

Adolescents and young adults (AYA) diagnosed with cancer between 15 and 39 years of age have poor survival when compared with patients diagnosed during childhood (1 to 14 years old). They also have not seen the same improvement in survival – leaving an AYA Gap.(1) In light of this phenomenon, the National Cancer Institute (NCI) has deemed AYAs a vulnerable population. Hodgkin Lymphoma (HL) represents a prototypical AYA malignancy, with incidence peaking between 20 and 25 years; furthermore, the improvements in childhood HL survival have not been seen in AYAs.(1, 2) While previous studies have examined the impact of race/ethnicity, socioeconomic status (SES) and insurance on survival,(1–8) health care delivery remains unstudied in HL AYAs. In particular, aspects of cancer care delivery such as supportive care, multidisciplinary decision-making and therapy delivery mechanisms remain unstudied. This is further complicated by the fact that there is no validated, systematic and widely-available measure that captures cancer care delivery at a granular level.(9, 10)
In order to evaluate currently-unmeasurable aspects of health care delivery, we used care at NCI-designated Comprehensive Cancer Centers (CCC; or Children’s Oncology Group [COG] for patients <21y) to serve as a surrogate. We also investigated barriers and facilitators to access to CCC/COG facilities for AYAs with HL.
We constructed a population-based cohort of 1,094 patients with newly-diagnosed HL between the ages of 1 and 39 years, using the Los Angeles (LA) County cancer registry (Cancer Surveillance Program [CSP]). Patients were eligible for inclusion if they were diagnosed between 1998 and 2008, both living in and receiving treatment in LA County. CSP is a member of the NCI-funded Surveillance, Epidemiology and End Results program.(11) This project was approved by the State of California’s Committee for the Protection of Human Subjects and the institutional review boards of City of Hope and the University of Alabama at Birmingham.
ICDO-3 histology codes were used to identify cases, and the CSP collaborative staging schema was employed for staging.(11) Nodular lymphocyte predominant HL was excluded due to small numbers (n=41). Similar to other diseases examined by our group with this approach,(12, 13) we assigned patients to the facility where they received all or part of the first course of treatment after systematically examining the facility associated with each episode of care in the registry. We considered patients treated at CCC/COG if: (1) at any age they were cared for at one of three CCCs in LAC (UCLA/Jonsson, USC/Norris/CHLA or City of Hope) or (2) at ≤21 years they were cared for at one of three COG sites without CCC designation (Kaiser Permanente, Harbor-UCLA, or Cedars-Sinai). All other patients were considered to have received care at non-CCC/COG sites. CSP provided each patient’s residential address at diagnosis. After geocoding hospital addresses, we used Geographic Information Systems (GIS) to measure straight line distance between the patient residence and nearest CCC/COG [ArcMap 10.2, esri, Redlands, CA].
To calculate overall survival, Kaplan-Meier survival analysis was used. Hazard ratio (HR) of mortality and associated 95% confidence interval (CI) was calculated using Cox regression analyses. Multivariable regression was stratified by treatment site and the results in Table 1 depict stepwise model-building. Payor and SES were collinear in predicting overall survival, therefore a combination variable was created; patients with private insurance and high SES served as the referent group, and were compared to all others. Logistic regression was used to model predictors of receiving care at a CCC/COG. Odds ratios (OR) with 95% CI represented the magnitude of association for each predictor. We examined the facilitators/barriers to CCC/COG care stratified by age (1–21 and 22–39 years) due to payor-driven access to healthcare (equal in California for all patients 21 years and younger). Because payor and SES were not collinear in predicting care by treatment site, they were included separately in the multivariable model. Two-sided tests with p<0.05 were considered statistically significant. SAS 9.3 (SAS Institute, Cary, NC) was used for all analyses.
Table 1.
Risk of All-cause mortality in Hodgkin Lymphomaa: Multivariable Analysis Stratified by Treatment Site (CCC/COGb vs. Non-CCC/COG Facilities)
| Age Group | Gender | Stage | Race/Ethnicity e | Insurance + Socioeconomic Status (SES) | Treatment Site | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1–29y | 30–39y | Female | Male | Localized | Regional | Remote | NHW | AA/Hisp | API | Private + High SES | Public/None + Mid/Low SES | CCC/COG | Non-CCC/COG | ||
| Treated at NCI-Designated Comprehensive Cancer Center or Children’s Oncology Group site | |||||||||||||||
| Model 1 | HR (95%CI) |
1.0 | 0.7 (0.1–5.9) |
1.0 | 2.6 (0.5–13.3) |
1.0 | 0.4 (0.1–2.4) |
0.1 (0.01–1.5) |
|||||||
| p-value | – | 0.7 | – | 0.3 | – | 0.3 | 0.1 | ||||||||
| Model 2 | HR (95%CI) |
1.0 | 0.7 (0.1–7.9) |
1.0 | 2.6 (0.5–13.5) |
1.0 | 0.5 (0.1–2.5) |
0.2 (0.01–1.7) |
1.0 | 1.1 (0.2–5.8) |
– e | ||||
| p-value | – | 0.8 | – | 0.3 | – | 0.4 | 0.1 | – | 0.9 | – | |||||
| Model 3 | HR (95%CI) |
1.0 | 0.7 (0.1–7.2) |
1.0 | 2.6 (0.5–13.7) |
1.0 | 0.5 (0.1–2.6) |
0.2 (0.01–1.7) |
1.0 | 1.1 (0.2–5.8) |
– e | 1.0 | 0.6 (0.1–4.2) |
||
| p-value | – | 0.8 | 0.3 | – | 0.4 | 0.1 | – | 0.9 | – | – | 0.6 | ||||
| Not Treated at NCI-Designated Comprehensive Cancer Center or Children’s Oncology Group site | |||||||||||||||
| Model 1 | HR (95%CI) |
1.0 |
2.1 (1.4–3.3) |
1.0 |
2.0 (1.2–3.1) |
1.0 | 0.9 (0.4–2.0) |
2.1 (1.0–4.3) |
|||||||
| p-value | – | <0.001 | – | 0.005 | – | 0.8 | 0.04 | ||||||||
| Model 2 | HR (95%CI) |
1.0 |
2.1 (1.4–3.4) |
1.0 |
2.0 (1.3–3.2) |
1.0 | 1.0 (0.5–2.2) |
2.3 (1.1–4.6) |
1.0 |
1.7 (1.1–2.6) |
0.5 (0.1–1.9) |
||||
| p-value | – | <0.001 | – | 0.003 | – | 1.0 | 0.03 | – | 0.03 | 0.3 | |||||
| Model 3 | HR (95%CI) |
1.0 |
2.2 (1.4–3.4) |
1.0 |
2.0 (1.3–3.2) |
1.0 | 1.0 (0.5–2.2) |
2.3 (1.1–4.6) |
1.0 |
1.6 (1.0–2.5) |
0.5 (0.1–1.9) |
1.0 | 1.2 (0.6–2.5) |
||
| p-value | – | <0.001 | 0.004 | – | 1.0 | 0.03 | – | 0.05 | 0.3 | – | 0.6 | ||||
Cox regression multivariable analysis adjusted for variables denoted above in addition to lymphoma stage and gender.
CCC/COG: NCI-Designated Comprehensive Cancer Center or Children’s Oncology Group site
Hazard Ratios (HR) with 95% Confidence Intervals (CI).
Bolded values represent statistically significant findings, p<0.05
Patients of all race/ethnicity categories were included in analyses performed on the full cohort as well as the stratified analysis performed in non-CCC/COG patients; API patients were excluded from the CCC/COG stratified analysis as there were no events at CCC/COG sites for these patients (n=12).
The majority of the 1,094 newly-diagnosed HL patients were AYAs (88%). The distribution of patients by stage was comparable across CCC/COG and non-CCC/COG sites (p=0.9). CCC/COG sites saw a higher proportion of patients who were publicly insured (p=0.03) and in the highest SES group (p=0.01). Patients treated at CCC/COGs lived closer to a CCC/COG (p<0.001). [Supplementary Table 1]
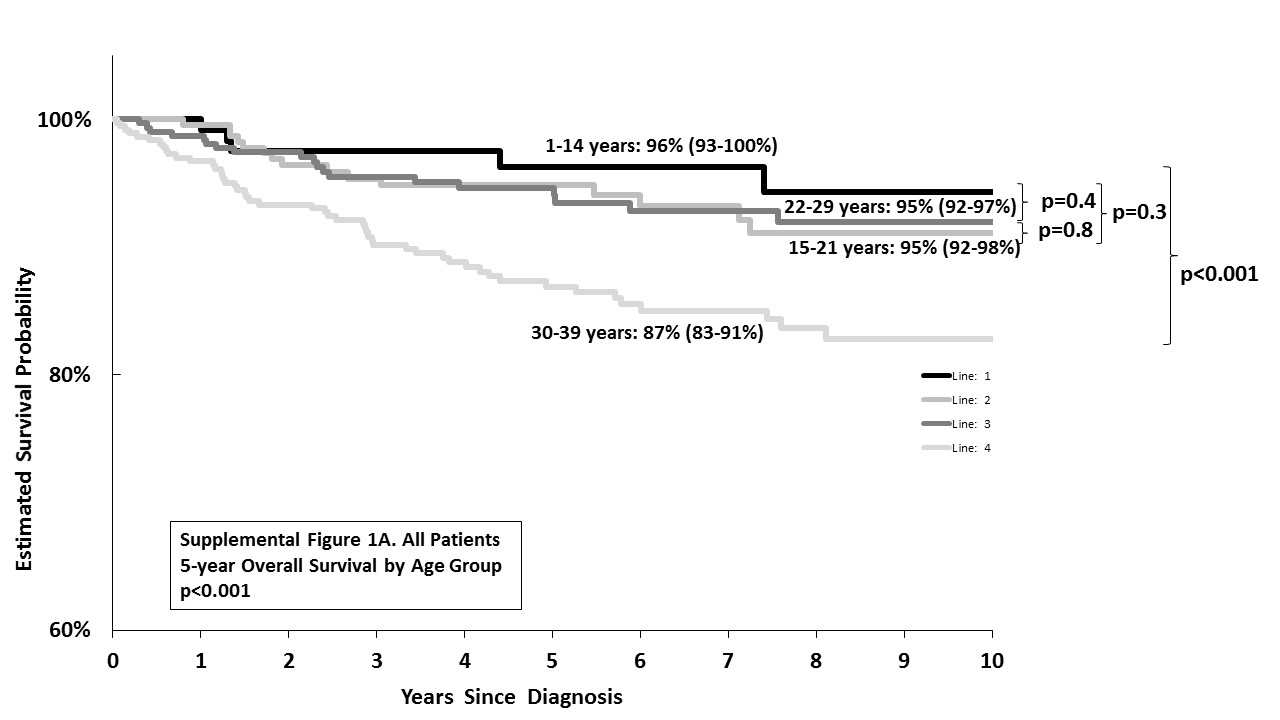
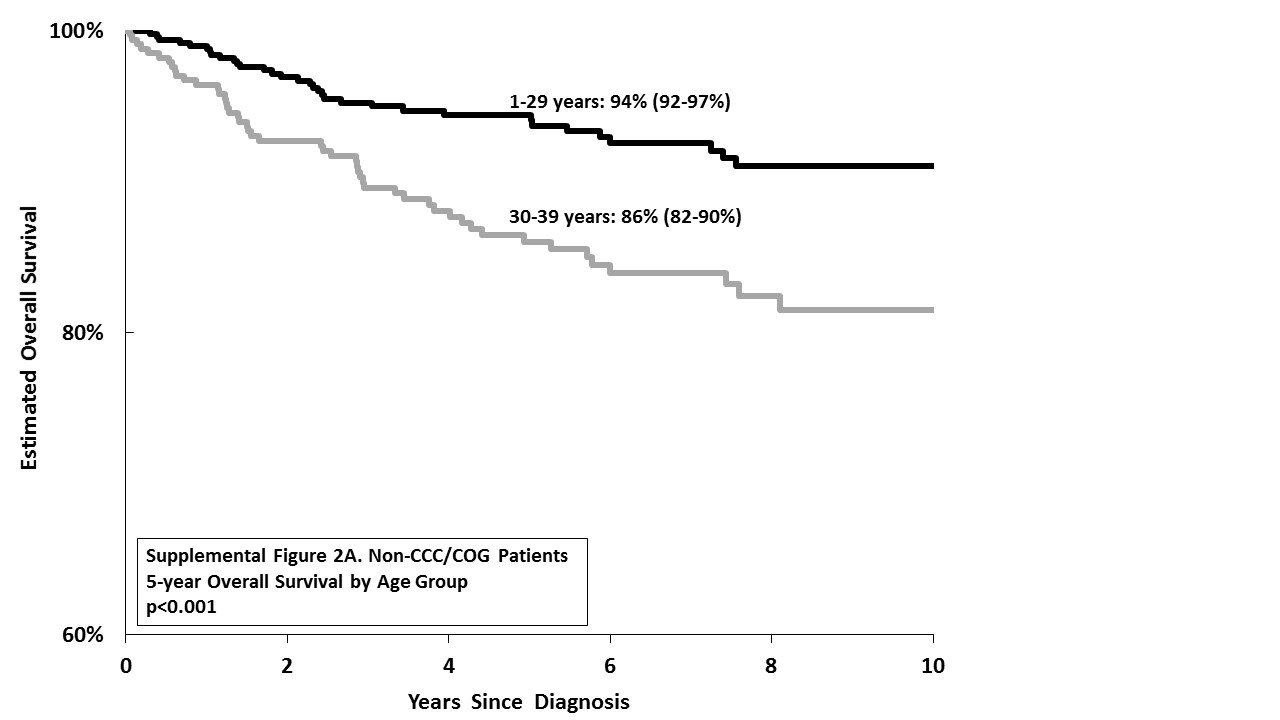
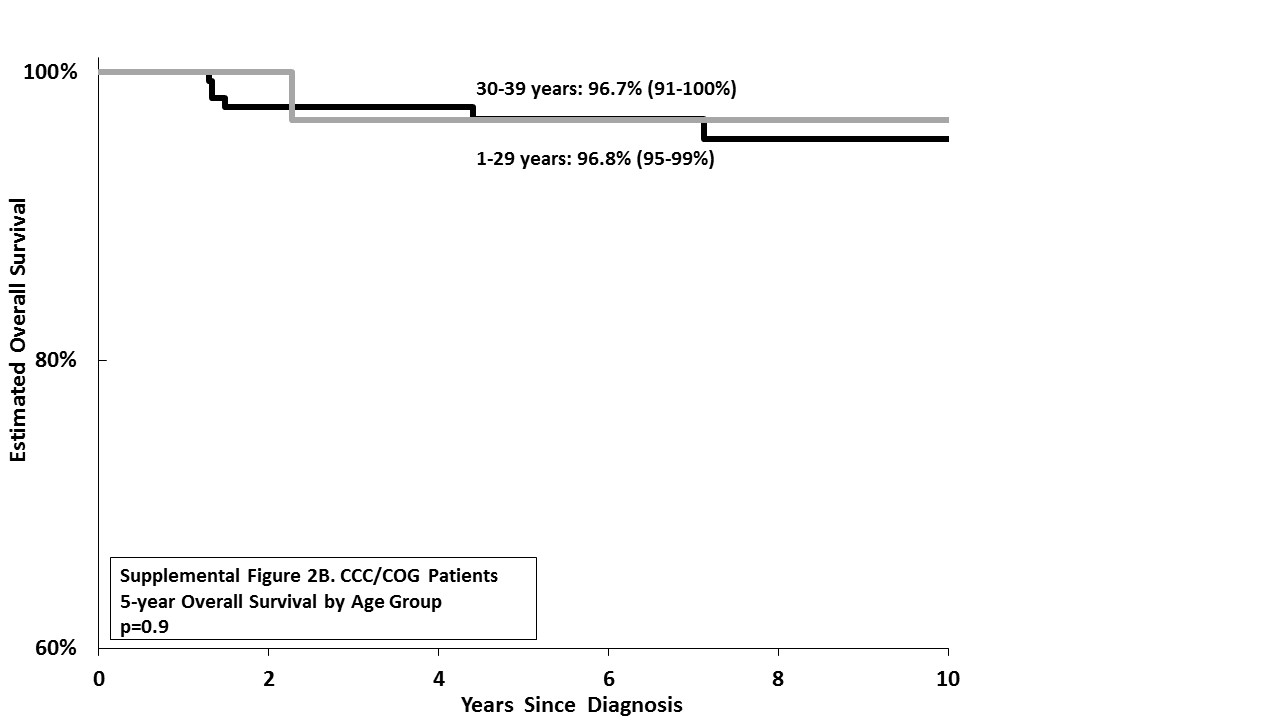
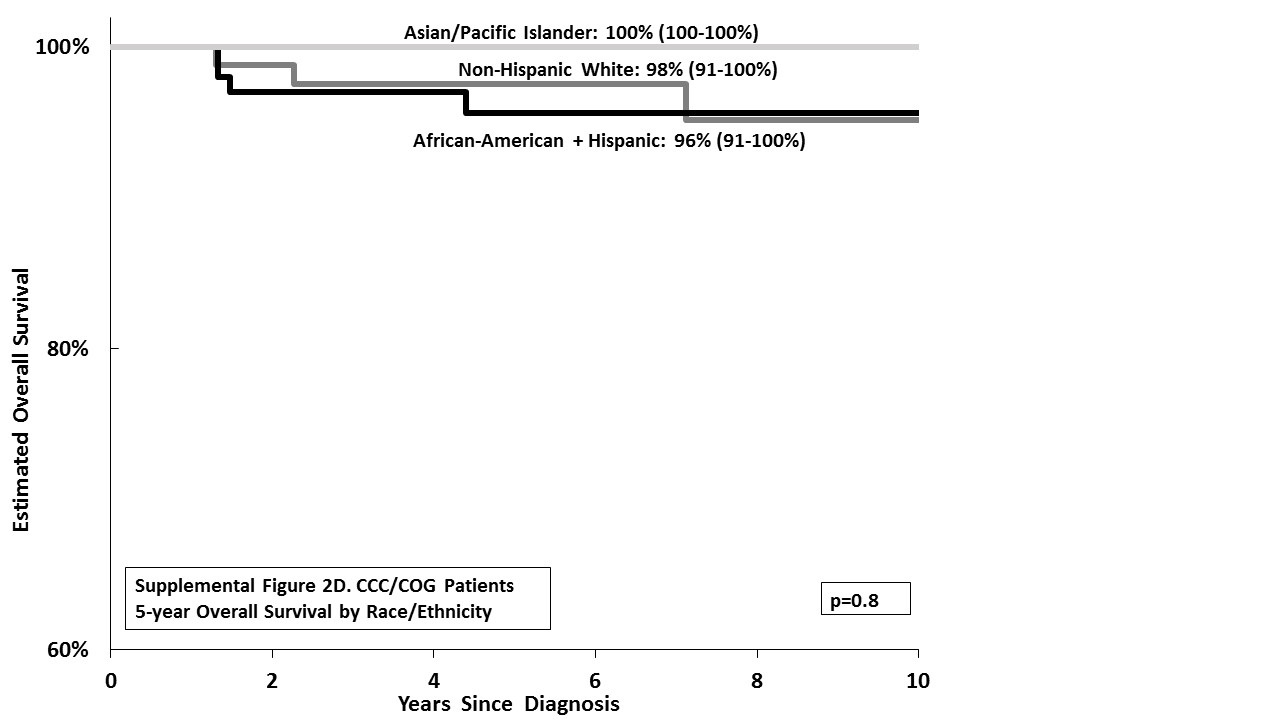
The 5-year overall survival was comparable between children (1–14 years: 96%, 95%CI, 93–100%) and younger AYAs (15–21 years: 95%, 95%CI, 92–98%, p=0.3; 22–39 years: 95%, 95%CI, 92–97%, p=0.4), but significantly inferior among older AYAs (30–39 years: 87%, 95%CI, 83–91%; p<0.001). This allowed us to combine the children and younger AYAs into a single group for all subsequent analyses; older AYAs (30–39 years) experienced an inferior outcome as compared to all younger patients combined (1–29 years: 95%, 95%CI, 93–97%, p<0.001). [Supplementary Figure 1] This inferior outcome in older AYAs persisted when they were treated at non-CCC/COG sites (30–39 years: 86%, 95%CI, 82–90% vs. 1–29 years: 94%, 95%CI, 92–97%; p<0.001), but not when they were treated at CCC/COG sites (30–39 years: 96.7%, 95%CI, 91–100% vs. 1–29 years: 96.8%, 95%CI, 95–99%; p=0.9). Finally, overall survival differed by race/ethnicity (Asian/Pacific-Islander (API): 97%, 95%CI, 92–100%; NHWs: 96%, 95%CI, 93–98%; and African-American/Hispanics: 89%, 95%CI, 89–95%; p=0.03). However while these racial/ethnic differences in outcome held true at non-CCC/COG sites (API: 96%, 95%CI, 91–100%; NHW: 95%, 95%CI, 93–98%; African-American/Hispanics: 90%, 95%CI, 87–94%, p=0.03), there were no statistically significant racial/ethnic differences in overall survival at CCC/COG sites (API: 100%; NHW: 98%, 95%CI, 91–100%; African-American/Hispanic: 96%, 95%CI, 91–100%, p=0.8). [Supplementary Figure 2]
Table 1 presents a series of multivariable models stratified by treatment site. Model 1 examined the impact of age at diagnosis on survival, adjusting for sex and stage. Model 2 examined the impact of race/ethnicity, adjusting for variables in Model 1. Model 3 examined the impact of SES/payor, adjusting for variables in Model 2.
With respect to age at diagnosis, we observed a 2.2-fold higher risk of mortality for 30–39 year-olds (p<0.001; referent group: 1–29 years) among those not treated at CCC/COG sites, after adjusting for all clinical and sociodemographic variables. However, those treated at CCC/COG sites did not demonstrate any difference in mortality by age (HR=0.7, p=0.8; referent group 1–29 years).
Regarding race/ethnicity, African-American/Hispanics were at a 1.7-fold higher risk of mortality when compared with NHW (p=0.03) among those not treated at CCC/COG sites (Model 2: after adjusting for age at diagnosis, sex and stage). Adjusting for SES/payor status did not alter these findings. However, for those treated at CCC/COG sites, after adjusting for the same variables, the risk of mortality was comparable between African-American/Hispanics and NHWs (HR=1.1, p=0.9; Models 2 and 3).
Insurance/SES did not have an impact on mortality, among either those treated at the CCC/COG (p=0.6) or those at non-CCC/COG sites (p=0.6).
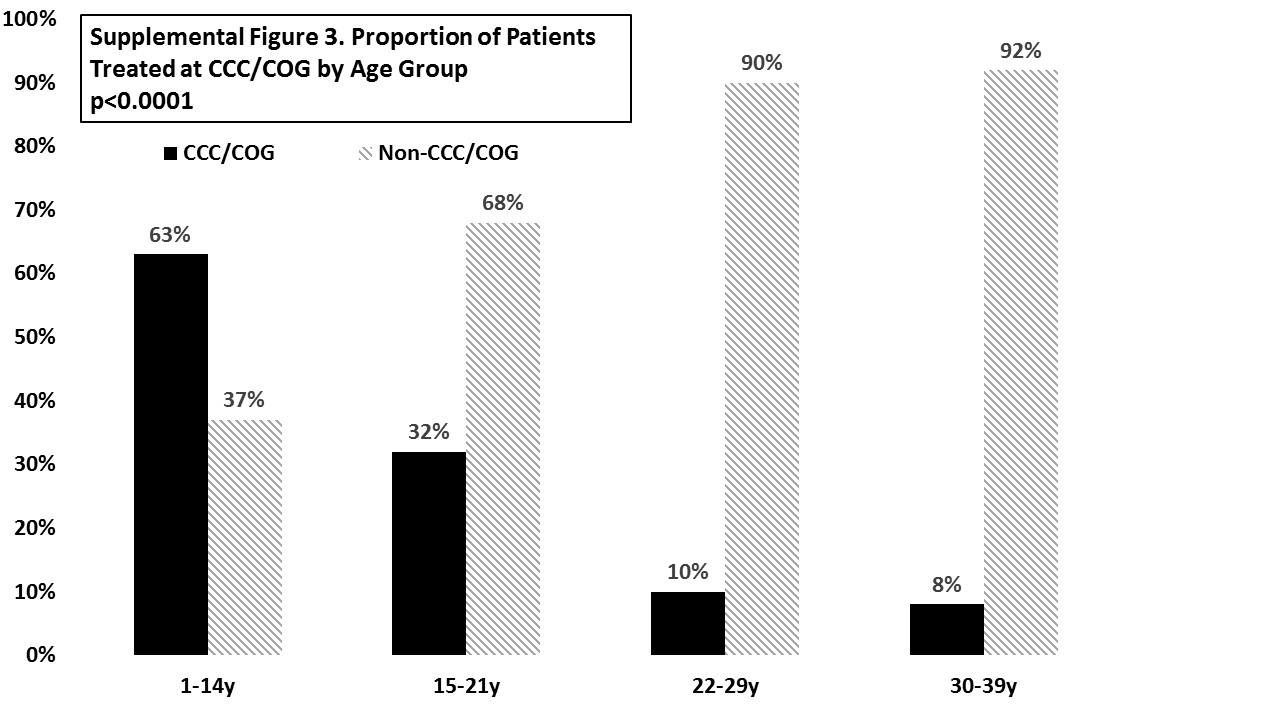
In examining predictors of care at CCC/COG sites, a higher proportion of children with HL were treated at CCC/COG (1–14y: 63%) as compared to 15–21 year-olds (32%), 22–29 year-olds (10%) or 30–39 year-olds (8%, p<0.0001). [Supplemental Figure 3] Table 2 presents findings from multivariable models which explored the predictors of being treated at CCC/COG sites, stratified by age at diagnosis of HL (≤21 vs. 22–39 years).
Table 2.
| ≤ 21 year-olds | 22–39 year-olds | ||||
|---|---|---|---|---|---|
| OR (95% CI) c,d | p-value | OR (95% CI) | p-value | ||
| Age Group | |||||
| ≤14 years | 1.0 | – | 22–29 years | 1.0 | – |
| 15–21 years | 0.2 (0.1–0.4) | <0.001 | 30–39 years | 1.2 (0.7–2.2) | 0.5 |
| Gender | |||||
| Female | 1.0 | – | 1.0 | – | |
| Male | 0.8 (0.5–1.2) | 0.3 | 1.0 (0.6–1.9) | 0.9 | |
| Race/Ethnicity | |||||
| Non-Hispanic White | 1.0 | – | 1.0 | – | |
| African-American/Hispanic | 1.4 (0.8–2.4) | 0.3 | 0.4 (0.2–0.7) | 0.01 | |
| Asian-Pacific Islander | 1.6 (0.5–4.9) | 0.4 | 1.0 (0.4–2.7) | 1.0 | |
| Socioeconomic Status (SES) | |||||
| High | 1.0 | – | 1.0 | – | |
| Middle/Low SES | 0.4 (0.2–0.8) | 0.01 | 0.6 (0.3–1.1) | 0.1 | |
| Insurance | |||||
| Private | 1.0 | – | 1.0 | – | |
| Public/None | 1.6 (1.0–2.7) | 0.07 | 0.6 (0.2–1.5) | 0.3 | |
| Distance from nearest age-appropriate CCC/COG sites | |||||
| ≤10 miles | 1.0 | – | 1.0 | – | |
| >10 miles | 0.7 (0.4–1.2) | 0.2 | 0.4 (0.2–0.8) | 0.01 | |
Logistic Regression, adjusted for all variables including lymphoma stage
CCC/COG: NCI-Designated Comprehensive Cancer Center or Children’s Oncology Group site
Odds Ratios (OR) with 95% Confidence Intervals (CI)
Bolded values: statistically significant, p<0.05
Among ≤21 year-olds, older age (15–21 years: OR=0.2, p<0.001) and lower SES (mid/low SES: OR=0.4, p=0.01) predicted lower odds of treatment at a CCC/COG site. Patients who were ≤21 years with public or no insurance trended towards a higher odds of receiving treatment at CCC/COG sites but this did not reach statistical significance. Distance did not predict treatment site in younger patients. [Table 2]
Among patients >21 years at diagnosis, race/ethnicity (African-American/Hispanic: OR=0.4, p=0.02) and living >10 miles from the nearest CCC/COG site (OR=0.4, p=0.01) predicted lower odds of treatment at such a site. [Table 2]
In summary, older AYAs (30–39 years) and patients from African-American or Hispanic backgrounds with newly-diagnosed HL experience inferior survival when compared with younger or non-Hispanic white patients. Importantly, treatment at CCC/COG can mitigate these outcome disparities. We identify potential barriers to receiving treatment at a CCC/COG facility in both younger patients (AYA age and lower SES) and older AYAs (African-American/Hispanic race/ethnicity and living further from the nearest CCC/COG site).
Using a system-level approach, we generate novel hypotheses in AYAs with HL that build upon previously described disparities.(2–8, 14) We use a surrogate measure (CCC/COG) which includes aspects of supportive care, multidisciplinary decision-making and therapy delivery mechanisms, all components of the NCI comprehensiveness designation(15) – the best possible option in the absence of a granular, validated measure.(10)
These population-level findings indicate that poor survival in older AYAs (30–39 years) and African-American/Hispanic patients with HL can be mitigated by treatment at CCC/COGs. These results highlight a prevailing need to address health care delivery in cancer, specifically in AYAs and patients facing barriers to access (lower SES; underrepresented minorities; living further from specialized care).
Supplementary Material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgments
This work was supported by the National Institutes of Health (K12CA001727) and the St. Baldrick’s Foundation (JW) and includes work performed in the Survey Research Core supported by the National Cancer Institute (P30CA33572).
Footnotes
Presented in abstract form: Annual meeting of the American Society of Hematology, San Francisco, CA, December 2014
Supplementary information is available at Leukemia’s website.
DISCLOSURES OF CONFLICTS OF INTEREST: The authors have no relevant conflicts of interest to disclose.
References
- 1.Bleyer A, O’Leary M, Barr R, Ries L, editors. Cancer Epidemiology in Older Adolescents and Young Adults 15 to 29 Years of Age, Including SEER Incidence and Survival: 1975–2000. Bethesda, MD: NIH Pub. No. 06-5767; 2006. [Google Scholar]
- 2.Kahn JM, Keegan THM, Tao L, Abrahão R, Bleyer A, Viny AD. Racial disparities in the survival of American children, adolescents, and young adults with acute lymphoblastic leukemia, acute myelogenous leukemia, and Hodgkin lymphoma. Cancer. 2016;122(17):2723–30. doi: 10.1002/cncr.30089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Keegan THM, Clarke CA, Chang ET, Shema SJ, Glaser SL. Disparities in Survival after Hodgkin Lymphoma: A Population-Based Study. Cancer Causes & Control. 2009;20(10):1881–92. doi: 10.1007/s10552-009-9382-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shenoy P, Maggioncalda A, Malik N, Flowers CR. Incidence Patterns and Outcomes for Hodgkin Lymphoma Patients in the United States. Advances in Hematology. 2011;2011 doi: 10.1155/2011/725219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Puckett Y, Ta A. Socioeconomic Factors Impact Inpatient Mortality in Pediatric Lymphoma Patients. Cureus. 2016;8(5):e624. doi: 10.7759/cureus.624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rosenberg AR, Kroon L, Chen L, Li CI, Jones B. Insurance status and risk of cancer mortality among adolescents and young adults. Cancer. 2015;121(8):1279–86. doi: 10.1002/cncr.29187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Parikh RR, Grossbard ML, Harrison LB, Yahalom J. Impact of delays in definitive treatment on overall survival: a National Cancer Database study of patients with Hodgkin lymphoma. Leukemia & lymphoma. 2016;57(5):1074–82. doi: 10.3109/10428194.2015.1094696. [DOI] [PubMed] [Google Scholar]
- 8.Keegan TH, DeRouen MC, Parsons HM, Clarke CA, Goldberg D, Flowers CR, et al. Impact of Treatment and Insurance on Socioeconomic Disparities in Survival after Adolescent and Young Adult Hodgkin Lymphoma: A Population-Based Study. Cancer Epidemiol Biomarkers Prev. 2016;25(2):264–73. doi: 10.1158/1055-9965.EPI-15-0756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Laura L, Erin B, Sharyl N, Patricia AG, editors. Delivering High-Quality Cancer Care: Charting a New Course for a System in Crisis. The National Academies Press; 2013. [PubMed] [Google Scholar]
- 10.Hewitt M, Simone JV, editors. Ensuring Quality Cancer Care. The National Academies Press; 1999. [PubMed] [Google Scholar]
- 11.USC KSoMo. CSPedia - Los Angeles Cancer Surveillance Program: User’s Guide to Data Elements 2007. [updated 2010. Available from: http://cspedia.usc.edu/whnjs.htm.
- 12.Wolfson JA, Sun CL, Wyatt LP, Hurria A, Bhatia S. Impact of care at comprehensive cancer centers on outcome: Results from a population-based study. Cancer. 2015;121(21):3885–93. doi: 10.1002/cncr.29576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wolfson J, Sun C-L, Kang T, Wyatt L, D’Appuzzo M, Bhatia S. Impact of Treatment Site in Adolescents and Young Adults With Central Nervous System Tumors. Journal of the National Cancer Institute. 2014;106(8) doi: 10.1093/jnci/dju166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Howell DL, Ward KC, Austin HD, Young JL, Woods WG. Access to Pediatric Cancer Care by Age, Race, and Diagnosis, and Outcomes of Cancer Treatment in Pediatric and Adolescent Patients in the State of Georgia. J Clin Oncol. 2007;25(29):4610–5. doi: 10.1200/JCO.2006.07.6992. [DOI] [PubMed] [Google Scholar]
- 15.NCI. NCI-Designated Cancer Centers. 2012 [updated 08/13/2012 Available from: http://www.cancer.gov/researchandfunding/extramural/cancercenters/about.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.