

Abstract
Postoperative atrial fibrillation (POAF) is a frequent complication of cardiac surgery, which results in increased morbidity, mortality, length of stay, and hospital costs. We developed and followed a process map to implement a protocol to decrease POAF: (1) identify stakeholders and form a working committee, (2) formal literature and guideline review, (3) retrospective analysis of current institutional data, (4) data modeling to determine expected effects of change, (4) protocol development and implementation into the electronic medical record, and (5) ongoing review of data and protocol adjustment. Retrospective analysis demonstrated that POAF occurred in 29.8% of all cardiovascular surgery cases. Median length of stay was 2 days longer (P<0.001), and median total variable costs $2495 higher (P<0.001) in POAF patients. Modeling predicted that up to 60 cases of POAF and >$200 000 annually could be saved. A clinically based electronic medical record tool was implemented into the electronic medical record to aid preoperative clinic providers in identifying patients eligible for prophylactic amiodarone. Initial results during the 9-month period after implementation demonstrated a reduction in POAF in patients using the protocol, compared with those who qualified but did not receive amiodarone and those not evaluated (11.1% versus 38.7% and 38.8%; P=0.022); however, only 17.3% of patients used the protocol. A standardized methodological approach to quality improvement and electronic medical record integration has potential to significantly decrease the incidence of POAF, length of stay, and total variable cost in patients undergoing elective coronary artery bypass graft and valve surgeries. This framework for quality improvement interventions may be adapted to similar clinical problems beyond POAF.
Keywords: amiodarone, atrial fibrillation, coronary artery bypass, electronic medical record, quality improvement
Goals and Vision of the Program
Complications can occur after nearly all types of cardiovascular intervention. The key to adequately addressing and preventing these adverse events lays in a methodological approach to focused quality improvement projects. As the population ages, the number of cardiac surgeries performed annually is predicted to grow.1 As such, practitioners will find themselves faced more frequently with complications, including postoperative atrial fibrillation (POAF), which is among the most prevalent. Estimates indicate that nearly one third of all coronary artery bypass graft (CABG) patients will experience POAF, with that number climbing to 40% for valvular procedures and ≤50% when these procedures are combined.2,3 POAF is associated with increased morbidity and mortality up to a year after surgery4,5 and an increase in the length of stay (LOS), leading to >$10 000 in additional hospital cost.6 Given both the magnitude and importance of these clinical outcomes, it is a desirable goal to prevent the development of POAF.
Patients at highest risk for POAF include those aged >70 years with left atrial enlargement and hypertension.7 Previous studies have demonstrated that directed medical therapy, particularly with β-blockers and amiodarone, may reduce the burden of POAF in this population, with subsequent improvement in adverse clinical outcomes including death.8–10 Among the most influential of these studies is the PAPABEAR trial (Prophylactic Oral Amiodarone for the Prevention of Arrhythmias that Begin Early After Revascularization, Valve Replacement, or Repair), which demonstrated that amiodarone, prescribed prophylactically to those undergoing planned cardiac surgery, reduced POAF by >45%. This study provided support for prophylactic amiodarone use being labeled an American College of Cardiology Foundation/American Heart Association guideline IIa recommendation, level of evidence A, in the prevention of POAF.10,11
The increased availability of electronic medical records (EMR) has stimulated interest and excitement on its use for quality and research. The purpose of this study was to use prevention of POAF as a case study in the development of a quality improvement process, using the EMR. We will use this process to (1) determine the incidence of POAF in a large, multihospital system including 3 distinct cardiovascular surgery programs, (2) model changes in clinical and financial outcomes based on POAF prevention, (3) develop institution-wide guidelines aimed at decreasing the incidence of POAF in post–cardiac surgery patients, and (4) report initial utilization and clinical results after implementation of the institutional guidelines.
Local Challenges in Implementation
Although some challenges are specific to certain projects or populations, most barriers to change can be categorized into 3 broad categories: (1) design and planning of improvement interventions, (2) organizational and institutional contexts, and (3) sustainability and spread.12 In most situations, initial efforts focus on the first 2 domains, with the understanding that early planning will allow sustainability to be addressed more easily in the future.
Specific to the issue of POAF at our institution, individual providers needed to understand the local magnitude of POAF to become invested in addressing the issue (organizational and institutional contexts). Furthermore, given the vast and varied literature on the topic, large variation in practice existed between providers (design and planning domain). Fortunately, the integrated EMR offered a tool, which could be leveraged during the project to reduce POAF rates (sustainability and spread domain).
Setting
To fully grasp the local challenges (and opportunities for improvement), it is essential to understand the local setting. Allina Health System is one of the largest healthcare delivery systems in the upper Midwest, including 11 hospitals, 82 clinics, and 3 ambulatory care centers. This includes 3 independent cardiovascular surgery programs at Abbott Northwestern in Minneapolis, United Hospital in St. Paul, and Mercy Hospital in Coon Rapids, Minnesota. These institutions and their clinics share a common, integrated EMR. Although the presented study specifically focuses on inpatient, postoperative outcomes, preventative therapy necessitates identification and management of patients at high risk for POAF in the outpatient setting.
Design of the Initiative
To address the issues of recognition by stakeholders and variations in current practice, a committee of individuals most involved in the care of POAF patients was assembled. This stakeholder committee consisted of cardiologists (noninvasive and electrophysiologists), cardiothoracic surgeons, and nursing and administrative staff and was primarily tasked with reducing the POAF rate. The target patient population was all patients undergoing elective CABG, aortic valve or mitral valve surgery without a previous history of atrial fibrillation.
The first barrier to change involved informing providers of the magnitude of the problem. To this end, the committee completed a retrospective analysis of institutional data, highlighting the clinical and economic impact of POAF annually. To address the issue of clinical practice variation, the committee completed a guideline and literature review of current methods for the prevention of POAF. On the basis of these findings, the committee selected a prophylactic strategy and then modeled expected changes in outcomes based on their retrospective analysis and selected prophylactic strategy. Subsequently, they developed institutional guidelines for preoperative evaluation and prevention measures for POAF based on their literature review and modeling. This process was submitted to and approved by the institutional review board.
Retrospective Analysis and Magnitude of POAF
Using Allina’s integrated EMR, a retrospective analysis of all patients undergoing CABG, with or without valve surgery, isolated mitral valve surgery, and isolated aortic valve surgery from January 2009 through December 2011, was performed to assess overall incidence of POAF, LOS, and total variable cost. These patients were divided into elective, urgent, and emergent cases based on definitions used in the Society of Thoracic Surgeons Adult Cardiac Surgery Database.13 A subgroup analysis of the elective patients in each group was subsequently performed to evaluate the same prespecified outcomes.
From January 2009 through December 2011, 2517 CABG, isolated mitral, and isolated aortic valve surgeries were performed at 3 different hospitals within the Allina Network. Of the observed surgeries, 1297 (51.5%) were elective, 1067 (42.4%) were urgent, and 153 (6.1%) were emergent. The composite incidence of POAF for all cases was 29.8%, similar to the 30.2% in elective cases, slightly lower with CABG, and slightly higher in valve surgeries (Figure 1).
Figure 1.
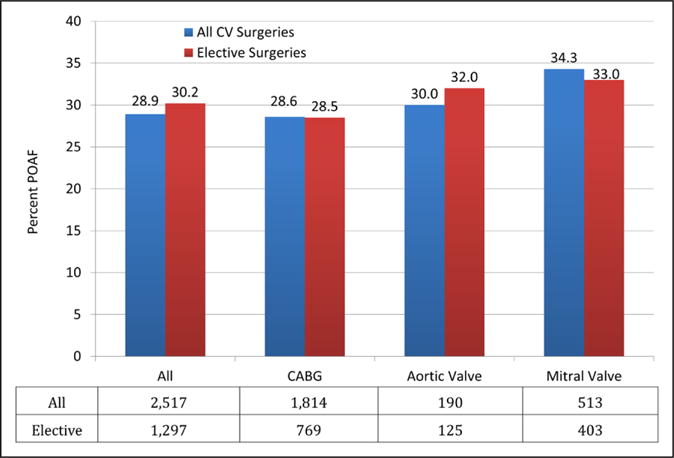
Retrospective analysis of incidence of postoperative atrial fibrillation (POAF) across surgery type, stratified by all cases (elective, urgent, and emergent) and elective cases alone. CABG indicates coronary artery bypass graft; and CV, cardiovascular.
Subgroup analysis of the elective cases demonstrated that the median LOS for all patients who developed POAF was 7 days compared with 5 days in those who did not develop POAF (P<0.001; Figure 2A). Assessment of total variable cost demonstrated that the median cost for all elective cases in which the patient developed POAF was $18 370 compared with $15 875 for those who did not develop POAF (P<0.001; Figure 2B).
Figure 2.
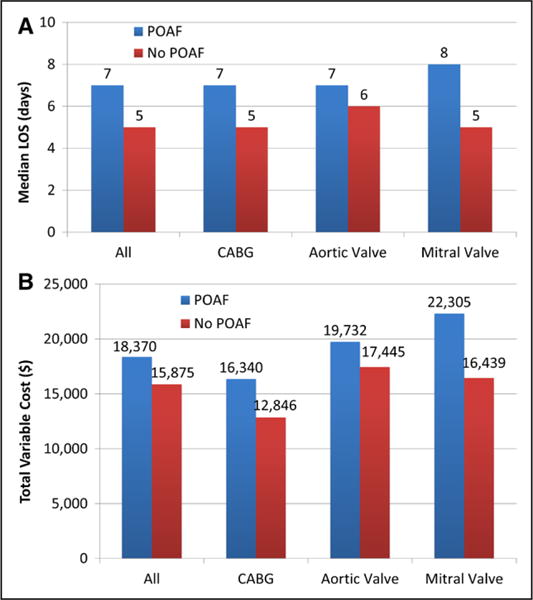
Retrospective analysis of length of stay (LOS) (A) and total variable cost (B) of elective surgical cases, stratified by type of surgery. CABG indicates coronary artery bypass graft; and POAF, postoperative atrial fibrillation.
Guideline and Literature Review
The Stakeholder Committee initiated a literature and guideline review to determine appropriate interventions for the prevention of POAF. The 2011 American College of Cardiology Foundation/American Heart Association Guidelines for patients undergoing CABG list preoperative β-blockers as a class I and preoperative amiodarone as a class IIa recommendation for the prevention of postoperative dysrhythmias.14 β-Blocker therapy is the most studied of the pharmacological methods to reduce POAF but also has the largest heterogeneity between studies. Sotalol has demonstrated efficacy in reducing POAF; however, it has also been shown to have higher rates of hypotension and bradyarrhythmias.15 A class III antiarrhythmic, amiodarone had the advantage of more consistent data, ease of administration, and overall tolerability. Therefore, the consensus committee chose amiodarone as the recommended agent to prevent POAF.9,10,15 The committee completed a retrospective analysis, from which modeling was performed of the expected effects of prophylactic amiodarone therapy on our cardiac surgery patients based on the results of the PAPABEAR trial.10
Of note, literature on various other preventative measures, including calcium channel blockers, magnesium, and overdrive pacing, was reviewed; however, given the relative lack of evidence to support their use, they were not included in the committee’s recommendations.
Given the results of the retrospective analysis, the committee made the recommendation to pursue modeling of prophylactic treatment with Amiodarone.
Modeling
On the basis of the determined incidence of POAF, LOS, and total variable costs in the Allina system, modeling was performed to determine the expected changes to each variable based on obtaining similar reductions with the use of prophylactic amiodarone, as seen in the PAPABEAR trial.
Modeling was performed based on the data for elective cases, as these are most amenable to prophylactic intervention. Using Allina’s observed 30.2% overall incidence of POAF for elective cases, we calculated the number of fewer POAF cases we would expect annually based on achieving 50% or 100% of the rate reduction in POAF documented in the PAPABEAR trial, equating to 22.7% and 45.4% rate reductions, respectively. Given the large range between these values, 3 further models were completed at intermittent values. These 5 cost-savings prediction models were used to estimate the overall reduction in LOS and total variable costs annually that would be achieved if their respective rate reductions in incidence of POAF were met. For each model, we first calculated the number of fewer POAF cases that we would expect annually in elective cardiovascular surgery patients. On the basis of the number of fewer POAF cases predicted in each model, we used the difference in median LOS and total variable cost between POAF cases and non-POAF cases to calculate the expected savings we would achieve in overall LOS and total variable costs annually compared with baseline. The estimated reductions in annual POAF cases, hospital days, and total variable costs based on these models are shown in Table.
Table.
Modeling Scenarios of Expected Reductions in Number of Patients Who Experience POAF, Hospitalization Costs, and Hospital Days, Based on Varying Levels of Achievement of the PAPABEAR Trial Outcomes
| Incidence of POAF | Number of Fewer POAF Patients (Annual) | Hospitalization Cost Savings (Annual) | Number of Fewer Hospital Days (Annual) | |
|---|---|---|---|---|
| Current scenario | 30.2% | 0 | $0 | 0 |
| Scenario 1 | 25.0% | 23 | $86 891 | 42.3 |
| Scenario 2 | 24.0% | 27 | $102 002 | 49.7 |
| Scenario 3 (50% of PAPABEAR reduction rate) | 23.3% | 30 | $113 336 | 55.2 |
| Scenario 4 | 18.2% | 52 | $196 449 | 95.7 |
| Scenario 5 (100% of PAPABEAR reduction rate) | 16.5% | 60 | $226 672 | 110.4 |
PAPABEAR indicates Prophylactic Oral Amiodarone for the Prevention of Arrhythmias that Begin Early After Revascularization, Valve Replacement, or Repair; and POAF, postoperative atrial fibrillation.
Implementation of the Initiative
Modeling Data Review and Protocol Development
Modeling data were reviewed by the Stakeholder Committee, who determined that this intervention would accomplish the goal of reducing the rate of POAF. Recognizing the integrated EMR as an enabler of change, the committee recommended development of an EMR-based decision support tool. Because the PAPABEAR trial required a preoperative visit, the committee recommended that all patients undergoing elective cardiac surgery must have a preoperative visit, during which the EMR-based, real-time decision support tool would prompt providers to prescribe amiodarone in patients without the prespecified exclusion criteria. Exclusion criteria were identical to the PAPABEAR trial, including patients with myocardial infarction within the preceding 2 weeks, any rhythm other than sinus, New York Heart Association class IV heart failure symptoms, persistent hypotension (systolic blood pressure <80 mm Hg), sinus bradycardia (<50 bpm), PR interval >220 ms, second- or third-degree atrioventricular block, history of sustained atrial tachyarrhythmias, corrected QT interval >480 ms, interstitial pulmonary disease, or clinical hypothyroidism. β-Blocker therapy was continued if already prescribed.
Protocol Launch
Although the protocol was developed for all 3 cardiovascular hospitals in the Allina System, the Stakeholder Committee decided it should be piloted at a single institution first, to ensure feasible integration into the workflow. As such, this protocol was integrated into the EMR and implemented at Abbott Northwestern Hospital in April 2013. On completion of the EMR-based support tool during the preoperative visit, if no contraindications were noted, the provider was prompted to prescribe prophylactic amiodarone therapy, consisting of 10 mg/kg/d, divided into 2 daily doses, for a total of 6 days before and 6 days after surgery, the same as in the PAPABEAR trial.10
Statistical Analysis
Descriptive statistics are displayed as medians and 25th and 75th percentiles for continuous variables; number and percentage with characteristic are given for categorical variables. Categorical variables were analyzed using Pearson χ2 or Fisher exact tests. Continuous variables were analyzed using ANOVA for normally distributed variables or Kruskal–Wallis tests for continuous variables with non-normal distribution. A value of P<0.05 was considered significant, and P values are 2 sided where possible. Given the goal of the study was simply to decrease the overall rate of POAF during the index admission, time-to-event analyses were not performed. All statistical calculations and plots were performed with Stata 14.1 (StataCorp LP, College Station, TX).
Success of the Initiative
The first 9 months of data (April 2013 through December 2013) were reviewed to assess efficacy. During this time period, there were 156 elective cardiac surgery cases, of which 27 patients (17.3%) received standardized preoperative evaluation and qualified for prophylactic amiodarone, 80 (51.3%) received preoperative evaluation without amiodarone and 49 (31.4%) had no preoperative evaluation or amiodarone. Preoperatively evaluated patients who received amiodarone had lower rates of POAF (11.1% versus 38.7% and 38.8%; P=0.022) and any complication (22.2% versus 51.3% and 49.0%; P=0.027) when compared with patients who had preoperative evaluation and received no amiodarone or those without any preoperative evaluation (Figure 3). Complications other than POAF are listed in Table I in the Data Supplement. Assessment of prophylactic amiodarone therapy compliance and development of postdischarge POAF fell outside of the scope of the study and was not obtained. Given the reductions in the POAF rates, the protocol was expanded to all 3 hospitals in the Allina system.
Figure 3.
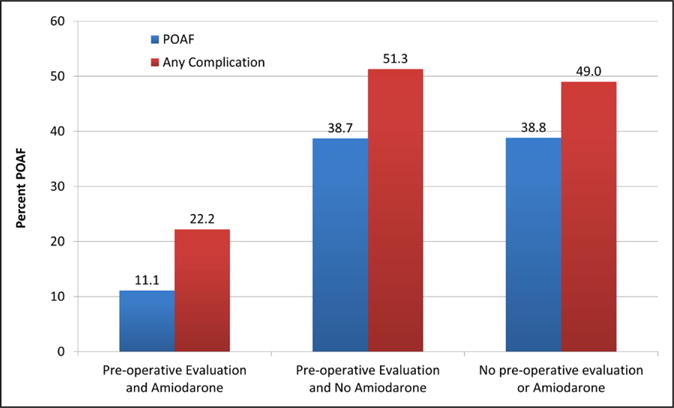
Prospective analysis of the incidence of postoperative atrial fibrillation (POAF) and any complication of all 156 elective cardiovascular surgery cases during the first 9 mo after implementation of the POAF prevention provider support tool, stratified by adherence to the protocol.
Summary of the Experience, Future Directions, and Challenges
We describe a quality improvement protocol that may be adapted to multiple cardiovascular conditions, using POAF prevention as a case study. To address the challenge of a lack of provider understanding of the problem, a retrospective analysis of the rate of POAF in those undergoing CABG or valvular surgery at our large-volume cardiac centers was performed. Although the results were similar to previously reported rates in the literature,2 the local institutional results provided tangible evidence for the need to focus on POAF.
Next, guideline and literature review on POAF prevention strategies allowed for modeling based on expected rate of reductions in POAF with a standardized protocol of prophylactic amiodarone. The potential reductions in POAF, in LOS, and in total variable cost led to the development and implementation of a standardized protocol in April 2013, with preliminary data showing significant reductions in POAF in on-protocol patients.
One of the most influential components of the study for stakeholders was the modeling findings. According to the above models, if outcomes reach only 50% of those achieved in the PAPABEAR trial, 30 fewer cardiac surgery patients will develop POAF, saving an estimated 55 hospital days and >$113 000 annually. Similarly, if the PAPABEAR outcomes are reproduced with a 45.4% reduction in POAF, 60 fewer patients would develop POAF, resulting in 110 fewer hospital days, saving nearly a quarter of a million dollars annually. Although these numbers are modest on an institutional level, extrapolation to the healthcare system as a whole has implications to save far more hospital days and dollars nationwide. Although not specifically addressed in this study, given the known risks of stroke, heart failure, and 30-day mortality associated with POAF,7,10 there is an expected reduction in morbidity and mortality. The ongoing prospective analysis of the effect of this protocol will allow for determination of changes in morbidity, mortality, LOS, and cost, as well as in unintended consequences such as complications of amiodarone.
Recognition of the possible improvements seen in the models led Allina to integrate the consensus committee’s recommendations into a physician support tool in the system-wide EMR. This allows for a prospective analysis of the effect on POAF rates, LOS, and cost, as well as the complication rates associated with POAF. Our preliminary data demonstrate that patients who underwent presurgical evaluation and were started on amiodarone were less likely to develop any postsurgical complication, specifically including POAF. Unfortunately, only 17% of elective surgical patients had a preoperative clinic visit and met all inclusion criteria. This illustrates 2 important aspects of the process: ongoing evaluation of the project success and subsequent protocol adjustment to improve the process (Figure 4).
Figure 4.
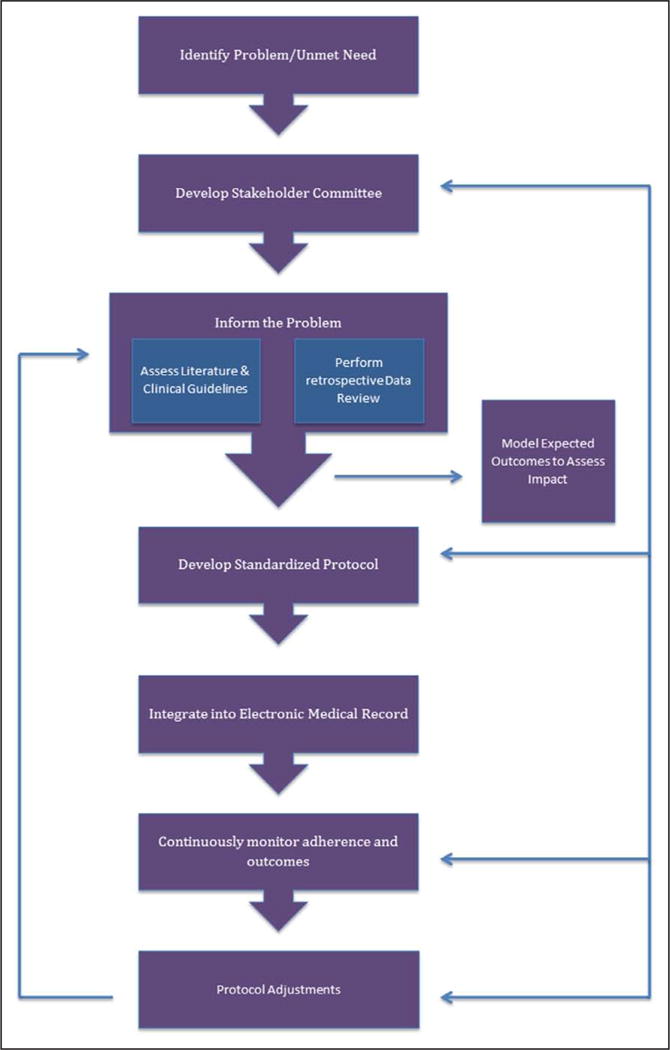
Roadmap for the development of a quality improvement project using the electronic medical record.
From an outcomes perspective, these data demonstrate that the implementation of a protocol to prophylactically treat cardiovascular surgery patients with amiodarone decreases the rate of POAF. Although many hurdles were overcome, this process also illustrates other challenges that exist in the implementation of such protocols in a large, diverse health-care system, and further research is required to understand and address them systematically. Specifically, in this study, over half of patients with clinic visits did not receive POAF prophylaxis, whereas nearly one third did not have a preoperative clinic visit at all. Further research is required to determine whether the reason was a specific exclusion criteria for amiodarone, patient preference, or provider nonadherence to the protocol. Suboptimal utilization of new protocols, especially across multiple care organizations as was done in this study, is a known challenge in implementation research.16 Implementation requires education across multiple systems with 3 large cardiology groups and 3 cardiovascular surgery groups with a larger number of physicians and midlevel providers. The EMR-based tool will allow for continued evaluation of adherence and education of providers about the achievable reductions in POAF, which have already been demonstrated, to help boost adherence. This information is continually reviewed by the Stakeholder Committee, after which changes may be made. This process is currently ongoing at our institution.
Another challenge specific to this case study is to use the EMR to expand the patient population to include patients without preoperative clinic visits, those with exclusion criteria, or those who undergo urgent or emergent surgery. Thus, to identify candidates for future novel approaches to prevention of POAF. Data from the EMR will aid the previously formed multidisciplinary committee in enhancing the protocol to address the needs of patients not eligible for amiodarone or those unable to attend a preoperative clinic visit. Of note, the committee also developed a standardized protocol for the treatment of patients who develop POAF, with the ultimate goal being to prevent as many cases of POAF as possible and to quickly treat it when it does develop to reduce the total burden of morbidity and mortality related to POAF.
As the importance of standardized approaches to developing and implementing sustainable systems in healthcare becomes more widely recognized, a growing number of proposed models have been developed.17 We propose the protocol described in this case study as a roadmap for the use of EMRs in implementation science research (Figure 4).
As healthcare costs continue to grow, the importance of using data and guidelines to improve quality and decrease cost becomes ever more vital. This study demonstrates how collaborative effort can identify easy targets for intervention, develop plans to combat them, and model the expected outcomes. It also demonstrates the power of the EMR in facilitating these analyses and implementing recommended guidelines into current systems of care. Future studies are required to confirm these findings and further explore the ability of the EMR to facilitate implementation and analysis.
Supplementary Material
Footnotes
Disclosures
None.
References
- 1.David Etzioni VAS. The epidemiology and economics of cardiothoracic surgery in the elderly. In: Katlic MR, editor. Cardiothoracic Surgery in the Elderly. New York: Springer-Verlag; 2011. [Google Scholar]
- 2.Alqahtani AA. Atrial fibrillation post cardiac surgery trends toward management. Heart Views. 2010;11:57–63. doi: 10.4103/1995-705X.73212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Raiten J, Patel PA, Gutsche J. Management of postoperative atrial fibrillation in cardiac surgery patients. Semin Cardiothorac Vasc Anesth. 2015;19:122–129. doi: 10.1177/1089253214551283. [DOI] [PubMed] [Google Scholar]
- 4.Philip F, Becker M, Galla J, Blackstone E, Kapadia SR. Transient postoperative atrial fibrillation predicts short and long term adverse events following CABG. Cardiovasc Diagn Ther. 2014;4:365–372. doi: 10.3978/j.issn.2223-3652.2014.09.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lee SH, Kang DR, Uhm JS, Shim J, Sung JH, Kim JY, Pak HN, Lee MH, Joung B. New-onset atrial fibrillation predicts long-term newly developed atrial fibrillation after coronary artery bypass graft. Am Heart J. 2014;167:593–600.e1. doi: 10.1016/j.ahj.2013.12.010. [DOI] [PubMed] [Google Scholar]
- 6.Aranki SF, Shaw DP, Adams DH, Rizzo RJ, Couper GS, VanderVliet M, Collins JJ, Jr, Cohn LH, Burstin HR. Predictors of atrial fibrillation after coronary artery surgery. Current trends and impact on hospital resources. Circulation. 1996;94:390–397. doi: 10.1161/01.cir.94.3.390. [DOI] [PubMed] [Google Scholar]
- 7.Omae T, Kanmura Y. Management of postoperative atrial fibrillation. J Anesth. 2012;26:429–437. doi: 10.1007/s00540-012-1330-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mitchell LB. Prophylactic therapy to prevent atrial arrhythmia after cardiac surgery. Curr Opin Cardiol. 2007;22:18–24. doi: 10.1097/HCO.0b013e3280117cc5. [DOI] [PubMed] [Google Scholar]
- 9.Bagshaw SM, Galbraith PD, Mitchell LB, Sauve R, Exner DV, Ghali WA. Prophylactic amiodarone for prevention of atrial fibrillation after cardiac surgery: a meta-analysis. Ann Thorac Surg. 2006;82:1927–1937. doi: 10.1016/j.athoracsur.2006.06.032. [DOI] [PubMed] [Google Scholar]
- 10.Mitchell LB, Exner DV, Wyse DG, Connolly CJ, Prystai GD, Bayes AJ, Kidd WT, Kieser T, Burgess JJ, Ferland A, MacAdams CL, Maitland A. Prophylactic oral amiodarone for the prevention of arrhythmias that begin early after revascularization, valve replacement, or repair: PAPABEAR: a randomized controlled trial. JAMA. 2005;294:3093–3100. doi: 10.1001/jama.294.24.3093. [DOI] [PubMed] [Google Scholar]
- 11.January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW, ACC/AHA Task Force Members 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–2104. doi: 10.1161/CIR.0000000000000040. [DOI] [PubMed] [Google Scholar]
- 12.Dixon-Woods M, McNicol S, Martin G. Ten challenges in improving quality in healthcare: lessons from the Health Foundation’s programme evaluations and relevant literature. BMJ Qual Saf. 2012;21:876–884. doi: 10.1136/bmjqs-2011-000760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jacobs JP, Shahian DM, Prager RL, Edwards FH, McDonald D, Han JM, D’Agostino RS, Jacobs ML, Kozower BD, Badhwar V, Thourani VH, Gaissert HA, Fernandez FG, Wright C, Fann JI, Paone G, Sanchez JA, Cleveland JC, Jr, Brennan JM, Dokholyan RS, O’Brien SM, Peterson ED, Grover FL, Patterson GA. Introduction to the STS National Database Series: outcomes analysis, quality improvement, and patient safety. Ann Thorac Surg. 2015;100:1992–2000. doi: 10.1016/j.athoracsur.2015.10.060. [DOI] [PubMed] [Google Scholar]
- 14.Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, Cigarroa JE, Disesa VJ, Hiratzka LF, Hutter AM, Jr, Jessen ME, Keeley EC, Lahey SJ, Lange RA, London MJ, Mack MJ, Patel MR, Puskas JD, Sabik JF, Selnes O, Shahian DM, Trost JC, Winniford MD. 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124:2610–2642. doi: 10.1161/CIR.0b013e31823b5fee. [DOI] [PubMed] [Google Scholar]
- 15.Burgess DC, Kilborn MJ, Keech AC. Interventions for prevention of postoperative atrial fibrillation and its complications after cardiac surgery: a meta-analysis. Eur Heart J. 2006;27:2846–2857. doi: 10.1093/eurheartj/ehl272. [DOI] [PubMed] [Google Scholar]
- 16.Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, Griffey R, Hensley M. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38:65–76. doi: 10.1007/s10488-010-0319-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ward V, House A, Hamer S. Developing a framework for transferring knowledge into action: a thematic analysis of the literature. J Health Serv Res Policy. 2009;14:156–164. doi: 10.1258/jhsrp.2009.008120. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.