

Abstract
Introduction:
Large size bone tumors are rare as patients present quite early. The current article reports a large chondrosarcoma removed from left humerus. The rarity of such large size tumors is focus of the report.
Case Report:
Forty year old male presented with a huge mass in this left arm. The same patient apparently was admitted three years back for excision of the arm swelling which was relatively small that time. However the patient did not undergo surgery and was takin treatment from local bone setters during the last three years and tumor grew to a larger size during this period. The current dimensions of tumor was 32x28 cms with circumference of 87 cms. X-ray showed complete destruction of the upper humerus with central calcification. Biopsy releveled a chondrosarcoma. Skeletal survey and bone scan did not reveal any other lesion in the body. A forequarter amputation was done and a 16 kg tumor mass was excised. At three years follow up, the patient has no complains with no recurrence of the tumor.
Conclusion:
Large musculoskeletal tumors are rare and probable reason for such late presentation in our case is ignorance and cultural beliefs. Patients should be properly counselled on first presentations regarding management and prognosis
Keywords: megatumor, chondrosarcoma, delayed presentation
What to Learn from this Article?
Large size musculoskeletal tumors are unusual and may present due to delayed presentation of patient as they waste time with quacks and bone setters.
Introduction
Large Musculoskeletal tumors are not a rarity, but it is very unusual to see mega-tumors of more than 10 kg. in weight, because patients usually come for the treatment before such size is reached. Guinness World Record for the Largest Tumor belongs to India. The documentation is 16.5 Kg. bone tumor removed from the right thigh of a 35 Yrs. male at Himalyan Institute of Medical Sciences, Dehradoon on 10/3/2002 [1]. The Tumor was 45Cms. long & 30Cms. wide. Such Tumors cause lot of discomfort to the patient and are likely to have metastatic deposits in the body. We are reporting successful removal of an equally large tumor from the upper limb of a patient
Case Report
A 40-yrs-old male came to the orthopaedic OPD holding his left arm with the right one and the arm and shoulder were covered with a cloth. When the cloth was removed, there showed a shockingly huge mass in the left arm and shoulder with veins prominent all over it and a small wound over its posterior aspect. The tumour was pressing into the chest wall on the left side, but without causing any dyspnoea. Vascular status was normal distal to the tumour mass, but there was complete motor deficit with no power in muscles on forearm and hand. On taking history, it was found that, patient had come 3 yrs. Back with a small swelling in left upper arm and was admitted for the excision of the mass, but the patient absconded due to fear of surgery and started receiving treatment from some bone setters. Present situation developed over a period of 3 years. Patent came back to the hospital as he could no longer manage with the tumor due to the large size and weight of the growth and also due to social queries directed at his condition.
On measurement, tumour was 32 cms long, 28Cms wide and the circumference was 87Cms (Fig. 1). X-Ray of the area showed complete destruction of upper half of the humerus with central calcification of the tumour mass (Fig 2). CT Angiography showed extensive destruction of the osseous tissue with calcification and there appeared involvement of lateral aspect of scapula also (Fig 3). Blood flow in major vessels was normal without undue hyper vascularity in the tumour area & the tumour mass was pushing the thoracic cage inwards. A radiographic skeletal survey and bone scan did not reveal any other lesion. Biopsy of the tumour mass confirmed the diagnosis of Chondrosarcoma. It was decided to get rid of the bulky mass from the body, so as to make the patient comfortable and to clear the surrounding area of any suspected tumour mass. Forequarter amputation with adequate margins was performed.
Figure 1.

a- 40 year old man presented with huge swelling in left upper arm and shoulder measuring 28 cms across (b), 32 cms vertical (c) and 87 cms circumference (d)
Figure 2.
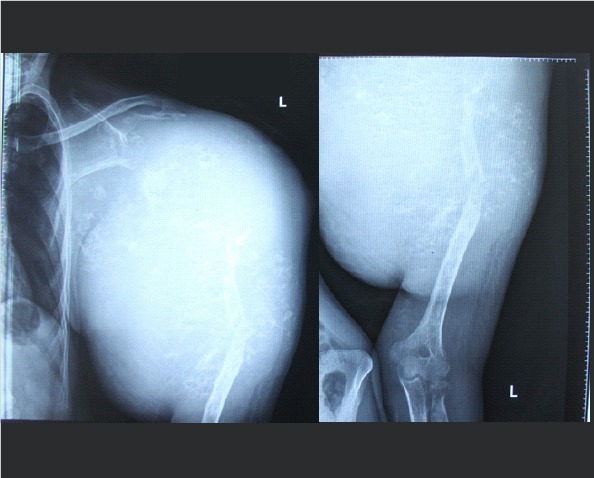
X-Ray of the area showed complete destruction of upper half of the humerus with central calcification of the tumour mass.
Figure 3.

CT Angiography showed extensive destruction of the osseous tissue with calcification & there appeared involvement of lateral aspect of scapula also. Blood flow in major vessels was normal without undue hyper vascularity in the tumour area & the tumour mass was pushing the thoracic cage inwards.
Surgical Procedure (Fig 4): The patient was placed in a right lateral decubitus position to expose the thorax with the left upper extremity free. Anterior approach was used. An elliptical incision was made with the superior apex over the clavicle on one end and inferior apex was made at the mid axillary line and continued posterio superiorly over the scapula to join the superior apex. The clavicle was divided at the proximal third and carefully elevated to expose the subclavian artery, vein and brachial plexus (Fig 4a,b). The subclavian artery was ligated and cut first, then the subclavian vein was tied. Branches of the brachial plexus were divided proximally. Next, the chest wall attachments of the pectoralis major and minor were divided. Posteriorly, fasciocutaneous skin flaps were developed and all periscapular muscles were released (Fig 4c). This allowed the shoulder girdle to be freed and the whole extremity to fall away from the trunk along with the scapula (Fig 4d). The anterior and posterior skin flaps were used to close the defect primarily over a corrugated drain Fig 4 e). Cautery was used extensively for cutting and patient required two blood transfusions. Removed limb weighed 16 Kgs along with the tumor (Fig 4f) At three years follow up the patient had no complains and had rejoined his work at a government office (Fig 5)
Figure 4.

a - Osteotomy of the Clavicle. B - Identification of the Major Neuro-vascular Bundle and ligation. C- Soft tissue dissection. D- disarticulation of the limb with scapula. Ewound sutured over drain. F- Disarticulated Limb with Tumour.
Figure 5.

Three years after surgery, patient is healthy and working in the Govt. set up, as before.
Discussion
Although this case report is presented to report the large size of the tumor that was extracted, this is not the main point of discussion. Large size tumors are not unusual but not many reports describe them as size of the tumor does not really add much to the literature. The point to be highlighted here is one of more subjective topic related to patients perceptions and their decision making specially in such cases like tumors. Poverty and Ignorance in any society is the biggest bane for the humanity. If this patient had not absconded on his first admission, limb sparing surgery would have been very successful. Patient probably would have had his left limb which was functional. Also the risk of developing a metastasis due to prolonged waiting was real and it was very fortunate for the patient that he did not develop such complications. It is due to many social and cultural factors that patients continue to visit such bone setters and quacks [2]. Also there are other political reasons for unhindered growth of such practices [3]. The menace of bone setters in the developing countries must be tackled properly to save many such sufferers. There is also a need to create awareness among the society
Unusual size and weight of tumour in itself is a reason to present it to the orthopaedic fraternity. It is also stressed that despite the mega size and malignancy, tumour can remain localised, without metastasis.Management in this case was dictated by the size of the tumor, no metastasis and complete neuromuscular paralysis distal to the tumor. The limb was anyways not functional and a forequarter amputation with extended margins saved the life of the patient and made him comfortable too.
Conclusion
The case is being presented to highlight the ignorance of many sections of the society towards the proper treatment needs to such problems and for awareness to curb the menace of unqualified quacks in the society.
What to learn for the case: Large size musculoskeletal tumors are unusual and may present due to delayed presentation of patient as they waste time with quacks and bone setters.
Biography


Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.world-records/largest-bone-3.Pulla P. Are India’s quacks the answer to its shortage of doctors? [tumour accessed on 14th Sep 2016 Jan];BMJ. 2016 21:352–291. doi: 10.1136/bmj.i291. http:www.guinnessworldrecords.com/. [DOI] [PubMed] [Google Scholar]
- 2.Sharma R. Flowerpot sequestrum of the Humerus Neglect for 10 years. J Orthop Case Rep. 2012 Oct-Dec;2(4):32–4. [PMC free article] [PubMed] [Google Scholar]
- 3.Pulla P. Are India’s quacks the answer to its shortage of doctors? BMJ. 2016 Jan 21;352:291. doi: 10.1136/bmj.i291. [DOI] [PubMed] [Google Scholar]