

Abstract
Background/study aim
Linked color imaging (LCI) by a laser endoscope (Fujifilm Co, Tokyo, Japan) is a novel narrow band light observation. In this study, we aimed to investigate whether LCI could improve the visibility of colorectal polyps using endoscopic videos.
Patients and methods
We prospectively recorded videos of consecutive polyps 2 – 20 mm in size diagnosed as neoplastic polyps. Three videos, white light (WL), blue laser imaging (BLI)-bright, and LCI, were recorded for each polyp by one expert. After excluding inappropriate videos, all videos were evaluated in random order by two experts and two non-experts according to a published polyp visibility score from four (excellent visibility) to one (poor visibility). Additionally, the relationship between polyp visibility scores in LCI and various clinical characteristics including location, size, histology, morphology, and preparation were analyzed compared to WL and BLI-bright.
Results
We analyzed 101 colorectal polyps (94 neoplastic) in 66 patients (303 videos). The mean polyp size was 9.0 ± 8.1 mm and 54 polyps were non-polypoid. The mean polyp visibility scores for LCI (2.86 ± 1.08) were significantly higher than for WL and BLI-bright (2.53 ± 1.15, P < 0.001; 2.73 ± 1.47, P < 0.041). The ratio of poor visibility (score 1 and 2) was significantly lower in LCI for experts and non-experts (35.6 %, 33.6 %) compared with WL (49.6 %, P = 0.015, 50.5 %, P = 0.046). The polyp visibility scores for LCI were significantly higher than those for WL for all of the factors. With respect to the comparison between BLI-bright and WL, the polyp visibility scores for BLI-bright were not higher than WL for right-sided location, < 10 mm size, sessile serrated adenoma and polyp histology, and poor preparation. For those characteristics, LCI improved the lesions with right-sided location, SSA/P histology, and poor preparation significantly better than BLI.
Conclusions
LCI improved polyp visibility compared to WL for both expert and non-expert endoscopists. It is useful for improving polyp visibility in any location, any size, any morphology, any histology, and any preparation level.
Introduction
The number of colorectal cancer deaths is increasing in the West and in Asian countries. The adenoma-carcinoma sequence is thought to be one of the main pathways for the development of colorectal cancers 1 . Therefore, adenomas are resected using endoscopic treatments such as polypectomy, endoscopic mucosal resection (EMR), and endoscopic submucosal dissection (ESD) 2 3 4 . Colonoscopy is the most effective tool for detecting colorectal adenomas. However, the polyp miss rate under white light (WL) observation was reported to be 20 – 25 % 5 . Therefore, narrow-band imaging (NBI; Olympus Medical Co., Tokyo, Japan), flexible spectral imaging color enhancement (FICE; Fujifilm Co., Tokyo, Japan), and chromoendoscopy were investigated to determine whether they could improve the polyp detection rate; however, most of them failed 6 7 8 9 10 11 .
A LASER endoscope system was developed in 2012. There were two modes of narrow-band imaging observation in that system: blue laser imaging (BLI; Fujifilm Co., Tokyo, Japan) mode and BLI-bright mode 12 13 14 15 . Previously, we have reported that BLI-bright improved polyp visibility compared with WL using recorded polyp videos 16 . To make a polyp more visible is considered to be one of the most important factors related to efficient polyp detection. Recently, new narrow-band light observation, named linked color imaging (LCI), has been developed for diagnosing chronic gastritis in the LASER endoscope 17 . It is brighter than BLI-bright and may also improve colorectal polyp detection.
In the present study, we aimed to investigate whether LCI could improve the visibility of colorectal polyps compared to WL and BLI-bright using endoscopic videos.
Video 1: A polypoid neoplastic polyp (adenoma), size 3 mm, on the left-sided colon (sigmoid colon). WL: score 2. LCI score 4. BLI-bright: score 4. Patients and methods
This was a prospective study and was conducted at the Department of Molecular Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine. We examined consecutive colorectal polyps diagnosed as neoplastic polyps and captured videos of the polyps using three modes (LCI, BLI-bright, and WL) with the LASER endoscope system (LL-4450 light source, and VP-4450HD video processor, Fujifilm Co., Tokyo, Japan) from January 2016 to July 2016. The inclusion criteria were as follows: (1) patients receiving colonoscopies performed only by one expert (N.Y.) were enrolled to retain video quality; (2) patients with colorectal polyps diagnosed as neoplastic polyps between 2 mm and 20 mm in size that had been detected through colonoscopy just before ESD with BLI-bright mode or WL ( Fig. 1 ).
Fig. 1.
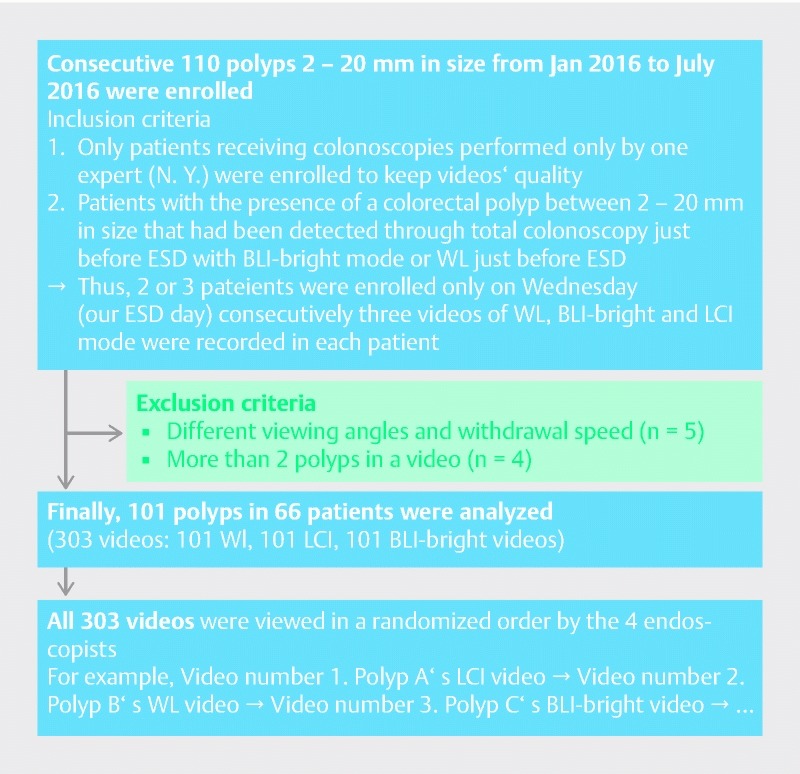
A flow diagram of this study.
Diagnosis of neoplastic polyps was performed with BLI magnification according to previous reports 12 13 18 . Thus, two or three patients were enrolled consecutively only on Wednesdays (our ESD day). In each patient, the number of recorded polyps was limited to a maximum of three on account of patient fatigue during the recording of videos. Three videos in WL, BLI-bright, and LCI mode were recorded for each polyp ( Fig. 1 ). Each video included a range of 3 – 5 cm proximal to the polyp to 3 – 5 cm distal to the polyp (a 5- to 10-second clip). Three videos were recorded for a polyp under the same conditions if possible about the presence of fluid, the amount of insufflation, and the withdrawal speed. Polyp visibility was evaluated using a published polyp visibility score 16 ranging from Score 4 to Score 1. Score 4 indicates excellent visibility; it is easy to detect a polyp. Score 3 indicates good visibility. If an endoscopist looks in the same direction as a polyp in the monitor, it is easy to detect the polyp. Score 2 indicates fair visibility. It is hard to detect the polyp without careful observation. Score 1 indicates poor visibility ( Fig. 2 , Video 1 ). We excluded polyps with noticeable variations of recorded conditions (air, speed, fluid, etc.). Additionally, videos were excluded when more than two polyps were present in the same video. Recurrent lesions after a previous EMR or T2 – T4 colorectal cancers were also excluded.
Fig. 2.
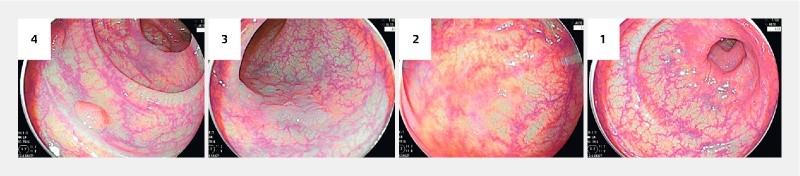
Examples of polyp visibility score. Score 4, excellent visibility; score 3, good visibility; score 2, fair visibility; score 1, poor visibility.
The polyp locations were divided into three parts: the right-sided colon (from the cecum to the transverse colon), the left-sided colon (from the descending colon to the sigmoid colon), and the rectum. With regard to morphology, polyps were divided into polypoid and non-polypoid according to the Paris classification 19 . The size of a polyp was defined by its maximum diameter and was calculated in accordance with the size of the snares.
All of the sets of videos taken during the study period were collected. The evaluation was performed by four endoscopists who had not viewed any of these videos before this study. Of the four endoscopists, two were classified as non-experts (had performed < 5000 colonoscopies and 10 – 30 withdrawing colonoscopies with BLI-bright and LCI) and two were classified as experts (had performed ≥ 5000 colonoscopies and 300 withdrawing colonoscopies with BLI-bright and LCI) according to a previous report 9 . All of the videos were viewed in a randomized order. For example, Video number 1, a LCI video of polyp A, was followed by Video number 2, which was a WL video of polyp B. Each endoscopist assigned a polyp visibility score to each polyp. Scores for each mode (WL, BLI-bright and LCI) were compared and the ratios of polyps with poor visibility (scores 1 and 2) for experts and non-experts in each mode were examined. In addition, the mean polyp visibility scores of WL, LCI and BLI-bright mode in terms of various clinical characteristics including location (right-sided or not right-sided), size (≥ 10 mm or < 10 mm), histology (adenoma + intramucosal cancer or sessile serrated adenoma and polyp (SSA/P)), morphology (polypoid or non-polypoid), and preparation (good or poor) were analyzed. With respect to preparation level, good preparation was defined as local Boston bowel preparation score (BBPS) 2 or 3, and poor preparation was defined as local BBPS 0 or 1. Moreover, the inter-observer agreements of polyp visibility score for experts and non-experts in each mode were analyzed for objective evaluation of polyp visibility scores.
With regard to bowel preparation, patients followed a low-residue diet and were given 10 mL sodium picosulfate 1 day before the examination. All patients also received 1.0 L of a highly concentrated polyethylene glycol solution with ascorbic acid (MoviPrep; Ajinomoto Pharma Co., Ltd, Tokyo, Japan) in the morning on the day of the examination according to our previous report 20 .
All patients provided written informed consent to participate in this study. This study was conducted in accordance with the World Medical Association Helsinki Declaration. It was also approved by the institutional review board and the ethics committees of Kyoto Prefectural University of Medicine. In addition, this study was a subgroup analysis of a study registered in the University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR) as number UMIN000013770.
Histological diagnosis
The tumor specimens were obtained by polypectomy and EMR. Thereafter, they were fixed with 10 % formalin and evaluated histologically. Histological diagnosis was performed by two clinical pathologists (M. K. and A. Y.) according to the World Health Organization classification 21 . Thus, polyps were divided into neoplastic or non-neoplastic categories based on the histological diagnosis. SSA/P were defined as neoplastic lesions in this study.
LASER endoscope and LCI mode
The LASER endoscope system used in this study has been described in previous reports 12 13 . In brief, this system uses a semiconductor laser as the light source and has a narrow-band light observation function called BLI and LCI. It has two types of laser with 410 nm and 450 nm wavelengths. There are two modes for BLI, i. e. BLI mode and BLI-bright mode. BLI mode is useful for acquiring magnified mucosal surface vessels and structure. BLI-bright mode is brighter than BLI mode and it is expected to be useful in tumor detection. However, the weakness of BLI is that the residual liquid becomes reddish. LCI mode is a novel mode and is based on the image captured by light similar to BLI-bright mode; however, further post image processing is applied so that the strong red-tint color becomes more reddish and the pale red-tint color becomes paler. This difference between red color and pale color makes a lesion more noticeable and LCI is brighter than BLI-bright mode ( Fig. 3 ). In addition, the residual liquid was not reddish in LCI mode compared to BLI-bright mode.
Fig. 3.
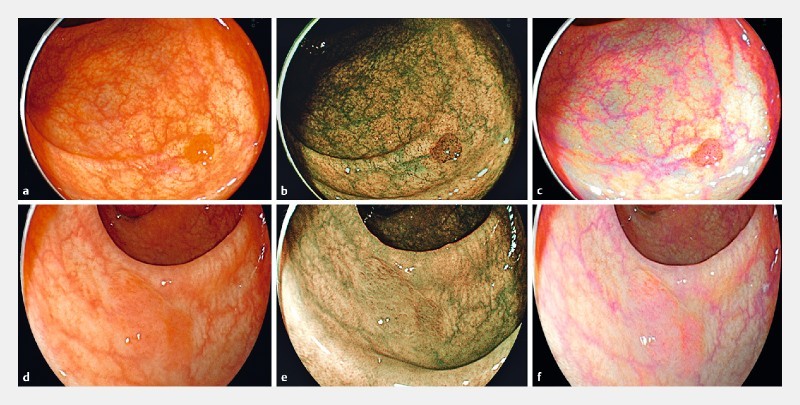
Case presentation. a A polypoid neoplastic polyp (adenoma), 3 mm on the left-sided colon (sigmoid colon). WL: score 2. b BLI-bright: score 4. c LCI score 4. d A non-polypoid polyp (SSA/P), 8 mm in size on the right-sided colon (transverse colon), WL: score 2. e BLI-bright: score 3. f LCI: score 3.
Statistical assessment
In a pilot study on the visibility of 33 colorectal polyps by a single expert endoscopist, LCI achieved superior polyp visibility scores compared with WL in 15 polyps (15/33; 45.4 %). Using a sign test, the α error was 5 % and β error was 20 %. Thus, the minimum sample size was calculated to be 25. The pilot study was performed by one expert and subgroup analysis was designed for location, polyp size, etc. Thus, we decided to use a sample size of 100. The Mann-Whitney U test, Wilcoxon signed-rank test with Bonferroni correction, and the chi-squared test (SPSS version 22.0 for Windows, IBM Japan, Ltd., Tokyo, Japan) were used in this study. Continuous variables such as patient age and tumor size were analyzed using the Mann-Whitney U test. The four phases of the evaluation (polyp visibility scores 1 – 4) were used as ordered-categorical variables, and comparisons between methods used the Wilcoxon signed-rank test with Bonferroni correction. Inter-observer agreement for polyp visibility scores was determined by the quadratic-weighted kappa coefficient of Cohen. A P value < 0.05 was considered to be statistically significant.
Results
In total, videos from 110 consecutive polyps (WL, LCI, and BLI-bright) were recorded and nine polyps were excluded according to the decided criteria ( Fig. 1 ). Finally, a total of 101 polyps (mean polyp size 9.0 ± 8.1 mm) in 66 patients (303 videos) were investigated in this study ( Table 1 ). Forty-seven polyps (46.5 %) were polypoid and 55 polyps (54.5 %) were in the right-sided colon. Ninety-four polyps (93.1 %) were neoplastic ( Table 1 ).
Table 1. Clinical characteristics of 101 colorectal polyps.
| Number of polyps | 101 |
| Number of patients | 66 |
| Sex (male/female) | 45/21 |
| Age, mean ± SD (range), years | 67.7 ± 9.8 (39 – 85) |
| Polyp size, mean ± SD (range), mm | 9.0 ± 8.1 (2 – 20) |
| Location, (right-sided: left-sided: rectum), n (%) | 55:29:17 (54.5:28.7:16.8) |
| Morphology (polypoid or non-polypoid), n (%) | 47:54 (46.5:53.5) |
| Histopathological diagnosis | |
|
7 (6.9):94 (93.1) |
|
7:20:51:23 |
Right-sided: from the cecum to the transverse colon; left-sided: from the descending colon to the sigmoid colon; SSA/P: sessile serrated adenoma/polyp; HP: hyperplastic polyp; Ad: adenoma; Tis: intramucosal cancer.
The mean polyp visibility scores of LCI mode (2.86 ± 1.08) were significantly higher than those of WL (2.53 ± 1.15, P < 0.001) and BLI-bright (2.73 ± 1.47, P = 0.041) ( Table 2 ). For non-experts, the polyp visibility scores of LCI (2.83 ± 1.07) were higher than WL (2.51 ± 1.14, P < 0.001) and BLI-bright (2.70 ± 1.12, P = 0.047). On the other hand, for experts, the polyp visibility scores of LCI (2.83 ± 1.07) were higher than WL (2.58 ± 1.19, P < 0.001), but not significantly higher than BLI-bright (2.78 ± 1.17, P = 0.30) ( Table 2 ).
Table 2. Mean polyp visibility scores of colorectal polyps in WL, LCI, and BLI-bright mode for all endoscopists, experts, and non-experts.
| WL | LCI | BLI-bright | P value | |
| All | 2.53 ± 1.15 | 2.86 ± 1.08 | 2.73 ± 1.47 |
WL vs. LCI
P
< 0.001
WL vs. BLI-bright P = 0.005 LCI vs. BLI-bright P = 0.041 |
| Experts | 2.58 ± 1.19 | 2.87 ± 1.12 | 2.78 ± 1.17 |
WL vs. LCI
P
< 0.001
WL vs. BLI-bright P = 0.01 LCI vs. BLI-bright P = 0.30 |
| Non-experts | 2.51 ± 1.14 | 2.83 ± 1.07 | 2.70 ± 1.12 |
WL vs. LCI
P
< 0.001
WL vs. BLI-bright P = 0.006 LCI vs. BLI-bright P = 0.047 |
WL: white light; LCI: linked color imaging; BLI: blue laser imaging.
The ratios of poor visibility (score 1 or 2) of WL, BLI-bright, and LCI for experts and non-experts were analyzed ( Fig. 4 ). For the experts, the mean ratio of poor visibility was significantly lower in LCI (16.8 + 18.8: 35.6 %) than in WL mode (24.8 + 24.8: 49.6 %) ( P = 0.015). For the non-experts, the mean ratio of poor visibility in LCI (15.8 + 17.8: 33.6 %) was also significantly lower than that in WL (25.7 + 24.8: 50.5 %) ( P = 0.046).
Fig. 4.
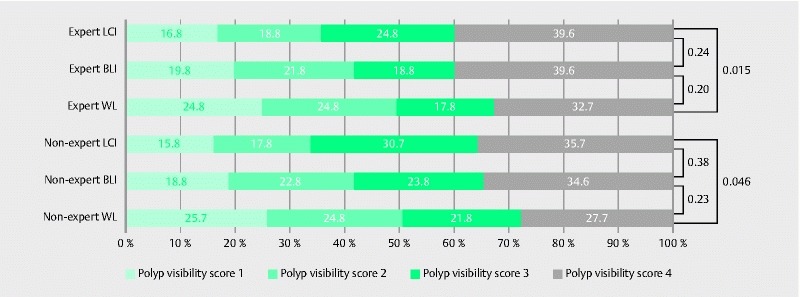
Graphic for derivation of the ratios of poor polyp visibility scores (1 or 2) in LCI, BLI-bright, and WL modes.
The mean polyp visibility scores of WL, LCI and BLI-bright mode in terms of various clinical characteristics are shown in Table 3 . The polyp visibility scores for LCI mode were significantly higher than those for WL for all of the factors. With respect to the comparison between BLI and WL, the polyp visibility scores of BLI were not higher than WL in right-sided location, < 10 mm size, SSA/P histology, and poor preparation. For those clinical characteristics, the visibility scores of lesions with right-sided location, SSA/P histology, and poor preparation were significantly higher with LCI than with BLI ( Fig. 5 ).
Table 3. Mean polyp visibility scores for each clinical characteristic in WL, LCI and BLI-bright mode.
| P value | |||||||
| Number of patients | WL | LCI | BLI | WL vs LCI | WL vs BLI | LCI vs BLI | |
| Right-sided | 55 | 2.22 ± 1.04 | 2.61 ± 1.07 | 2.32 ± 1.08 | < 0.001 | 0.12 | < 0.001 |
| Not right-sided | 46 | 2.91 ± 1.17 | 3.15 ± 1.03 | 3.32 ± 0.99 | < 0.001 | < 0.001 | 0.18 |
| ≥ 10 mm | 38 | 2.65 ± 1.15 | 3.00 ± 1.21 | 2.82 ± 1.13 | < 0.001 | 0.04 | 0.03 |
| < 10 mm | 63 | 2.46 ± 1.15 | 2.67 ± 1.13 | 2.68 ± 1.47 | < 0.001 | 0.07 | < 0.001 |
| Ad, Tis | 74 | 2.68 ± 1.17 | 3.06 ± 1.04 | 2.91 ± 1.13 | < 0.001 | < 0.001 | 0.009 |
| SSA/P | 20 | 2.08 ± 1.03 | 2.20 ± 0.99 | 2.00 ± 0.94 | 0.04 | 0.43 | 0.02 |
| Polypoid | 47 | 2.56 ± 1.22 | 2.81 ± 1.15 | 2.69 ± 1.22 | < 0.001 | 0.02 | 0.06 |
| Non-polypoid | 54 | 2.51 ± 1.10 | 2.90 ± 1.03 | 2.76 ± 1.06 | < 0.001 | 0.03 | < 0.001 |
| Poor preparation | 23 | 2.42 ± 1.13 | 2.72 ± 1.11 | 2.31 ± 1.09 | 0.004 | 0.33 | < 0.001 |
| Good preparation | 78 | 2.55 ± 1.19 | 2.89 ± 1.09 | 2.79 ± 1.18 | < 0.001 | 0.03 | < 0.001 |
WL: white light; LCI: linked color imaging; BLI: blue laser imaging; Ad: adenoma; Tis: intramucosal cancer; SSA/P: sessile serrated adenoma/polyp.
Fig. 5.
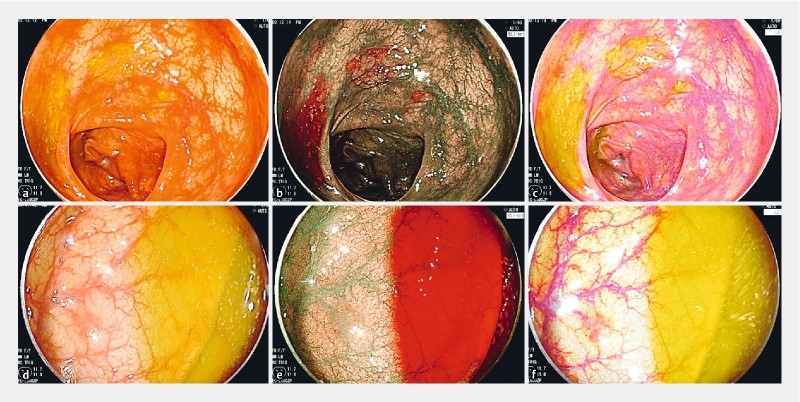
Case presentation. a A non-polypoid neoplastic polyp (SSA/P) in poor preparation, size 8 mm on the right-sided colon (ascending colon). WL: score 2. b BLI-bright: score 2. Residual liquid became reddish and, when viewing the lesion from the oral side, the colon was dark. c LCI score 3. Residual liquid was yellowish and, when viewing the lesion from the oral side, the colon was bright. d A non-polypoid neoplastic polyp (adenoma) in poor preparation, size 2 mm on the rectum. WL: score 2. e BLI-bright: score 3. f LCI: score 3.
With respect to the analysis of inter-observer agreement, the kappa values for the four endoscopists (expert A vs expert B, non-expert A vs non-expert B) were calculated in LCI, WL, and BLI-bright mode. The kappa values for experts were 0.87 for LCI, 0.91 for WL, and 0.84 for BLI-bright. The kappa values for non-experts were 0.86 for LCI, 0.97 for WL, and 0.78 for BLI-bright mode.
Discussion
LCI mode strengthens the color contrast between normal mucosa and colorectal lesions and it is brighter than other narrow-band light observations such as BLI and NBI. Thus, the color of the lesion becomes reddish and the surrounding mucosa becomes whitish. An earlier study reported an improvement in the visibility of diffuse redness of gastric mucosa in Helicobacter pylori induced gastritis with LCI 22 . Theoretically, reddish neoplastic lesions such as adenoma and cancer are detected in LCI mode according to the increase in reddish color in vascular rich areas of those lesions. On the other hand, whitish neoplastic lesions such as SSA/P are detected according to the increase in whitish color in vascular poor areas of those lesions. In addition, the residual liquid is not reddish compared to BLI and NBI modes. Generally, poor preparation is detected in 20 – 25 % of all colonoscopies 23 24 . In those cases, NBI and BLI are not effective due to the reddish color of the residual liquid; however, LCI is thought to have increased efficacy in those cases. In our study, LCI showed higher polyp visibility scores than WL and BLI-bright in poor preparation cases.
Our previous study on polyp visibility between WL and BLI-bright showed that, for non-experts, the polyp visibility scores for all clinical characteristics (location, size, histology, and morphology) in BLI-bright mode were significantly higher than those in WL. On the other hand, for experts, the scores for right-sided polyps, non-neoplastic polyps (including SSA/P), and polypoid polyps in BLI-bright mode were not higher than those in WL. One of the possible reasons for this was because the brightness of BLI-bright might not be sufficient for the wider right-sided colon. In the present study, the mean polyp visibility scores of LCI mode were higher than for WL for all clinical polyp parameters (location, size, histology, morphology). Compared to BLI-bright, those were higher in right-sided location and SSA/P histology, which were weak points of BLI-bright. Generally, right-sided polyps and non-polypoid polyps are sometimes difficult to be detected with WL, especially for non-experts because of poor polyp visibility. However, LCI enables us to increase polyp visibility in polyps with various clinical characteristics and detect those polyps more easily than with WL for both experts and non-experts.
Polyp detection is related to many factors such as lesion characteristics (location, morphology, size, and bowel preparation) and endoscopist’s experience, especially insertion and withdrawal techniques, and polyp visibility. Among these factors, we believe that improvement in polyp visibility is one of the most important factors for improving polyp detection and the adenoma detection rate. In this study, only a small segment of video from the whole colonoscopic observation was used and we could control many factors including withdrawal speed and bowel preparation. We have previously reported video studies similar to this study 16 25 . One of our studies showed that the previous NBI system (EVIS LUCERA Spectrum system) did not increase polyp visibility and a more recent NBI system (EVIS LUCERA Elite system) increased polyp visibility 25 . Those findings are consistent with the failure of NBI studies on polyp detection 6 7 . We believe that this kind of video study is closer to a real colonoscopy than one using endoscopic images. In addition, the randomized video method is easier to be performed than a real polyp detection study. We believe that if this kind of video study is performed as a pre-study to evaluate the polyp visibility of a new modality, it is useful in deciding whether a subsequent polyp detection study should be performed. In this video study, LCI showed better polyp visibility than BLI-bright and WL. Thus, we believe that LCI is a good indication for a further polyp detection study.
There were some limitations to our study. Only patients receiving ESD in our center were enrolled in this study and all videos evaluated were recorded by the same expert endoscopist. Thus, there might be selection bias. This study was a single-center study and was performed by the review of videos to examine polyp visibility. Our final goal is to improve polyp detection, but the improvement in polyp visibility may not affect polyp detection in clinical cases because polyp detection is influenced by various factors other than polyp visibility.
In conclusion, our study showed that LCI improved polyp visibility compared to WL for both expert and non-expert endoscopists. It is useful for improving polyp visibility in any location and with any size, morphology, histology and preparation level.
Acknowledgment
We thank Dr. Norihiro Yamamoto, Dr. Mototsugu Kato, Dr. Takashi Hisabe, and Dr. Kenshi Yao for designing the study. We also thank Kubo Masahiro for assistance with procedures related to the Fujifilm LASEREO system. Moreover, we thank all members of the Department of Molecular Gastroenterology and Hepatology, Kyoto Prefectural University of Medicine for helping with this study.
Footnotes
Competing interests Yoshito Itoh is affiliated with FUJIFILM Medical Co. Ltd. Yuji Naito received research grants from Otsuka Pharmaceutical Co., Ltd. and Takeda Pharmaceutical Co., Ltd. The other authors have no conflicts of interest to declare.
References
- 1.Vogelstein B, Fearon E R, Hamilton S R et al. Genetic alterations during colorectal-tumor development. N Engl J Med. 1988;319:525–532. doi: 10.1056/NEJM198809013190901. [DOI] [PubMed] [Google Scholar]
- 2.Saito Y, Uraoka T, Yamaguchi Y et al. A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video) Gastrointest Endosc. 2010;72:1217–1225. doi: 10.1016/j.gie.2010.08.004. [DOI] [PubMed] [Google Scholar]
- 3.Kudo S, Tamegai Y, Yamano H et al. Endoscopic mucosal resection of the colon: the Japanese technique. Gastrointest Endosc Clin N Am. 2001;11:519–535. [PubMed] [Google Scholar]
- 4.Tanaka S, Haruma K, Oka S et al. Clinicopathological features and endoscopic treatment of superficially spreading colorectal neoplasms larger than 20 mm. Gastrointest Endosc. 2001;54:62–66. doi: 10.1067/mge.2001.115729. [DOI] [PubMed] [Google Scholar]
- 5.van Rijn J C, Reitsma J B, Stoker J et al. Polyp miss rate determined by tandem colonoscopy: a systematic review. Am J Gastroenterol. 2006;101:343–350. doi: 10.1111/j.1572-0241.2006.00390.x. [DOI] [PubMed] [Google Scholar]
- 6.Adler A, Pohl H, Papanikolaou I S et al. A prospective randomised study on narrow-band imaging versus conventional colonoscopy for adenoma detection: does narrow-band imaging induce a learning effect? Gut. 2008;57:59–64. doi: 10.1136/gut.2007.123539. [DOI] [PubMed] [Google Scholar]
- 7.Rex D K, Helbig C. High yields of small and flat adenomas with high-definition colonoscopes using either white light or narrow band imaging. Gastroenterology. 2007;133:42–47. doi: 10.1053/j.gastro.2007.04.029. [DOI] [PubMed] [Google Scholar]
- 8.Inoue T, Murano M, Murano N et al. Comparative study of conventional colonoscopy and pan-colonic narrow-band imaging system in the detection of neoplastic colonic polyps: a randomized controlled trial. J Gastroenterol. 2008;43:45–50. doi: 10.1007/s00535-007-2125-x. [DOI] [PubMed] [Google Scholar]
- 9.Horimatsu T, Sano Y, Tanaka S et al. Next-generation narrow band imaging system for colonic polyp detection: a prospective multicenter randomized trial. Int J Colorectal Dis. 2015;30:947–954. doi: 10.1007/s00384-015-2230-x. [DOI] [PubMed] [Google Scholar]
- 10.Chung S J, Kim D, Song J H et al. Efficacy of computed virtual chromoendoscopy on colorectal cancer screening: a prospective, randomized, back-to-back trial of Fuji Intelligent Color Enhancement versus conventional colonoscopy to compare adenoma miss rates. Gastrointest Endosc. 2010;72:136–142. doi: 10.1016/j.gie.2010.01.055. [DOI] [PubMed] [Google Scholar]
- 11.Pohl J, Lotterer E, Balzer C et al. Computed virtual chromoendoscopy versus standard colonoscopy with targeted indigocarmine chromoscopy: a randomised multicentre trial. Gastrointest Endosc. 2009;69:734–741. doi: 10.1136/gut.2008.153601. [DOI] [PubMed] [Google Scholar]
- 12.Yoshida N, Hisabe T, Inada Y et al. The ability of a novel blue laser imaging system for the diagnosis of invasion depth of colorectal neoplasms. J Gastroenterol. 2014;49:73–80. doi: 10.1007/s00535-013-0772-7. [DOI] [PubMed] [Google Scholar]
- 13.Yoshida N, Yagi N, Inada Y et al. The ability of a novel blue laser imaging system for the diagnosis of colorectal polyps. Dig Endosc. 2014;26:250–258. doi: 10.1111/den.12127. [DOI] [PubMed] [Google Scholar]
- 14.Miyaki R, Yoshida S, Tanaka S et al. A computer system to be used with laser-based endoscopy for quantitative diagnosis of early gastric cancer. J Clin Gastroenterol. 2015;49:108–115. doi: 10.1097/MCG.0000000000000104. [DOI] [PubMed] [Google Scholar]
- 15.Osawa H, Yamamoto H. Present and future status of flexible spectral imaging color enhancement and blue laser imaging technology. Dig Endosc. 2014;26 01:105–115. doi: 10.1111/den.12205. [DOI] [PubMed] [Google Scholar]
- 16.Yoshida N, Hisabe T, Hirose R et al. Improvement in the visibility of colorectal polyps by using blue laser imaging. Gastrointest Endosc. 2015;82:542–549. doi: 10.1016/j.gie.2015.01.030. [DOI] [PubMed] [Google Scholar]
- 17.Sun X, Dong T, Bi Y et al. Linked color imaging application for improving the endoscopic diagnosis accuracy: a pilot study. Sci Rep. 2016;6:33473. doi: 10.1038/srep33473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yamashina T, Takeuchi Y, Uedo N et al. Diagnostic features of sessile serrated adenoma/polyps on magnifying narrow band imaging: a prospective study of diagnostic accuracy. J Gastroenterol Hepatol. 2015;30:117–123. doi: 10.1111/jgh.12688. [DOI] [PubMed] [Google Scholar]
- 19.Participants in the Paris workshop The Paris endoscopic classification of superficial neoplastic lesions: Esophagus, stomach, and colon-November 30 to December 1, 2002 Gastrointest Endosc 200358(Suppl)S3–S43. [DOI] [PubMed] [Google Scholar]
- 20.Yoshida N, Naito Y, Murakami T et al. Safety and efficacy of a same-day low-volume 1 L PEG bowel preparation in colonoscopy for the elderly people and people with renal dysfunction. Dig Dis Sci. 2016;61:3229–3235. doi: 10.1007/s10620-016-4262-7. [DOI] [PubMed] [Google Scholar]
- 21.Hamilton SR, Aaltonen LA, eds. World Health Organization classification of tumors . Lyon, France: IARC Press; 2010. Pathology and genetics of tumours of the digestive system; pp. 104–109. [Google Scholar]
- 22.Dohi O, Yagi N, Onozawa Y et al. Linked color imaging improves endoscopic diagnosis of active Helicobacter pylori infection. Endosc Int Open. 2016;4:E800–805. doi: 10.1055/s-0042-109049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Froehlich F, Wietlisbach V, Gonvers J J et al. Impact of colonic cleansing on quality and diagnostic yield of colonoscopy: the European Panel of Appropriateness of Gastrointestinal Endoscopy European multicenter study. Gastrointest Endosc. 2005;6:378–384. doi: 10.1016/s0016-5107(04)02776-2. [DOI] [PubMed] [Google Scholar]
- 24.Harewood G C, Sharma V K, de Garmo P. Impact of colonoscopy preparation quality on detection of suspected colonic neoplasia. Gastrointest Endosc. 2003;58:76–79. doi: 10.1067/mge.2003.294. [DOI] [PubMed] [Google Scholar]
- 25.Ogiso K, Yoshida N, Siah K TH et al. New generation narrow band imaging improves visibility of polyps: a colonoscopy video evaluation study. J Gastroenterol. 2016;51:883–890. doi: 10.1007/s00535-016-1167-3. [DOI] [PubMed] [Google Scholar]