

Abstract
Background:
A prothrombotic state is associated with the presence and severity of organ damage in hypertensive patients. In these patients, evidence of subclinical carotid functional changes anticipates major cardiovascular events. The aim of this study was to investigate the association of hemostatic markers with carotid artery stiffness in hypertension.
Materials and Methods:
In 116 untreated essential hypertensive patients recruited at a referral center in the University of Udine, we assessed common carotid artery stiffness by B-mode ultrasonography and measured plasma fibrinogen, D-dimer, plasminogen activator inhibitor-1 (PAI-1), and homocysteine by the currently available methods. For statistical reasons, the patients were divided according to the median value of each index of carotid stiffness, and continuous variables were further analyzed by univariate correlation and stepwise multivariate regression analysis.
Results:
PAI-1 levels were significantly higher in patients with low coefficient of distensibility (P = 0.018) and high Young's elastic modulus (P = 0.012), whereas no association of fibrinogen, D-dimer, and homocysteine levels was observed with carotid coefficient of distensibility, Young's elastic modulus, and β-stiffness. On univariate analysis, Young's elastic modulus was significantly and positively correlated with PAI-1 levels (r = 0.286, P = 0.002), a correlation that on multivariate regression resulted to be independent of other confounders (β = 0.289, P = 0.028).
Conclusion:
An independent association of plasma PAI-1 levels with carotid artery stiffness suggests a possible contribution of decreased fibrinolytic activity to the early functional abnormalities of arterial vessels in hypertensive patients. This contribution might be relevant for subsequent development of hypertension-related cardiovascular complications.
Keywords: Beta stiffness, carotid artery, fibrinolysis, plasminogen activator inhibitor-1, primary hypertension, Young's elastic modulus
INTRODUCTION
In addition to traditional cardiovascular risk factors, other factors that are commonly referred to as “emerging” or “nontraditional” are possibly involved in the occurrence of atherosclerosis-related events.[1] Among these emerging risk factors, the coagulation system has been called into play and robust epidemiological evidence indicates its involvement in the pathophysiology of atherosclerotic vascular disease.[2] For instance, an activated coagulation system is associated with more severe cardiovascular complications[3] and left ventricular changes[4] in individuals with high blood pressure, suggesting a contribution of a prothrombotic state.
The early stages of atherosclerosis are characterized by subtle functional and/or structural changes of arterial vessels that could be assessed noninvasively by ultrasound examination of carotid arteries.[5] Carotid stiffness is a reproducible marker of early vascular disease that predicts major cardiovascular events[5,6] and development of hypertension,[7] providing important information for stratification of cardiovascular risk.[8] A significant association of an activated hemostatic system with early arterial changes has been reported in individuals without clinically overt atherosclerotic disease, suggesting a contribution of a prothrombotic state.[9,10] In hypertensive patients, changes of carotid arteries have specific relevance because they are a reliable marker of the overall vascular damage. In these patients, the carotid intima-media thickness (IMT) has been found to be independently associated with fibrin D-dimer,[11] a breakdown fragment of fibrin and a marker of the overall activity of the hemostatic system. However, data on the possible association of a prothrombotic state with carotid artery stiffness are not available, and this is why we sought to investigate the relationship of hemostatic variables with carotid distensibility in hypertensive patients.
MATERIALS AND METHODS
Patients
One-hundred and sixteen patients (63 males, 53 females; age 49 ± 13 years) with Grade 1–2 primary hypertension who were consecutively referred from July 2014 to December 2015 to the hypertension clinic at the University of Udine were included in the cross-sectional study. All patients were light-skinned people and were representative of the hypertensive population in this area. Blood pressure was measured with an automated device (Omron M6, OMRON Healthcare Co., Kyoto, Japan) after each individual had been supine for 15 min, and the average of three readings was recorded. Diagnosis of hypertension was established in all patients according to the current guidelines.[8] Patients younger of 18 years and older than 80 years were excluded, together with patients with glomerular filtration rate of <30 ml/min/1.73 m,[2] cardiovascular complications, secondary hypertension, use of drugs that could interfere with hemostatic variables, and acute illness. Cardiovascular complications were identified for exclusion by the analysis of medical records, physical examination, electrocardiography (ECG), echocardiography, and ultrasound examination of aorta, carotid, iliac, and femoral arteries. Additional evaluations included exercise testing, myocardial scintigraphy, and angiography and were done when needed.[12] Secondary forms of hypertension were excluded after extensive clinical and laboratory investigations that included duplicate measurements of 24-h creatinine clearance, plasma active renin and aldosterone, urinary cortisol and catecholamines, and renal ultrasound examination with themeasurement of renal resistance index. Renal angio magnetic resonance imaging/computed tomography scan and additional functional tests were performed when appropriate.[8,13]
Forty-eight (41%) of 116 patients had never been treated with antihypertensive drugs. The remaining 68 patients (59%) were treated with drugs that were washed out for a minimum of 2 weeks before the study. All patients were closely monitored during the wash-out period, and in those with blood pressure persistently higher than 180/110 mmHg, alpha-blockers and/or calcium-channel blockers were given. Before evaluation, patients ate a standard diet for 7 days to keep a sodium intake of 100–150 mmol/day that was checked with the measurement of sodium excretion in 24-h urine collections. Patients were defined as smokers if they had smoked for at least 5 years and up to 1 year before the study, and smoking habit was quantified by the average number of cigarettes/day. Alcohol intake was estimated by a questionnaire[14] as g/day. The study was performed in accordance with the principles of the Declaration of Helsinki and received approval from the local Institutional Review Board. Informed consent was obtained from all patients
Assessment of carotid artery distensibility
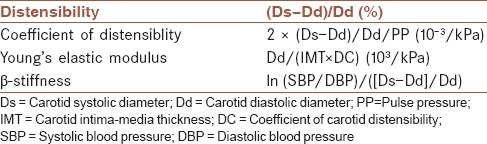
Carotid arteries were examined with a duplex scanner (Toshiba Aplio CV, Japan) using a 7 MHz linear array transducer.[15] The same trained operator performed all examinations. B-mode ultrasound examination of carotid arteries permits assessment of carotid artery stiffness with a good degree of reproducibility and provides information comparable to other echo-tracking methods with specificity and sensitivity of more than 90%.[16] After patients had been laying quietly in a room for 15 min, and immediately before performing carotid artery ultrasound examination, blood pressure was measured at the left arm. The average of the last 2 of 3 consecutive measurements obtained in 5 min was considered, and the pulse pressure (PP) was calculated as the difference between systolic and diastolic blood pressure. Longitudinal scan of right and left common carotid arteries was performed under ECG guide to measure carotid systolic diameter (Ds) and diastolic diameter (Dd), and the average of measurements obtained in three consecutive cardiac cycles was calculated for both arteries according to consensus.[16] Measurements used to calculate carotid distensibility are shown in Table 1 together with the formulas that have been used for calculation and the respective units. Intra-observer variability of all ultrasound measurements was below 8%, and the correlation coefficient (r) of duplicate measurements for all parameters was >0.850 showing good reproducibility of these measurements.
Table 1.
Indices of carotid artery distensibility that were measured in the study patients and formulas that are used for their calculation
Laboratory measurements
A sample of venous blood was collected in the morning after an overnight fast with the patients in sitting position. Blood was collected into silicone-treated tubes containing trisodium citrate, and plasma was immediately separated and frozen at −80°C until assaying, usually within 1 month from sampling. Plasma glucose was assayed using the glucose-oxidase method. Total cholesterol and triglycerides were assayed enzymatically by an automated method. High-density lipoprotein cholesterol was assayed enzymatically after magnesium chloride-dextran sulfate precipitation of apolipoprotein B-containing lipoproteins, and low-density lipoprotein cholesterol was calculated with the formula of Friedewald. Glomerular filtration rate was measured by duplicate measurement of 24-h creatinine clearance and normalized for body surface area. Hemostatic variables were measured as reported previously.[4,17] Briefly, plasma fibrinogen was determined by a functional assay in an automated coagulometer autoanalyzer (Instrumentation Laboratory, Lexington, Massachusetts, USA; inter- and intra-assay coefficient of variation: 6.8% and 5.1%, respectively), D-dimer was measured immunoenzymatically (according to the method of Rylatt; inter- and intra-assay coefficient of variation: 7.1% and 5.3%, respectively), and plasminogen activator inhibitor-1 (PAI-1) was assayed by enzyme immunoassay (Innotest PAI-1; Byk-Sangtec, Dietzenbach, Germany; inter- and intra-assay coefficient of variation: 6.8% and 4.6%, respectively). Homocysteine was determined by a nephelometric method (Dimension Vista System, Siemens Healthcare Diagnostics, Milan, Italy; inter- and intra-assay coefficients of variation: 8.2% and 7.0%, respectively).[18]
Statistical methods
Values are expressed as mean ± standard deviation for normally distributed variables, with median and interquartile ranges used for variables with skewed distributions. Normality of distribution was assessed with Kolmogorov–Smirnov test, and variables with skewed distributions were analyzed after logarithmic transformation. The Student's t-test was used for comparison between two independent groups after adjustment for age, body mass index, and blood pressure values. Pearson's hi-square test was used to compare frequency distributions. Relationships between continuous variables were examined through linear regression analysis, with correlation expressed by Pearson's orrelation coefficient. Stepwise multivariate regression analysis was used to ascertain which variables were independently related to indices of carotid stiffness. The sample size was calculated to provide a power >90% with a probability of <5% in the detection of a 20% difference in hemostatic variables between individuals with low or high carotid stiffness. Probability values of <5% were considered to indicate statistical significance. Data analyses were done with the Stata 9.2 software system (StataCorp LP, College Station, TX, USA).
RESULTS
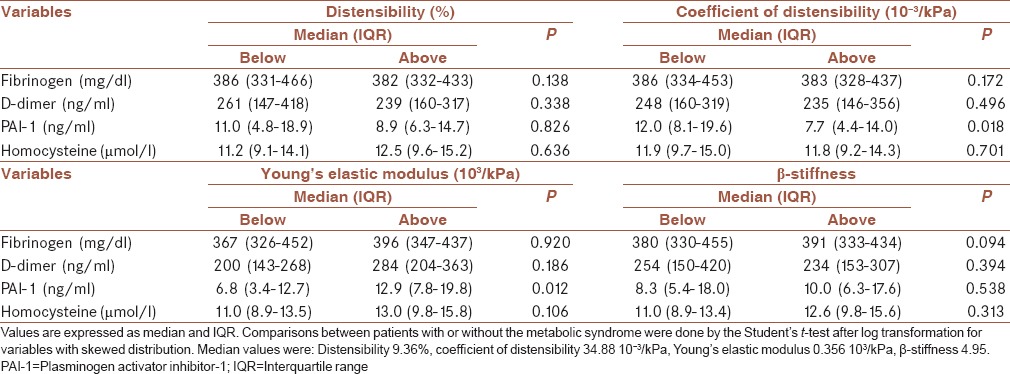
The clinical characteristics, biochemical variables, and indices of carotid artery stiffness of the patients included in the study are summarized in Table 2. Patients were divided according to the median value of the distribution of each index of carotid stiffness, and plasma levels of fibrinogen, D-dimer, PAI-1, and homocysteine are reported in Table 3. After adjustment for the confounding effects of age, body mass index, and blood pressure value, PAI-1 levels were significantly higher in patients with low values of coefficient of distensibility and high values of the Young's elastic modulus. No significant differences were observed in fibrinogen, D-dimer, and homocysteine between patients with values below or above the median of carotid distensibility, coefficient of distensibility, Young's elastic modulus, and β-stiffness.
Table 2.
Clinical characteristics, biochemical variables, and markers of carotid artery distensibility of the study patients
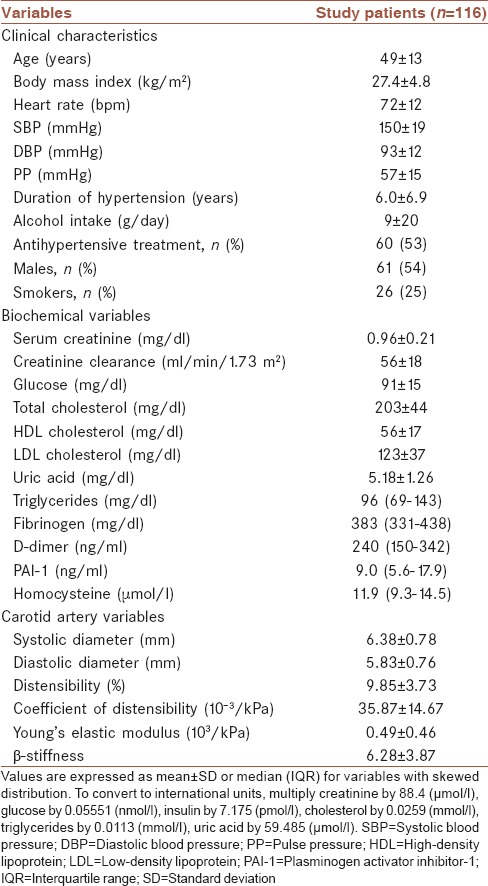
Table 3.
Plasma concentrations of hemostatic markers according to values (below or above the median of the distribution) of six different indices of carotid artery distensibility
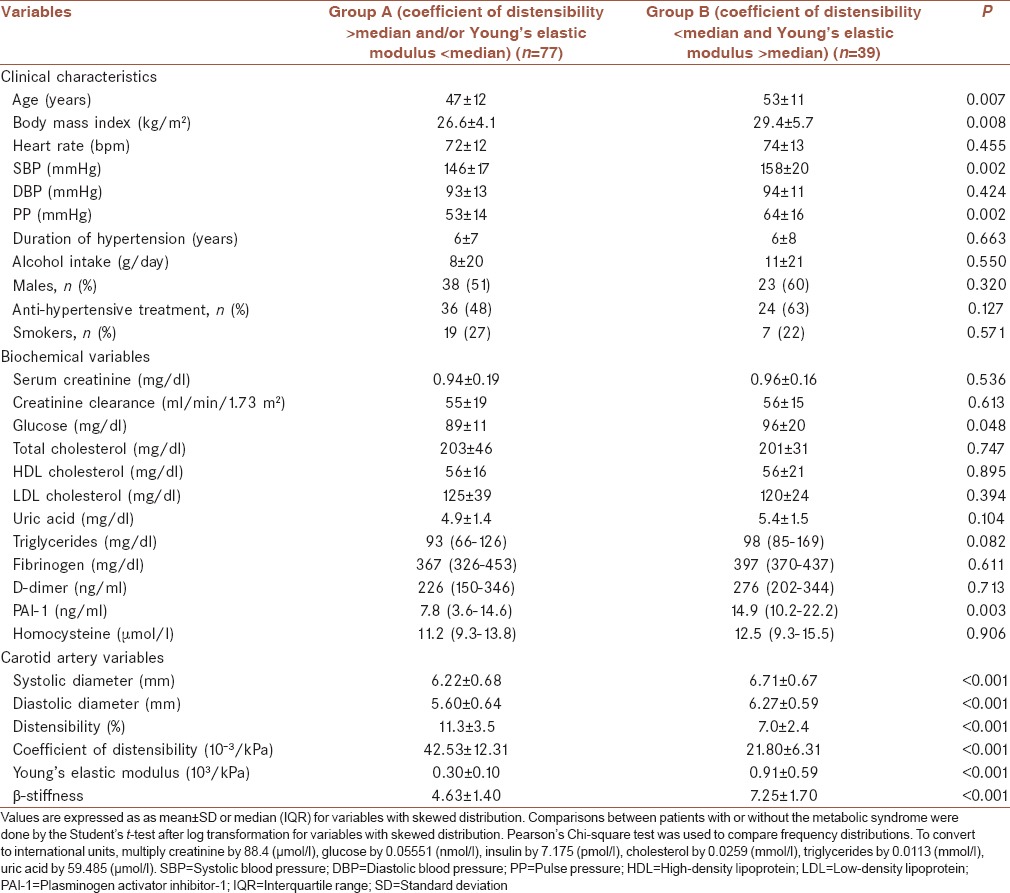
Because the coefficient of distensibility and Young's elastic modulus are, respectively, the markers that best define the relationship of vascular dimension changes through cardiac cycle with the blood pressure change (PP) and geometry of the vascular wall (relative wall thickness),[8] we combined these two variables to select among the study patients a group of individuals with the worst carotid stiffness profile (coefficient of distensibility below the median and Young's elastic modulus above the median) and compared these with the remaining patients [Table 4]. Patients with higher carotid artery stiffness were older and had greater body mass index, systolic pressure and PP, fasting glucose, and PAI-1 levels than patients with better carotid stiffness profile, whereas no differences were observed in fibrinogen, D-dimer, and homocysteine.
Table 4.
Clinical characteristics, biochemical variables, and indices of carotid artery distensibility of study patients who were grouped according to severity of aortic stiffness as Group A (patients with coefficient of distensibility below or Young's elastic modulus above median of the distribution) and Group B (patients with both coefficient of distensibility below and Young's elastic modulus above the median of the distribution)
Univariate regression analysis indicated an inverse significant relationship of the coefficient of distensibility with age (r = −0.226, P = 0.015), body mass index (r = −220, P = 0.018), log-transformed plasma glucose (r = −0.219, P = 0.018), triglycerides (r = −0.270, P = 0.003), and PAI-1 levels (r = −0.197, P = 0.034). Young's elastic modulus was directly and significantly correlated with age (r = 0.349, P < 0.001) and PAI-1 levels (r = 0.286, P = 0.002). No further significant correlation was observed between hemostatic markers and indices of carotid stiffness [Table 5]. Stepwise multivariate regression analysis that included demographic, anthropometric, and plasma lipid variables indicated that the Young's elastic modulus was independently related with both age (β =0.360, P = 0.011) and PAI-1 (β =0.289, P = 0.028).
Table 5.
Univariate correlation analysis of hemostatic markers and indices of carotid artery distensibility

DISCUSSION
Many nontraditional cardiovascular risk factors are associated with the presence and severity of organ damage in hypertensive patients. Definition of the pathophysiology of subclinical vascular damage in these patients is of great relevance because its detection anticipates major cardiovascular events. Moreover, previous studies indicate an involvement of the hemostatic system in the development of structural changes of the carotid arteries. The present study has examined the association of hemostatic markers with early functional changes of the carotid arteries. Findings indicate that plasma levels of PAI-1 are directly and independently related to carotid artery stiffness as assessed by the coefficient of distensibility and Young's elastic modulus, suggesting a contribution of decreased fibrinolytic activity to the early functional abnormalities of arterial vessels.
Increased arterial stiffness has long been considered a consequence of aging. In fact, progressive fragmentation and derangement of the elastic laminae of the arterial wall occur in major central arteries resulting in age-related vascular stiffening.[19] In addition to aging, however, other cardiovascular risk factors contribute to reduction of distensibility of the vascular wall including smoking,[20] dyslipidemia,[21] diabetes,[22] and hypertension.[6] Moreover, cross-sectional studies have reported that increased carotid stiffness is associated with greater cardiovascular risk in patients with atherosclerotic risk factors or who have already developed vascular disease.[7] Evidence of the role of increased arterial stiffness in prediction of cardiovascular events was obtained also in longitudinal studies that were conducted in patients with hypertension,[23] impaired glucose tolerance,[24] and end-stage renal disease.[25]
Hypertension causes structural changes of the arterial wall that are associated with hypertrophy of the muscular layer, increase in extracellular matrix, and geometric remodeling,[26] resulting in functional abnormalities that anticipate major hypertension-related cardiovascular complications.[5,7] In addition to increased blood pressure, other conditions including a prothrombotic state might contribute to these vascular changes and the related complications. In a study conducted in hypertensive patients, a relationship of plasma fibrinogen and D-dimer levels with the presence and severity of target-organ damage that was independent of age, blood pressure, and duration of hypertension was reported.[3] In another group of patients with hypertension, it was shown that elevated levels of fibrinogen, fibrin D-dimer, and homocysteine are associated with high carotid IMT although this association was independent of possible confounders only for D-dimer.[11] These findings together with those of other studies conducted in the general population[27,28] and patients with type-2 diabetes[29] indicate a contribution of a prothrombotic state to the early structural changes of carotid arteries. Moreover, these findings set the stage for the present study in which we have tested the hypothesis that an activated hemostatic system might contribute also to carotid artery stiffness in patients with hypertension. Our findings indicate that levels of PAI-1 are significantly and independently related to carotid artery stiffening, suggesting a role of decreased fibrinolytic activity. However, in agreement with previous studies,[30] we have not observed associations of carotid stiffness with plasma fibrinogen, D-dimer, and homocysteine.
Limitations of this study should be highlighted. First, use of a clinic sample of patients with hypertension limits the possibility to extrapolate the present observations to the general population. Second, inclusion of a relevant percentage of hypertensive patients who were not treatment-naive might have introduced, despite a relatively long wash-out period, a possible confounder affecting some of the variables measured in this study. It must be noticed, however, that no differences in indices of carotid distensibility or hemostatic markers were observed between untreated patients and patients who were treated with different classes of antihypertensive drugs.
CONCLUSION
This study demonstrates a significant and independent relationship of plasma PAI-1 levels with carotid artery stiffness, suggesting a possible contribution of decreased fibrinolytic activity to the early functional abnormalities of arterial vessels that are commonly detected in patients with high blood pressure. This relationship might be relevant for the subsequent development of hypertension-related cardiovascular complications. Further research in appropriately designed longitudinal studies would be warranted to better explore this hypothesis.
Financial support and sponsorship
C.C. was the recipient of a European Cooperation in the field of Scientific and Technical Research (COST-BM1301) grant. This work was supported by a generous contribution of the Piersilverio Nassimbeni Foundation to C.C. and L.A.S.
Conflicts of interest
The authors have no conflicts of interest.
Acknowledgments
This study was supported by a generous contribution of the Piersilverio Nassimbeni Foundation.
REFERENCES
- 1.Catena C, Novello M, Lapenna R, Baroselli S, Colussi G, Nadalini E, et al. New risk factors for atherosclerosis in hypertension: Focus on the prothrombotic state and lipoprotein(a) J Hypertens. 2005;23:1617–31. doi: 10.1097/01.hjh.0000178835.33976.e7. [DOI] [PubMed] [Google Scholar]
- 2.Cushman M, Lemaitre RN, Kuller LH, Psaty BM, Macy EM, Sharrett AR, et al. Fibrinolytic activation markers predict myocardial infarction in the elderly. The Cardiovascular Health Study. Arterioscler Thromb Vasc Biol. 1999;19:493–8. doi: 10.1161/01.atv.19.3.493. [DOI] [PubMed] [Google Scholar]
- 3.Sechi LA, Zingaro L, Catena C, Casaccio D, De Marchi S. Relationship of fibrinogen levels and hemostatic abnormalities with organ damage in hypertension. Hypertension. 2000;36:978–85. doi: 10.1161/01.hyp.36.6.978. [DOI] [PubMed] [Google Scholar]
- 4.Catena C, Colussi G, Fedrizzi S, Sechi LA. Association of a prothrombotic state with left-ventricular diastolic dysfunction in hypertension: A tissue-Doppler imaging study. J Hypertens. 2013;31:2077–84. doi: 10.1097/HJH.0b013e328362d951. [DOI] [PubMed] [Google Scholar]
- 5.Bots ML, Dijk JM, Oren A, Grobbee DE. Carotid intima-media thickness, arterial stiffness and risk of cardiovascular disease: Current evidence. J Hypertens. 2002;20:2317–25. doi: 10.1097/00004872-200212000-00002. [DOI] [PubMed] [Google Scholar]
- 6.Simons PC, Algra A, Bots ML, Grobbee DE, van der Graaf Y. Common carotid intima-media thickness and arterial stiffness: Indicators of cardiovascular risk in high-risk patients. The SMART Study (Second Manifestations of ARTerial disease) Circulation. 1999;100:951–7. doi: 10.1161/01.cir.100.9.951. [DOI] [PubMed] [Google Scholar]
- 7.Liao D, Arnett DK, Tyroler HA, Riley WA, Chambless LE, Szklo M, et al. Arterial stiffness and the development of hypertension. The ARIC study. Hypertension. 1999;34:201–6. doi: 10.1161/01.hyp.34.2.201. [DOI] [PubMed] [Google Scholar]
- 8.Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, et al. 2007 guidelines for the management of arterial hypertension: The task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) J Hypertens. 2007;25:1105–87. doi: 10.1097/HJH.0b013e3281fc975a. [DOI] [PubMed] [Google Scholar]
- 9.Folsom AR, Wu KK, Shahar E, Davis CE. Association of hemostatic variables with prevalent cardiovascular disease and asymptomatic carotid artery atherosclerosis. The Atherosclerosis Risk in Communities (ARIC) Study Investigators. Arterioscler Thromb. 1993;13:1829–36. doi: 10.1161/01.atv.13.12.1829. [DOI] [PubMed] [Google Scholar]
- 10.Batagini NC, da Silva ES, Pinto CA, Puech-Leão P, de Luccia N. Analysis of risk factors and diseases associated with atherosclerosis in the progression of carotid artery stenosis. Vascular. 2016;24:59–63. doi: 10.1177/1708538115571404. [DOI] [PubMed] [Google Scholar]
- 11.Catena C, Colussi G, Brosolo G, Sechi LA. A prothrombotic state is associated with early arterial damage in hypertensive patients. J Atheroscler Thromb. 2012;19:471–8. doi: 10.5551/jat.10819. [DOI] [PubMed] [Google Scholar]
- 12.Sechi LA, Zingaro L, Catena C, De Marchi S. Increased fibrinogen levels and hemostatic abnormalities in patients with arteriolar nephrosclerosis: Association with cardiovascular events. Thromb Haemost. 2000;84:565–70. [PubMed] [Google Scholar]
- 13.Catena C, Zingaro L, Casaccio D, Sechi LA. Abnormalities of coagulation in hypertensive patients with reduced creatinine clearance. Am J Med. 2000;109:556–61. doi: 10.1016/s0002-9343(00)00567-2. [DOI] [PubMed] [Google Scholar]
- 14.Catena C, Novello M, Dotto L, De Marchi S, Sechi LA. Serum lipoprotein(a) concentrations and alcohol consumption in hypertension: Possible relevance for cardiovascular damage. J Hypertens. 2003;21:281–8. doi: 10.1097/00004872-200302000-00018. [DOI] [PubMed] [Google Scholar]
- 15.Catena C, Colussi G, Frangipane A, Russo A, Verheyen ND, Sechi LA. Carotid artery stiffness is related to hyperinsulinemia and insulin-resistance in middle-aged, non-diabetic hypertensive patients. Nutr Metab Cardiovasc Dis. 2015;25:968–74. doi: 10.1016/j.numecd.2015.06.009. [DOI] [PubMed] [Google Scholar]
- 16.Bianchini E, Bozec E, Gemignani V, Faita F, Giannarelli C, Ghiadoni L, et al. Assessment of carotid stiffness and intima-media thickness from ultrasound data: Comparison between two methods. J Ultrasound Med. 2010;29:1169–75. doi: 10.7863/jum.2010.29.8.1169. [DOI] [PubMed] [Google Scholar]
- 17.Sechi LA, Novello M, Colussi G, Di Fabio A, Chiuch A, Nadalini E, et al. Relationship of plasma renin with a prothrombotic state in hypertension: Relevance for organ damage. Am J Hypertens. 2008;21:1347–53. doi: 10.1038/ajh.2008.293. [DOI] [PubMed] [Google Scholar]
- 18.Catena C, Colussi G, Nait F, Capobianco F, Sechi LA. Elevated homocysteine levels are associated with the metabolic syndrome and cardiovascular events in hypertensive patients. Am J Hypertens. 2015;28:943–50. doi: 10.1093/ajh/hpu248. [DOI] [PubMed] [Google Scholar]
- 19.Benetos A, Laurent S, Hoeks AP, Boutouyrie PH, Safar ME. Arterial alterations with aging and high blood pressure. A noninvasive study of carotid and femoral arteries. Arterioscler Thromb. 1993;13:90–7. doi: 10.1161/01.atv.13.1.90. [DOI] [PubMed] [Google Scholar]
- 20.Liang YL, Shiel LM, Teede H, Kotsopoulos D, McNeil J, Cameron JD, et al. Effects of blood pressure, smoking, and their interaction on carotid artery structure and function. Hypertension. 2001;37:6–11. doi: 10.1161/01.hyp.37.1.6. [DOI] [PubMed] [Google Scholar]
- 21.Simons PC, Bots ML, Algra A, van Teeffelen AS, van der Graaf Y. Effect of timing of blood pressure measurement in the assessment of arterial stiffness: The SMART Study. Ultrasound Med Biol. 1998;24:1285–9. doi: 10.1016/s0301-5629(98)00097-0. [DOI] [PubMed] [Google Scholar]
- 22.Emoto M, Nishizawa Y, Kawagishi T, Maekawa K, Hiura Y, Kanda H, et al. Stiffness indexes beta of the common carotid and femoral arteries are associated with insulin resistance in NIDDM. Diabetes Care. 1998;21:1178–82. doi: 10.2337/diacare.21.7.1178. [DOI] [PubMed] [Google Scholar]
- 23.Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, et al. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. 2001;37:1236–41. doi: 10.1161/01.hyp.37.5.1236. [DOI] [PubMed] [Google Scholar]
- 24.van Dijk RA, Dekker JM, Nijpels G, Heine RJ, Bouter LM, Stehouwer CD. Brachial artery pulse pressure and common carotid artery diameter: Mutually independent associations with mortality in subjects with a recent history of impaired glucose tolerance. Eur J Clin Invest. 2001;31:756–63. doi: 10.1046/j.1365-2362.2001.00884.x. [DOI] [PubMed] [Google Scholar]
- 25.Blacher J, Pannier B, Guerin AP, Marchais SJ, Safar ME, London GM. Carotid arterial stiffness as a predictor of cardiovascular and all-cause mortality in end-stage renal disease. Hypertension. 1998;32:570–4. doi: 10.1161/01.hyp.32.3.570. [DOI] [PubMed] [Google Scholar]
- 26.Safar ME, Laurent S, Pannier BM, London GM. Structural and functional modifications of peripheral large arteries in hypertensive patients. J Clin Hypertens. 1987;3:360–7. [PubMed] [Google Scholar]
- 27.Salomaa V, Riley W, Kark JD, Nardo C, Folsom AR. Non-insulin-dependent diabetes mellitus and fasting glucose and insulin concentrations are associated with arterial stiffness indexes. The ARIC Study. Atherosclerosis Risk in Communities Study. Circulation. 1995;91:1432–43. doi: 10.1161/01.cir.91.5.1432. [DOI] [PubMed] [Google Scholar]
- 28.Grebe MT, Luu B, Sedding D, Heidt MC, Kemkes-Matthes B, Schaefer CA, et al. Fibrinogen promotes early atherosclerotic changes of the carotid artery in young, healthy adults. J Atheroscler Thromb. 2010;17:1003–8. doi: 10.5551/jat.3715. [DOI] [PubMed] [Google Scholar]
- 29.Corrado E, Rizzo M, Muratori I, Coppola G, Novo S. Association of elevated fibrinogen and C-reactive protein levels with carotid lesions in patients with newly diagnosed hypertension or type II diabetes. Arch Med Res. 2006;37:1004–9. doi: 10.1016/j.arcmed.2006.06.005. [DOI] [PubMed] [Google Scholar]
- 30.Sie MP, Isaacs A, de Maat MP, Mattace-Raso FU, Uitterlinden AG, Kardys I, et al. Genetic variation in the fibrinogen-alpha and fibrinogen-gamma genes in relation to arterial stiffness: The Rotterdam Study. J Hypertens. 2009;27:1392–8. doi: 10.1097/HJH.0b013e32832a95b0. [DOI] [PubMed] [Google Scholar]