

Abstract
Introduction:
An inferior hip dislocation also called luxatio erecta femoris is a rare type of hip dislocation that is not widely reported in literature. Only 12 cases are reported in British literature.
Case Report:
This article reports a 17-year-old male involved in a road traffic accident, sustaining inferior hip dislocation. Following resuscitation, computed tomography confirmed the clinical diagnoses. Several attempts to perform a closed reduction of the hip under sedation and general anesthesia failed to reduce the dislocation. The patient underwent open reduction of his hip and capsule repair. Postoperatively no traction was applied, and the patient advised non-weight bearing on that side for 3 months.
Conclusion:
To our knowledge, this is the first reported case of an adult with an inferior hip dislocation not associated with a trochanteric fracture and required open reduction.
Keywords: Hip dislocation, capsular lesion, inferior hip dislocation, traumatic dislocation
What to learn from this Article?
Luxatio erecta femoris is a rare type of hip dislocation that requires urgent reduction using closed methods first; however, the open reduction may be needed especially in cases of associated femoral head fracture.
Introduction
Hip dislocations are infrequent occurrences, but most cases are associated with trauma [1]. Inferior dislocations represent only 2-5% of all hip dislocations, where the majority are posterior dislocations [2, 3, 4, 5].
Inferior dislocation of the hip, also called luxatio erecta femoris or infracotyloid dislocation, is the rarest type of hip dislocation with a poorly understood mechanism of injury, mainly occurring from high energy incidents, mostly from road traffic accidents or sports [1, 6, 7].
In this article, we are reporting a unique case of traumatic inferior hip dislocation and femoral head fracture within an adolescent sustained in road traffic injury eventually requiring open reduction in theater along with a literature review in order guide surgeons on how to treat this uncommon injury.
There are few cases of traumatic inferior dislocation reported in English literature, and most were managed with closed reduction except a case associated with a trochanteric fracture. To our knowledge, this is the first reported case of an adult with an inferior hip dislocation managed with open reduction and treated without skin traction.
The patient provided written informed consent for publication of this case report.
Case Report
A 17-year-old male was an unrestrained passenger in an automobile travelling between 60 and 70 mph. This car was the involved in a road traffic collision at an oblique angle with another vehicle. The patient in question was a rear seat, nearside passenger.
At the scene of the collision, the passenger-side front seat trapped the patient for approximately 1½ h. Once released the patient was then transferred by helicopter to a local trauma center.
Upon arrival, the patient was stable despite tachydcardia with Glascow coma scale of 15/15. Primary and secondary surveys were performed, and trauma team noted open wounds in both right forearm and left thigh. There were bruises and patient was complaining of pain and difficulty in using his jaw. The abdomen was soft and normal oxygen saturations were maintained. The extremities were neurovascularly intact distally, and the patient was complaining of pain in the right leg.
He had been administered opiate analgesia, oxygen and tranexamic acid. Once stabilized the patient was transferred for an urgent computer aided tomography (CT) scan, which revealed the following injuries: Subcondylar fracture of the mandible, open fracture of the right ulna and radius, open fracture of the left femur, inferior dislocation of the right hip joint, small splenic laceration, and contusion of left pulmonary base.
The same day as admission the patient was taken to the operating theater for reduction under general anesthesia of the inferior dislocation of the right hip joint. With hip abduction traction, external rotation and flexion of the hip joint multiple attempts were made to reduce the hip joint, but unsuccessfully. It was therefore considered necessary to attempt an open reduction of the inferior dislocation. An anterior approach was used and the hip capsule opened anteriorly. The acetabulum was empty and the ligamentum teres ruptured. The femoral head was stuck within the obturator region; inferior to the transverse acetabular ligament. Cuffing of the anterolateral and superior portion of the femoral head was noted. The capsular attachment was torn and buttonholed. The femoral head was reduced into the acetabulum using a bone hook on the neck of the femur. Satisfactory reduction was achieved; several further procedures were also carried out at this visit to theater.
The patient kept immobilized with weight bearing instructions on both hips for 6 weeks and without any skin traction. The patient had IM nailing of the contralateral femur and associated ipsilateral foot fracture treated conservatively. Upon follow-up reviews, the patient is progressing well with no hip pain although weight-bearing status is limited by other injuries sustained. A 3 month follow-up X-ray was satisfactory, and there were no reports of re-dislocation or signs of avascular necrosis of the head.
Discussion
An inferior dislocation is a rare form of hip dislocation. Extensive literature review showed around 15 studies that reported 32 cases related to inferior dislocation of the hip, louxation erecta femoris or infracotyloid hip dislocation. The majority of cases were reported in non-English literature. So far around 12 cases of hip dislocations have been published English literature 6 of them reported by Beauchesne et al. in 1994 followed by 5 cases since then [8].
The age of patients presented with hip dislocations ranging from 10 years old in the Aggarwal series to 72 years old in a Wendel study. The majority of the cases between children and adolescents may be due to lax ligaments. Bartley et al. and Ferguson et al. also reported this condition in adults and young men.
Patients are not always able to recall the exact mechanism of injury. Louxatio erecta femoris is usually caused when the hip joint is flexed to a degree that the distal end of the femur rises above the horizontal plane of the pelvis at the acetabular level. The cases described in English literature were mostly children or teenagers with a few cases of adults who were intoxicated at time of injury [9, 10].
Inferior dislocation of the hip is sub-divided into two main subtypes, dependent on the position of the femur; inferior anterior (obtrator foramen dislocation) which is most common subtype and true inferior dislocation were the head lies below the acetabulum alongside and lateral to the ischial tuberosity, which is less common. In the later, the patient presented with pain and may be seen supporting an acutely flexed thigh that rests against the lower abdomen nearly parallel with the long axis of the body [11, 12, 13].
Inferior hip dislocation can be managed usually with closed reduction under general anesthesia and sufficient sedation. Reduction usually achieved by maintaining traction and gradual knee extension with some internal rotation if needed [1, 13]. Postreduction patients were kept immobilized for 6 weeks followed by partial weight bearing. In one case, there was re-dislocation in 10 months following the initial injury. In the other case, there was traumatic related intertrochanteric fracture treated operatively.
With all types of hip dislocations, there is always a risk of complications which could include avascular necrosis (AVN) in around 10% [14, 15, 16] associated fractures in <40% (as in this case) [15], neurovascular compromise in <25% [14, 17, 18, 19, 20] and articular cartilage injury is reported in about 6% of the cases [17, 20]. Therefore, this kind of injury should be treated as emergency and reduction preformed as soon as possible within 6 h of surgery under sufficient anesthesia and muscle relaxant to reduce chances of AVN [21].
In this 17 years old boy, he was not able to recall the mechanism of injury that led to this hip dislocation (Fig. 1). There were few attempts to reduce his hip in closed fashion but without any luck. His CT scan showed an inferior hip dislocation associated with what looked like small femoral head fracture, which could be the reason of mechanical block that prevented close reduction of hip dislocation (Fig. 2). The patient taken to theatre and hip reduced with open reduction (Fig. 3).
Figure 1.
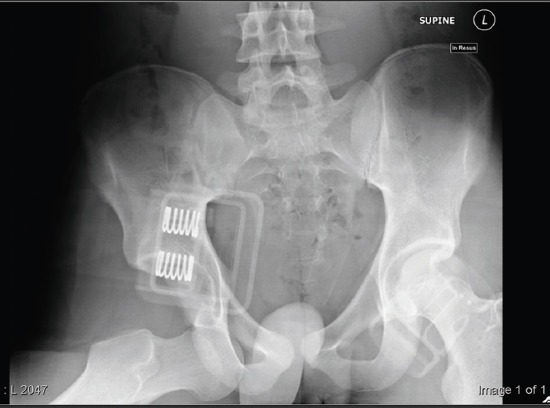
A plain radiograph taken on arrival to the emergency department displaying the inferior dislocation of the hip.
Figure 2.

A computerized tomography image displaying the inferior dislocation of the right hip joint.
Figure 3.

A plain post-operative radiography showing relocation of the femoral head.
In one of the cases, there was intertrochanteric fracture with inferior dislocation that required open reduction and internal fixation [8, 22]. In our case, the patient was treated with 6 weeks immobilization without skin traction Immediate postoperatively and 3 months postoperatively the radiographs of the hip was satisfactory with no signs of AVN (Fig. 4).
Figure 4.
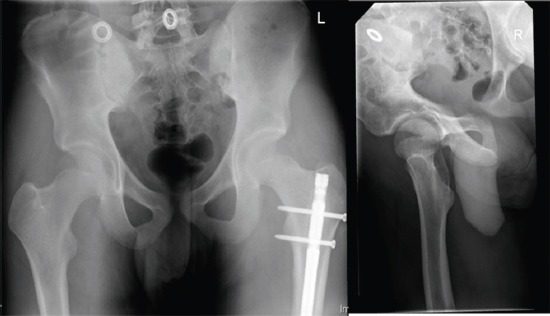
3 month follow-up radiographs.
Conclusion
Inferior hip dislocation is a rare type of hip dislocation and with a small number of cases published in literature. Diagnosis of this injury evident clinically with the position of limb on presentation and later through radiological investigations like X-ray and CT. Usually, this type of dislocation treated with closed reduction under sufficient general anesthesia and muscle relaxant to be performed as soon as possible. If closed reduction is unsuccessful then a fracture could be the cause of the difficulty. If the hip joint is stable post reduction then you may not need 6 weeks of traction. Follow-up is important to monitor any signs of AVN.
Clinical Message.
Inferior hip dislocation is a rare type with small number of cases reported worldwide. Clinical suspension and findings of examination are important in identifying this kind of injuries in addition radiological investigations such as X-ray and CT scans. Failure of close reduction in these cases may raise suspecsion of associated femoral head fractures which will require open reduction to relocate the hip joint.
Biography

Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Abad Rico JI, Barquet A. Luxatio erecta of the hip. A case report and review of the literature. Arch Orthop Trauma Surg. 1982;99(4):277–279. doi: 10.1007/BF00381407. [DOI] [PubMed] [Google Scholar]
- 2.Phillips AM, Konchwalla A. The pathologic features and mechanism of traumatic dislocation of the hip. Clin Orthop Relat Res. 2000;377:7–10. doi: 10.1097/00003086-200008000-00003. [DOI] [PubMed] [Google Scholar]
- 3.Dudkiewicz I, Salai M, Horowitz S, Chechik A. Bilateral asymmetric traumatic dislocation of the hip joints. J Trauma. 2000;49(2):336–338. doi: 10.1097/00005373-200008000-00024. [DOI] [PubMed] [Google Scholar]
- 4.Azar N, Yalçinkaya M, Akman YE, Uzümcügil O, Kabukçuoglu YS. Asymmetric bilateral traumatic dislocation of the hip joint:A case report. Eklem Hastalik Cerrahisi. 2010;21(2):118–121. [PubMed] [Google Scholar]
- 5.Ashraf T, Iraqi AA. Bilateral anterior and posterior traumatic hip dislocation. J Orthop Trauma. 2001;15(5):367–368. doi: 10.1097/00005131-200106000-00012. [DOI] [PubMed] [Google Scholar]
- 6.Hung NN. Traumatic hip dislocation in children. J Pediatr Orthop B. 2012;21(6):542–551. doi: 10.1097/BPB.0b013e328356371b. [DOI] [PubMed] [Google Scholar]
- 7.Avery DM, Carolan GF. Traumatic obturator hip dislocation in a 9-year-old boy. Am J Orthop (Belle Mead NJ) 2013;42(9):E81–E83. [PubMed] [Google Scholar]
- 8.Singh R, Sharma SC, Goel T. Traumatic inferior hip dislocation in an adult with ipsilateral trochanteric fracture. J Orthop Trauma. 2006;20(3):220–222. doi: 10.1097/00005131-200603000-00010. [DOI] [PubMed] [Google Scholar]
- 9.Eddy RJ, Connell DG. Luxatio erecta of the hip. AJR Am J Roentgenol. 1988;151(2):412. doi: 10.2214/ajr.151.2.412-a. [DOI] [PubMed] [Google Scholar]
- 10.Walther MM, McCoin NS. Luxatio erecta of the hip. J Emerg Med. 2013;44(5):985–986. doi: 10.1016/j.jemermed.2012.11.016. [DOI] [PubMed] [Google Scholar]
- 11.Brogdon BG, Woolridge DA. Luxatio erecta of the hip:A critical retrospective. Skeletal Radiol. 1997;26(9):548–552. doi: 10.1007/s002560050284. [DOI] [PubMed] [Google Scholar]
- 12.Kolar MK, Joseph S, McLaren A. Luxatio erecta of the hip. J Bone Joint Surg Br. 2011;93(2):273. doi: 10.1302/0301-620X.93B2.24890. [DOI] [PubMed] [Google Scholar]
- 13.Beauchesne R, Kruse R, Stanton RP. Inferior dislocation (luxatio erecta) of the hip. Orthopedics. 1994;17(1):72–74. doi: 10.3928/0147-7447-19940101-14. [DOI] [PubMed] [Google Scholar]
- 14.Herrera-Soto JA, Price CT. Traumatic hip dislocations in children and adolescents:Pitfalls and complications. J Am Acad Orthop Surg. 2009;17(1):15–21. doi: 10.5435/00124635-200901000-00003. [DOI] [PubMed] [Google Scholar]
- 15.Mehlman CT, Hubbard GW, Crawford AH, Roy DR, Wall EJ. Traumatic hip dislocation in children. Long-term followup of 42 patients. Clin Orthop Relat Res. 2000;376:68–79. [PubMed] [Google Scholar]
- 16.Nötzli HP, Siebenrock KA, Hempfing A, Ramseier LE, Ganz R. Perfusion of the femoral head during surgical dislocation of the hip. Monitoring by laser Doppler flowmetry. J Bone Joint Surg Br. 2002;84(2):300–304. doi: 10.1302/0301-620x.84b2.12146. [DOI] [PubMed] [Google Scholar]
- 17.Schlonsky J, Miller PR. Traumatic hip dislocations in children. J Bone Joint Surg Am. 1973;55(5):1057–1063. [PubMed] [Google Scholar]
- 18.Epstein HC. Traumatic dislocations of the hip. Clin Orthop Relat Res. 1973;92:116–142. doi: 10.1097/00003086-197305000-00011. [DOI] [PubMed] [Google Scholar]
- 19.Offierski CM. Traumatic dislocation of the hip in children. J Bone Joint Surg Br. 1981;63:194–197. doi: 10.1302/0301-620X.63B2.7217141. [DOI] [PubMed] [Google Scholar]
- 20.Hougaard K, Thomsen PB. Traumatic hip dislocation in children. Follow up of 13 cases. Orthopedics. 1989;12(2):375–378. doi: 10.3928/0147-7447-19890301-07. [DOI] [PubMed] [Google Scholar]
- 21.Rockwood CA, Beaty JH, Kasser JR. Rockwood and Wilkins’; In: Beaty JH, Kasser JR, Skaggs DL, Flynn JM, Waters PM, editors. Fractures in Children. 7th ed. Philadelphia, PA, London: Lippincott Williams & Wilkins; 2010. [Google Scholar]
- 22.Aggarwal S, Kumar V, Bhagwat KR, Shashikanth VS, Ravikumar HS. Inferior dislocation of the hip:A case series and literature review. Chin J Traumatol. 2012;15(5):317–320. [PubMed] [Google Scholar]