

Abstract
Sufficient sleep duration is crucial for maintaining normal physiological function and has been linked to cancer risk; however, its contribution to lung cancer mortality is unclear. Therefore, we evaluated the relationship between average sleep duration in various age-periods across the adult lifecourse, and risk of lung cancer mortality in Xuanwei, China. An ambidirectional cohort study was conducted in 42,422 farmers from Xuanwei, China. Participants or their surrogates were interviewed in 1992 to assess average sleep hours in the age-periods of 21-30, 31-40, 41-50, 51-60, 61-70, and ≥71 years, which were categorized as ≤7, 8 (reference), 9, and ≥10 hours/day. Vital status was followed until 2011. Sex-specific Cox regression models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CI) for lung cancer mortality in 1994-2011, adjusted for demographic, anthropometric, medical, and household characteristics. J-shaped relationships were found between average sleep duration and lung cancer mortality. The patterns were consistent across sex, age-periods, and fuel usage. Compared to sleeping 8 hours/day on average, ≤7 hours/day was associated with significantly increased HRs ranging from 1.39 to 1.58 in ages ≥41 years in men, and 1.29 to 2.47 in ages ≥51 years in women. Furthermore, sleeping ≥10 hours/day was associated with significantly increased HRs ranging from 2.44 to 3.27 in ages ≥41 year in men, and 1.31 to 2.45 in ages ≤60 years in women. Greater and less than 8 hours/day of sleep in various age-periods may be associated with elevated risk of lung cancer mortality in Xuanwei, China.
Keywords: Lifecourse, sleep duration, lung cancer, mortality, Xuanwei, China
Introduction
Sleep is characterized by recurrent periods of physical inactivity and augmented neurological activity that are essential for maintaining normal physiological function. Deprivation and overabundance of sleep have detrimental effects on hormone levels, metabolism, and immune function (1-10). Furthermore, numerous studies found that insufficient and excess sleep were associated with increased risks of cancer-related and all-cause mortality (11-15). The several studies of sleep duration that focused on lung cancer incidence and mortality in various countries around the world have yielded inconsistent findings (13,15-20). Taken together, results from previous investigations suggests that the intricate relationship between sleep duration and lung cancer incidence and mortality may depend on a variety of factors including sex, age, race/ethnicity, and nationality.
Despite its rapid urbanization, nearly 650 million people in China still live in underdeveloped rural communities (21). Xuanwei is one such region that has attracted the attention of global health researchers, as it possesses the highest rates of lung cancer among never-smokers in the country (22). In Xuanwei, lung cancer diagnosis and mortality occurs relatively earlier than other chronic diseases, with an average age at death from lung cancer of 59-60 years. Therefore, lung cancer mortality constitutes a strong competing risk for death from all other causes, which typically occur later. In comparison, the average age of lung cancer diagnosis is much later at 70 years in the United States (23). The alarming public health burden of lung cancer in Xuanwei has been attributed to indoor air pollution from residential combustion of smoky (bituminous) coal for heating and cooking (24); however, there is still significant variability in lung cancer risk and mortality. Aside from environmental exposures, lifestyle factors such as sleep duration may be important contributors. Despite the established relationships between sleep duration and various health outcomes, no large cohort study to our knowledge has focused on sleep duration across the lifecourse, and its relationship with risk of lung cancer mortality. The Xuanwei Cohort Study of farmers was a unique platform in which to investigate this relationship. Unlike other studies which evaluated sleep duration in a single time frame up, our study used a unique “lifecourse approach” which collected detailed information in various age-periods throughout adulthood in a population with limited circadian disruption. This novel “lifecourse approach” provides further etiologic and public health insight into the induction time of sleep duration on lung cancer mortality. Our study objective was to assess the associations between average sleep duration in various age-periods across the adult lifecourse, and risk of lung cancer mortality in residents of Xuanwei, China.
Materials and Methods
Study Design and Population Sample
Characteristics of the study population were previously described elsewhere (25,26). Briefly, participants were sampled from four communes in rural Xuanwei, China including Rongcheng, Laibin, Jingwai, and Reshui. Local administrative records were used to identify all residents who were born in 1917-1951 and living in the area as of January 1, 1976. Among these residents, 42,422 individuals were available for the study. The participants were predominantly farmers who lived traditional agrarian lifestyles.
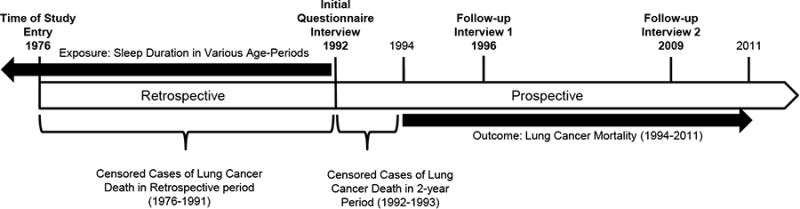
An ambidirectional (incident-prevalent) cohort study was conducted to assess the associations between average sleep hours in various age-periods across the lifecourse and risk of lung cancer mortality. This investigation was initiated as a retrospective cohort study (January 1, 1976 – December 31, 1992) and subsequently extended with two prospective follow-ups in 1996 and 2009-2011 (Figure 1). Standardized questionnaires were administered in 1992 by trained interviewers to all participants. Interviews were directly conducted when feasible (59%), whereas surrogate (next-of-kin and close friends) respondents were interviewed when individuals were deceased or not present in 1992 (41%). The interviewers collected retrospective information on average time spent sleeping in various age-periods across the lifecourse, demographic factors, residential history, lifetime use of household stove and fuel type, occupational history, past and current active smoking, cooking practices, time spent indoors and outdoors, medical history, and family history of lung cancer and other chronic diseases. Prospective follow-ups were subsequently conducted in 1996 and 2009-2011. Among participants who were alive in 1992, there was only 6% attrition in 2009-2011. Only baseline covariate data from interviews/questionnaires conducted in 1992 were used in this analysis.
Figure 1. Timeline of the Ambidirectional Incident-Prevalent Cohort Study of Farmers in Xuanwei, China.
This study was approved by the Institutional Review Board of the Chinese Academy of Preventive Medicine. Signed informed consent was obtained from all literate respondents. Study procedures were orally explained to each illiterate individual in the presence of a literate relative. If the individual provided oral consent, the relative signed the consent form as a surrogate. The National Institutes of Health Office of Human Subjects Research (OHSR) determined that federal regulations for the protection of human subjects do not apply to this secondary analysis (Exemption #5213).
Exposure Assessment: Average Sleep Hours Across the Lifecourse
Retrospective sleep data from six age-periods were collected in 1992 via questionnaires or interviews. Participants or their surrogates were asked the average number of sleep hours in the age-periods of 21-30, 31-40, 41-50, 51-60, 61-70, and ≥71 years. In total, 59% of participants reported their own average sleep hours while 41% were reported by surrogates. Among those alive in 1992, 75% of participants reported their own sleep hours, while the rest was reported by surrogates. Only sleep data from interviews/questionnaires conducted in 1992 were used in this study because age-period specific sleep data were not collected during the follow-ups in 1996 and 2009-2011.Outcome Assessment: Lung Cancer Mortality
The outcome of interest was time to death due to lung cancer starting on January 1, 1976. The calendar dates and causes of all deaths in the retrospective and prospective study periods (1976-2011) were extracted from death records. The causes of death were coded by the Xuanwei Center for Disease Control according to ICD-9 (International Classification of Diseases, 9th revision). Death attributed to lung cancer was designated ICD-9 code: 162.Analysis
Multivariable-adjusted sex-specific Cox regression models were used to estimate hazard ratios (HR) and 95% confidence intervals (CIs) for lung cancer mortality, in relation to average sleep hours in various age-periods and potential confounders. The cause-specific Cox models accounted for censoring from competing risks from loss to follow-up and death from all other causes, while the timescale was attained age (years lived). Proportional hazards assumptions were assessed using Supremum tests and interaction terms between explanatory variables and time (27). Effect modification was assessed by including interaction terms with sleep duration.
In the primary analysis, the exposure of interest was average sleep hours in six age-periods including: 21-30, 31-40, 41-50, 51-60, 61-70, and ≥71 years, as specified in the interviews/questionnaires. Average sleep hours were integers and categorized as ≤7, 8 (reference), 9, and ≥10 hours/day. The reference of 8 hours/day was chosen based on the distribution of sleep data in each age-period and because 7-9 hours/day was the recommended duration (depending on age) of the American Academy of Sleep Medicine and Sleep Research Society (28). We also conducted sensitivity analyses using 8-9 hours/day as the reference group, as 9 hours/day was the upper recommended sleep duration. Trend tests for linearity were conducted by fitting average sleep hours as ordinal categories in the Cox models. Non-linear J-shaped trends were considered noteworthy if ≤7 hours/day was significantly associated with increased risk, together with monotonically increasing risks with 9 and ≥10 hours/day. Separate Cox models were fitted for average sleep hours in each age period as main effects (six separate models). Additionally, separate analyses were conducted for men and women because most men were smokers, while the women were almost exclusively non-smokers, in addition to having occupational and lifestyle differences.
In men, the Cox models were adjusted for: average hours spent performing indoor activities in the same age-period as sleep (counts), type of respondent (self, surrogate), other work besides farming (yes, no), educational attainment (illiterate, primary school, middle/vocational school or higher), ever active smoking (yes, no), duration of smoking (years), ethnicity (Han Chinese, other), average number of rooms and people in residences from 1976-1992 (continuous), fuel type used in first residence (smoky coal, smokeless coal, other), installation of a chimney for ventilation (stove improvement) (yes, no), family history of any cancer (yes, no), average tons of fuel/coal used from 1976-1992 (continuous), ever employed as a miner (yes, no), age in 1976 (birth cohort; years), and an indicator variable for history of respiratory comorbidities (asthma, emphysema, chronic bronchitis, and/or chronic obstructive pulmonary disorder). In women, duration of smoking, ever smoking, and ever employed as a miner were removed due to lack of variability, while age at which one began cooking (years) was included. Covariates were chosen based on previous literature, causal criteria for confounders (29,30), and if they changed the estimates by >10%.
Sensitivity analyses were performed that included: 1) counting only incident cases occurring in 1994-2011 as events, while censoring cases occurring in 1976-1993 (primary analyses, Figure 1), 2) counting only incident cases occurring in 1992-2011 as events, while censoring prevalent cases occurring in 1976-1991, and 3) counting all cases in 1976-2011 as events. Censoring prevalent cases in 1976-1991 and incident cases in the first two years of the prospective follow-up (1992-1993) was intended to mitigate potential reporting-bias of sleep hours due to undiagnosed disease during the retrospective period, and surrogate reported data from those who died before 1992. Additional sensitivity analyses included: 4) restricting to participants who were alive in 1992 and self-reported their own sleep data, excluding those who died before data collection and surrogate reporting (prospective cohort analyses), and 5) restricting to participants who ever-used smoky coal prior to 1992, and further stratified by average tons of coal use (dichotomized using the median of 3.3 tons).
Non-linear relationships between average sleep duration in each age-period and risk of lung cancer mortality in 1994-2011 were assessed by fitting restricted cubic splines in the multivariable-adjusted Cox models, using previously described methods (31). Knots were placed at 6, 7, 8, 9, and 10 hours/day, while sleeping 8 hours/day was used as the reference (nadir).
Inflated family-wise error rate was accounted for using Bonferroni-corrected significance thresholds. P-values <0.05 were considered statistically noteworthy, while p-values below a Bonferroni-corrected α-level of 0.0028 (0.05/18 tests from 6 age-periods × 3 categories of sleep duration) were considered statistically significant. All analyses were performed using SAS v9.3 (SAS Institute Inc., Cary, NC, USA).
Results
Characteristics of the Study Population
The study population consisted of 21,701 men and 20,721 women, mostly of Han Chinese ethnicity (97%) (Table 1). The average age in 1976 was 39 years. Most participants were born in 1917-1936 (47%), 26% were born in 1937-1945, and 27% were born in 1946-1951. The male participants were predominantly ever-smokers (92.2%), whereas a miniscule proportion of women had ever-smoked (0.3%). Most men were illiterate (54.1%) and only 8.7% had an educational attainment higher than middle/vocational school. The proportion of illiteracy was even higher among women (76.7%). A significant proportion of men worked in other professions besides farming (22.2%) and 5.1% worked as miners. The average age at which women started cooking was 18.3 (SD 3.7) years. Of the men who reported that they cooked (8.5%), the average age at which they started was much later at 27.8 (SD 14.7) years.
Table 1. Study Population Characteristics of the Xuanwei Cohort Study (1976-2011).
| Men | Women | |||
|---|---|---|---|---|
|
|
||||
| n=21701 | n=20721 | |||
| Age in 1976, years, Mean, SD | 39.5 | 10.6 | 39 | 10.6 |
| Birth Cohort, n, % | ||||
| 1917-1936 | 10285 | 47.4 | 9529 | 46 |
| 1937-1945 | 5710 | 47.4 | 5267 | 25.4 |
| 1946-1951 | 5706 | 47.4 | 5925 | 28.6 |
| Ever Actively Smoked (≤ 1992), n, % | 20010 | 47.4 | 61 | 0.3 |
| Duration of Active Smoking, years, Mean, SD | 31.1 | 47.4 | - | - |
| n=21686 | ||||
| Respondent, n, % | ||||
| Self | 12624 | 58.2 | 12519 | 60.4 |
| Surrogate | 9077 | 41.8 | 8202 | 39.6 |
| Ethnicity, n, % | ||||
| Han Chinese | 21122 | 97.3 | 20116 | 97.1 |
| Other | 579 | 2.7 | 605 | 2.9 |
| Education, n, % | ||||
| Illiterate | 11748 | 54.1 | 15885 | 76.7 |
| Primary School | 8073 | 37.2 | 4352 | 21 |
| Middle/Vocational School or Higher | 1880 | 8.7 | 484 | 2.3 |
| Other work besides farming (≤ 1992), n, % | 4816 | 22.2 | 1193 | 5.8 |
| Ever worked as a miner (≤ 1992), n, % | 1117 | 5.1 | 28 | 0.1 |
| Age at which started cooking, years, Mean, SD | 27.8 | 14.7 | 18.3 | 3.7 |
| n=1836 | n=20315 | |||
| Average sleep duration (≤ 1992), hours/day, Mean, SD | ||||
| 21-30 years | 8.3 | 0.8 | 8.3 | 0.7 |
| n=21700 | n=20721 | |||
| 31-40 years | 8.1 | 0.7 | 8.1 | 0.7 |
| n=21647 | n=20684 | |||
| 41-50 years | 8 | 0.7 | 8 | 0.7 |
| n=21308 | n=20419 | |||
| 51-60 years | 7.9 | 0.8 | 7.9 | 0.8 |
| n=12590 | n=11527 | |||
| 61-70 years | 7.8 | 1 | 7.8 | 1 |
| n=6184 | n=5698 | |||
| ≥71 years | 7.7 | 1.2 | 7.7 | 1.2 |
| n=1452 | n=1275 | |||
| Average time indoor activities (≤ 1992), hours/day, Mean, SD | ||||
| 21-30 years | 3.3 | 1.3 | 3.5 | 1.3 |
| n=21693 | n=20721 | |||
| 31-40 years | 3.4 | 1.3 | 3.6 | 1.3 |
| n=21639 | n=20682 | |||
| 41-50 years | 3.5 | 1.3 | 3.7 | 1.3 |
| n=21299 | n=20415 | |||
| 51-60 years | 3.7 | 1.3 | 3.9 | 1.4 |
| n=12585 | n=11525 | |||
| 61-70 years | 3.9 | 1.4 | 4 | 1.4 |
| n=6183 | n=5693 | |||
| ≥71 years | 4.2 | 1.5 | 4.3 | 1.5 |
| n=1448 | n=1273 | |||
| Fuel type used in first residence (≤1992), n, % | ||||
| Smoky Coal | 14306 | 65.9 | 13153 | 63.5 |
| Smokeless Coal | 5447 | 25.1 | 4848 | 23.4 |
| Coal Cakes and Others | 1948 | 9 | 2720 | 13.1 |
| Stove improvement (≤ 1992), n, % | 12529 | 58 | 12186 | 59 |
| Average tons of fuel used in residences (≤1992), Mean, SD | 3.2 | 1.2 | 3.2 | 1.2 |
| Average number people in residences (≤1992), Mean, SD | 5.2 | 1.2 | 5.3 | 1.1 |
| Average number of rooms in residences (≤1992), Mean, SD | 1.7 | 0.8 | 1.7 | 0.8 |
| Cases of Lung Cancer Death (1976-1991), n, % | 1094 | 5 | 1064 | 5.1 |
| Cases of Lung Cancer Death (1992-1993), n, % | 164 | 0.8 | 153 | 0.7 |
| Cases of Lung Cancer Death (1994-2011), n, % | 1337 | 6.2 | 1017 | 4.9 |
| Average Age of Death from Lung Cancer (1976-2011), Mean, SD | 60 | 10.2 | 59.2 | 9.9 |
| Family History of Any Cancer (≤ 1992), n, % | 1023 | 4.7 | 710 | 3.4 |
Average sleep duration was comparable for men and women throughout the lifecourse. The average reported sleep duration in the age-period of 21-30 years was 8.3 hours/day, which decreased over time. Among participants who survived to ≥71 years of age, the average reported sleep duration was 7.7 hours/day. The average time spent performing indoor activities in the age-period of 21-30 years was 3.4 hours/day. By ages ≥71 years, the average time spent performing indoor activities increased to 4.2 hours/day.
Most participants lived in a maximum of two residences in their lifetime (53.0%). Among those who moved residences at least once (92.3%), participants lived an average of 25.1±11.4 SD years in their first residence, and 22.1±10.4 SD years in their second residence. Most participants used smoky coal for heating and cooking in their first residence (65.9% for men, 63.5% for women), and most homes had stove improvement performed by 1992 (58% for men, 59% for women). Although 92.3% of participants moved residences at least once, coal type use was highly correlated between residences; 99.6% of people who initially used smoky coal continued its use in their second home. The participants used an average of 3.2 tons of fuel per year in their residences from 1976-1992, whereas ever smoky coal users used an average of 3.3 tons of smoky coal per year. An average of five people lived in participants' residences and there was an average of 1.7 rooms in the dwellings.
There were 2,158 cases of lung cancer-related death in 1976-1991 and 2,671 cases in the prospective follow-up in 1992-2011. In men, there were 2,595 lung cancer related-deaths from 1976-2011 and a crude lung cancer mortality rate of 1.78 (95% CI: 1.71, 1.85) deaths per 1,000 person-years lived (pyl). In women, there were 2,234 lung cancer-related deaths from 1976-2011 and a crude lung cancer mortality rate of 1.60 (95% CI: 1.53, 1.67) deaths per 1,000 pyl. Among those who died of lung cancer between 1976 and 2011, the average age at death was 60.3 (10.2 SD) years for men and 59.4 (10.0 SD) years for women.
Average Sleep Duration in Various Age-periods Across the Adult Lifecourse and Risk of Lung Cancer Mortality
In general, curvilinear relationships were found between average sleep duration and risk of lung cancer mortality (Figure 2). In men, J-shaped relationships were found in the mid to later adult age-periods of 41-50, 51-60, and 61-70 (Table 2). Compared to sleeping 8 hours/day on average, ≤7 hours/day from age 41 to 70 years was associated with significantly increased mortality risks ranging from 1.39 (95% CI: 1.19, 1.63, p<0.0001) to 1.58 (95% CI: 1.23, 2.03, p=0.0004). Sleeping ≥10 hours/day in ages ≥41 years was associated with significantly increased risks ranging from 2.44 (95% CI: 1.91, 3.30, p<0.0001) to 3.27 (95% CI: 2.31, 4.62, p<0.0001). In women, a J-shaped relationship was observed in ages 51-60 years (Table 2). Sleeping ≤7 hours/day in ages ≥51 years was associated with noteworthy increased risks ranging from 1.29 (95% CI: 1.06, 1.57, p=0.0130) to 2.47 (95% CI: 1.13, 5.38, p=0.0233) (Table 2). Sleeping ≥10 hours/day in ages ≤60 years was associated with noteworthy or significantly increased risks ranging from 1.31 (95% CI: 1.03, 1.66, p=0.0262) to 2.45 (95% CI: 1.76, 3.41, p<0.0001).
Figure 2. Curvilinear Relations between Average Sleep Duration in Various Age-Periods and Risk of Lung Cancer Mortality in 1994-2011.
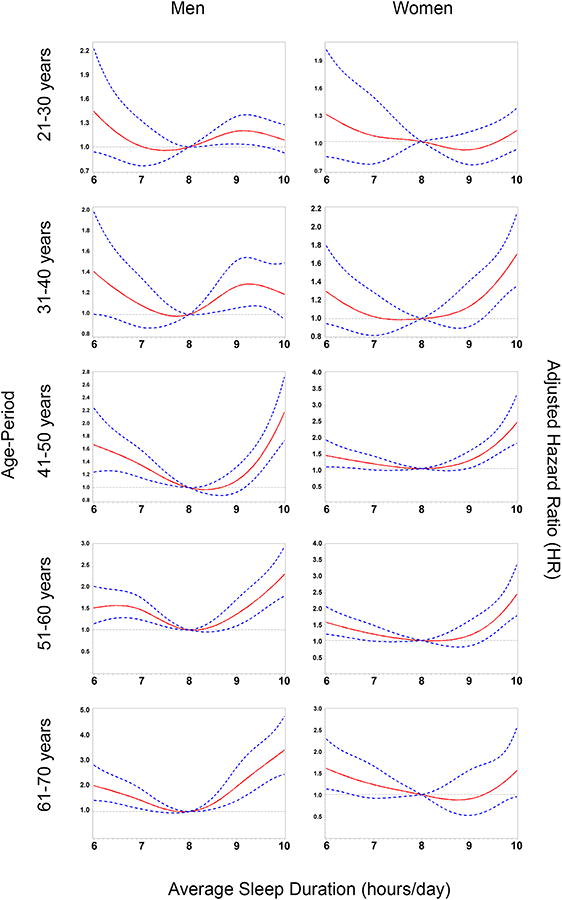
Multivariable adjusted Cox models fitted with restricted cubic splines for sleep hours. Hazard Ratios (HR) (solid red lines). 95% confidence intervals (CI) (dashed blue lines).
Table 2. Average Sleep Duration in Various Age-Periods Across the Adult Lifecourse and Risk of Lung Cancer Mortality in Xuanwei, China (1994-2011).
| Age-Period | MEN | WOMEN | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||||||||||||
| 95% CI | 95% CI | p-value | 95% CI | 95% CI | p-value | ||||||||||||||
| Cases | pyl | n | HR | Lower | Upper | Cases | pyl | n | HR | Lower | Upper | ||||||||
|
|
|
||||||||||||||||||
| 21-30 years | 21-30 years | ||||||||||||||||||
| ≤7 hours/day | 60 | 68423 | 1023 | 1.03 | 0.78 | 1.35 | 0.856 | ≤7 hours/day | 49 | 72421 | 1078 | 1.06 | 0.78 | 1.45 | 0.7095 | ||||
| 8 hours/day | 968 | 1054283 | 15744 | Ref | 8 hours/day | 760 | 1014389 | 15130 | Ref | ||||||||||
| 9 hours/day | 188 | 201693 | 3010 | 1.07 | 0.91 | 1.26 | 0.4016 | 9 hours/day | 117 | 192052 | 2838 | 0.86 | 0.7 | 1.05 | 0.138 | ||||
| ≥10 hours/day | 121 | 130949 | 1923 | 1.19 | 0.98 | 1.45 | 0.0836 | ≥10 hours/day | 91 | 115069 | 1675 | 1.31 | 1.03 | 1.66 | 0.0262 | * | |||
| P-trend (ordinal) | 0.2071 | P-trend (ordinal) | 0.976 | ||||||||||||||||
|
| |||||||||||||||||||
| 31-40 years | 31-40 years | ||||||||||||||||||
| ≤7 hours/day | 109 | 140172 | 2097 | 1.12 | 0.91 | 1.39 | 0.2717 | ≤7 hours/day | 83 | 139278 | 2080 | 1.06 | 0.83 | 1.35 | 0.6304 | ||||
| 8 hours/day | 1004 | 1086846 | 16214 | Ref | 8 hours/day | 773 | 1049743 | 15612 | Ref | ||||||||||
| 9 hours/day | 137 | 145489 | 2149 | 1.25 | 1.04 | 1.49 | 0.017 | * | 9 hours/day | 81 | 128549 | 1900 | 1.17 | 0.93 | 1.49 | 0.1798 | |||
| ≥10 hours/day | 87 | 81325 | 1187 | 1.21 | 0.97 | 1.52 | 0.0989 | ≥10 hours/day | 80 | 75290 | 1092 | 1.72 | 1.34 | 2.22 | <0.0001 | ** | |||
| P-trend (ordinal) | 0.0122 | * | P-trend (ordinal) | 0.0222 | * | ||||||||||||||
|
| |||||||||||||||||||
| 41-50 years | 41-50 years | ||||||||||||||||||
| ≤7 hours/day | 211 | 229143 | 3399 | 1.39 | 1.19 | 1.63 | <0.0001 | ** | ≤7 hours/day | 151 | 230990 | 3428 | 1.18 | 0.98 | 1.42 | 0.0774 | |||
| 8 hours/day | 924 | 1012682 | 14977 | Ref | 8 hours/day | 713 | 971742 | 14364 | Ref | ||||||||||
| 9 hours/day | 127 | 154389 | 2276 | 1.06 | 0.88 | 1.28 | 0.5218 | 9 hours/day | 98 | 141742 | 2079 | 1.26 | 1.01 | 1.56 | 0.0396 | * | |||
| ≥10 hours/day | 75 | 44537 | 656 | 2.44 | 1.91 | 3.12 | <0.0001 | ** | ≥10 hours/day | 51 | 37932 | 548 | 2.45 | 1.76 | 3.41 | <0.0001 | ** | ||
| P-trend (ordinal) | <0.0001 | ** | P-trend (ordinal) | 0.0013 | ** | ||||||||||||||
|
| |||||||||||||||||||
| 51-60 years | 51-60 years | ||||||||||||||||||
| ≤7 hours/day | 197 | 215623 | 3000 | 1.46 | 1.23 | 1.73 | <0.0001 | ** | ≤7 hours/day | 150 | 207399 | 2849 | 1.29 | 1.06 | 1.57 | 0.013 | * | ||
| 8 hours/day | 509 | 564024 | 7813 | Ref | 8 hours/day | 378 | 515564 | 7123 | Ref | ||||||||||
| 9 hours/day | 74 | 91962 | 1263 | 1.29 | 1 | 1.65 | 0.0466 | * | 9 hours/day | 40 | 78370 | 1066 | 1.21 | 0.87 | 1.69 | 0.2607 | |||
| ≥10 hours/day | 61 | 36258 | 513 | 2.51 | 1.91 | 3.3 | <0.0001 | ** | ≥10 hours/day | 50 | 35290 | 489 | 2.4 | 1.73 | 3.33 | <0.0001 | ** | ||
| P-trend (ordinal) | <0.0001 | ** | P-trend (ordinal) | 0.0009 | ** | ||||||||||||||
|
| |||||||||||||||||||
| 61-70 years | 61-70 years | ||||||||||||||||||
| ≤7 hours/day | 109 | 148925 | 1969 | 1.58 | 1.23 | 2.03 | 0.0004 | ** | ≤7 hours/day | 90 | 145649 | 1902 | 1.4 | 1.06 | 1.85 | 0.0188 | * | ||
| 8 hours/day | 166 | 238759 | 3132 | Ref | 8 hours/day | 136 | 220194 | 2870 | Ref | ||||||||||
| 9 hours/day | 49 | 51399 | 671 | 2.12 | 1.52 | 2.95 | <0.0001 | ** | 9 hours/day | 14 | 43418 | 563 | 0.93 | 0.53 | 1.65 | 0.814 | |||
| ≥10 hours/day | 41 | 30971 | 412 | 3.27 | 2.31 | 4.62 | <0.0001 | ** | ≥10 hours/day | 20 | 28076 | 363 | 1.59 | 0.96 | 2.64 | 0.0704 | |||
| P-trend (ordinal) | <0.0001 | ** | P-trend (ordinal) | 0.0194 | * | ||||||||||||||
|
| |||||||||||||||||||
| ≥71 years | ≥71 years | ||||||||||||||||||
| ≤7 hours/day | 16 | 44517 | 555 | 1.62 | 0.81 | 3.26 | 0.1762 | ≤7 hours/day | 25 | 44232 | 538 | 2.47 | 1.13 | 5.38 | 0.0233 | * | |||
| 8 hours/day | 20 | 48244 | 595 | Ref | 8 hours/day | 12 | 41616 | 510 | Ref | ||||||||||
| 9 hours/day | 8 | 13313 | 164 | 2.14 | 0.89 | 5.14 | 0.0886 | 9 hours/day | 3 | 9526 | 116 | 1.77 | 0.46 | 6.81 | 0.4069 | ||||
| ≥10 hours/day | 8 | 11251 | 138 | 2.55 | 1.07 | 6.08 | 0.0343 | * | ≥10 hours/day | 3 | 9106 | 111 | 1.16 | 0.29 | 4.64 | 0.8382 | |||
| P-trend (ordinal) | 0.0751 | P-trend (ordinal) | 0.0255 | * | |||||||||||||||
p-values and p-trends <0.05 were considered statistically noteworthy.
p-values and p-trends below a Bonferroni-corrected α-level of 0.0028 (0.05/18 tests from 6 age-periods × 3 parameters of sleep duration) were considered statistically significant.
Separate Cox models were fitted for each age-period. Separate analyses were performed for men and women. In men, Cox models were adjusted for: average hours spent performing indoor activities in the same age period as sleep (continuous counts), type of respondent (self, surrogate), other work besides farming (yes, no), educational attainment (illiterate, primary school, middle/vocational school or higher), duration of smoking (years), ever active smoking (yes, no), ethnicity (Han Chinese, other), average number of rooms and people in residences from 1976-1992 (continuous), fuel type used in first residence (smoky coal, smokeless coal, coal cakes, other), installation of a chimney for ventilation (stove improvement) (yes, no), family history of any cancer (yes, no), average tons of fuel/coal used from 1976-1992 (continuous), ever employed as a miner (yes, no), age in 1976 (years), and an indicator variable for history of respiratory comorbidities (Asthma, Emphysema, Chronic Bronchitis, and Chronic Obstructive Pulmonary Disorder). In women, duration of smoking, ever smoking, and ever employed as a miner were removed due to lack of variability, while age at which one began cooking (years) was included. Prevalent (1976-1991) and incident lung cancer mortality cases in the first two years of follow-up (1992-1993) were censored, only events from 1994-2011 were counted. Sample sizes (n) represent those with sleep data in each age period. Abbreviations: Hazard Ratio (HR), 95% Confidence Interval (95% CI), Person-Years Lived (Attained Age) (pyl), Lung Cancer related mortality (Cases).
In the age period of 21-30 years, the J-shaped trend was more apparent in women, with ≥10 sleep hours/day associated with a noteworthy increased risk of lung cancer mortality (HR=1.31 (95% CI: 1.03, 1.66, p=0.0262)) (Table 2). This pattern was less apparent in men. Similar trends were observed in the subsequent age-period of 31-40 years for men and women; however, ≥10 hours/day was associated with an even greater risk in women (HR=1.72 (95% CI: 1.34, 2.22, p<0.0001).
In the age-period of 41-50 years, the J-shaped trends became pronounced for both men and women. In men, both ≤7 hours/day (HR=1.39, 95% CI: 1.19, 1.63, p<0.0001) and ≥10 hours/day (HR=2.44, 95% CI: 1.91, 3.12, p<0.0001) were significantly associated with increased risks. In women, the increased risk with ≤7 hours/day (HR=1.18, 95% CI: 0.98, 1.42, p=0.0774) was nominal, but the increased risk with ≥10 hours/day (HR=2.45, 95% CI: 1.76, 3.41, p<0.0001) was significant.
In the age-period of 51-60 years, the J-shaped trends became most apparent for both men and women. In men, both ≤7 hours/day (HR=1.46, 95% CI: 1.23, 1.73, p<0.0001) and ≥10 hours/day (HR=2.51, 95% CI: 1.91, 3.30, p<0.0001) were significantly associated with increased risks. Similarly, both ≤7 hours/day (HR=1.29, 95% CI: 1.06, 1.57, p=0.0130) and ≥10 hours/day (HR=2.40, 95% CI: 1.73, 3.33, p<0.0001) had noteworthy associations with increased risks in women. In the subsequent age-period of 61-70 years, the J-shaped relations were still apparent for men and women. Furthermore, ≥10 hours/day in this age-period had the greatest magnitude of risk throughout the entire life course of men (HR=3.27, 95% CI: 2.31, 4.62, p<0.0001). In women, the increased risk associated with ≥10 hours/day was nominal (HR=1.59, 95% CI: 0.96, 2.64, p=0.0704).
When restricting to ever-users of smoky coal and stratified by average tons used prior to 1992 (low tonnage: <3.3 and high tonnage: ≥3.3), similar trends with greater magnitudes of association were found in those with low tonnage (Supplementary Table 1). In the prospective analyses that excluded those who died before 1992 and surrogated reported data, similar trends and magnitudes of association were observed compared to analyses including all participants (Supplementary Table 2). The findings were similar to sensitivity analyses that included all prevalent and incident cases of lung cancer mortality from 1976 to 2011 (Supplementary Table 3), and only incident cases from 1992-2011 (data not shown). The findings were also similar when using 8-9 sleep hours/day as the reference category, rather than 8 hours/day (Supplementary Table 4).
Discussion
We found J-shaped relationships between average sleep duration in various age-periods across the adult lifecourse, and risk of lung cancer mortality in Xuanwei, China. The overall patterns were generally consistent across sex, age-periods, and fuel usage. In men, a deficit and excess of sleep were related to the most pronounced risks in mid to later life. In women, a sleep deficit was found to be most detrimental in later life, while excessive sleep was associated with significantly increased risks in early to mid-adulthood. This study was novel in that it was the first investigation to our knowledge that assessed age-period specific sleep duration throughout the lifecourse, and evaluated their associations with lung cancer mortality.
The relationship between sleep duration and cancer is thought to be driven by cumulative exposure to melatonin, a hormone that has been shown in experimental studies to have anti-proliferative properties, and in clinical trials to be related with increased survival rate (32-35). However, sleep duration may also be proxy for a variety of social, environmental, and physiological factors that affect incidence and mortality risk (17). Therefore, the interrelationships underlying the observed associations remain unclear. Further studies to assess the underlying biological mechanisms are warranted.
Several factors may explain our findings; therefore, sensitivity analyses were conducted to assess their potential influence. First, participants who slept more in their homes may have had greater exposure to smoky coal emissions. Similar findings were observed when the analyses were restricted to ever-users of smoky coal. Additionally, when the ever-users of smoky coal were stratified by tonnage, similar trends were observed in the participants with low tonnage, but not in those with high tonnage; indicating that the observed associations were not due to greater household smoky coal use. We were unable to assess the associations restricted to non-smoky coal users due to limited cases in these participants. Second, we assessed the potential influence of differential reporting bias of sleep hours from surrogates of participants who were deceased by 1992. In the prospective analyses that were restricted to those alive in 1992 and self-reported their own sleep data, similar results were found compared to analyses with all participants; suggesting that survivor bias and surrogate reporting were not influential factors. Third, there was the potential for underlying, undiagnosed disease to affect reporting of sleep hours during the retrospective follow-up period (1976-1991). Therefore, we assessed the potential influence of including all incident and prevalent cases identified in 1976-2011 as events and found similar results compared to the analyses that included only incident cases that occurred after 1992 as events; suggesting that the findings were robust against the potential of reporting-bias of sleep hours from the prevalent cases.
The curvilinear trends found in this study were consistent with other investigations of the relationship between sleep duration and total and lung cancer mortality (15,36). A prospective cohort study of 113,138 middle-aged and elderly Chinese participants in the Shanghai Women's and Men's Health Studies found a significant curvilinear trend with lung cancer mortality in women with a nadir of 6-7 sleep hours/day, but not men (15). Despite these trends, only ≥10 sleep hours/day was significantly associated with increased lung cancer mortality in men (15). In the Cancer Prevention Study II, one of the largest studies of sleep and mortality comprised of 1.1 million U.S. men and women, participants who reported sleeping <6 and ≥8 hours/day had significantly higher total mortality risks (37). In the Jichi Medical School Cohort Study of residents in rural Japan, the risks of all-cause mortality for individuals sleeping <6 hours and ≥9 hours were significantly elevated compared to those with 7-7.9 hours of sleep (16). Another community-based study in Japan also found that both short and long sleep duration were associated with increased total mortality (38). Additionally, the Nurses' Health Study found similar curvilinear trends with total mortality with a nadir of 6-7 hours (14). Although the overall trends were consistent across studies, there were different nadirs. These differences may be due to the unique characteristics of each population and/or variations in the assessment of sleep duration.
This study had numerous strengths in addressing the study objectives. First, this study was conducted in a large, well-powered cohort with extensive lifecourse data. Second, although sleep and covariate data were retrospectively assessed, cases of lung cancer mortality were prospective, which allowed temporality to be established. The prospective aspect of the study design strengthens the case for a causal relationship between sleep duration and lung cancer mortality. Third, censoring both prevalent and incident cases of lung cancer mortality in the first two years of follow-up mitigated the potential of reporting bias of sleep hours from underlying, undetected disease. Fourth, given the rural nature of the cohort, the influence of potential confounding factors such as shift-work and circadian misalignment could likely be excluded.
Despite its strengths, this study had limitations. First, average sleep hours in various age-periods were self and surrogate reported and thus subject to individual recollection. Random misclassification of sleep hours would attenuate the estimates towards the null; however, statistically significant estimates of sizable magnitude were still found. Differential misclassification (recall bias) of the exposure may occur if the surrogates of the participants who died from lung cancer under or over-reported sleep hours compared to participants who were alive and self-reported. However, our findings were similar when restricting the analyses only to those who self-reported their sleep hours in 1992. Second, random misclassification of lung cancer mortality was possible if doctors or coroners misreported the cause of death, or if there were multiple causes (39). However, in analyses with the outcome restricted to deaths with medically/histologically confirmed lung cancer occurrence, similar overall trends were still observed (data not shown). Third, given that the residents of rural Xuanwei were unique in their lifestyle and environmental exposures, findings from this study may have narrow generalizability. However, similar trends have been consistently reported throughout the body of literature (36). Fourth, there was the possibility of unmeasured confounding. In particular, information on body mass index (BMI) was not collected. However, the variability in adiposity was assumed to be narrow in Chinese farmers (40). Additionally, we were unable to assess perturbations to circadian rhythm. However, the influence of shift-work and circadian misalignment could likely be excluded in this farming community. Fifth, we did not collect information on sleep quality and sleep apnea, which may be important confounders. Despite the potential for unmeasured and residual confounding, the magnitude of bias would have to be substantial to explain the considerable and consistent associations that were observed in this study. Lastly, multiple-testing may have inflated the family-wise error rate and led to false-positive results. However, our findings were consistent with previous studies of sleep duration and we used stringent Bonferroni-corrected significance levels to account for false-positives.
In summary, we found J-shaped relationships between average sleep duration in various age-periods across the adult lifecourse and risk of lung cancer mortality. The patterns were consistent across sex, age-periods, and fuel usage. A deficit of sleep ≤7 hours/day might be related to increased risks of lung cancer mortality, while an excess of sleep ≥10 hours/day might be related to even greater risks. These findings suggest that maintaining a sleep regiment of approximately 8 hours/day across the adult lifecourse might be beneficial in mitigating the risk of death from lung cancer in this high-risk population. Future studies would benefit from longitudinal prospective follow-ups of larger sample populations, in addition to continuous monitoring of sleep duration, sleep quality, and circadian rhythm.
Supplementary Material
Acknowledgments
Funding: This study was supported by funding awarded to Qing Lan by the Chinese Academy of Preventive Medicine (Beijing, China), the Yunnan Province Anti-epidemic Station (Kunming, China), the U.S. Environmental Protection Agency (Contract 5D2290NFFX), and the Intramural Research Program of the U.S. National Cancer Institute, National Institutes of Health, Department of Health and Human Services.This study was supported by the Chinese Academy of Preventive Medicine (Beijing, China), the Yunnan Province Anti-epidemic Station (Kunming, China), the U.S. Environmental Protection Agency (Contract 5D2290NFFX), and the Intramural Research Program of the U.S. National Cancer Institute, National Institutes of Health.
Abbreviations
- HR
hazard ratio
- CI
confidence interval
- pyl
person-years lived
Footnotes
The authors declare no conflicts of interest.
References
- 1.Pronk A, Ji BT, Shu XO, Xue S, Yang G, Li HL, et al. Night-shift work and breast cancer risk in a cohort of Chinese women. American journal of epidemiology. 2010;171(9):953–9. doi: 10.1093/aje/kwq029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Schernhammer ES, Kroenke CH, Laden F, Hankinson SE. Night work and risk of breast cancer. Epidemiology. 2006;17(1):108–11. doi: 10.1097/01.ede.0000190539.03500.c1. [DOI] [PubMed] [Google Scholar]
- 3.Schernhammer ES, Rosner B, Willett WC, Laden F, Colditz GA, Hankinson SE. Epidemiology of urinary melatonin in women and its relation to other hormones and night work. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2004;13(6):936–43. [PubMed] [Google Scholar]
- 4.Hurley S, Goldberg D, Bernstein L, Reynolds P. Sleep duration and cancer risk in women. Cancer causes & control : CCC. 2015;26(7):1037–45. doi: 10.1007/s10552-015-0579-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Qian X, Brinton LA, Schairer C, Matthews CE. Sleep duration and breast cancer risk in the Breast Cancer Detection Demonstration Project follow-up cohort. British journal of cancer. 2015;112(3):567–71. doi: 10.1038/bjc.2014.600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wang P, Ren FM, Lin Y, Su FX, Jia WH, Su XF, et al. Night-shift work, sleep duration, daytime napping, and breast cancer risk. Sleep medicine. 2015;16(4):462–8. doi: 10.1016/j.sleep.2014.11.017. [DOI] [PubMed] [Google Scholar]
- 7.Sigurdardottir LG, Valdimarsdottir UA, Fall K, Rider JR, Lockley SW, Schernhammer E, et al. Circadian disruption, sleep loss, and prostate cancer risk: a systematic review of epidemiologic studies. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2012;21(7):1002–11. doi: 10.1158/1055-9965.EPI-12-0116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Miller MA, Cappuccio FP. Inflammation, sleep, obesity and cardiovascular disease. Current vascular pharmacology. 2007;5(2):93–102. doi: 10.2174/157016107780368280. [DOI] [PubMed] [Google Scholar]
- 9.Spiegel K, Tasali E, Leproult R, Van Cauter E. Effects of poor and short sleep on glucose metabolism and obesity risk. Nature reviews Endocrinology. 2009;5(5):253–61. doi: 10.1038/nrendo.2009.23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lu Y, Tian N, Yin J, Shi Y, Huang Z. Association between sleep duration and cancer risk: a meta-analysis of prospective cohort studies. PloS one. 2013;8(9):e74723. doi: 10.1371/journal.pone.0074723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Xiao Q, Keadle SK, Hollenbeck AR, Matthews CE. Sleep duration and total and cause-specific mortality in a large US cohort: interrelationships with physical activity, sedentary behavior, and body mass index. American journal of epidemiology. 2014;180(10):997–1006. doi: 10.1093/aje/kwu222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Yeo Y, Ma SH, Park SK, Chang SH, Shin HR, Kang D, et al. A prospective cohort study on the relationship of sleep duration with all-cause and disease-specific mortality in the Korean Multi-center Cancer Cohort study. Journal of preventive medicine and public health = Yebang Uihakhoe chi. 2013;46(5):271–81. doi: 10.3961/jpmph.2013.46.5.271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tamakoshi A, Ohno Y, Group JS. Self-reported sleep duration as a predictor of all-cause mortality: results from the JACC study, Japan. Sleep. 2004;27(1):51–4. [PubMed] [Google Scholar]
- 14.Patel SR, Ayas NT, Malhotra MR, White DP, Schernhammer ES, Speizer FE, et al. A prospective study of sleep duration and mortality risk in women. Sleep. 2004;27(3):440–4. doi: 10.1093/sleep/27.3.440. [DOI] [PubMed] [Google Scholar]
- 15.Cai H, Shu XO, Xiang YB, Yang G, Li H, Ji BT, et al. Sleep duration and mortality: a prospective study of 113 138 middle-aged and elderly Chinese men and women. Sleep. 2015;38(4):529–36. doi: 10.5665/sleep.4564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Amagai Y, Ishikawa S, Gotoh T, Doi Y, Kayaba K, Nakamura Y, et al. Sleep duration and mortality in Japan: the Jichi Medical School Cohort Study. Journal of epidemiology / Japan Epidemiological Association. 2004;14(4):124–8. doi: 10.2188/jea.14.124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Grandner MA, Hale L, Moore M, Patel NP. Mortality associated with short sleep duration: The evidence, the possible mechanisms, and the future. Sleep medicine reviews. 2010;14(3):191–203. doi: 10.1016/j.smrv.2009.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Luojus MK, Lehto SM, Tolmunen T, Erkkila AT, Kauhanen J. Sleep duration and incidence of lung cancer in ageing men. BMC public health. 2014;14:295. doi: 10.1186/1471-2458-14-295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Suzuki K Japan Collaborative Cohort Study for Evaluation of C. Health conditions and mortality in the Japan Collaborative Cohort Study for Evaluation of Cancer (JACC) Asian Pacific journal of cancer prevention : APJCP. 2007;(8 Suppl):25–34. [PubMed] [Google Scholar]
- 20.Khawaja O, Petrone AB, Aleem S, Manzoor K, Gaziano JM, Djousse L. Sleep duration and risk of lung cancer in the physicians' health study. Zhongguo fei ai za zhi = Chinese journal of lung cancer. 2014;17(9):649–55. doi: 10.3779/j.issn.1009-3419.2014.09.02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.http://data.worldbank.org. 2015 The World Bank. <http://data.worldbank.org/indicator/SP.RUR.TOTL.ZS>.
- 22.Lan Q, He X, Costa DJ, Tian L, Rothman N, Hu G, et al. Indoor coal combustion emissions, GSTM1 and GSTT1 genotypes, and lung cancer risk: a case-control study in Xuan Wei, China. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2000;9(6):605–8. [PubMed] [Google Scholar]
- 23.Society AC. 2017 https://cancerstatisticscenter.cancer.org/#/
- 24.Seow WJ, Hu W, Vermeulen R, Hosgood Iii HD, Downward GS, Chapman RS, et al. Household air pollution and lung cancer in China: a review of studies in Xuanwei. Chinese journal of cancer. 2014;33(10):471–5. doi: 10.5732/cjc.014.10132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lan Q, Chapman RS, Schreinemachers DM, Tian L, He X. Household stove improvement and risk of lung cancer in Xuanwei, China. Journal of the National Cancer Institute. 2002;94(11):826–35. doi: 10.1093/jnci/94.11.826. [DOI] [PubMed] [Google Scholar]
- 26.Shen M, Chapman RS, Vermeulen R, Tian L, Zheng T, Chen BE, et al. Coal use, stove improvement, and adult pneumonia mortality in Xuanwei, China: a retrospective cohort study. Environmental health perspectives. 2009;117(2):261–6. doi: 10.1289/ehp.11521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Fisher LD, Lin DY. Time-dependent covariates in the Cox proportional-hazards regression model. Annu Rev Public Health. 1999;20:145–57. doi: 10.1146/annurev.publhealth.20.1.145. [DOI] [PubMed] [Google Scholar]
- 28.Watson NF, Badr MS, Belenky G, Bliwise DL, Buxton OM, Buysse D, et al. Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society on the Recommended Amount of Sleep for a Healthy Adult: Methodology and Discussion. Sleep. 2015;38(8):1161–83. doi: 10.5665/sleep.4886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hernan MA, Robins JM. Estimating causal effects from epidemiological data. Journal of epidemiology and community health. 2006;60(7):578–86. doi: 10.1136/jech.2004.029496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Greenland S, Robins JM. Identifiability, exchangeability, and epidemiological confounding. International journal of epidemiology. 1986;15(3):413–9. doi: 10.1093/ije/15.3.413. [DOI] [PubMed] [Google Scholar]
- 31.Heinzl H, Kaider A. Gaining more flexibility in Cox proportional hazards regression models with cubic spline functions. Comput Methods Programs Biomed. 1997;54(3):201–8. doi: 10.1016/s0169-2607(97)00043-6. [DOI] [PubMed] [Google Scholar]
- 32.Lissoni P, Chilelli M, Villa S, Cerizza L, Tancini G. Five years survival in metastatic non-small cell lung cancer patients treated with chemotherapy alone or chemotherapy and melatonin: a randomized trial. Journal of pineal research. 2003;35(1):12–5. doi: 10.1034/j.1600-079x.2003.00032.x. [DOI] [PubMed] [Google Scholar]
- 33.Blask DE, Dauchy RT, Sauer LA, Krause JA. Melatonin uptake and growth prevention in rat hepatoma 7288CTC in response to dietary melatonin: melatonin receptor-mediated inhibition of tumor linoleic acid metabolism to the growth signaling molecule 13-hydroxyoctadecadienoic acid and the potential role of phytomelatonin. Carcinogenesis. 2004;25(6):951–60. doi: 10.1093/carcin/bgh090. [DOI] [PubMed] [Google Scholar]
- 34.Karbownik M. Potential anticarcinogenic action of melatonin and other antioxidants mediated by antioxidative mechanisms. Neuro endocrinology letters. 2002;23(1):39–44. [PubMed] [Google Scholar]
- 35.Wu AH, Wang R, Koh WP, Stanczyk FZ, Lee HP, Yu MC. Sleep duration, melatonin and breast cancer among Chinese women in Singapore. Carcinogenesis. 2008;29(6):1244–8. doi: 10.1093/carcin/bgn100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cappuccio FP, D'Elia L, Strazzullo P, Miller MA. Sleep duration and all-cause mortality: a systematic review and meta-analysis of prospective studies. Sleep. 2010;33(5):585–92. doi: 10.1093/sleep/33.5.585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kripke DF, Garfinkel L, Wingard DL, Klauber MR, Marler MR. Mortality associated with sleep duration and insomnia. Archives of general psychiatry. 2002;59(2):131–6. doi: 10.1001/archpsyc.59.2.131. [DOI] [PubMed] [Google Scholar]
- 38.Ikehara S, Iso H, Date C, Kikuchi S, Watanabe Y, Wada Y, et al. Association of sleep duration with mortality from cardiovascular disease and other causes for Japanese men and women: the JACC study. Sleep. 2009;32(3):295–301. doi: 10.1093/sleep/32.3.295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.D'Amico M, Agozzino E, Biagino A, Simonetti A, Marinelli P. Ill-defined and multiple causes on death certificates--a study of misclassification in mortality statistics. European journal of epidemiology. 1999;15(2):141–8. doi: 10.1023/a:1007570405888. [DOI] [PubMed] [Google Scholar]
- 40.Jin ZY, Wu M, Han RQ, Zhang XF, Wang XS, Liu AM, et al. Household ventilation may reduce effects of indoor air pollutants for prevention of lung cancer: a case-control study in a Chinese population. PloS one. 2014;9(7):e102685. doi: 10.1371/journal.pone.0102685. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.