

Abstract
Background:
Apart from the mortality, road traffic injuries are associated with significant morbidities. This study has aimed to examine the pattern of traffic accident-related extremity fractures/dislocations and their related disabilities.
Methods:
A retrospective hospital-based study was conducted to assess the characteristics of limb fractures/dislocations among road traffic accident victims registered in Trauma Research Center registry of Kashan University of Medical Sciences, Kashan, Iran, during 2012-2013. Age and sex distribution, cause of injury, and site of fractures/dislocations were recorded. Years lived with disability (YLD) was calculated as a scale to measure the disability. One-way ANOVA and chi-square tests were used for data analysis.
Results:
From a total of 962 subjects, 812 (84.4%) were males (the male/female sex ratio: 5.4:1). The mean age of victims was 32.7±17.9. Leg (37%) and forearm (19%) fractures were the most frequent fractures. Shoulder dislocations were among the most affected joints accounting for 36.6% of the cases. The total calculated YLD was 135.6 (34.4 for temporal and 101.2 for lifelong disabilities, and totally 117.3 and 18.3 for males and females, respectively). The highest YLD was for motorcyclists (104) and while the most YLD was for 15-29 years (68.2).
Conclusion:
Young men motorcyclist accidents are a major problem in Kashan region. Generally, they have been accounted for the highest YLD due to fractures/dislocations, especially in lower extremity. Although the calculated YLD will be decreased with increasing age, the elder people also had the high rate of traffic-related limb injuries.
Keywords: Dislocation, Fracture, Road traffic accident, Years lived with disability
Introduction
Road traffic injuries (RTIs) as the 9th leading cause of death worldwide (2nd in Iran) are a major public health problem (1, 2). Apart from the RTIs burden on the society in terms of death, 20-50 million people suffer from non-fatal injuries annually. Most of these injuries cause disability and account for 34% of all years lived with disability (YLDs) (3, 4). In Iran, road traffic accidents (RTAs) kill almost 28,000 people and injure or disable over 300,000 annually (5). Road traffic accidents have repeatedly been documented as the cause of most fractures, especially in developing low-income countries (6). The survivors and their families usually experience unfavorable social, physical and psychological effects. Many families face problems with prolonged medical care costs or the extra funds needed to care for disabled people (7). On the other hand, temporary unemployment or early retirement after injury imposes great costs to the insurance companies and society. Most of the epidemiological studies conducted in Iran have emphasized on different aspects of RTIs like patterns, mortality rate, demographic characteristics of the victims, and some other features like costs while less attention has been paid to disabilities, especially those caused by extremity injuries (8-13). The YLDs is the number of years that somebody lives with health problems and depends on the severity of the disability. People in car, motorcycle, or other accidents often have multiple bone fractures. Although most fractures heal with no permanent injury and only disable the injured ones for a short time, there are several complications that can occur with broken bones and may lead to long-life disabilities. Knowing the pattern of the extremity fractures as the most common RTA fractures is very important for policymakers and strategy planners with great impact on public emergency services, health and rehabilitation centers to determine priorities, apply preventive strategies and improve the services provided (14, 15). This study has aimed to determine the pattern of the extremity fractures and dislocations in RTA victims admitted to a level III trauma center in Kashan, Iran, during a one-year period with emphasis on the disability caused by such fractures in terms of YLDs.
Materials and Methods
The approval to conduct this study was provided by the ethics committee of Kashan University of Medical Sciences (KAUMS). Throughout a retrospective descriptive hospital- based study, the registration system of Trauma Research Center of KAUMS, Kashan, Iran, from March 2012 to March 2013 was used for data analysis. This registry covers all governmental hospitals. Since the treatment cost for traffic casualties is free in Iran, most victims of traffic accidents are referred to governmental hospitals for treatment; however, the information from the only private hospital in the region was also collected to prevent possible dropout cases of discharge due to personal satisfaction. The duplicate cases in terms of name, national code, type of injury, and date of accidents were removed. The International Classification of Diseases and Causes of Death (ICD 10) codes for orthopedic traffic injury admissions were used for data analysis. Finally, 962 RTI victims with extremity fractures and valid ICD-10 codes from Kashan region (including Kashan and Aran-Bidgol counties) that led to hospital filing were included in this study. The age and gender composition of Kashan Region in 2012 were provided by the department of statistics, KAUMS. The global burden of disease (GBD) approach was used to calculate YLDs (16). The YLDs calculation for orthopedic traumas needs estimates of injury incidence, average duration of associated disability, and the disability weight. A disability weight indicates the average severity of any physical disability associated with each injury. The disability weights are expressed as a number on a scale from 0 to 1, with 0 representing the ideal health and 1 representing death. YLD is calculated as follows:

where i is the injury, x is the age and gender category, N is the number of incident cases, DW is the disability weight and L is the average duration (17).
A case the incident of trauma was defined as a serious enough event to necessitate treatment by the emergency services or hospitalization (17). Our trauma registry system met these criteria. Assuming that all RTI victims have been finally referred to one of the regional hospitals, the number of registered cases in the health centers as traffic injury victims was considered as incidence. All injuries were also assumed as treated.
For the purposes of the present study, it was decided to use the disability weights determined by the WHO as used in the original global burden of disease study and national burden of disease in Iran (18). The short and long-term GBD durations for injuries were used as the duration of disability (19). The duration of lifelong injuries was based on the remaining life expectancy of the person. Thus, it was assumed that a lifelong injury would not reduce the life-expectancy of the casualty. The remaining life expectancy data were calculated based on the life table that was used in the previous burden of disease studies (20).
Only one injury (the injury with the highest YLD) was included in victims with multiple fractures to avoid unrealistically high calculated YLDs (20, 21). The YLDs were only calculated for upper and lower extremity fractures and dislocations.
Data analysis was done by SPSS software version 16.0 (SPSS Inc., Chicago, Illinois, USA) using one-way ANOVA and chi-square test. A P<0.05 was considered as statistically significant.
Results
For the one year study period, 2206 cases with valid ICD-10 codes were recorded as hospitalized road traffic accident victims in Kashan region; among whom, 962 cases (812 males (84.4%), a male/female sex ratio of 5.4:1) had limb fractures and dislocations based on the corresponded codes and were enrolled in the study. Multiple traumas were observed in about 25% of the victims. As shown in Table 1, leg (tibia and fibula) (37.6%) and forearm (radius and ulna) (19.3%) had the most frequent fractures. Shoulder dislocations were the most common joint dislocations, accounting for 2.7% of the cases. Regarding the mechanism of limb injuries, the highest percentage of upper extremity injuries was found in bicyclists (64.7% P=0.03), while the highest percentage of lower extremity fracture was found in pedestrians (67.7%), followed by motorcyclists (62.2% P=0.04) [Table 2]. Men and women were constituted as the majority of motorcyclists (92.6%) and pedestrian victims (41.4%) (P=0.000), respectively [Table 2]. Although the most frequent extremity fracture/dislocation rate was observed in 15-29 year age group (416 cases, 43.2%), elder people (age>60 y) also had a high rate of traffic-related limb injuries (262 per 100000) [Table 2; Figure 1]. A significant difference was found between the mean age of traffic limb injured cases regarding the mechanism of injury (P=0.000) [Table 2]. Motorcyclists had the lowest (30.9 ± 15.70) and pedestrians had the highest (38 ± 24.9) mean age.
Table 1.
Disrtibution of fractures and dislocations
| Fractures | No. | % |
|---|---|---|
| Bone | ||
| Femur | 139 | 14.4 |
| Tibia and fibula | 362 | 37.6 |
| Radius and ulna | 186 | 19.3 |
| Humerus | 39 | 4 |
| Clavicle | 41 | 4.3 |
| Pelvis | 32 | 3.3 |
| Hand | 110 | 11.4 |
| Foot | 53 | 5.5 |
| Patella | 17 | 1.8 |
| Dislocations | ||
| Joint | ||
| Hip | 14 | 1.5 |
| Shoulder | 26 | 2.7 |
| Ankle | 9 | 0.9 |
| Wrist | 10 | 1 |
| Elbow | 9 | 0.9 |
| Knee | 3 | 0.3 |
Table 2.
Study variables based on vehicle used by Upper and Lower limb injured† victims
| Variable | Type of vehicle | P | |||||
|---|---|---|---|---|---|---|---|
| Pedestrian No (%) | Motorcycle No (%) | Car No (%) | Bicycle No (%) | Total No (%) | |||
| Upper extremity | 0.03 | ||||||
| Yes | 45 (33.8) | 274 (39.3) | 52(45.6) | 11(64.7) | 382 (39.7) | ||
| No | 88 (66.2) | 424 (60.7) | 62 (54.4) | 6 (35.3) | 580 (60.3) | ||
| Lower extremity | 0.04 | ||||||
| Yes | 90 (67.7) | 434 (62.2) | 64 (56.1) | 6 (35.3) | 594 (61.7) | ||
| No | 43 (32.3) | 264 (37.8) | 50 (43.9) | 11 (64.7) | 368 (38.3) | ||
| Gender | <0.001 | ||||||
| Male | 78 (58.6) | 646 (92.6) | 73 (64) | 15 (88.2) | 812 (84.4) | ||
| Female | 55 (41.4) | 52 (7.4) | 41 (36) | 2 (11.8) | 150 (15.6) | ||
| Age [mean(SD)] | 38 (24.9) | 30.9 (15.7) | 36.7 (17.5) | 36.8 (27.5) | 32.6 (17.9) | <0.001 | |
| Age group | <0.001 | ||||||
| <15 Year | 34 (25.6) | 45 (6.4) | 8 (7) | 5 (29.4) | 92 (9.6) | ||
| 15-29 | 22 (16.5) | 353 (50.6) | 37 (32.5) | 4 (23.5) | 416 (43.2) | ||
| 30-44 | 24 (18) | 168 (24.1) | 32 (28.1) | 1 (5.9) | 225 (23.4) | ||
| 45-59 | 15 (11.3) | 77 (11) | 26 (22.8) | 2 (11.8) | 120 (12.5) | ||
| >60 | 38 (28.6) | 55 (7.9) | 11 (9.6) | 5 (29.4) | 109 (11.3) | ||
| Total | 133 (100) | 698 (100) | 114 (100) | 17 (100) | 962 (100) | ||
| Type of injury | |||||||
| Dislocation | 0.4 | ||||||
| Yes | 6(2.1) | 45(3) | 6(1.6) | 3(5.3) | 60(2.7) | ||
| No | 285(97.9) | 1460(97) | 347(98.4) | 54(94.7) | 2146(97.3) | ||
| Fracture | <0.001 | ||||||
| Yes | 123(42.3) | 671(44.6) | 113(32) | 14(24.6) | 921(97) | ||
| NO | 168(57.7) | 834(55.4) | 240(68) | 43(75.4) | 41(3) | ||
Including fractures and dislocations only
Figure 1.
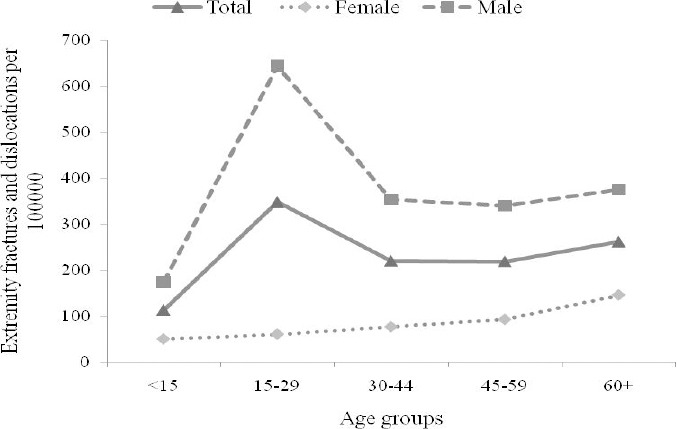
Extremities’ fractures and dislocations based on age and sex groups per 100000 populations.
Generally, the mean age of casualties was 32.7±17.9 years (31.7±17.4 for males and 37.6±20.3 for females, P=0.000). The total calculated YLD was nearly 135.6 (YLDs for temporal and lifelong disabilities were 34.4, and 101.2 respectively totally, 117.3 for males and 18.3 for females, 125.6 for lower limb and 10 for upper limb). The most YLD among fractures and dislocations was accounted for the femur fractures either for short-term or for lifelong (8 and 101.2, respectively), followed by tibia and fibula fractures (8). Based on the mechanism of injury, the most calculated YLD was accounted for motorcyclists (104), about 5 times more than the pedestrians. The highest YLD was accounted for 15-29 years patients (68.2) [Table 3].
Table 3.
Years lived with disability based on limb, mechanism of injury and age group
| Limb fracture-dislocation | Number of YLD | ||||||
|---|---|---|---|---|---|---|---|
| Male | Female | Total | |||||
| Temporal disability | Lifelong disability | Total | Temporal disability | Lifelong disability | Total | ||
| Upper limb | 8 | - | 8 | 2 | - | 2 | 10 |
| Lower limb | 19.1 | 90.2 | 109.3 | 5.3 | 11 | 16.3 | 125.6 |
| Total | 27.1 | 90.2 | 117.3 | 7.3 | 11 | 18.3 | 135.6 |
| Type of vehicle used by victims | |||||||
| Pedestrians | 15 | 6 | 21 | ||||
| Motorcycles | 93 | 11 | 104 | ||||
| Car | 9 | 1.2 | 10.3 | ||||
| Bicycle | 0.3 | 0.1 | 0.4 | ||||
| Total | 117.3 | 18.3 | 135.6 | ||||
| Age group | |||||||
| <15 | 12.1 | 6 | 18.1 | ||||
| 15-29 | 60.2 | 8 | 68.2 | ||||
| 30-44 | 34 | 2.1 | 36.1 | ||||
| 45-59 | 7 | 0.7 | 7.7 | ||||
| +60 | 4 | 1.5 | 5.5 | ||||
| Total | 117.3 | 18.3 | 135.6 | ||||
Discussion
This study considered 962 cases of RTA victims with extremity fractures and dislocations during one- year period. Fractures were observed more in lower extremities with tibia and fibula as the most fractured bones, followed by femur. Our findings seem to be consistent with other similar researches (22-26). The lower extremity fracture was the most frequent fracture among pedestrians while cyclists were the second vulnerable group to this type of injury. A similar study in Iran showed the same results (1). The high number of pedestrian lower extremity fractures could be attributed to the following issues: The drivers’ lack of respect for pedestrians, especially when crossing the crosswalk was a major problem in our region. In addition, law enforcement against the offending drivers is very weak.
Motorcycles are a common mode of transportation in small cities in Iran. Kashan City is not an exception and a recent study in Kashan showed that the motorcyclists were responsible for the most prevalent percentage of RTA victims (27). On the other hand, series of studies have shown that lower extremity fractures in motorcyclists are dominant among limb injuries (1, 5, 22, 28). Similar to the findings of Parreira, motorcyclists had the lowest mean age among other victims in our study (29). Youth drivers were considerably more likely to be involved in RTAs mainly due to the lack of enough experience as well as risky behaviors due to peer relationships (30, 31). In the present study, most of the injured victims were young men similar to the findings of many other studies (1, 7, 32, 33). Given that most of the injured cases were motorcyclists and the fact that about 57% of them were under 29 years old and on the other hand, lower extremity fracture was the most common fracture among motorcyclists, the higher YLD in this group is justifiable. It should be noted that lower limb fractures are accompanied with more disability years compared to upper limb fractures. Moreover, Injury at a young age is associated with more YLD.
Investment on public education in this age group, encouraging motorcyclists to wear safety guards and strict law enforcement may help to reduce such complications. Male predominance for bones and joint injuries could be attributed to the men’s involvement in more out-doors activities than women as breadwinners in our traditional society.
Despite the higher rate of extremity injuries in the 15-29 age group (384.5/100000), the second vulnerable group is people aged above 60 with the fracture/dislocation rate of 262/100000. Age-related changes affect many organ systems and finally lead to cognitive and motor function impairments, resulting in restricted movements and increased reaction time (34). Moreover, the frequency of fractures is increased with osteoporosis, which is a common finding in this age group. As a result, the risk of limb fracture will be increased in this population as well.
In this study, disability was considered as another aspect of RTA-related limb fractures and dislocations. For the purpose of this study to show health problems caused by limb fractures and dislocations it was decided to use YLD, the disability component of disability-adjusted life year, DALYs. YLD is defined as the years of productive life lost due to disability (17). Limb injuries, especially lower limb fractures may cause temporary motion restrictions. In some cases such as hip and femur fractures permanent gait problems may occur (35). In the present study, the most calculated YLDs was accounted for young men (15-29 y) and among motorcyclists. To the best of our knowledge, a few studies have dealt with transport mode specific YLDs and the details about YLDs caused by just limb fractures. Our findings are consistent with those of Lapostolle et al. (2009) who found 278 fracture-related YLD for a 5-year period (annual average of 55.6) in 15-24 year-old male victims of RTAs and also in line with Thailand national burden of road traffic injuries (17, 36).
There are some limitations regarding the present study. Firstly, traffic-related injuries to head, spine and trunk in RTAs victims have not been addressed in this study. Despite the fact that many victims in our study had multiple traumas, only limb fractures/dislocations have been considered. Undoubtedly, injury to these organs is a source of major disability. Secondly, soft tissue injuries and amputations were not also included in this study. However, as mentioned previously, the present study has aimed to focus on limb fractures and dislocations as one of the main important complications of traffic injuries. The strength of this study is to address the disability caused by the limb fractures due to traffic accidents in addition to transport mode specific YLDs.
In conclusion, the most obvious findings to emerge from this study are that traffic accidents are a leading cause of bone fractures and YLD especially in individuals between 15 – 29 years old. Males were observed to be mainly involved with the lower extremity fractures and related YLD. The largest number of limb fracture victims with the highest YLD was seen among the motorcyclists.
As the motorcycle crashes were the most leading cause of limb fracture, paying attention to motorcyclists is particularly important. Since the emphasis has been taken on helmet use in motorcyclists, less attention has been paid to protect extremities. It seems that due to the high incidence of lower extremity injuries and related disability in motorcyclists, it is rational to provide some strategies to protect the lower limb against traumas during motorcycle crashes. Emphasis on the use of mandatory lower limb safety guards in motorcycles and wearing of personal protective equipment such as protective clothing by motorcyclists seems logical. Furthermore, it is recommended that some complementary strategies like imparting minimum education regarding safer driving during giving license, especially to motorcyclists and more serious law enforcement be implemented (24). Improvements in infrastructures of hospitals and clinics regarding new surgical techniques and equipment and especially developing rehabilitation centers are necessary to reduce disability burden of traffic-related limb injuries.
Acknowledgments
This study was a part of PhD dissertation, supported by deputy of research, Kashan University of Medical Sciences (Grant no. 92173).
References
- 1.Soroush D, Talebi Deloei M, Reihani H, Vakili V, Mahmoodi Gharaee A, Tafakori A, et al. Characteristics of road traffic injuries in the second largest city of Iran. J Emerg Pract Trauma. 2015;1(2):48–51. [Google Scholar]
- 2.Dalal K, Lin Z, Gifford M, Svanström L. Economics of global burden of road traffic injuries and their relationship with health system variables. Int J Prev Med. 2013;4(12):1442–50. [PMC free article] [PubMed] [Google Scholar]
- 3.World Health Organization. WHO global status report on road safety 2013:supporting a decade of action. Geneva: World Health Organization; 2013. [Google Scholar]
- 4.Gabbe BJ, Lyons RA, Fitzgerald MC, Judson R, Richardson J, Cameron PA. Reduced population burden of road transport-related major trauma after introduction of an inclusive trauma system. Ann Surg. 2015;261(3):565–72. doi: 10.1097/SLA.0000000000000522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zargar M, Khaji A, Karbakhsh M. Pattern of motorcycle-related injuries in Tehran 1999 to 2000:a study in 6 hospitals. Eastern Mediterran Health J. 2006;12(1-2):81–7. [PubMed] [Google Scholar]
- 6.Thanni LO, Kehinde OA. Trauma at a Nigerian teaching hospital:pattern and documentation of presentation. Afr Health Sci. 2006;6(2):104–7. doi: 10.5555/afhs.2006.6.2.104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Celine TM, Antony J. A study on injuries sustained in road traffic accidents at a tertiary care level. Int J Environ Health Engine. 2014;3(1):23. [Google Scholar]
- 8.Ainy E, Soori H, Riahi M, Vahabzadeh E, Mohebi A, Amiri M. The effect of new road traffic laws on fatal and non-fatal injury rates in Iran. Int J Epidemiol Res. 2014;1(1):16–23. [Google Scholar]
- 9.Bahadorimonfared A, Soori H, Mehrabi Y, Delpisheh A, Esmaili A, Salehi M, et al. Trends of fatal road traffic injuries in Iran (2004–2011) PLoS One. 2013;8(5):e65198. doi: 10.1371/journal.pone.0065198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hasanzadeh J, Moradinazar M, Najafi F, Ahmadi-Jouybary T. Trends of mortality of road traffic accidents in Fars province, southern Iran 2004–2010. Iran J Public Health. 2014;43(9):1259–65. [PMC free article] [PubMed] [Google Scholar]
- 11.Heydari ST, Hoseinzadeh A, Ghaffarpasand F, Hedjazi A, Zarenezhad M, Moafian G, et al. Epidemiological characteristics of fatal traffic accidents in Fars province, Iran:a community-based survey. Public Health. 2013;127(8):704–9. doi: 10.1016/j.puhe.2013.05.003. [DOI] [PubMed] [Google Scholar]
- 12.Moharamzad Y, Taghipour H, Hodjati Firoozabadi N, Hodjati Firoozabadi A, Hashemzadeh M, Mirjalili M, et al. Mortality pattern according to autopsy findings among traffic accident victims in Yazd, Iran. Chin J Traumatol. 2008;11(6):329–34. doi: 10.1016/s1008-1275(08)60067-x. [DOI] [PubMed] [Google Scholar]
- 13.Paravar M, Hosseinpour M, Salehi S, Mohammadzadeh M, Shojaee A, Akbari H, et al. Pre-hospital trauma care in road traffic accidents in kashan, Iran. Arch Trauma Res. 2013;1(4):166–71. doi: 10.5812/atr.8780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pan RH, Chang NT, Chu D, Hsu KF, Hsu YN, Hsu JC, et al. Epidemiology of orthopedic fractures and other injuries among inpatients admitted due to traffic accidents:a 10-year nationwide survey in Taiwan. Sci World J. 2014;2014:637872. doi: 10.1155/2014/637872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Elachi IC, Yongu WT, Odoyoh OO, Mue DD, Ogwuche EI, Ahachi CN. An epidemiological study of the burden of trauma in Makurdi, Nigeria. Int J Crit Illn Inj Sci. 2015;5(2):99–102. doi: 10.4103/2229-5151.158404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jiang Y, Hesser JE. Using disability-adjusted life years to assess the burden of disease and injury in Rhode Island. Public Health Rep. 2012;127(3):293–303. doi: 10.1177/003335491212700309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lapostolle A, Gadegbeku B, Ndiaye A, Amoros E, Chiron M, Spira A, et al. The burden of road traffic accidents in a French Departement:the description of the injuries and recent changes. BMC Public Health. 2009;9(1):386. doi: 10.1186/1471-2458-9-386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Naghavi M, Abolhassani F, Pourmalek F, Lakeh MM, Jafari N, Vaseghi S, et al. The burden of disease and injury in Iran 2003. Popul Health Metr. 2009;7(1):9. doi: 10.1186/1478-7954-7-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Murray CJ, Lopez AD. Global burden of disease. Boston: Harvard University Press; 1996. [Google Scholar]
- 20.Tainio M, Olkowicz D, Teresi G, De Nazelle A, Nieuwenhuijsen MJ. Severity of injuries in different modes of transport, expressed with disability-adjusted life years (DALYs) BMC Public Health. 2014;14(1):765. doi: 10.1186/1471-2458-14-765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dhondt S, Pirdavani A, Macharis C, Bellemans T, Putman K. Translating road safety into health outcomes using a quantitative impact assessment model. Inj Prev. 2012;18(6):413–20. doi: 10.1136/injuryprev-2011-040286. [DOI] [PubMed] [Google Scholar]
- 22.Batista Fdos S, Silveira LO, Castillo JJ, de Pontes JE, Villalobos LD. Epidemiological profile of extremity fractures in victims of motorcycle accidents. Acta Ortop Bras. 2015;23(1):43–6. doi: 10.1590/1413-78522015230100998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Enweluzo GO, Giwa SO, Obalum DC. Pattern of extremity injuries in polytrauma in Lagos, Nigeria. Niger Postgrad Med J. 2008;15(1):6–9. [PubMed] [Google Scholar]
- 24.Ganveer GB, Tiwari RR. Injury pattern among non-fatal road traffic accident cases:a cross-sectional study in Central India. Indian J Med Sci. 2005;59(1):9–12. [PubMed] [Google Scholar]
- 25.Kara H, Bayir A, Ak A, Akinci M, Tufekci N, Degirmenci S, et al. Trauma in elderly patients evaluated in a hospital emergency department in Konya, Turkey:a retrospective study. Clin Interv Aging. 2014;9(1):17–21. doi: 10.2147/CIA.S56542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gichuhi K. Injury pattern among non-fatal road traffic crash victims. East Afr Orthop J. 2007;1(1):23–5. [Google Scholar]
- 27.Mahdian M, Sehat M, Fazel MR, Moraveji A, Mohammadzadeh M. Epidemiology of urban traffic accident victims hospitalized more than 24 hours in a level III trauma center, Kashan county, Iran, during 2012-2013. Arch Trauma Res. 2015;4(2):e28465. doi: 10.5812/atr.4(2)2015.28465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Lateef F. Riding motorcycles:is it a lower limb hazard? Singapore Med J. 2002;43(11):566–9. [PubMed] [Google Scholar]
- 29.Parreira JG, Gregorut F, Perlingeiro JA, Solda SC, Assef JC. Comparative analysis of injuries observed in motorcycle riders involved in traffic accidents and victims of other blunt trauma mechanisms. Rev Assoc Med Bras. 2012;58(1):76–81. [PubMed] [Google Scholar]
- 30.Subramanian R. Motor vehicle traffic crashes as a leading cause of death in the United States. Young. 2002;2005;1(3):1–2. [Google Scholar]
- 31.Arnett JJ. Developmental sources of crash risk in young drivers. Inj Prev. 2002;8(Suppl 2):ii17–23. doi: 10.1136/ip.8.suppl_2.ii17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Seid M, Azazh A, Enquselassie F, Yisma E. Injury characteristics and outcome of road traffic accident among victims at Adult Emergency Department of Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia:a prospective hospital based study. BMC Emerg Med. 2015;15(1):10. doi: 10.1186/s12873-015-0035-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ortho RS, Ali L, Ubbot M. The epidemiology of fractures and dislocations at district hospital Kathua (J&K) JK-Practitioner. 2007;14(2):114–7. [Google Scholar]
- 34.Elderly Safety-Focus on Accidental Injuries. Fact sheet:prevention of road traffic injuries among elderly. Barcelona, Spain: European Network for Safety Among Elderly; 2006. [Google Scholar]
- 35.Kline Mangione K, Craik RL, Lopopolo R, Tomlinson JD, Brenneman SK. Predictors of gait speed in patients after hip fracture. Physiother Can. 2008;60(1):10–8. doi: 10.3138/physio/60/1/10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ditsuwan V, Veerman LJ, Barendregt JJ, Bertram M, Vos T. The national burden of road traffic injuries in Thailand. Popul Health Metr. 2011;9(1):2. doi: 10.1186/1478-7954-9-2. [DOI] [PMC free article] [PubMed] [Google Scholar]