

Abstract
This study aimed to 1) investigate the incidence and characteristics of injuries in emerging rugby league players; and 2) explore the differences in injury incidence and characteristics between the various sub-elite competitions. An NRL emerging player development squad (n = 34) was observed from the beginning of pre-season until the finish of competition. Time-loss injury was defined as any physical pain or impairment sustained that resulted in players missing a match. Injuries were categorised according to circumstance, incidence, characteristics, playing position and competition level. Of a total of 196 injuries that were recorded, 45 were time-loss and 151 were transient. The total injury incidence was 7.9/1,000 playing hours. The most common sites for time-loss injuries were the shoulder, ankle/foot and knee. Ligament injuries accounted for the highest number of injuries by type. Forwards sustained the greatest number of injuries. However, backs suffered the greatest injury cost. The majority of time-loss injuries were sustained during competition matches. Injuries sustained during open age matches resulted in significantly higher injury cost to those received at NYC matches. NRL development and emerging rugby league players are exposed to high risk of injury. Lower limb and shoulder injuries to bone or connective tissue are prevalent as a result of contact during match play. Players at this developmental level feed into several different playing squads where disparities in physical development, maturation, playing intensity and training regimes are evident. This presents a challenge in matching physiological capabilities with playing demands for NRL development squads.
Key points.
Developing players experience a high proportion of shoulder injuries. Compared to previous studies.
A Higher percentage of fractures was observed compared to previous studies.
Injuries sustained during open age competition (RM/SS) demonstrated greater severity than those sustained in the NYC competition.
Severe injuries sustained late in the competition rounds highlight the need for extensive follow up post season.
Key words: Injury surveillance, Rugby, athlete development
Introduction
Rugby league is a physically demanding, high intensity collision sport requiring a multidisciplinary skill set of sprinting, tackling, accelerating, decelerating and changing direction(Gabbett et al., 2008). Due to the nature and volume of the contact and high intensity effort in rugby league, injuries are common (Gabbett, 2003a). It has been identified as one of the most injurious sports for players 5-14 years (31.4 injuries/100,000 persons) and 15-34 years (55.6 injuries/100,000 persons) (Centre, 2006; Statistics, 2003). Musculoskeletal injuries (Gabbett, 2003a), categorised as contact or non-contact injuries are common. High incidences of soft tissue injury have been previously observed in training and matches (Gabbett, 2004b). Recently, injury incidence of 37.1 injuries per 1000 hours was observed in junior elite players, predominantly during match play (90%)
The ankle and head/face were most frequently injured (Orr and Cheng, 2016). Previously junior rugby league match injury rates have been observed to range from 1 to 197 per 1000 playing hours, while amateur match injury rates ranging from 134 to 701 per 1000 playing hours have been documented. Semi-professional participation has observed the highest injury rates, ranging from 115 to 825, with professional level injury rates ranging from 58 to 211 per 1000 playing hours (King et al., 2010b).
The physiological demands of rugby league, both in competition and training, increase sharply from junior elite to sub-elite levels (Gabbett et al., 2008). Higher incidence of injury has been observed with higher playing intensities and higher competition levels (Gabbett, 2000; 2001a; Stephenson et al., 1996). Thus, as younger players are selected to compete against older, more experienced athletes for positions at sub-elite and elite level competition it is important to monitor the effects of these increased physiological demands on the developing athlete.
Injury risk in rugby league players is associated with multifactorial parameters which can be broadly categorized as external or internal influences (Drew and Finch, 2016). External influences include, but are not limited to, physiological demands, playing experience/competition level, match and training intensity, pre-season preparation and the input of support staff. Increased physiological demands are a key factor in the increases observed in negative outcomes such as injury associated with higher playing intensities and competitive levels (Gabbett, 2005). Match duration increases from 60-70 minutes at junior level to 80 minutes at senior level. Junior elite level players typically train 3 days per week for approximately 6 hours in total, whereas sub-elite level players generally train 4-5 days per week for approximately 12-18 hours per week. A recent study in Australian Football players found significant effects of increased duration of training and match play on injury incidence of emerging players when compared with established elite level players (Fortington et al., 2016). Increased training injuries have been observed in the earlier stages of a season (i.e. pre-season) when training intensity and duration are high (Gabbett, 2003b), while match injuries increase progressively throughout the course of a season (Gabbett, 2000; Gabbett, 2003b), and in total, exceed training injuries (Brito et al., 2012; Brooks et al., 2008; King et al., 2010a). Additionally, higher incidence of injury has been observed in rugby league players who undertake <18 weeks pre-season training (Gabbett and Domrow, 2005). As many sub-elite training squads do not have the resources to conduct pre-season training programs of 18 weeks or greater, this places them at greater risk of injury given they play a season of equivalent length to professional teams. For elite rugby league players, the contribution of training and recovery programs, medical, conditioning and support staff (dietitians, massage therapists, psychologists), state of the art technology (global positioning systems, sleep pods, ultrasound, hormone analysis), on injury prevention and management cannot be understated. Sub-elite players, by contrast, have limited access to such support, which can subject players to increased risk of injury or delayed return to sport.
The internal influences that may impact injury in rugby league players include age/maturation, body composition (Fortington et al., 2016; Gabbett, 2000; 2001a) and physiological characteristics (strength, power, speed, agility and aerobic capacity) (Gabbett et al., 2008; Meir, 1994). In addition, inter-relationships between these factors have been observed. For example, age and maturation demonstrate a significant effect on body mass, muscular power, speed, agility, and estimated maximal aerobic power (Gabbett, 2002). Compared to professional rugby league athletes, junior elite players have significantly lower body mass, mesomorphy and greater skinfold thickness (Cheng et al., 2014). Increases in body mass of 12.9 kg in forwards and 12.1 kg in backs between the ages of 14 and 18 with further increases of 9.8 kg in forwards and 8.2 kg in backs between under 19 and open age sub-elite players have been observed (Gabbett, 2002). The physiological characteristics of junior elite through to sub-elite players have been well established (Cheng et al., 2014; Gabbett, 2002). Lower levels of muscular power, speed, agility and aerobic capacity have all been observed between junior elite and sub-elite players (Gabbett, 2002). These physiological characteristics specifically have been linked to increased injury incidence in developing players (Gabbett and Domrow, 2005). Defensive performance and tackle proficiency in sub elite players have been associated with greater lower-body muscle power (Gabbett et al. 2009), height and body mass (Gabbett, 2009). Furthermore, these key tackle performance indicators have been linked to increased injury incidence (Cheng et al., 2014).
Due to the multifaceted nature of injury risk in emerging rugby league players it is imperative consideration is given to the implementation of injury prevention programs, particularly at the developmental levels where resources are often inadequate. Such programs should be multilayered and sequential in nature. This approach should include identification of the extent and nature of injury issues facing the organization, specifically incidence, types, sites and mechanisms of common injuries. Only then can appropriate injury prevention programs based on the aetiology previously identified be put in place. Finally, the program must be evaluated in order to provide insight into its effectiveness and potential future directions. Van Mechelen (1992) has previously described such modelling.
Injuries resulting in lost matches may influence team selections, alter team structure, reduce cohesion between players, and in turn, have a profound impact on team performance. At both the elite and sub-elite levels in sport it is critical to have the maximum number of players available for selection throughout the season (Gabbett, 2004a; Orchard, 2009). Sub-elite development squads typically form the pathway from junior elite to professional level competition. As such they are predominantly younger players (17-19 years) with little to no full time training experience. Limited experience with lengthy (>12 weeks) demanding pre-season training schedules leaves these players relatively underdeveloped for participation in open age competitions. Given that open age players are mainly adult males, often with an additional five to ten years training experience, the disparity may contribute to increased risk of injury in younger players.
Therefore, this study aimed to: 1) investigate the incidence and characteristics of injuries in sub-elite and emerging rugby league players; and 2) explore the differences in injury incidence and characteristics (severity, type, site, mechanism) and playing position between the various sub-elite competitions in which emerging National Rugby League (NRL) players participate.
Methods
A prospective cohort study of an NRL emerging player development squad (n = 35) was conducted from the pre-season (November 2014) until the finish of 26 competition matches (September 2015). All procedures were approved by The University of Sydney Human Research Ethics Committee, (protocol number 2015/415), in accordance with the Declaration of Helsinki. Written informed consent was obtained from participants and/or their parent/carer. The development squad included players participating in the second-tier competitions: under 20 years National Youth Competition (NYC, n = 33), open age competitions (Ron Massey Cup (RM), n = 3 and Sydney Shield (SS), n = 17) and players promoted from the under 18 years Junior Representative Competition (SG Ball, n = 3). Players within the squad played between competitions depending on selection policy; they may have played across two or three competitions throughout the season. This is standard practice for emerging sub-elite youth rugby league players. Injuries were recorded using a standardised validated musculoskeletal injury reporting tool (Orr and Cheng, 2016). Injuries were diagnosed and assessed by the club’s physiotherapist and medical trainer and categorised as circumstance (match/training, contact/non-contact), incidence, characteristics (site, type, severity, mechanism) and by playing position and competition level (King et al., 2009).
Injury incidence (King et al., 2009) was calculated as
Exact total minutes played for interchange players were not possible. Therefore, all match play calculations were based on whole match participation only. Precise follow-up data on players post season was also unattainable.
Time-loss injury was defined as any physical pain or impairment sustained during a match or training that resulted in players subsequently missing a match (Gabbett, 2000). Injuries were classified into severity categories based on the number of matches missed (0: transient; 1: mild; 2–4: moderate; ≥5: major). Complex injury characteristics required grouping of injuries with similar traits i.e. categorisation of injury by site included the grouping of shoulder injuries (dislocations/subluxations, acromioclavicular joint sprains and rotator cuff) and injuries by type i.e. ligament (shoulder subluxations, ankle syndesmosis/inversion sprains and medial collateral ligament (MCL) tear).
Results
A total of 35 players (mean age 18.3 ± 0.7 yr., mean body mass: 95.9 ± 9.4 kg (forwards: 99.1 ± 8.1 kg, backs: 90.9 ± 9.6 kg)) participated in the study. From pre-season to the end of competition, the squad sustained a total of 196 injuries comprising 45 time-loss (23%) and 151 transient (77%) injuries. The majority of time-loss injuries were sustained during competition matches (n = 38, 84.4%) in NYC (17 injuries, 42 missed matches), Sydney Shield/Ron Massey (17 injuries, 54 missed matches), SG Ball (3 injuries, 9 missed matches) and school (one injury, one missed match) competitions. The 45 time-loss injuries in 27 players resulted in 131 missed matches which averaged to three missed matches per injury throughout the season, and 5.5 players being unavailable for selection each competition round. Ten players (29%) sustained a transient injury. Training injuries (n=6, 13.3%) resulted in 23 missed matches (mean = 3.8 missed matches per injury). Total match play injury incidence was 7.9/1000 playing hours (transient: 6.1/1000 playing hours and time-loss: 1.8/1000 playing hours). When compared by the different competitions, the injury incidence showed no significant difference (p < 0.05) in NYC and SS/RM players but this was lower in SG Ball players (0.7/1000, 0.8/1000 and 0.4/1000 playing hours, respectively).
The most common injury sites for time-loss injuries were the shoulder, ankle/foot and knee resulting in average match loss of 2.9, 2.3 and 2.5 matches, respectively (Figure 1). There were six dislocations/subluxations, four acromioclavicular joint injuries and one rotator cuff injury recorded for the shoulder. These injuries accounted for 32 missed matches over the duration of the study. The knee injury required surgery to repair torn cartilage, while the single hamstring injury (tendon) resulted in eight missed matches.
Figure 1.
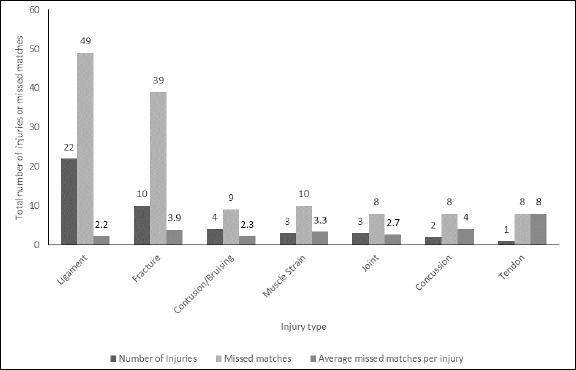
Injury number and resulting missed matches by site.
Ligament injuries (n = 22, mean = 2.2 missed matches, 36.9% of total missed matches) accounted for the highest number of injuries by type (Figure 2) including shoulder subluxations, ankle syndesmosis/inversion sprains and medial collateral ligament (MCL) tear. Fractures (mean = 3.9 missed matches, 29.7% of total missed matches) accounted for 39 missed games. Notably, of the two reported concussions (eight missed matches), one player with previous concussion history missed seven matches.
Figure 2.
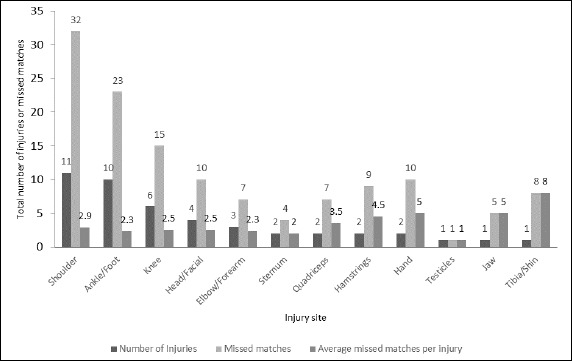
Injury number and resulting missed matches by type.
There were 91 missed matches in total as a result of contact injuries resulting in a mean of 2.8 missed matches per injury. By level of participation, the SS/RM accounted for 39.4% (n = 13) contact injuries, the NYC accounted for 36.4% (n = 12) of contact injuries and the rest (15.2%; n = 5) occurred during training activities. There were 12 non-contact injuries (muscle strains, meniscal tears and ankle/foot injuries) that were sustained in the gym during training and these accounted for 40 missed games (mean = 3.4 missed matches) over the duration of the study.
There were 17 (37.8%) minor, 13 (28.9%) moderate and 15 (33.3%) major time-loss injuries resulting in 17, 33 and 81 missed matches, respectively. Seven major injuries (46.7%, 37 missed matches) were sustained during SS matches, five (33.3%, 26 missed matches) during NYC matches and three (20%, 21 missed matches) during training. On average 5.5 players were unavailable for selection each round due to injury (Figure 3). Five major injuries (dislocated shoulder (NYC), two ankle syndesmosis sprains (NYC), fractured eye socket (SS), MCL tear (NYC); three of which required surgery) suffered in the final four rounds amounted to eight recorded games missed. Yet the true cost was estimated by medical staff as 40 missed matches.
Figure 3.
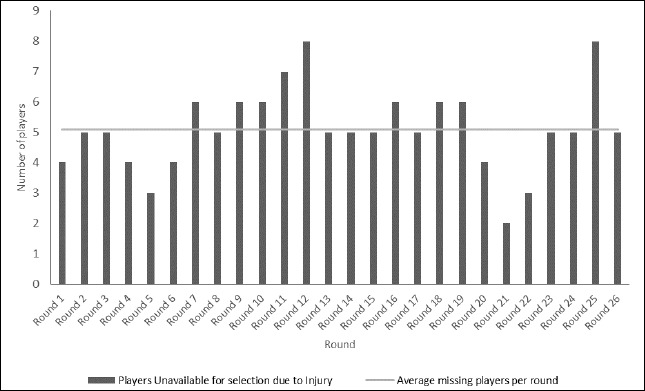
Mean number of players unavailable for selection for each competition round.
Although forwards sustained the greatest number of injuries (21 injuries resulting in 62 missed matches, mean = 3 missed matches), backs suffered the greatest injury cost (14 injuries, 45 missed matches, mean = 3.2 missed matches). Adjustables were the least injured group (9 injuries, 24 missed matches, mean = 2.7 missed matches). Shoulder injuries, contributing to the greatest number of matches missed, were predominantly sustained by adjustables (n = 5, 45.5%). However, shoulder injuries in backs resulted in the greatest severity (50% of missed matches). The majority of injuries sustained by backs occurred during SS/RM matches. Ankle injuries primarily sustained by adjustables showed the greatest cost (43.5% missed matches). Two fractures were sustained by forwards (18 missed matches) compared with backs (n = 4, 11 missed matches) and adjustables (n = 4, 10 missed matches). Backs were more severely affected by ligament injuries (4.3 missed matches/injury) than forwards and adjustables (1.8 and 2 missed matches/injury, respectively). Forwards recorded more hand and head injuries than the other positions and were the only group to sustain hamstring injuries (n = 2) and concussions (n = 2).
Although the numbers of injuries at SS (n = 14) and RM (n = 3) matches were similar to those received at NYC matches (17), the associated time-loss was greater for SS/RM 54 (41.2%) vs NYC 42 (32.1%) missed matches (Figure 4). SS/RM recorded significantly higher cost of injuries than NYC (3.2 vs 2.5 matches per injury, respectively) (p ≤ 0.05).
Figure 4.
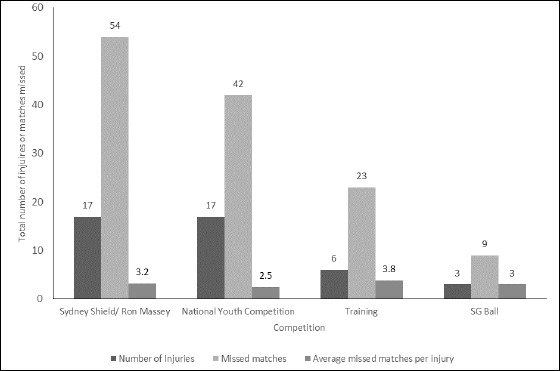
Injury number and resulting missed matches and playing level
Discussion
This is the first study to investigate the injury incidence and characteristics of a sub-elite NRL development squad and the different competitions participated in. The overall injury incidence of 7.9/1,000 playing hours was lower than previously reported in junior players (Gabbett, 2008). However, the findings in the current study indicate that the characteristics of injuries in NRL development squads are similar to those of elite level playing groups (Gabbett and Jenkins, 2011; Gabbett and Ullah, 2012). Approximately one quarter (23%) of all injuries recorded in this study resulted in missed matches. Lower limb injuries, particularly the knee and the ankle/foot, and ligament sprains and fracture/dislocations were the most prevalent injuries. Although the nature of these injuries is indicative of contact mechanisms, our observations indicate that injury severity is greater from those injuries received via non-contact mechanisms during training. These injuries were predominantly muscular strain/ tendon type injuries (e.g. hamstring) which typically require lengthy rehabilitation processes. Forwards who engage in more collisions during match play sustained a greater number of total injuries; however, the injuries sustained by outside backs were more costly in terms of mean missed matches. Furthermore, injuries to players participating in the open age competitions resulted in a higher injury cost than those playing at NYC level.
The overall injury incidence may be lower than typically observed due to the fact the algorithm used is more accurate when injury data is captured from all 17 players in the team (Orr and Cheng, 2016). Where data is not collected from every player as in this study, the aforementioned calculation may fail to account for bench time, interchanges and extra time, resulting in an underestimation of injury risk (Orr and Cheng, 2016). The total number of time-loss injuries recorded is similar to that observed in previous studies (Gabbett, 2004d; Gabbett and Jenkins, 2011). However, five significant injuries were recorded in the last four rounds of competition thereby underestimating injury incidence and severity by definition. These injuries amounted to eight recorded games missed. Yet the true cost was estimated by medical staff as 40 missed matches. In particular dislocated shoulder with an avulsion fracture (NYC) was estimated to cost 16 weeks after requiring surgery. Two ankle syndesmosis sprains (NYC) had an estimated true cost of 6 weeks each, and an MCL tear (NYC) also required surgery placing its true estimated cost at 6 weeks.
This study observed a greater number of time-loss injuries due to match play when compared with training situations. Similarly, sub-elite rugby league players have also shown greater incidence of time-loss injuries from match play when compared to training, (Gabbett, 2004c) while other studies of professional rugby league players have not (Gabbett and Jenkins, 2011). The high number of fractures (22.2%) and ligament injuries (48.8%) may be indicative of collisions experienced within match-play. Furthermore, the high proportion of shoulder injuries (24.4%) compared to previous studies (Gabbett and Domrow, 2007; Killen et al., 2010) is consistent with the higher intensities of collisions experienced from junior elite to sub-elite level competition. The severity of head injuries sustained by this cohort (concussion and multiple facial fractures) may also be subsequent to the increased intensity of contact from junior elite to sub-elite competition.
The majority of non-contact injuries (lower limb muscle strains) experienced at training cost 3.3 matches per injury. This finding is consistent with previous studies (Gabbett and Jenkins, 2011) and may be a consequence of the additional training volumes undertaken by these athletes when transitioning from junior elite to sub-elite competition.
Analysis of injury by playing level provides a valuable insight into a key aspect of injury characteristics for this cohort. While similar injury incidence was observed for both the NYC and SS/RM open age competitions, the injury cost of the latter proved to be greater. This may reflect the disparity between physical maturation and development of young SS/RM players and the fully developed adult males they were competing against for the first time in their careers. The relevance of our findings is especially highlighted by the smaller number of players in the SS/RM playing group. These players are younger (typically 18 years), therefore, not as physically developed as those competing in NYC (typically 19 years) or others in the open age competition. Additionally, these players do not receive the same level of medical treatment and rehabilitation as elite level payers (Gabbett, 2001b). Indeed, owing to a lack of financial resources at this level (a small fraction of the elite level) typically physiotherapists are employed on a part time basis providing limited treatment time. In addition, medical trainers and strength and conditioning coaches are also often employed part time or volunteers and massage therapists are not typically engaged at this level. This allows limited time for design and implementation of thorough rehabilitation programs
These findings underscore the issue of smaller, younger players playing against fully developed adult males for the first time in their career. This finding is particularly important given the current discussions about the future viability of the NYC competition format. The format will change after the 2017 season and the competition will become a state based league. Therefore, it may be advisable to reconsider the structure of such playing squads. The potential for greater injury rates with underdeveloped 17-19 year olds playing against more fully developed or adult males is reflected by the results of this study.
The limitations in this study included the standard, basic calculations used for calculating injury incidence. Exact minutes played including interchange players would allow for a more precise incidence figure. The lack of precise follow-up data on the five major injuries sustained in the final four rounds of competition leads to a further underestimation of incidence.
Future research should investigate the nature of injuries and their severity in emerging NRL talent squads. Furthermore, research into this area may highlight a need for changes to training methodologies such as the nature and volume of field training loads, resistance training and recovery methods. Investigation of field training loads should include analysis of short and long term training volumes. Moreover, as the majority of the more severe injuries in the second-tier competition were to outside backs (being of smaller stature and body mass), future research may assist to guide more discerning selection policies of coaching staff.
Conclusion
NRL development and emerging rugby league players are exposed to high risk of injury. Lower limb and shoulder injuries to bone or connective tissue are prevalent as a result of contact during match play. Players at this developmental level feed into several different playing squads where disparities in physical development, maturation, playing intensity and training regimes are evident. The present challenges for rugby league administrators exist in matching physiological capabilities with playing demands for NRL development squads and emerging players. Given the complex nature of the physiological development/competitive demands paradox, it would be prudent for high performance teams to monitor training programs and implement professional injury prevention strategies at the second-tier level of development.
Biographies
Mark BOOTH
Employment
Sport Scientist Canterbury Bulldogs
Degree
MaClinExPhys&Rehab, MaExSci (Strngth&Cond), MaNut/Diet, BaAppSci (Ex&SpSci)
Research interests
Training load, injury surveillance, performance enhancement, rugby league, GPS
E-mail: mark.booth@sydney.edu.au
Rhonda ORR
Employment
Senior Lecturer, Discipline of Exercise and Sport Science, The University of Sydney
Degree
BPharm, MExSpSc, PhD
Research interests
Sports injury, concussion, GPS, rugby league, performance enhancement, sports science
E-mail: rhonda.orr@sydney.edu.au
References
- Brito J., Malina R.M., Seabra A., Massada J.L., Soares J.M., Krustrup P., Rebelo A. (2012) Injuries in Portuguese youth soccer players during training and match play. Journal Athletic Training 47, 191-197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks J.H., Fuller C.W., Kemp S.P., Reddin D.B. (2008) An assessment of training volume in professional rugby union and its impact on the incidence, severity, and nature of match and training injuries. Journal of Sports Sciences 26, 863-873. [DOI] [PubMed] [Google Scholar]
- Centre N.I.R.M.R. (2006) A profile of hospitalisations and deaths due to sport and leisure injuries in New South Wales, 2000-2004. IRMRC, Ed. [Google Scholar]
- Cheng H.L., O'Connor H., Kay S., Cook R., Parker H., Orr R. (2014) Anthropometric characteristics of Australian junior representative rugby league players. Journal of Science and Medicine in Sport 17, 546-551. [DOI] [PubMed] [Google Scholar]
- Drew M.K., Finch C.F. (2016) The Relationship Between Training Load and Injury, Illness and Soreness: A Systematic and Literature Review. Sports Medicine 46(6), 861-883. [DOI] [PubMed] [Google Scholar]
- Fortington L.V., Berry J., Buttifant D., Ullah S., Diamantopoulou K., Finch C.F. (2016) Shorter time to first injury in first year professional football AFL players. Journal of Science and Medicine in Sport 19(1)18-23. [DOI] [PubMed] [Google Scholar]
- Gabbett T. (2001a) Performance, fatigue and injuries in rugby league. Rugby League Coaching Manuals; 22-26. [Google Scholar]
- Gabbett T., King T., Jenkins D. (2008) Applied physiology of rugby league. Sports Medicine 38, 119-138. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J. (2000) Incidence, site, and nature of injuries in amateur rugby league over three consecutive seasons. British Journal of Sports Medicine 34, 98-103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gabbett T.J. (2001b) Severity and cost of injuries in amateur rugby league: a case study. Journal of Sports Sciences 19, 341-347. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J. (2002) Physiological characteristics of junior and senior rugby league players. British Journal of Sports Medicine 36, 334-339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gabbett T.J. (2003a) Incidence of injury in semi-professional rugby league players. British Journal of Sports Medicine 37, 36-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gabbett T.J. (2003b) Incidence of injury in semi-professional rugby league players. British Journal of Sports Medicine 37, 36-43; discussion 43-4, Feb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gabbett T.J. (2004a) Influence of injuries on team playing performance in Rugby League. Journal of Science and Medicine in Sport 7, 340-346. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J. (2004b) Influence of training and match intensity on injuries in rugby league. Journal of Sports Sciences 22, 409-417. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J. (2004c) Influence of training and match intensity on injuries in rugby league. Journal of Sports Sciences 22, 409-417. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J. (2004d) Reductions in pre-season training loads reduce training injury rates in rugby league players. British Journal of Sports Medicine 38, 743-749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gabbett T.J. (2005) Science of rugby league football: a review. Journal of Sports Sciences 23, 961-976. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J. (2008) Incidence of injury in junior rugby league players over four competitive seasons. Journal of Science and Medicine in Sport 11, 323-328. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J. (2009) Physiological and anthropometric correlates of tackling ability in rugby league players. Journal of Strength and Conditioning Research 23, 540-548. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J., Domrow N. (2005) Risk factors for injury in subelite rugby league players. American Journal Sports Medicine 33, 428-434. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J., Domrow N. (2007) Relationships between training load, injury, and fitness in sub-elite collision sport athletes. Journal of Sports Sciences 25, 1507-1519. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J., Jenkins D.G. (2011) Relationship between training load and injury in professional rugby league players. Journal of Science and Medicine in Sport 14, 204-209. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J., Jenkins D.G., Abernethy B. Relationships between physiological, anthropometric, and skill qualities and playing performance in professional rugby league players. Journal of Sports Sciences 29, 1655-1664. [DOI] [PubMed] [Google Scholar]
- Gabbett T.J., Ullah S. (2012) relationship between running loads and soft-tissue injury in elite team sport athletes. Journal of Strength and Conditioning Research 26, 953-960. [DOI] [PubMed] [Google Scholar]
- Killen N.M., Gabbett T.J., Jenkins D.G. (2010) training loads and incidence of injury during the preseason in professional rugby league players. Journal of Strength and Conditioning Research 24, 2079-2084. [DOI] [PubMed] [Google Scholar]
- King D.A., Gabbett T.J., Gissane C., Hodgson L. (2009) Epidemiological studies of injuries in rugby league: suggestions for definitions, data collection and reporting methods. Journal of Science and Medicine in Sport 12, 12-19. [DOI] [PubMed] [Google Scholar]
- King D.A., Hume P.A., Milburn P.D., Guttenbeil D. (2010a) Match and Training Injuries in Rugby League. Sports Medicine 40, 163-178. [DOI] [PubMed] [Google Scholar]
- King D.A., Hume P.A., Milburn P.D., Guttenbeil D. (2010b) Match and training injuries in rugby league: a review of published studies. Sports Medicine 40, 163-178. [DOI] [PubMed] [Google Scholar]
- Meir R. (1994) A model for the integration of macrocycle and microcycle structure in professional rugby league. Strength & Conditioning Coach 2, 6-12. [Google Scholar]
- Orchard J.W. (2009) On the value of team medical staff: can the "Moneyball" approach be applied to injuries in professional football? British Journal of Sports Medicine 43, 963-965. [DOI] [PubMed] [Google Scholar]
- Orr R., Cheng H.L. (2016) Incidence and characteristics of injuries in elite Australian junior rugby league players. Journal of Science and Medicine in Sport 19, 212-217. [DOI] [PubMed] [Google Scholar]
- Statistics A.B.o. (2003) National health survey: Injuries, Australia 2001, Statistics, A.B.o., Ed, Canberra, Australia. [Google Scholar]
- Stephenson S., Gissane C., Jennings D. (1996) Injury in rugby league: a four year prospective survey. British Journal of Sports Medicine 30, 331-334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Mechelen W., Hlobil H., Kemper H.C. (1992) Incidence, severity, aetiology and prevention of sports injuries. Sports Medicine 14, 82-99. [DOI] [PubMed] [Google Scholar]