ESWT effects on tissues by sending high-energy pulses two to three times per second and it takes about 12 weeks to appear its complete and beneficial effects.[10]
Since conservative treatments are generally prolonged and based on patient cooperation in doing recommended movements and on the other hand, the possibility of surgery is not always available, thus, the use of ESWT as a non-invasive procedure can be considered as an effective measure that does not require patient cooperation. In conducted studies, the positive effect of ESWT on lateral epicondylitis has been proved and the effect seems to be dose dependent.[4,11,12,13] For instance, in 2004, Rompe et al. concluded that ESWT is effective on tennis players’ elbow. They could achieve good therapeutic effects by applying focus type of ESWT and dosage of 0.09 mj/mm2 (low dose).[4] In 2005, Pettrone et al. proved the positive effect of low-dose ESWT on lateral epicondylitis,[6] but in 2011, Aroona et al. conducted the high-dose (0.22 mj/mm2) ESWT on lateral epicondylitis; this dosage had also good results in treatment,[7] but the levels of energy (low dose or high dose) has not been investigated yet. Thus, the present study was done with the aim of determining the effect of ESW in low dosage and high dosage in treating the patients with lateral epicondilitis.
Materials and Methods
This study is a clinical trial study done in 2013 in Al Zahra Medical Center of Isfahan. Samples were selected among the patients referring to the clinic of physical medicine with the diagnosis of lateral epicondylitis resistant to be treated on the base of clinical examination.
The meaning of being resistant to the treatment of lateral epicondylitis is failure to respond to a period of conventional treatments such as physical therapy, medication or injection of corticosteroids. In this study, 40 patients who met the inclusion criteria were selected and randomly divided into two groups of 20. Patients less than 18 years, pregnant women, patients with previous fractures and infections in the elbow and forearm as well as infected with RA and patients with coagulation disorders were excluded.
The first group, after doing VAS, was treated by Duolith SD1 shock wave device with focus method with the energy of 0.25 mj/mm2 and 1000 shocks; the second group was treated by focus with the energy of 0.10 mj/mm2 and 1000 shocks. Each session was of 15 minutes with weekly intervals of three sessions. During this period, in addition to the mentioned treatment, the patients were also treated by drugs (NSAIDs) and were re-tested by visual analog scale (VAS) a week after the last session and 12 weeks after finishing the treatment.
In order to do VAS, the patients were examined in five aspects including the patients’ main complain, the patient’s pain during wrist extension which is affected, the pain during the middle finger extension, pain in grip and pain in touching the maximum point of tenderness.
These data along with demographic information were finally analyzed by SPSS software and t tests, Chi-square and ANOVA test with repetition of observations.
Results
In this study, 40 patients were participated and they were divided into two groups of 20. The first group was treated with low dose and the second group was treated with high dose of shock wave. Average ages of the two groups receiving low and high doses were respectively 41.6 ± 9.3 and 44.8 ± 8.8 years and according to the T test, there was no significant difference between the two groups (P = 0.27). In case of gender distribution in these two groups, there were four and six males, respectively (30% vs. 20%) and the remaining patients were females and according to the Chi-square test, there was no significant difference based on gender distribution (P = 0.47).
Table 1 illustrates the mean and standard deviation of variables related to the treatment method applied to both high and low doses. According to the obtained results, the mean of pain intensity which was considered as the main complain of patients at the pre-intervention was respectively 6.25 ± 1.52 and 6.25 ± 1.52 in low-dose and high-dose groups and there was no difference between the two groups. One week after treatment, reduction of pain intensity in the low-dose group was higher so that the pain intensity reduced from 6.25 to 1.65 while in the high-dose group, reduction of pain intensity was lower and reached from 6.25 to 4.15. Also, in after 3 months the pain intensity in the high-dose group was higher than the low-dose group. The repeated measures ANOVA indicated that the average of differences in pain intensity from before the treatment to 3 months after that has significant difference between the two groups (P = 0.001). Changes in other parameters including middle finger extension test (MFET), wrist extension test (WET) and PG were the same with pain condition in patients and reduction in pain intensity was more in the low-dose group than the high-dose group. Also, the ANOVA test with repetition of observations indicated that changes in mentioned variables from before the treatment to 3 months after that among the two groups had significant difference (P > 0.05).
Table 1.
The mean and deviation of pain parameters in both groups
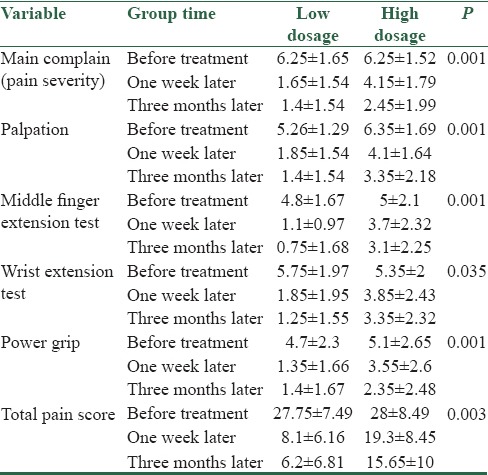
The average of total pain scores in mentioned maneuvers at pre-intervention in two groups of low and high doses were respectively 49/7 ± 75/27 and 49/8 ± 28. In a week after treatment, the mean of total pain score in two groups was respectively 16/6 ± 1/8 and 45/8 ± 3/19 and 3 months after treatment it was respectively 8/6 ± 2/6 and 10 ± 65/15; and according to the ANOVA test with repetition of observations, the changes in pain score had a significant difference between the two groups (P = 0.003). Also indicates the changes in total pain score in the two groups.
Discussion
The overall objective of this study was to compare the effect of ESWT high–low dose in treating the patients with lateral epicondylitis. In this study, two groups of 20 patients with mentioned disease were tested under two different doses of ESWT and treatment results of these two groups were compared. The two study groups didn’t have significant difference in case of age and sex distribution; thus, the confounding effect of these factors are likely to be neutralized in this study and obtained results are related to therapeutic effects of ESWT in patients.
Regarding the results of this study, the patients’ pain intensity before intervention was approximately equal in both groups, but a week after the treatment the pain reduction in the low-dose group was considerably lower and this difference also existed 3 months after the treatment. Of course, such a process existed also in palpation, MFET, PG and the total pain score; generally, the use of low-dose radiation has more desirable therapeutic results for the patients. Also, the use of low dose has lower possible side effects for the patients.
ESWT effects on the tissues by sending high-energy pulses at two to three times per second and it takes about 12 weeks to appear its complete and beneficial effects. So, the overall conclusion of the effectiveness of this treatment method can be evaluated and compared at the end of the third month. It also seems that the effect of ESWT is dose dependent, so that in 2004, Rompe et al. concluded that ESWT has an effect on tennis players’ elbow; they applied focus type of ESWT with a dosage of 0.09 (mj/mm2) (low dosage) and could achieve good therapeutic effects.[1] In another study which was conducted in 2011 by Mudo et al., high dose of ESWT (mj/mm2 0.22) was applied on lateral epicondylitis and this dosage had also good therapeutic effects.[3] In one study that was done in 2010, ESWT had a positive effect of plantar fasciitis.[10] Thus, the overall conclusion we can get from this study is that the use of ESWT can be effective in the treatment of lateral epicondylitis but due to the characteristics of this method, usually the therapeutic effects of this method appear in the patient 2 to 3 months after the treatment. On the other hand, the use of low dose of this treatment method has more beneficial therapeutic effects for the patients and the possibility of occurring side effects is less with the low dose. The use of this treatment method is recommended for the patients with mentioned disease.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Rompe JD, Decking J, Schoellner C, Theis C. Repetitive low-energy shock wave treatment for chronic lateral epicondylitis in tennis players. Am J Sports Med. 2004;32:734–43. doi: 10.1177/0363546503261697. [DOI] [PubMed] [Google Scholar]
- 2.Pettrone FA, McCall BR. Extracorporeal shock wave therapy without local anesthesia for chronic lateral epicondylitis. J Bone Joint Surg Am. 2005;87:1297–304. doi: 10.2106/JBJS.C.01356. [DOI] [PubMed] [Google Scholar]
- 3.Mudoo AD, Jing Y, Le-hua Y. Extracorporeal shock wave therapy for musculoskeletal disorders. Journal of Clinical Rehabilitative: Tissue Engineering Research Journal. 2011;5:6222–5. [Google Scholar]
- 4.Rompe JD, Maffulli N. Repetitive shock wave therapy for lateral elbow tendinopathy (tennis elbow): A systematic and qualitative analysis. Br Med Bull. 2007;83:355–78. doi: 10.1093/bmb/ldm019. [DOI] [PubMed] [Google Scholar]
- 5.Crowther MA, Bannister GC, Huma H, Rooker GD. A prospective, randomised study to compare extracorporeal shock-wave therapy and injection of steroid for the treatment of tennis elbow. J Bone Joint Surg Br. 2002;84:678–9. doi: 10.1302/0301-620x.84b5.12741. [DOI] [PubMed] [Google Scholar]
- 6.Faro F, Wolf JM. Lateral epicondylitis: Review and current concepts. J Hand Surg Am. 2007;32:1271–9. doi: 10.1016/j.jhsa.2007.07.019. [DOI] [PubMed] [Google Scholar]
- 7.Haake M, König IR, Decker T, Riedel C, Buch M, Müller HH Extracorporeal Shock Wave Therapy Clinical Trial Group. Extracorporeal shock wave therapy in the treatment of lateral epicondylitis. J Bone Joint Surg Am. 2002;84-A:1982–91. doi: 10.2106/00004623-200211000-00012. [DOI] [PubMed] [Google Scholar]
- 8.Speed CA, Nichols D, Richards C, Humphreys H, Wies JT, Burnet S, et al. Extracorporeal shock wave therapy for lateral epicondylitis--a double blind randomised controlled trial. J Orthop Res. 2002;20:895–8. doi: 10.1016/S0736-0266(02)00013-X. [DOI] [PubMed] [Google Scholar]
- 9.Stasinopoulos D, Johnson MI. Effectiveness of extracorporeal shock wave therapy for tennis elbow. Br J Sports Med. 2005;39:132–6. doi: 10.1136/bjsm.2004.015545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Vahdatpour B, Sajadieh S, Bateni B, Karami M, Sajjadieh H. Extracorporeal shock wave therapy in patients with plantar fasciitis. A randomized, placebo-controlled trial with ultrasonographic and subjective outcome assessments. J Res Med Sci. 2012;17:834–8. [PMC free article] [PubMed] [Google Scholar]
- 11.Hsu RW, Hsu WH, Tai CL, Lee KF. Effect of shock-wave therapy on patellar tendinopathy in a rabbit model. J Orthop Res. 2004;22:221–7. doi: 10.1016/S0736-0266(03)00138-4. [DOI] [PubMed] [Google Scholar]
- 12.Ohtori S, Inoue G, Mannoji C, Saisu T, Takahashi K, Mitsuhashi S, et al. Shock wave application to rat skin induces degeneration and reinnervation of sensory nerve fibres. Neurosci Lett. 2001;315:57–60. doi: 10.1016/s0304-3940(01)02320-5. [DOI] [PubMed] [Google Scholar]
- 13.Dorotka R, Sabeti M, Jimenez-Boj E, Goll A, Schubert S, Trieb K. Location modalities for focused extracorporeal shock wave application in the treatment of chronic plantar fasciitis. Foot Ankle Int. 2006;27:943–7. doi: 10.1177/107110070602701113. [DOI] [PubMed] [Google Scholar]