

Abstract
BACKGROUND:
Awareness regarding cancer signs and symptoms and their screening and treatment method was low in India.
OBJECTIVES:
To assess the awareness level of common cancers, perception regarding prevention and treatment of common cancers, association between sociodemographic variables with the awareness level of common cancers in the adult population.
MATERIALS AND METHODS:
A cross-sectional study was conducted among 299 adults from the field practice areas of Our Rural Health Centre, Puducherry, during April–May 2014. Using systematic random sampling, 299 adults were interviewed through a pretested semi-structured questionnaire. Data were entered into EpiData version 3.1 and were analyzed by Statistical Package for Social Sciences version 20. Chi-square test was used.
RESULTS:
Nearly, 64% were in the age group of ≥40 years, the majorities were females (56.2%) and 64% were in lower socioeconomic class. Symptoms reported majorities were unusual bleeding (41.6%), followed by nagging cough (34.1%). Risk factors reported majorities were smoking (65%), chewing tobacco (59%) followed by alcohol use (46.5%). Only 10% reported cancer could be diagnosed early and 27% perceived cancer could be preventable. Only 6% perceived cancer could be cured fully. The adequate awareness level regarding lung and oral cancer were 14%, but breast and cervical cancer were <5%. The younger age group (<40 years) had more adequate awareness level compared to age group ≥40 years (P < 0.05).
CONCLUSION:
The awareness level of common cancers was very poor. Vigorous health education program should improve the status of early diagnosis and proper treatment for common cancers such as oral, breast, and cervical cancer.
Keywords: Awareness, common neoplasms, India, perceptions, rural
Introduction
Noncommunicable diseases (NCDs) are increasing in number among the adult population in both developing and developed countries. Cancer is one of the major NCDs and is emerging as a major health problem globally with over 10 million new cases and more than 6 million deaths (12% of all deaths) worldwide every year.[1] According to the World Cancer Report (2008), there is a high incidence rate of cancer throughout the world and it may reach about 20 million by 2030, nearly 70% of cancer deaths occurs in low- and middle-income countries.[1,2] The burden of cancer is increasing in developing countries with an increase in life expectancy and increased exposure to cigarette smoking, higher consumption of saturated fat, calorie-dense foods, and reduced physical activity.[3]
Cancer has become one of the leading causes of death in India. Every year, about 4 lakh deaths occur due to cancer (Ministry of Health and Family Welfare 2009–10).[4] Data from population-based cancer registry on the pattern of cancer have remained unchanged over the years, namely oral cavity, lungs, esophagus, and stomach among men and cervix, breast, and oral cavity among women. Cancers of oral and lungs in males and cervix and breast in females account for more than 50% of all cancer deaths in India.
The studies done by Kumar et al.[5] and Pedgaonkar et al.[6] in Mumbai slums found that awareness regarding symptoms, risk factors, and screening methods of common cancer was poor. Similar findings were found in studies done in Chandigarh and New Delhi.[3,7] These research studies were lacking from South India, especially from rural areas. The country-wise awareness regarding symptoms and risk factors of common cancer was done by Raj et al.[8] Besides that they have not studied about awareness regarding screening methods, prevention methods, and perception of treatment available for common cancer in India.
According to the World Health Organization, most cases of cancer are detected only in the advanced stages, when they are untreatable (Indian Council of Medical Research, 2004),[9] this was especially true in developing countries. The fact is that in the case of head and neck cancers, cervical cancer, and breast cancer, i.e., the most common cancers in India, there are proven screening methods to catch the disease at an early stage when it is curable. Facilities for proper screening and management of cancer patients are grossly limited in countries like India, and the awareness regarding cancer signs and symptoms and their screening and treatment method was also low here. These were reasons that most of the cancer patients were diagnosed at an advanced and untreatable stage in India.[10]
The objectives of this study were to assess the awareness level of common cancers, to find out the perception regarding prevention and treatment of common cancers, and to find out the association between sociodemographic variables with the awareness level of common cancers in the population aged 18 years and above.
Materials and Methods
The present study was a community-based, cross-sectional study conducted in the field practice areas of Our Rural Health Centre, Puducherry, during April–May 2014. Rural Health Centre (RHC) is located at Ramanathapuram village, which is at a distance of about 14 km from our institute. RHC provides comprehensive health care to a population of 9170 in four villages, namely Pillayarkuppam (2451), Thuthipet (830), Ramanathapuram (2355), and Thodamanthanam (3534). The present study was conducted among adults population 18 years or above.
Considering awareness of cervical cancer was 25%,[8] with absolute precision of 5%, the sample size was calculated to be 288 with the confidence interval of 95%. A total of 300 households were contacted using stratified sampling method with 72, 124, 24, and 80 households from Ramanathapuram (500-HH), Thodamanthanam (852-HH), Thuthipet (165-HH), and Pillayarkuppam (572-HH) village, respectively. The first house in the respective village was selected randomly, and then every seventh house was included in the study. If the selected household was locked, next household was selected, but the sequence was not changed. Households those who were living in the respective areas for at least 6 months were included in the study. Using simple random method, one adult from each selected household was interviewed.
The questionnaire was formed by the various literature published in these topics. The interview was done by a group of four interns those were trained for interview techniques. The pretesting of the questionnaire was done before the proper study. The supervision of the interview was done by both the authors. One interview took around 40–45 min. Information on cancers, awareness of symptoms, risk factors, screening method and prevention method, perception regarding prevention, and treatment was obtained using a pretested semi-structured questionnaire after obtaining informed consent. All the four ethical principles were followed throughout the study. Sociodemographic factors such as age, gender, education, and occupation were obtained during the interview. The education status was classified based on the Tamil Nadu education board. Socioeconomic status was classified using modified Prasad classification 2014 based on income.[11]
In the present study, the awareness level of common cancers was based on a scoring system. Scoring was based on all the domains of cancer awareness regarding symptoms, risk factors, and screening and prevention method of common cancers. The maximum score would be 7. score < 4 were considered as poor awareness, and score of 4 and above were considered as adequate awareness.
Statistical methods
Data were entered into EpiData version 3.0 (EpiData Association 2000-2016),[12] and analysis was done using SPSS Version 20.0 (IBM Corp.: Armonk, NY).[13] Description of all sociodemographic variables and symptoms, risk factors of common cancers were reported in percentages. The awareness level of common cancer was also reported as percentages. The univariate analysis was carried out to find out the association between sociodemographic variables with the awareness level of common cancers by Chi-square test and Fisher's extract test. The P value for significance testing was set at the level of 0.05.
Results
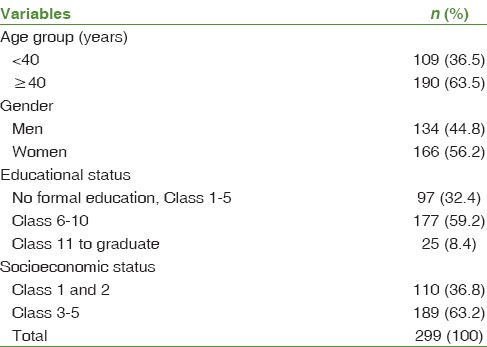
Table 1 showed the sociodemographic details of the study population. Of the 299 cases, nearly 64% (190) were in the age group of ≥40 years and majorities were women (56.2%).
Table 1.
Sociodemographic details of the study population
Around 40% of the study population was reported that common cancers affecting men were lung and oral cancer. Nearly, 17% of them reported stomach cancer could be common cancer affecting men. About one-third of cases, 32% reported breast cancer was common cancer affecting women. Uterine and cervical cancer were reported nearly 10% (29).
On enquiry regarding the common symptoms of cancer, the respondents came out with unusual bleeding or discharge 124 (41.6%), nagging cough 102 (34.1%), nonhealing sore 72 (24.1%), and lump or swelling 69 (23.1%) [Figure 1]. Similarly, regarding risk factors of common cancer, smoking was reported by majority (65%) followed by chewing tobacco (59%) and alcohol intake (46.5%) [Figure 2].
Figure 1.
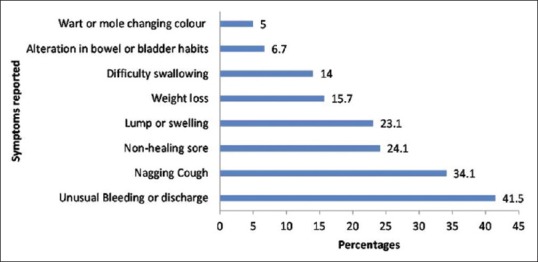
Various symptoms of common cancers reported by study population (*multiple answers possible)
Figure 2.
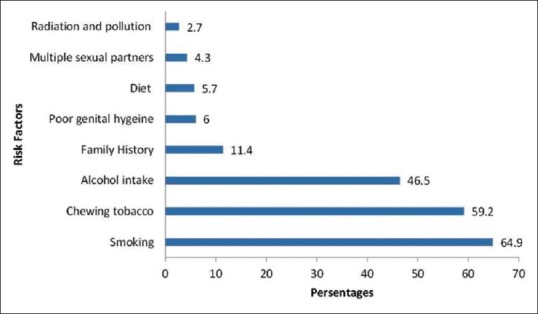
Various risk factors of common cancers reported by study population (*multiple answers possible)
Of the 299 study population, only 10% of them reported cancer could be diagnosed early by proper screening method and 78% reported that cancer could not be diagnosed early. The rest 12% of the study population reported did not know what to say about screening method for cancer.
Nearly, 60% of the study population perceived cancer has no cure, only 5.7% believe cancer could be cured fully, and the rest 35% of the study population believed cancer could be treated partially. Around 27% (82) of the study population perceived cancer could be preventable; moreover, majority of the study population 42% (125) perceived cancer could not be preventable and the rest 31% (92) of them did not know what to perceive about preventive method for cancer.
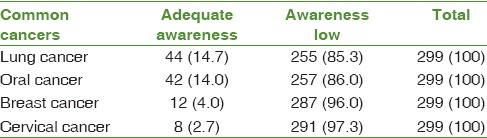
Table 2 shows that “adequate” awareness level regarding lung and oral cancer was 14% of the study population. Similarly, <5% of the study population showed adequate awareness level regarding breast and cervical cancer.
Table 2.
Awareness level of common cancers in the study population (based on the scoring pattern)
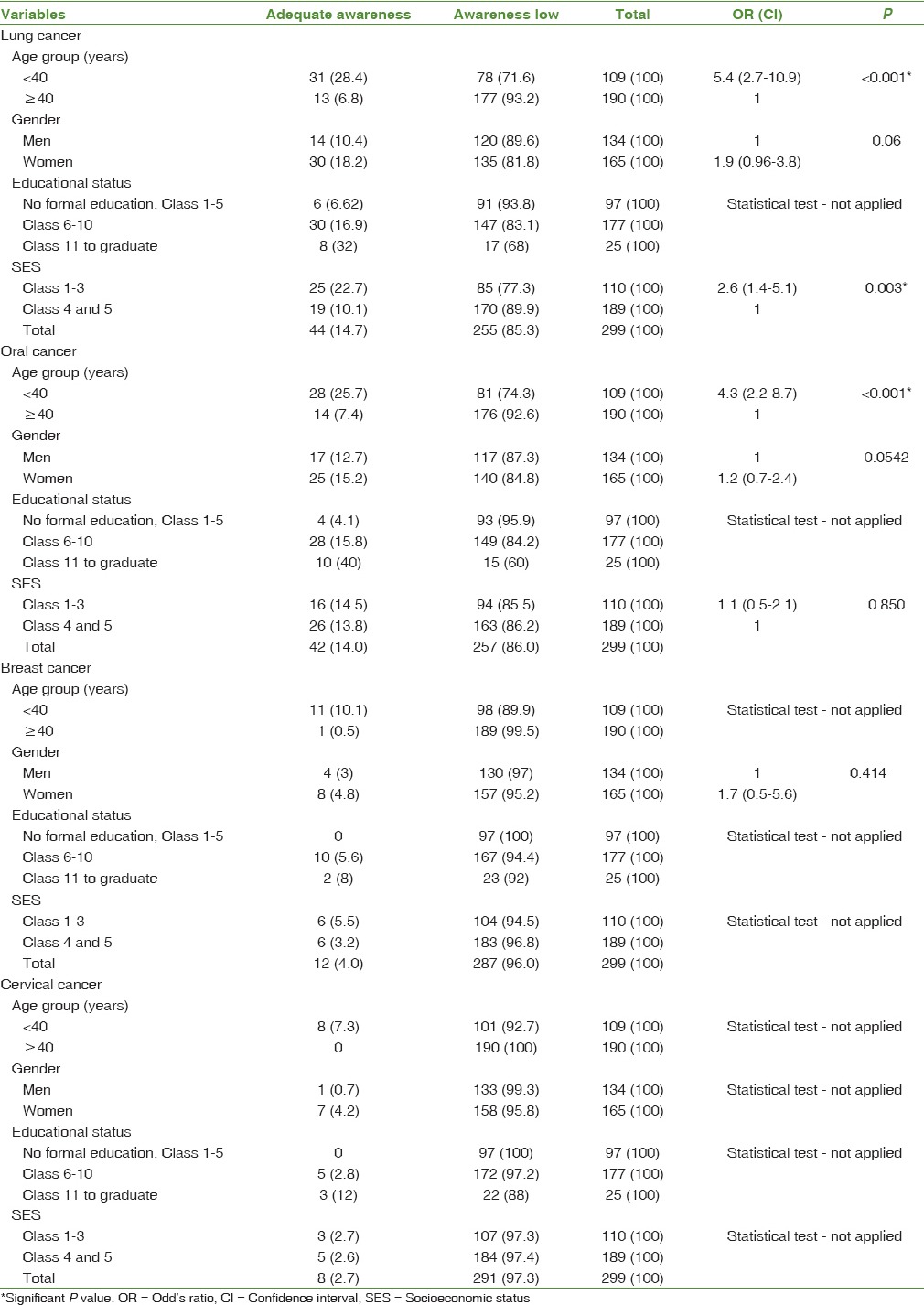
In regard to the association between awareness levels of common cancers with sociodemographic variables, population below the age group of 40 years was having more awareness level compared to the age group of 40 years and above (P < 0.05) for lung and oral cancers [Table 3]. Although females had more adequate awareness level compared to males, still this was not showing statistically significant difference in lung and oral cancers. Participants belonging to middle- and high-socioeconomic group were having more adequate awareness level compared to the low-socioeconomic group in both lung and oral cancers though the statistical significant difference was found only in the lung cancer. Association between awareness levels of breast and cervical cancers with sociodemographic variables could not be done because of low awareness, i.e., < 5% in the both cancers.
Table 3.
Association between sociodemographic variables with awareness level of common cancers
Discussion
In the present study, it was found that majority of study population knew about the common cancers affecting men and women such as lung, oral, breast, and cervix cancer. These findings were comparable to the studies done from the various places of India Puri et al.; Kumar et al.; Raj et al.[3,5,8] In the present study, unusual bleeding was reported as a cancer symptom from a majority of the study population (41.5%). Besides that people were hardly aware of other symptoms of cancer such as nagging cough, nonhealing sore, lump or swelling, and persistent indigestion. Studies done by Puri et al.[3] and Raj et al.[8] reported that unusual bleeding was the major symptom for cancer as 23% and 66%, respectively. This minor difference in proportion due to the place of study, Raj et al. have found in various six states of India and Puri et al. have found in Chandigarh.
Similarly, most of study population (60%) was aware of smoking and smokeless tobacco as a risk factor for cancers. However, most of the population was hardly aware of other risk factors such as industrial radiation, early child-bearing, nulliparity, and overweight. Similar results were found in various studies done in India by Puri et al., Pedgaonkar et al., Raj et al., Ray and Mandal.[3,6,8,14] Moreover, health education activities hardly publicize other important risk factors such as consumption of alcohol and red meat, industrial radiation, early child-bearing, nulliparity, and overweight. As a result of the poor awareness about signs and symptoms, population might not pay much attention to important but less known symptoms. Such a poor awareness might cause a delay in detection of cancers. India is not an exception to such findings that are consistent with those of a few studies in other developing countries (San Turgay et al., 2005;[10] Saha et al., 2010[15]).
In the present study, majority of the study population (42%), perceived cancer could not be preventable, and around 30% of them did not know what to perceive about the preventive methods for cancer. However, the study done in Mumbai by Kumar et al.[5] has found that around 55% perceived cancer could be preventable. This difference in the findings of the present study as compared to Mumbai study could be due to the difference in the population characters. Thus, health education activities should be carried out about the harmful effects of tobacco and discourage its use. Besides that the awareness program should focus mainly on other risk factors such as physical activity, avoiding obesities, healthy dietary practices, reducing occupational and environmental exposures, reducing alcohol use, immunization against hepatitis B virus, and safe sexual practices for avoiding cancer genesis to the people.[16]
In the present study, majority of the study population (80%) were not aware of the screening methods available for common cancer such as cervix and breast. Similarly, most of the study population perceived that there was no cure for cancer (58.2%) Only 5% of the population perceived cancer could be completely cured. This showed that most of the study population was not aware of screening and treatment method of common cancer such as cervical and breast cancer. These findings were comparable to the study done by Puri et al.[3] and in contrast to the study done by Kumar et al.[5] in Mumbai. This difference in the findings of the present study as compared to Mumbai study could be due to self-reported bias or social desirability bias, i.e., procedures of cancer screening, fear of pain involving procedures. Hence, awareness program should conduct about the cancer screening and treatment. The oral cavity, uterine cervix, and female breast cancer are very amenable to early detection. In the 1970s, the Government of India designed primary and secondary prevention strategies for the control of cancer. The major thrust area of cancer control program included – public education, treatment, palliative care, and training facilities for human resource development. Under the National Cancer Control Program, such efforts were envisaged to be carried out through the district cancer control projects for educating the people about the signs, symptoms, and early detection. Several state-wise programs such as Kerala (10-year action plan), Tamil Nadu (Kancheepuram Cancer Screening Program), and opportunistic screening programs in social regions have been implemented by some State Governments and Regional Cancer Centers for an early detection of different cancers in India. These types of programs and activities should be conducted in all over India to screen all the population.
In the present study, only 14% of the study population had the adequate level of awareness regarding oral and lung cancers. However, the adequate level of awareness regarding breast and cervical cancer was even very low (5%) among the study population. It may be because major sources of information are TV and newspapers that give publicity of commonly occurring cancers, but no structured and targeted Information Education Communication (IEC) activities are promoted through programmatic effort. Poor awareness toward the cancer is considered to be a serious issue, which not only affects the public recognition toward disease but also delays the process of timely diagnosis and treatment. Similar findings were reported in other studies done in Delhi and Chandigarh.[7]
In the present study, in regards to the association of sociodemographic variables with the awareness level of cancer, only age group <40 years were found to be the significant association with the awareness level of cancer compare to age group ≥40 years. This finding may be possible due to the education level of young age group was high compared to the older age group. Hence, activities under the program should emphasis the older age compared to younger age group.
Strengths and limitation
The present study found that the awareness level of common cancer was based on all the domains such as symptoms, risk factors, screening, prevention, and treatment methods for particular cancer. Hence, this was the only study assessed the awareness level based on all the domains of cancer. Moreover, if health education activities focused only one particular domain, there might be the failure. Hence, health education should focus all the domains regarding cancer. Thus, this study would help the program officers and health educators to prepare about health education materials for cancer. This was one of the few studies that studied the perception regarding cancer treatment and perception. Next strength of this study was found about the association of sociodemographic variables with the awareness level of common cancer. Generalizability of these study findings to rural Puducherry could be possible due to the population of rural Puducherry and their de-variant sociodemographic variables.
The present study was based on the pretested semi-structured questionnaire. Hence, the possible bias could be self-reported bias and social desirability bias that could not be eliminated from the study findings. However, these biases have controlled by proper interview techniques training to the interviewers. Another bias this study was not studied about the cultural factors and barriers among the people to make awareness regarding common cancers. These factors would help the program officers to plan accordingly for making the people aware about common cancers. Thus, further studies are needed to find these factors.
Conclusion
The study found that awareness level of common cancer among the study population was very poor, and the majority of the study population was not aware of symptoms, risk factors, and screening methods of common cancer. The study also found that perception regarding the cancer prevention and treatment were in negative track. Hence, there is a need for vigorous health education program about awareness of all the domains of cancer like its symptoms, risk factors, screening method, prevention, and treatment. Under the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke, health workers should be trained to provide the awareness of common cancers through proper IEC activities. Mass media such as television, radio, newspaper, and internet should be used for the mass communication to the whole country. These activities should improve the status of early diagnosis and proper treatment for common cancers such as oral, breast, and cervical cancer.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to acknowledge the doctors V. Ashvini, Ashwin Chandran, Bala, Chrishanti Joseph for their help in data collection.
References
- 1.World Cancer Report. World Health Organization. 2008. [Last cited on 2015 Nov 15]. Available from: http://www.iarc.fr/en/publications/books/wcr/
- 2.Jugal Kishore. Kishore's National Health Programs in India. 7th ed. New Delhi: Century Publications; 2007. p. 391. [Google Scholar]
- 3.Puri S, Mangat C, Bhatia V, Kaur A, Kohli D. Knowledge of cancer and its risk factors in Chandigarh, India. Internet Sci Publ. 2014;8:1–7. [Google Scholar]
- 4.GOI, Annual Report. New Delhi: Ministry of Health and Family Welfare; 2009-2010. [Last cited on 2015 Nov 15]. Available from: http://www.mohfw.nic.in/ [Google Scholar]
- 5.Kumar YS, Mishra G, Gupta S, Shastri S. Level of cancer awareness among women of low socioeconomic status in Mumbai slums. Asian Pac J Cancer Prev. 2011;12:1295–8. [PubMed] [Google Scholar]
- 6.Pedgaonkar S, Velhal G, Mahajan H, Sharma B. Awareness about cancer in urban slum population of Mumbai, India. J Dent Med Sci. 2012;2:1–10. [Google Scholar]
- 7.Seth T, Kotwal A, Thakur R, Singh P, Kochupillai V. Common cancers in India: Knowledge, attitudes and behaviours of urban slum dwellers in New Delhi. Public Health. 2005;119:87–96. doi: 10.1016/j.puhe.2004.05.013. [DOI] [PubMed] [Google Scholar]
- 8.Raj S, Piang LK, Nair KS, Tiwari VK, Kaur H, Singh B. Awareness regarding risk factors, symptoms and treatment facilities for cancer in selected states of India. Asian Pac J Cancer Prev. 2012;13:4057–62. doi: 10.7314/apjcp.2012.13.8.4057. [DOI] [PubMed] [Google Scholar]
- 9.Development of an Atlas of Cancer in India. First All India Report 2001-2002: An Overview. New Delhi: ICMR, Supported by the World Health Organization; 2004. [Last cited on 2015 Nov 15]. Available from: http://www.mohfw.nic.in/ [Google Scholar]
- 10.San Turgay A, Sari D, Türkistanli EC. Knowledge, attitudes, risk factors, and early detection of cancer relevant to the school teachers in Izmir, Turkey. Prev Med. 2005;40:636–41. doi: 10.1016/j.ypmed.2004.09.038. [DOI] [PubMed] [Google Scholar]
- 11.Mangal A, Kumar V, Panesar S, Talwar R, Raut D, Singh S. Updated BG Prasad socioeconomic classification, 2014: A commentary. Indian J Public Health. 2015;59:42–4. doi: 10.4103/0019-557X.152859. [DOI] [PubMed] [Google Scholar]
- 12.Epidata Entry. Epidata Association. [Last cited on 2015, Nov 2015]. Available from: http://www.epidata.dk/
- 13.IBM. SPSS Statistics for Windows. Armonk, New York: IBM Corp; 2013. [Google Scholar]
- 14.Ray K, Mandal S. Knowledge about cancer in West Bengal – A pilot survey. Asian Pac J Cancer Prev. 2004;5:205–12. [PubMed] [Google Scholar]
- 15.Saha A, Chaudhury AN, Bhowmik P, Chatterjee R. Awareness of cervical cancer among female students of premier colleges in Kolkata, India. Asian Pac J Cancer Prev. 2010;11:1085–90. [PubMed] [Google Scholar]
- 16.Dinshaw K, Shastri S, Patil S. Cancer control programme in India: Challenges for the new millennium. Health Adm. 2004;17:10–3. [Google Scholar]