

Abstract
The 3-hydroxy-methylglutaryl coenzyme A reductase inhibitors (statins), have been used for thirty years to prevent coronary artery disease and stroke. Their primary mechanism of action is the lowering of serum cholesterol through inhibiting hepatic cholesterol biosynthesis thereby upregulating the hepatic low-density lipoprotein (LDL) receptors and increasing the clearance of LDL-cholesterol (LDL-C). Statins may exert cardiovascular protective effects that are independent of LDL-C lowering called “pleiotropic” effects. Because statins inhibit the production of isoprenoid intermediates in the cholesterol biosynthetic pathway, the post-translational prenylation of small guanosine triphosphate binding proteins such as Rho and Rac, and their downstream effectors such as Rho kinase and nicotinamide adenine dinucleotide phosphate oxidases are also inhibited. In cell culture and animal studies, these effects alter the expression of endothelial nitric oxide synthase, the stability of atherosclerotic plaques, the production of pro-inflammatory cytokines and reactive oxygen species, the reactivity of platelets, and the development of cardiac hypertrophy and fibrosis. The relative contributions of statin pleiotropy to clinical outcomes, however, remain a matter of debate and are hard to quantify since the degree of isoprenoid inhibition by statins correlates to some extent with the amount of LDL-C reduction. This review examines some of the currently proposed molecular mechanisms for statin pleiotropy and discusses whether they could have any clinical relevance in cardiovascular disease.
Introduction
Cardiovascular diseases remain the leading cause of death worldwide.1 The development of coronary atherosclerosis involves a complex interplay between metabolic and inflammatory processes.2 Mechanistic and genetic evidence shows that apolipoprotein B (ApoB) containing lipoproteins, specifically low-density lipoprotein cholesterol (LDL-C) is causal for atherogenesis.3 Statins or 3-hydroxy-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors, decrease cholesterol biosynthesis and decrease serum LDL-C and triglyceride levels 4 Landmark clinical trials have demonstrated the efficacy of statins for both primary and secondary prevention of coronary heart disease (CHD).5-17 It has been proposed that statins exert both LDL-C-dependent and LDL-C-independent (or pleiotropic) effects.18 Clinical studies show statin benefits in diseases that are not clearly related to LDL-C (Table 1), but some of the outcomes may be due to direct cholesterol lowering.19-30 Decreased gallstone formation could be due to decreased hepatic cholesterol formation, decreased cholesterol reduces platelet aggregation and could lead to less deep vein thrombosis, and decreased cholesterol could affect the progression of renal disease by decreasing renal artery atherosclerosis.20,25,31 The clinical significance of the pleiotropic effects of statins in the cardiovascular system remains controversial given the overwhelming benefits of cholesterol reduction in preventing cardiovascular events.
Table 1.
The effect of statins on LDL-C independent diseases
| Kidney disease | ↓ Creatinine with normal and abnormal renal function19,20 |
| Pneumonia | ↓ Incidence22 |
| ↓ Mortality21 | |
| Venous thromboembolism | ↓ Incidence31 |
| Multiple Sclerosis | ↓ Whole brain atrophy23 |
| ↓ Disability23 | |
| Bone strength | ↓ Hip fracture in postmenopausal women24 |
| Gastrointestinal | ↓ Cholecystectomy for gallstones25 |
| ↓ Pancreatitis with normal triglycerides26 | |
| Erectile dysfunction | ↑ Function in sildenafil nonresponders27 |
| Periodontal disease | ↓ Periodontal inflammation28 |
| Rheumatoid arthritis | ↓ Mortality29 |
| ↓ Inflammatory markers and improved disease activity score30 |
Pharmacokinetic Properties of Statins
HMG-CoA reductase produces mevalonate and is the rate limiting enzyme for cholesterol biosynthesis in the liver, and it is competitively and reversibly inhibited by statins through their lactone ring and side chains that help them bind to the enzyme’s active site (Figure 1).32 Statins were initially identified as metabolites of fungi, have been on the market since 1987, and each vary in their lipophilicity, elimination half lives, and potency (figure 2).32-34 Inhibition of cholesterol synthesis leads to decreased cholesterol production and upregulation of the LDL receptor.4
Figure 1.
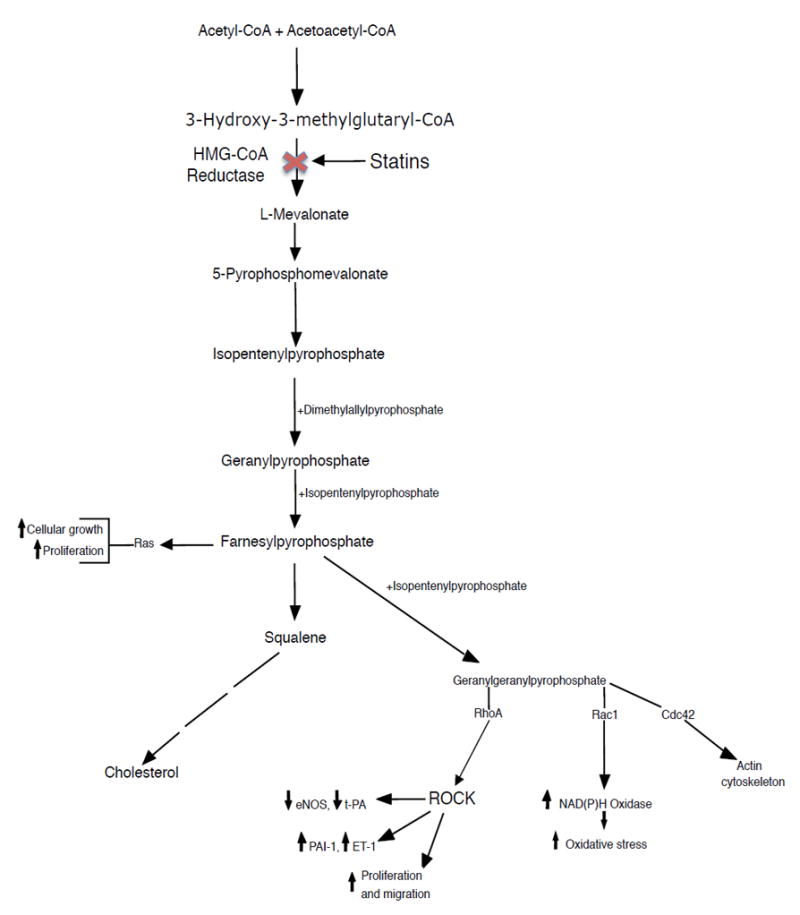
Cholesterol and isoprenoid synthesis pathway which shows the inhibition of 3-hydroxy-3-methyl-glutaryl-coenzyme A (HMG-CoA) reductase by statins. Decrease in isoprenylation of signaling molecules, such as Ras, Rho, and Rac, leads to the modulation of various signaling pathways. ROCK – rho associate protein kinase, NAD(P)H – nicotinamide adenine dinucleotide phosphate, eNOS – endothelial nitric oxide synthase, t-Pa – tissue-type plasminogen activator, ET-1 – endothelin 1, PAI-1 – plasminogen activator inhibitor 1.
Figure 2.
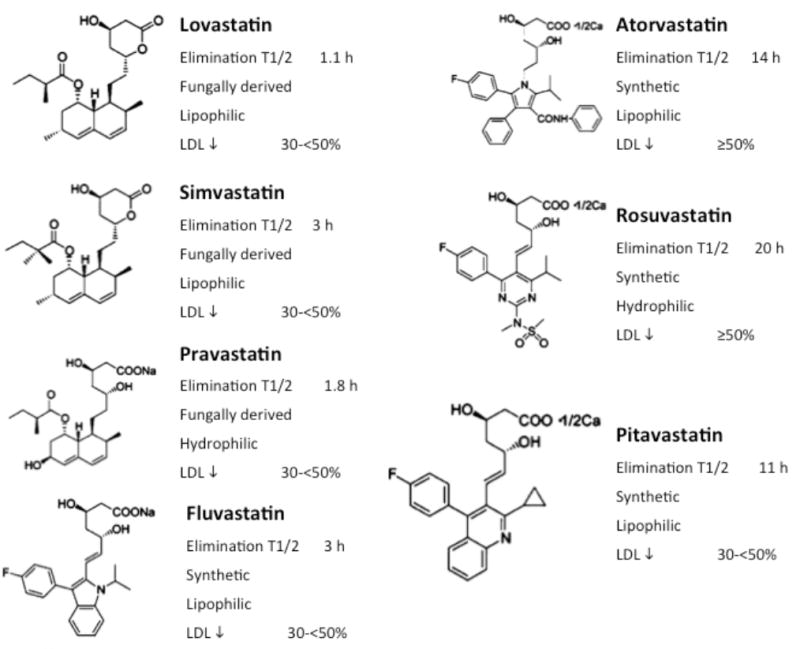
The structure and pharmacokinetic properties of the commercially available statins.32 LDL – low density lipoprotein, T1/2 – half life, h - hours
The lipophilic statins cross cell membranes largely by passive diffusion, while pravastatin and rosuvastatin require activated carrier-mediated transport with organic anion transporting polypeptide (OATP) 1B1 and are more selective for hepatic tissues.35-37 Similar transporters exist in other tissues, such as OATP 1A4 and OATP 2B1 although their efficacy in transporting hydrophilic statins is unknown.38-40 The concentrations of statins and mevalonate in different cell types are incompletely understood. It is unclear if the pleiotropic effects of statins are due to the hepatic or non-hepatic effects of isoprenoid inhibition.
It is unclear whether statins exert effects independent of mevalonate synthesis inhibition. One paper reported that statins could bind to an allosteric site within the β2 integrin leukocyte function-associated antigen-1 (LFA-1).41 LFA-1 is involved in leukocyte trafficking and T cell activation and binds intercellular adhesion molecule-1 (ICAM-1).42 ICAM-1 is crucial for the adhesion of monocytes to the endothelium and it is a biomarker for coronary events that is reduced by atorvastatin 43 However, to date, no consistent mevalonate-independent effects of any statin have been reported.
Evidence of Statin Pleiotropy in Clinical Trials
The concept of anti-inflammatory pleiotropic effects of statins has been tested for perioperative risk reduction. Several studies provide evidence for beneficial effects of statins on atrial fibrillation (AF) and outcomes after cardiac surgery 44-47 In contrast, in a study with 1922 patients in sinus rhythm who underwent elective cardiac surgery and received perioperative rosuvastatin 20 mg or placebo, statin therapy did not prevent postoperative AF or myocardial damage.48 Similarly, in a large trial among patients undergoing cardiac surgery, atorvastatin treatment did not reduce the risk of acute kidney injury.49 Cardiac surgery is pro-inflammatory and rosuvastatin reduced C-reactive protein (CRP) in one study, but subgroup analyses are not available from either study by CRP level. Although these clinical studies do not show benefits of statin therapy, they do not exclude whether statin pleiotropy exists, but rather that statins are not beneficial in these diseases.
Additional considerations regarding the pleiotropic effects of statins come from their effects on CRP. JUPITER was a primary prevention trial between rosuvastatin and placebo for 17,802 patients with a LDL-C of < 130 mg/dL and a CRP ≥ 2.0 mg/L.12 Rosuvastatin reduced LDL-C by 50%, CRP by 37%, and the primary endpoint by 44%.12 Plotting the expected benefit from JUPITER based on LDL-C lowering on the Cholesterol Treatment Trialists’ (CTT) Collaboration regression line, suggests that the realized benefit may be greater then the expected benefit based on LDL-C reduction alone (Figure 3). In contrast, the recent HOPE-3 study was a primary prevention trial with rosuvastatin 10 mg that did not have LDL-C or CRP as inclusion criteria and rosuvastatin reduced LDL-C by 26.5% and the co-primary outcomes by 24% and 25%.50 The benefit of rosuvastatin occurred in both high and normal CRP groups, and while rosuvastatin did lower CRP, the HOPE-3 study suggests that the benefit of statins may be primarily due to LDL-C lowering.50 In the A-Z trial, patients with acute coronary syndrome (ACS) received either simvastatin 40 mg for 1 month followed by titration to 80 mg versus placebo for 4 months and then simvastatin 20 mg. High dose simvastatin lowered LDL-C more effectively, but there was no difference in CRP levels at 30 days and the trial did not achieve its pre-specified endpoint 51 From month 4 onwards, there was a reduction of CRP in the high intensity simvastatin group, and the trend to benefit was stronger after 4 months then earlier.51 Both groups had relatively low CRP (2.5 mg/L versus 2.4 mg/L) at 1 month, which may explain the lack of effect.51 The MIRACL trial was a ACS trial comparing atorvastatin 80 mg with placebo and atorvastatin lowered the primary endpoint in patients with both high and normal LDL-C and lowered CRP by 83%.14,52 While these data on CRP suggest that statins reduce inflammation, there are no data showing the change in CRP correlates with efficacy and it is unclear whether the benefit seen with CRP reduction on medication is due to statin therapy or a lower baseline CRP, indicating a lower risk cohort..
Figure 3.
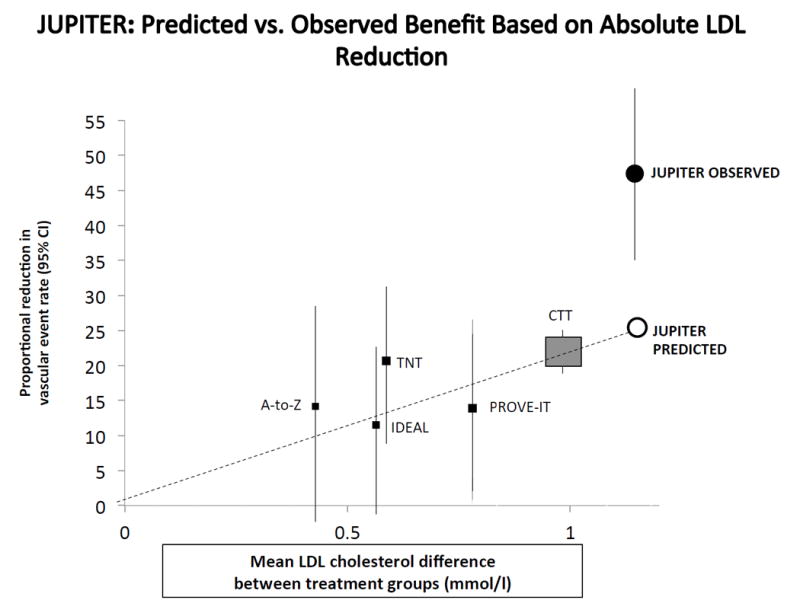
The predicted reduction in vascular event rate from the JUPITER trial based on its low density lipoprotein (LDL) cholesterol lowering. The gray square represents the average effect of statins versus placebo based on the Cholesterol Treatment Trialists’ collaboration regression line. The individual black squares represent individual trials, the open circle represents the predicted effect of atorvastatin in the Jupiter trial, the black circle represents the observed effect.12
It is difficult to separate the LDL-C lowering benefit of statins from their potential pleiotropic effects in clinical trials given the strong association between elevated cholesterol and CHD.53 Lowering ApoB containing lipoproteins, therefore, represents the most important mechanism of statins. Nevertheless, there is cumulative evidence for the existence of pleiotropic effects in humans but the contribution in addition to LDL-C lowering remains unknown for two reasons:54
Pleiotropic effects mediated by inhibition of isoprenoids correlate with the inhibition of cholesterol biosynthesis and are difficult to quantitate.
Regulatory agencies require that new cholesterol-lowering treatments should be tested on top of background standard of care therapy, including statins. This does not allow quantitating potential cholesterol-independent effects of statins because potential pleiotropic statin effects are present in both treatment arms.
Non-statin LDL-C lowering therapies could reduce the risk of CHD, thus confirming the cholesterol hypothesis. A recent meta-analysis suggests that non-statin therapies that increase the LDL receptor have the same benefits as statins and fall on the CTT regression line.55,56 Non-statin trials often take longer to show a benefit then statin trials. In the Lipid Research Clinic-Coronary Primary Prevention Trial (LRC-CPPT) with cholestyramine, the Program on the Surgical Control of Hyperlipidemias (POSCH) with partial ileal loop bypass surgery, and the IMPROVE-IT trial with ezetimibe in addition to simvastatin, benefits occurred after 7.4, 9.7, and 7.0 years, respectively whereas most of the statin trials showed benefits within 5 years (Table 2).56-58 Interpreting the time to benefit data is difficult because of the low event rates early in the trials prevent the separation of survival curves and both LRC-CPPT and POSCH were primary prevention trials with lower event rates but many of the statin trials are secondary prevention trials and the IMPROVE-IT trial was conducted until a pre-specified total event number was reached. Guidelines have generally recommended lifestyle changes and statins as first-line pharmacotherapy, with or without LDL-C targets. At present, non-statins are indicated only as adjunctive therapy for patients who are unable to reach their lipid goals despite optimal statin therapy.
Table 2.
Time to benefit for LDL-C lowering strategies
| Non-statins | Control | Trial | Time to benefit |
|---|---|---|---|
| Cholestyramine | placebo | LRC-CPPT57 | 7.4 years |
| partial ileal bypass surgery | no surgery | POSCH58 | 9.7 years |
| Ezetimibe with simvastatin 40 mg | placebo with simvastatin 40 mg | IMPROVE-IT56 | 7.0 years |
| Statins | |||
| Rosuvastatin | placebo | JUPITER12 | 1.9 years |
| Pravastatin | placebo | WOSCOPS8 | 5.0 years |
| placebo | CARE6 | 5.0 years | |
| placebo | LIPID17 | 6.1 years | |
| Atorvastatin | placebo | SPARCL184 | 4.9 years |
| placebo | ASCOT-LLA11 | 3.3 years | |
| Lovastatin | placebo | AFCAPS/Tex-CAPS9 | 5.2 years |
| Simvastatin | placebo | HPS10 | 2.0 years |
| placebo | 4S5 | 5.4 years | |
| Fluvastatin | placebo | LIPS16 | 3.9 years |
Studies using “clamped” cholesterol designs, e.g. comparing the effect of statin-mediated LDL-C lowering with equal LDL-C lowering mediated by another intervention (e.g. diet) have reported pleiotropic effects of statins in animals including cynomolgus monkeys.59 Non-statins such as the inhibitor of Niemann-Pick C1 like protein, ezetimibe, have been used in humans for this purpose. Ezetimibe lowers LDL-C by 15-20% and can only be compared with less potent statins, which makes vascular effects more difficult to observe. Ezetimibe reduces cholesterol absorption in the small intestine and animal data suggests an increase in the LDL-C receptor, but human data is inconsistent.60,61 Nevertheless, multiple small studies have attempted to determine if statins have pleiotropic effects compared to ezetimibe. These studies are characterized by surrogate endpoints. For example, a randomized study of heart failure patients with simvastatin 10 mg or ezetimibe 10 mg found a 15% reduction in LDL-C for both groups, but only simvastatin improved radial artery flow-dependent vasodilation, increased functionally-active endothelial progenitor cells (EPCs), and increased superoxide dismutase.62 Several studies randomized healthy volunteers or patients with CHD to protocols comparing high dose statins to a combination of lower dose statins and ezetimibe and reported greater improvement in endothelial function and vascular inflammation with high dose statins, despite comparable lowering of LDL-C in both groups.63-66 Other studies did not find differences between groups, suggesting the absence of statin pleiotropy.67-69 Additional evidence for pleiotropy stems from studies that report effects of statins that were observed before serum LDL-C was lowered. 70 All of these studies were relatively small, were performed in heterogeneous patient populations with different outcome measures and duration of therapy, and showed conflicting results. These studies provide interesting data but do not provide definitive clinical evidence of statin pleiotropy.
The notion of whether statin pleiotropy has clinical relevance in terms of cardiovascular risk reduction may benefit from ongoing trials with the proprotein convertase subtilisin kexin 9 inhibitors (PCSK9i) that lower LDL-C levels by about 60% alone and could be compared with a high dose statin in terms of equivalency in LDL-C reduction.71,72 High dose statin therapy has demonstrated impressive benefits on plaque reduction that has been postulated to be due to their anti-inflammatory effects in addition to their intensive LDL-C lowering effects.73,74 The GLAGOV (NCT01813422) results have been recently announced and will be published later this year and demonstrate that the PCSK9i reduce plaque size on top of optimal statin therapy demonstrating that plaque regression may not be due primarily to pleiotropic effects of statins. The large FOURIER (NCT01764633), ODYSEEY Outcomes (NCT01663402) and SIPRE1,2 (NCT01975376, NCT01975389) are event driven trials that test the effects of PCSK9i on cardiovascular outcomes and are expected to result in the next few years. It would be interesting to see if the outcomes benefits with PCSK9i are equivalent to outcome trials with high dose statins when comparable LDL-C lowering is considered.
PCSK9i lower LDL-C by a mechanism similar to statins because they increase the LDL receptor-mediated hepatic uptake of ApoB-containing lipoproteins. However, they do not inhibit the mevalonate pathway, and would not have similar pleiotropic effects stemming from Rho GTPase inhibition. Despite their potent LDL-C lowering effects, PCSK9i do not reduce serum markers of inflammation such as CRP, interleukins (IL) or tumor necrosis factor alpha (TNFα).75 These observations do not exclude anti-inflammatory effects on circulating monocytes or on vascular cells. Together with CANTOS (NCT01327846), a study testing the inhibition of the pro-inflammatory cytokine IL-1β and CIRT (NCT01594333) examining methotrexate, the PCSK9i outcome trials will provide important information on the relevance of the reduction of systemic inflammatory markers for clinical outcomes.
DIVERSE TARGET POINTS FOR STATIN ACTIONS
Statins and Isoprenylated Proteins
By inhibiting mevalonic acid synthesis, statins prevent the synthesis of isoprenoid intermediates farnesylpyrophosphate (FPP) and geranylgeranylpyrophosphate (GGPP).76 FPP and GGPP serve as lipid attachments for the post-translational modification of heterotrimeric G-proteins, including Ras and Rho.77 Ras and Rho regulate cell proliferation, differentiation, apoptosis, and the cytoskeleton.78 In endothelial cells (ECs), Ras translocation is dependent on farnesylation, whereas Rho translocation is dependent on geranylgeranylation.79,80 While the inhibition of isoprenoid intermediate synthesis is central to the possible pleiotropic effects of statins, it is unclear if the primary LDL-C lowering benefit of statins is due to reduced cholesterol production and reduced mevalonic acid production or upregulation of the LDL receptor.81 There is a relative paucity of human studies regarding the levels of FPP and GGPP with chronic statin therapy.
Statins and Rho/Rho Kinase
Rho kinases (ROCKs) are protein serine/threonine kinases of 160 kDa that contribute to the downstream effects of Rho GTPases.82 ROCK shifts to an active open conformation when RhoA binds to ROCK (Figure 4).82 ROCKs regulate actin cytoskeletal changes through effects on myosin light chain phosphorylation. This affects focal adhesion complex formation, smooth muscle contraction, cell migration, and gene expression.83
Figure 4.
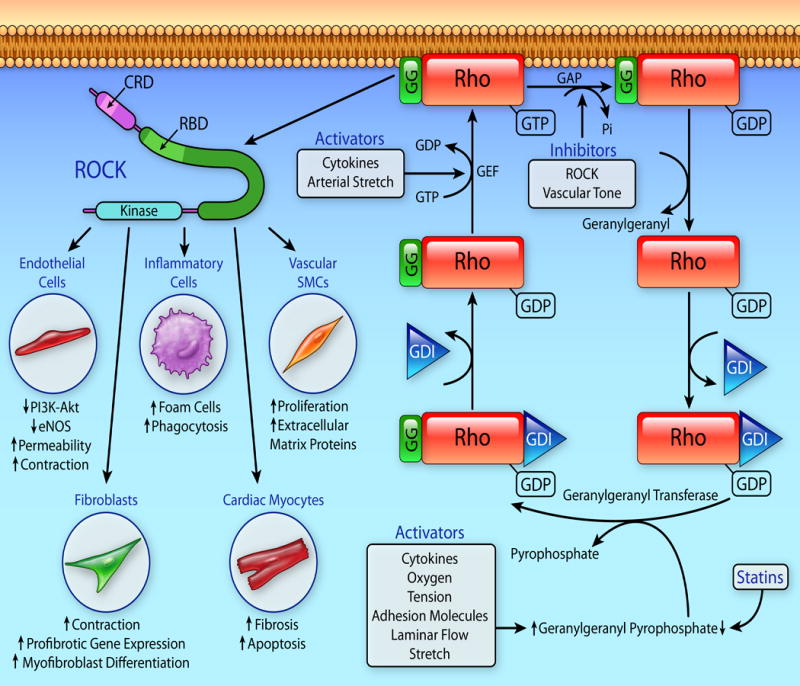
Regulation of the Rho GTPase cycle. Rho cycles between an inactive, cytoplasmic, guanosine diphosphate (GDP) bound form and after geranylgeranylation is translocated to the plasma membrane and activated when it is bound to guanosine triphosphate (GTP). Inhibition of mevalonate synthesis by statins decreases geranylgeranyl pyrophosphate and prevents the geranylgeranylation of Rho and therefore its activation of Rho kinase (ROCK). ROCK mediates the downstream effects of Rho and has effect on endothelial cells, inflammatory cells, fibroblasts, cardiomyocytes, and vascular smooth muscle cells (SMC) that promote atherosclerosis and cardiac remodeling and may be responsible for the pleiotropic effects of statins. GG – geranylgeranyl, GDI – guanine nucleotide dissociation inhibitors, GEF – guanine nucleotide exchange factors, GAP – GTPase – activating proteins, PI3K - phosphatidylinositol 3-kinase, eNOS – endothelial nitric oxide synthase, CRD – Cysteine rich domain, RBD – Rho-binding domain
In human aortic ECs, simvastatin prevented tissue factor induction by thrombin in a Rho/ROCK-dependent manner.84 In animal models, inhibition of ROCK has cardiovascular effects similar to statins, the ROCK inhibitors (fasudil and Y27632), limit cardiac fibrosis, hypertrophy, and pathologic remodeling in response to angiotensin II (Ang II) and NG-nitro-L-arginine methyl ester, transverse aortic constriction (TAC), and myocardial infarction (MI).85-88 Increased leukocyte ROCK activity is observed in patients with hypertension, pulmonary hypertension, metabolic syndrome, dyslipidemia, coronary artery disease (CAD), coronary vasospasm, left ventricular hypertrophy (LVH), and in heart failure with decreased systolic function.63,89-99 Statins reduce ROCK activity (Table 3).100-107 Statins have demonstrated inhibition of leukocyte ROCK activity in humans independent of LDL reduction.108 ROCK inhibition is a candidate for mediating statin pleiotropy because of ROCK’s effects on the cardiovascular system, ROCK activity is a biomarker of cardiovascular disease, and ROCK inhibition by statins occurs through cholesterol-independent mechanisms.
Table 3.
Studies Showing Statin Inhibition of Rho Kinase
| Author | Year | Sample | Effect |
|---|---|---|---|
| In vitro and animal studies | |||
| Eto et al84 | 2002 | Human endothelial cells | ↓ tissue factor induction |
| McNeish et al106 | 2013 | Rat middle cerebral arteries | ↓ thromboxane receptor stimulation |
| Massaro et al187 | 2010 | Human endothelial cells | ↓ COX2 and MMP-9 expression |
| Li et al144 | 2007 | Bovine pulmonary artery SMCs | ↓ SMC mitogensis and migration |
| Ma et al107 | 2012 | Rats with hypertension | ↓ ROCK activity |
| Ohnaka et al100 | 2001 | Human osteoblasts | ↓ ROCK activity and BMP-2 expression |
| Tramontano et al101 | 2004 | Human endothelial cells | ↓ endothelial micorparticle levels |
| Gojo et al102 | 2007 | Rats with diabetes | ↓ urinary albumin and 8- hydroxydeoxyguanosine excretion |
| Yamanouchi et al103 | 2005 | Rabbits with normal cholesterol and human endothelial cells | ↓ ROCK activity and carotid intimal hyperplasia |
| Kozai et al104 | 2005 | Human saphenous vein SMCs | ↓ ROCK activity and carotid intimal hyperplasia |
| Trebicka et al105 | 2007 | Rats with cirrhosis | ↓ ROCK activity and ↑ eNOS |
| Human studies | |||
| Rawlings et al108 | 2009 | Humans with stable CAD | ↓ ROCK activity |
| Liu et al63 | 2009 | Humans with hyperlipidemia | ↓ ROCK activity |
| Nohria et al94 | 2009 | Humans with stable CAD | ↓ ROCK activity |
COX2 – cyclooxygenase 2;MMP - matrix metalloproteinase; SMC – smooth muscle cell; ROCK – rho kinase; BMP-2 – bone morphogenetic protein 2; eNOS – endothelial nitric oxide synthase; CAD – coronary artery disease
Statins and Rac
Rac is a 20-39 kDa monomeric G-protein and a member of the Rho GTPase subfamily.109 Rac1 modulates phosphorylation of intercellular proteins occludin, vascular endothelial cadherin, and β-catenin, which are critical for tight junction and adherence junction integrity.110 Rac1 activates nicotinamide adenine dinucleotide phosphate (NADPH) oxidase and produces reactive oxygen species (ROS) leading to LVH.111 ROS could also modify LDL to oxidized LDL which is atherogenic and mediates foam cell formation.112 Elevated Rac1 and NADPH oxidase activity is seen in rats undergoing TAC, vascular smooth cells (SMC) stimulated by Ang II, in saphenous vein grafts and internal mammary artery after coronary artery bypass, in ischemic and non-ischemic cardiomyopathy (NICM), and AF and is attenuated by statins.54,113-118 The inhibition of Rac1 links statins to reduced ROS and NADPH oxidase activity, and may explain some of the pleiotropic actions of statins.
Statins and the Peroxisome Proliferator-Activated Receptor (PPAR)
Statins have been shown to activate PPARs.119 Statins acutely decrease lipopolysaccharide (LPS) related inflammation in wild type mice but not in PPARα-null mice, independent of cholesterol lowering mechanisms.120 Statins increase PPAR-γ activity and inhibit LPS induced TNFα and monocyte chemotactic protein 1 (MCP-1) activity.119,121 The administration of simvastatin in combination with PPAR-γ agonists elicits additive beneficial vascular effects.122 Atorvastatin reduces advanced glycation end products in rats and attenuates fibroblast proliferation and cardiac fibrosis, which was reversed with the PPAR-γ antagonist GW9662.123 Statins reduced ROS production by augmenting the messenger ribonucleic acid (mRNA) expression of the PPAR-γ co-activator, which is an important regulator of mitochondrial biogenesis.124 However, statins, especially the high intensity statins, increase the risk of diabetes.125 Thus, the ability of the PPAR-γ agonists, thiazolidinediones, to lower blood sugar is in contrast to the effects of statins on PPAR-γ and demonstrates the complex nature of statin interactions with other pathways, including glucose metabolism.
CELLULAR EFFECTS OF STATINS
Statins and the Endothelium
Endothelial dysfunction is caused by hypercholesterolemia and is characterized by impaired bioavailability of endothelial-derived nitric oxide (NO). Endothelial NO is important for vasodilation, platelet aggregation, vascular smooth muscle proliferation, and endothelial-leukocyte interactions.126 Statins increase endothelial NO production, in part, by upregulating endothelial NO synthase (eNOS), which may be a pleiotropic effect of statins (Table 4).79,80 While the increase in eNOS is important, it should be noted that much of the animal studies examining eNOS and other cellular targets used significantly higher doses of statins than are used in clinical practice.
Table 4.
The Pleiotropic Effects of Statins by Cell Type
| Endothelial cells | ↑ eNOS expression and activity79,80 |
| ↓ Plasminogen activator inhibitor-1 expression, and ↑ Tissue-type plasminogen activator expression 188 | |
| ↓ Endothelin-1 synthesis and expression182 | |
| ↓ ROS113 | |
| ↑ Peroxisome proliferator-activated receptor-α and γ expression119-121 | |
| ↓ Proinflammatory cytokines (IL-1β, IL- 6, cyclooxygenase-2) expression157,187 | |
| ↓ CD40 expression189 | |
| Vascular Smooth Muscle Cells | ↓ Migration and proliferation142,144 |
| ↓ ROS113,115,116 | |
| ↓ NADPH oxidase activity111,115,116 | |
| ↓ AT1 receptor expression113 | |
| ↓ Platelet derived growth fator141 | |
| Myocardium | ↓ NADPH oxidase activity114,151 |
| ↓ ROS124 | |
| ↓ Left ventricular fibrosis and hypertrophy114,149 | |
| ↑ Nitric oxide155,156 | |
| ↓ Apoptosis152 | |
| Platelets | ↓ Platelet reactivity163,166 |
| ↓ Thromboxane A2 biosynthesis167 | |
| Monocyte/Macrophages | ↓ Macrophage growth171 |
| ↓ MMP expression and secretion143,172 | |
| ↓ Tissue factor expression and activity84 | |
| ↓ Proinflammatory cytokines (IL-1β, IL- 6, IL-8, TNFα) expression120,170 | |
| ↓ Monocyte chemoattractant protein-1 secretion170,171,189 | |
| Vascular Inflammation | ↓ CRP level12,52 |
| ↓ Leukocyte-endothelial cell adhesion41,42,168,176,177 | |
| ↓ T cell activation134,168,173,174 | |
| ↓ Nuclear factor-κB activation143,169 | |
| Endothelial Progenitor Cells | ↑ Mobilization of stem cells136 |
IL indicates interluekin; CD – cluster of differentiation; AT1 – angiotensin type 1; TNF – tumor necrosis factor; NADPH – nicotamide adenine dinucleotide phosphate; ROS – reactive oxygen species; MMP - matrix metalloproteinase; eNOS – endothelial nitric oxide synthase
Statins upregulate eNOS through multiple mechanisms. One pathway involves Rho/ROCK signaling. In vitro studies show that Rho inhibition increases eNOS expression.80 Increased ROCK activity downregulates eNOS, and ROCK inhibitors (Y-27632 and fasudil) increase eNOS expression.127,128 The effects of statins on eNOS expression are not reversed by FPP or LDL-C, indicating that the effect is likely mediated through the geranylgeranylation of RhoA and ROCK signaling 80
Statins also increase eNOS activity by post-translational activation of the phosphatidylinositol 3-kinase/protein kinase Akt (PI3k/Akt) pathway as eNOS is phosphorylated by Akt.129 Inhibition of the Rho/ROCK pathway activates the PI3k/Akt pathway and cardioprotection.130,131 ROCK is a negative regulator of the Akt pathway, possibly through activation of phosphatase and tensin homologue.131
Statins also act on caveolin 1 which is an integral membrane protein that binds to eNOS in caveolae, and directly inhibits NO production. 132 Statins decrease caveolin-1 expression in vitro and in mice, thereby promoting eNOS activity.132
Statins could also exert pleiotropic effects through the transcription factor kruppel-like factor -2 (KLF2). Statins induce KLF2 mRNA in ECs, which may be required for eNOS expression.133 Statins reduce T proliferation through KLF2, which may explain some of their immunomodulatory effects.134
Statins may exert pleiotropic effects by enhancing the mobilization of EPCs. Impaired EPCs are associated with impaired endothelial function and decreased NO levels.135 Atorvastatin increases EPCs in patients with CAD within one week. 136 This effect is apparently observed only at low statin concentrations, higher concentrations of statins tend to have angiostatic effects, which may explain why high-intensity statins are able to reduce intraplaque angiogenesis in patients with atherosclerosis.137,138
Statins and Vascular Smooth Muscle
The proliferation of vascular SMCs is important in vascular lesion pathogenesis.139 Transplant arteriosclerosis is an immune response directed against donor ECs and vascular SMCs independent of hypercholesteremia that is still attenuated by statins.140 Inhibition of isoprenoid synthesis by statins decreased platelet derived growth factor (PDGF)-induced deoxyribonucleic acid (DNA) synthesis in vascular SMCs by increasing the cyclin-dependent kinase, p27Kip1, which was possibly mediated by Rho GTPase.141 Simvastatin decreases intimal thickening, reduces cellular proliferation, leukocyte accumulation, and PDGF receptor phosophorylation in LDL receptor deficient mice.142 In vitro, atorvastatin reduces the effects of the pro-inflammatory cytokine IL-18, which inhibits SMC migration, nuclear factor-κB (NF-κB) activation, and matrix metalloproteinase (MMP)-9 expression.143 In bovine pulmonary artery SMCs, atorvastatin inhibits migration of pulmonary artery SMC, which was reversed by GGPP and mevalonate, again implicating the potential for the Rho/ROCK pathway in SMC proliferation.144
Statins and the Myocardium
The GTP-binding proteins, Ras, Rho, and Rac play a critical role in cardiac hypertrophy.145 Mice without Rac1 showed decreased NADPH oxidase activity and myocardial oxidative stress, confirming that Rac1 is essential for myocardial hypertrophy.146 Rac1 also increases the activity of the mineralocorticoid receptor.147 In vitro, statins increase small guanosine triphosphate binding protein guanosine diphosphate dissociation stimulator (SmgGDS) and decrease Rac1 in a lipid-independent fashion.148 Statins decrease Rac1 levels, cardiomyocyte hypertrophy, and fibrosis in wild type mice, but not in mice that lack SmgGDS.149 Rac1 contributes to doxorubicin-related cardiotoxicity through both a ROS-dependent and independent mechanism.150 Finally, preoperative atorvastatin induced Rac1-mediated inhibition of NADPH in human atrial myocardium.151
The effect of statins on the myocardium is also mediated through RhoA and ROCK, because both lead to increased apoptosis and increased fibrosis, which could lead to the development of LVH and heart failure. Overexpression of RhoA in rat ventricular myocytes induces increased caspase-9 activation, DNA fragmentation, and apoptosis, which are blocked by ROCK inhibitors.152 Mice with a genetic deletion of ROCK1 had less ischemic reperfusion-related fibrosis compared to wild type mice.153 Mice without ROCK2 demonstrated less LVH, fibrosis, and apoptosis when exposed to Ang II or TAC compared to wild type mice.154 In humans, leukocyte ROCK levels are 4.5 times higher in patients with LVH and hypertension compared to those with hypertension without LVH and ROCK activity also is increased with LVH in chronic kidney disease.95,96 Statins increase NO bioavailability, which increases myocardial blood flow under hypoxic conditions and inhibits IL-6, IL-8, and vascular cell adhesion molecule-1 (VCAM-1).155-157 In vitro studies show that statins reduce mitochondrial dysfunction and cardiomyocyte death.158
There is, however, conflicting data about whether statins improve outcomes in NICM. A cohort study demonstrated decreased mortality and a small randomized controlled trial showed improvement in ejection fraction, symptoms, and lower levels of pro-inflammatory cytokines.159,160 However, both the large randomized GISSI-HF and CORONA trials did not show any benefit for either death or the composite endpoint.161,162 While there are questions about the efficacy of statins for heart failure, it is possible that statin therapy is beneficial if started earlier in the disease course.
Statins and Platelets
Platelets are essential in the pathogenesis of ACS. Hypercholesteremia is associated with increased platelet reactivity and thrombin generation, which is decreased with pravastatin and is likely both cholesterol associated and LDL-C independent.163 Mice treated with atorvastatin showed increased eNOS and down regulated platelet factor 4 and beta thromboglobulin in platelets, effects which are absent in eNOS knockout mice.164 Fluvastatin acts through PPARα and PPAR-γ to reduce platelet aggregation in response to arachidonic acid and decreased platelet aggregation compared to colestimide.165,166 Atorvastatin acutely inhibited platelet recruitment, decreased Nox2, Rac1, protein kinase C, platelet phospholipase A2 and thromboxane A2 while increasing NO levels.167 Finally, the anti-thrombotic effect was also shown in the JUPITER trial because treatment with rosuvastatin was associated with decreased thromboembolism, an effect that is likely to be unrelated to cholesterol reduction since hypercholesterolemia is not a particularly strong risk factor for venous thromboembolism. 31
DIRECT NON-LDL EFFECTS ON STATINS IN CARDIOVASCULAR DISEASE
Statins and Atherosclerosis
Atherosclerosis is a chronic inflammatory process of the vascular wall that is initiated by excessive LDL-C and is mediated by activated macrophages, T lymphocytes, B lymphocytes, and SMCs.2 Statins are anti-inflammatory and reduce inflammatory cytokines and adhesion molecules, and acting on both the innate and adaptive immune responses.168 Statins reduce Rac1-mediated ROS species production and reduce the oxidation sensitive inflammatory pathways.169 Statins decrease inflammatory cytokines such as IL-6, IL-8, and MCP-1.170 In vitro statins inhibited IL-6 induced monocyte chemotaxis and MCP-1 expression and inhibited Janus kinase and the signal transducers and activators of transmission pathway, an effect that was reversed by GGPP.171 Statins reduce MMP-1, MMP-3 and MMP-9 from both SMCs and macrophages in a rabbit model, which was reduced by both GGPP and mevalonate.172
In the adaptive immune system, statins have effects on T-cell differentiation. Simvastatin reduced the differentiation of the proinflammatory IL-17 helper T cells (Th17) and enhanced the production of forkhead box P3 (Foxp3)+ Cd4+ regulatory T cells (Tregs) in a geranylgeranylation dependent manner. 173 Transforming growth factor beta (TGF-β) induces Foxp3+ Cd4+ Tregs and simvastatin acts through geranylgeranylation to inhibit the TGF-β inhibitors Smad6 and Smad7 and therefore increase TGF-β and Foxp3+ Cd4+ Treg expression.174 Cd4+ T lymphocytes from patients with ACS induced EC apoptosis through an upregulated TNF-related apoptosis inducing ligand (TRAIL) receptor DR5 on ECs and increased TRAIL expression on T lymphocytes, an effect that was blocked by statins and may provide a pathway for improved plaque stability by statins.175
Statins decrease the leukocyte and EC interaction that occurs in atherogenesis. ICAM-1 and VCAM-1 regulate the migration of leukocytes to ECs and platelet and endothelial cell adhesion molecute-1 (PECAM-1) is involved in leukocytes crossing ECs.176,177 Statins inhibit VCAM-1 through PPARα and increased NO production.157,178 RhoA inhibition inhibits the clustering of VCAM-1 and ICAM-1 and decreases monocyte adhesion to ECs.179 Lovastatin regulates PECAM-1 expression, which was reversed by GGPP and mevalonate, suggesting a role of Rho in regulating leukocyte migration.180
Statins and Stroke
While elevated cholesterol and LDL-C are risk factors for ischemic strokes in many epidemiological studies, it has not been established in every study and the link remains more controversial then the link for CAD.181 Nonetheless statins reduce the risk of stroke by 25% in both the Heart Protection Study and the Treating to New Targets study and 48% in the JUPITER trial. 10,182,183 The SPARCL trial demonstrated that atorvastatin is effective for stroke secondary prevention.184 While there has been debate if non-statin cholesterol medications effect stroke incidence the IMPROVE-IT trial showed the ezetimibe in addition to simvastatin had a 21% reduction in ischemic stroke.56
A potential pleiotropic target for statins in stroke is the effect of statins on eNOS, given that mice without eNOS demonstrate larger infarcts.155 The effects of statins are likely mediated by Rho/ROCK because ROCK inhibitors upregulate eNOS and improve cerebral blood flow in mice.128
Conclusion
Given the cell culture and the animal studies as well as indirect evidence from clinical trials, it remains important to assess whether the non-LDL-C lowering effects of statins could be replicated by other cholesterol lowering therapies or by agents that act downstream of isoprenoid synthesis, e.g., squalene synthase inhibitors. Unfortunately, all of the current novel hyperlipidemia treatments are tested in patients receiving statins, which will only provide information regarding how much further to lower serum LDL-C, but does not exclude or include the potential pleiotropic effects of statins. The concept of statin pleiotropy has provided a window of opportunity to test and target other non-lipid-lowering signaling pathways that may affect cardiovascular disease. Agents that target inflammation alone, such as anti-IL-1β therapy (canakinumab) and methotrexate, are currently being tested in secondary prevention trials as adjunctive therapy to lipid lowering.185,186 Furthermore, the ROCK inhibitors, fasudil and ripasudil, which are currently approved in Japan for the treatment of cerebral vasospasm after subarachnoid hemorrhage and to treat glaucoma, respectively, may be of interest as novel therapies for reducing cardiovascular diseases. Finally, the PCSK9i may help provide evidence for statin pleiotropy, especially when low-dose PCSK9i is compared with high-potency statins that are matched for equivalent LDL-C lowering. This design would provide the opportunity to definitively test the clinical relevance of statin pleiotropy on cardiovascular outcomes.
Acknowledgments
Grant Support: NIH HL052233
Non-standard abbreviations and Acronyms
- ApoB
Apolipoprotein B
- LDL-C
low-density lipoprotein cholesterol
- HMG-CoA
hydroxy-methylglutaryl coenzyme A
- CHD
coronary heart disease
- OATP
organic anion transporting polypeptide
- LFA-1
leukocyte function-associated antigen-1
- ICAM-1
intercellular adhesion molecule-1
- AF
atrial fibrillation
- CRP
C-reactive protein
- ACS
acute coronary syndrome
- CTT
Cholesterol Treatment Trialists
- EPCs
endothelial progenitor cells
- PCSK9i
proprotein convertase subtilisin kexin 9 inhibitors
- IL
interleukins
- TNFα
tumor necrosis factor alpha
- EC
endothelial cells
- FPP
farnesylpyrophosphate
- ROCK
Rho kinase
- Ang II
angiotensin II
- TAC
transverse aortic constriction
- MI
myocardial infarction
- CAD
coronary artery disease
- LVH
left ventricular hypertrophy
- NADPH
nicotinamide adenine dinucleotide phosphate
- ROS
reactive oxygen species
- SMC
smooth muscle cells
- NICM
non-ischemic cardiomyopathies
- PPAR
peroxisome proliferator-activated receptor
- LPSM
lipopolysaccharide
- MCP-1
monocyte chemotactic protein-1
- mRNA
messenger ribonucleic acid
- NO
nitric oxide
- eNOS
endothelial nitric oxide synthase
- PI3K
phosphatidylinositol 3-kinase
- KLF2
kruppel-like factor -2
- PDGF
platelet derived growth factor
- DNA
deoxyribonucleic acid
- NFκB
nuclear factor κB
- MMP
matrix metalloproteinase
- SmgGDS
small GTP binding protein GDP dissociation stimulator
- VCAM-1
vascular cell adhesion molecule-1
- Tregs
regulatory T cells
- CD
cluster of differentiation
- Foxp3M
forkhead box P3
- Th17
IL-17 helper T cells
- TGF-β
Transforming growth factor beta
- TRAIL
TNF related apoptosis inducing ligand
- PECAM – 1
platelet and endothelial cell adhesion molecule-1
Footnotes
Conflict of Interest:
There are no conflicts of interests for all of the authors
References
- 1.Mendis S, Davis S, Norrving B. Organizational update: the world health organization global status report on noncommunicable diseases 2014; one more landmark step in the combat against stroke and vascular disease. Stroke. 2015;46:e121–122. doi: 10.1161/STROKEAHA.115.008097. [DOI] [PubMed] [Google Scholar]
- 2.Libby P, Tabas I, Fredman G, Fisher EA. Inflammation and its resolution as determinants of acute coronary syndromes. Circ Res. 2014;114:1867–1879. doi: 10.1161/CIRCRESAHA.114.302699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ference BA, Majeed F, Penumetcha R, Flack JM, Brook RD. Effect of naturally random allocation to lower low-density lipoprotein cholesterol on the risk of coronary heart disease mediated by polymorphisms in NPC1L1, HMGCR, or both: a 2 × 2 factorial Mendelian randomization study. J Am Coll Cardiol. 2015;65:1552–1561. doi: 10.1016/j.jacc.2015.02.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Istvan ES, Deisenhofer J. Structural mechanism for statin inhibition of HMG-CoA reductase. Science. 2001;292:1160–1164. doi: 10.1126/science.1059344. [DOI] [PubMed] [Google Scholar]
- 5.Scandinavian Simvastatin Survival Study G. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S) Lancet. 1994;344:1383–1389. [PubMed] [Google Scholar]
- 6.Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG, Brown L, Warnica JW, Arnold JMO, Wun C-C, Davis BR, Braunwald E. The Effect of Pravastatin on Coronary Events after Myocardial Infarction in Patients with Average Cholesterol Levels. N Engl J Med. 1996;335:1001–1009. doi: 10.1056/NEJM199610033351401. [DOI] [PubMed] [Google Scholar]
- 7.Group TL-TIwPiIDS. Prevention of Cardiovascular Events and Death with Pravastatin in Patients with Coronary Heart Disease and a Broad Range of Initial Cholesterol Levels. N Engl J Med. 1998;339:1349–1357. doi: 10.1056/NEJM199811053391902. [DOI] [PubMed] [Google Scholar]
- 8.Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, Macfarlane PW, McKillop JH, Packard CJ. Prevention of Coronary Heart Disease with Pravastatin in Men with Hypercholesterolemia. N Engl J Med. 1995;333:1301–1308. doi: 10.1056/NEJM199511163332001. [DOI] [PubMed] [Google Scholar]
- 9.Downs JR, Clearfield M, Weis S, et al. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: Results of afcaps/texcaps. JAMA. 1998;279:1615–1622. doi: 10.1001/jama.279.20.1615. [DOI] [PubMed] [Google Scholar]
- 10.MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebocontrolled trial. Lancet. 2002;360:7–22. doi: 10.1016/S0140-6736(02)09327-3. [DOI] [PubMed] [Google Scholar]
- 11.Sever PS, Dahlof B, Poulter NR, Wedel H, Beevers G, Caulfield M, Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, Mehlsen J, Nieminen M, O’Brien E, Ostergren J. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial--Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet. 2003;361:1149–1158. doi: 10.1016/S0140-6736(03)12948-0. [DOI] [PubMed] [Google Scholar]
- 12.Ridker PM, Danielson E, Fonseca FAH, Genest J, Gotto AMJ, Kastelein JJP, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ. Rosuvastatin to Prevent Vascular Events in Men and Women with Elevated C-Reactive Protein. N Engl J Med. 2008;359:2195–2207. doi: 10.1056/NEJMoa0807646. [DOI] [PubMed] [Google Scholar]
- 13.Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, Joyal SV, Hill KA, Pfeffer MA, Skene AM. Intensive versus Moderate Lipid Lowering with Statins after Acute Coronary Syndromes. N Engl J Med. 2004;350:1495–1504. doi: 10.1056/NEJMoa040583. [DOI] [PubMed] [Google Scholar]
- 14.Schwartz GG, Olsson AG, Ezekowitz MD, Ganz P, Oliver MF, Waters D, Zeiher A, Chaitman BR, Leslie S, Stern T. Effects of atorvastatin on early recurrent ischemic events in acute coronary syndromes: the MIRACL study: a randomized controlled trial. JAMA. 2001;285:1711–1718. doi: 10.1001/jama.285.13.1711. [DOI] [PubMed] [Google Scholar]
- 15.Hiro T, Kimura T, Morimoto T, Miyauchi K, Nakagawa Y, Yamagishi M, Ozaki Y, Kimura K, Saito S, Yamaguchi T, Daida H, Matsuzaki M. Effect of intensive statin therapy on regression of coronary atherosclerosis in patients with acute coronary syndrome: a multicenter randomized trial evaluated by volumetric intravascular ultrasound using pitavastatin versus atorvastatin (JAPAN-ACS study) J Am Coll Cardiol. 2009;54:293–302. doi: 10.1016/j.jacc.2009.04.033. [DOI] [PubMed] [Google Scholar]
- 16.Serruys PW, de Feyter P, Macaya C, Kokott N, Puel J, Vrolix M, Branzi A, Bertolami MC, Jackson G, Strauss B, Meier B. Fluvastatin for prevention of cardiac events following successful first percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;287:3215–3222. doi: 10.1001/jama.287.24.3215. [DOI] [PubMed] [Google Scholar]
- 17.Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med. 1998;339:1349–1357. doi: 10.1056/NEJM199811053391902. [DOI] [PubMed] [Google Scholar]
- 18.Liao JK, Laufs U. Pleiotropic effects of statins. Annu Rev Pharmacol Toxicol. 2005;45:89–118. doi: 10.1146/annurev.pharmtox.45.120403.095748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tonelli M, Moye L, Sacks FM, Cole T, Curhan GC. Effect of pravastatin on loss of renal function in people with moderate chronic renal insufficiency and cardiovascular disease. J Am Soc Nephrol. 2003;14:1605–1613. doi: 10.1097/01.asn.0000068461.45784.2f. [DOI] [PubMed] [Google Scholar]
- 20.Vidt DG, Cressman MD, Harris S, Pears JS, Hutchinson HG. Rosuvastatin-induced arrest in progression of renal disease. Cardiology. 2004;102:52–60. doi: 10.1159/000077704. [DOI] [PubMed] [Google Scholar]
- 21.Chopra V, Rogers MA, Buist M, Govindan S, Lindenauer PK, Saint S, Flanders SA. Is statin use associated with reduced mortality after pneumonia? A systematic review and meta-analysis. Am J Med. 2012;125:1111–1123. doi: 10.1016/j.amjmed.2012.04.011. [DOI] [PubMed] [Google Scholar]
- 22.Novack V, MacFadyen J, Malhotra A, Almog Y, Glynn RJ, Ridker PM. The effect of rosuvastatin on incident pneumonia: results from the JUPITER trial. CMAJ. 2012;184:E367–372. doi: 10.1503/cmaj.111017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chataway J, Schuerer N, Alsanousi A, et al. Effect of high-dose simvastatin on brain atrophy and disability in secondary progressive multiple sclerosis (MS-STAT): a randomised, placebo-controlled, phase 2 trial. Lancet. 2014;383:2213–2221. doi: 10.1016/S0140-6736(13)62242-4. [DOI] [PubMed] [Google Scholar]
- 24.Bauer DC, Mundy GR, Jamal SA, Black DM, Cauley JA, Ensrud KE, van der Klift M, Pols HA. Use of statins and fracture: results of 4 prospective studies and cumulative meta-analysis of observational studies and controlled trials. Arch Intern Med. 2004;164:146–152. doi: 10.1001/archinte.164.2.146. [DOI] [PubMed] [Google Scholar]
- 25.Erichsen R, Froslev T, Lash TL, Pedersen L, Sorensen HT. Long-term statin use and the risk of gallstone disease: A population-based case-control study. Am J Epidemiol. 2011;173:162–170. doi: 10.1093/aje/kwq361. [DOI] [PubMed] [Google Scholar]
- 26.Preiss D, Tikkanen MJ, Welsh P, et al. Lipid-modifying therapies and risk of pancreatitis: a meta-analysis. JAMA. 2012;308:804–811. doi: 10.1001/jama.2012.8439. [DOI] [PubMed] [Google Scholar]
- 27.El-Sisi AA, Hegazy SK, Salem KA, AbdElkawy KS. Atorvastatin improves erectile dysfunction in patients initially irresponsive to Sildenafil by the activation of endothelial nitric oxide synthase. Int J Impot Res. 2013;25:143–148. doi: 10.1038/ijir.2012.46. [DOI] [PubMed] [Google Scholar]
- 28.Subramanian S, Emami H, Vucic E, Singh P, Vijayakumar J, Fifer KM, Alon A, Shankar SS, Farkouh M, Rudd JH, Fayad ZA, Van Dyke TE, Tawakol A. High-dose atorvastatin reduces periodontal inflammation: a novel pleiotropic effect of statins. J Am Coll Cardiol. 2013;62:2382–2391. doi: 10.1016/j.jacc.2013.08.1627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Schoenfeld SR, Lu L, Rai SK, Seeger JD, Zhang Y, Choi HK. Statin use and mortality in rheumatoid arthritis: a general population-based cohort study. Ann Rheum Dis. 2016;75:1315–1320. doi: 10.1136/annrheumdis-2015-207714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.McCarey DW, McInnes IB, Madhok R, Hampson R, Scherbakov O, Ford I, Capell HA, Sattar N. Trial of Atorvastatin in Rheumatoid Arthritis (TARA): double-blind, randomised placebo-controlled trial. Lancet. 2004;363:2015–2021. doi: 10.1016/S0140-6736(04)16449-0. [DOI] [PubMed] [Google Scholar]
- 31.Glynn RJ, Danielson E, Fonseca FA, Genest J, Gotto AM, Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Ridker PM. A randomized trial of rosuvastatin in the prevention of venous thromboembolism. N Engl J Med. 2009;360:1851–1861. doi: 10.1056/NEJMoa0900241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sirtori CR. The pharmacology of statins. Pharmacol Res. 2014;88:3–11. doi: 10.1016/j.phrs.2014.03.002. [DOI] [PubMed] [Google Scholar]
- 33.Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S1–45. doi: 10.1161/01.cir.0000437738.63853.7a. [DOI] [PubMed] [Google Scholar]
- 34.McTaggart F. Comparative pharmacology of rosuvastatin. Atheroscler Suppl. 2003;4:9–14. doi: 10.1016/s1567-5688(03)00004-7. [DOI] [PubMed] [Google Scholar]
- 35.Schachter M. Chemical pharmacokinetic and pharmacodynamic properties of statins: an update. Fundam Clin Pharmacol. 2005;19:117–125. doi: 10.1111/j.1472-8206.2004.00299.x. [DOI] [PubMed] [Google Scholar]
- 36.Kivisto KT, Niemi M. Influence of drug transporter polymorphisms on pravastatin pharmacokinetics in humans. Pharm Res. 2007;24(2):239–247. doi: 10.1007/s11095-006-9159-2. [DOI] [PubMed] [Google Scholar]
- 37.Kitamura S, Maeda K, Wang Y, Sugiyama Y. Involvement of multiple transporters in the hepatobiliary transport of rosuvastatin. Drug Metab Dispos. 2008;36:2014–2023. doi: 10.1124/dmd.108.021410. [DOI] [PubMed] [Google Scholar]
- 38.Sakamoto K, Mikami H, Kimura J. Involvement of organic anion transporting polypeptides in the toxicity of hydrophilic pravastatin and lipophilic fluvastatin in rat skeletal myofibres. Br J Pharmacol. 2008;154:1482–1490. doi: 10.1038/bjp.2008.192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Grube M, Kock K, Oswald S, Draber K, Meissner K, Eckel L, Bohm M, Felix SB, Vogelgesang S, Jedlitschky G, Siegmund W, Warzok R, Kroemer HK. Organic anion transporting polypeptide 2B1 is a high-affinity transporter for atorvastatin and is expressed in the human heart. Clin Pharmacol Ther. 2006;80:607–620. doi: 10.1016/j.clpt.2006.09.010. [DOI] [PubMed] [Google Scholar]
- 40.Niessen J, Jedlitschky G, Grube M, et al. Human platelets express organic anion-transporting peptide 2B1, an uptake transporter for atorvastatin. Drug Metab Dispos. 2009;37:1129–1137. doi: 10.1124/dmd.108.024570. [DOI] [PubMed] [Google Scholar]
- 41.Weitz-Schmidt G, Welzenbach K, Brinkmann V, Kamata T, Kallen J, Bruns C, Cottens S, Takada Y, Hommel U. Statins selectively inhibit leukocyte function antigen-1 by binding to a novel regulatory integrin site. Nat Med. 2001;7:687–692. doi: 10.1038/89058. [DOI] [PubMed] [Google Scholar]
- 42.Lek HS, Morrison VL, Conneely M, Campbell PA, McGloin D, Kliche S, Watts C, Prescott A, Fagerholm SC. The spontaneously adhesive leukocyte function-associated antigen-1 (LFA-1) integrin in effector T cells mediates rapid actin- and calmodulin-dependent adhesion strengthening to ligand under shear flow. J Biol Chem. 2013;288:14698–14708. doi: 10.1074/jbc.M112.430918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Blanco-Colio LM, Martin-Ventura JL, de Teresa E, Farsang C, Gaw A, Gensini G, Leiter LA, Langer A, Martineau P, Egido J. Elevated ICAM-1 and MCP-1 plasma levels in subjects at high cardiovascular risk are diminished by atorvastatin treatment. Atorvastatin on Inflammatory Markers study: a substudy of Achieve Cholesterol Targets Fast with Atorvastatin Stratified Titration. Am Heart J. 2007;153:881–888. doi: 10.1016/j.ahj.2007.02.029. [DOI] [PubMed] [Google Scholar]
- 44.Kuhn EW, Slottosch I, Wahlers T, Liakopoulos OJ. Preoperative statin therapy for patients undergoing cardiac surgery. Cochrane Database Syst Rev. 2015 doi: 10.1002/14651858.CD008493.pub3. Cd008493. [DOI] [PubMed] [Google Scholar]
- 45.Patti G, Chello M, Candura D, Pasceri V, D’Ambrosio A, Covino E, Di Sciascio G. Randomized trial of atorvastatin for reduction of postoperative atrial fibrillation in patients undergoing cardiac surgery: results of the ARMYDA-3 (Atorvastatin for Reduction of MYocardial Dysrhythmia After cardiac surgery) study. Circulation. 2006;114:1455–1461. doi: 10.1161/CIRCULATIONAHA.106.621763. [DOI] [PubMed] [Google Scholar]
- 46.Lewicki M, Ng I, Schneider AG. HMG CoA reductase inhibitors (statins) for preventing acute kidney injury after surgical procedures requiring cardiac bypass. Cochrane Database Syst Rev. 2015 doi: 10.1002/14651858.CD010480.pub2. Cd010480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wang J, Gu C, Gao M, Yu W, Yu Y. Preoperative Statin Therapy and Renal Outcomes After Cardiac Surgery: A Meta-analysis and Meta-regression of 59,771 Patients. Can J Cardiol. 2015;3:1051–1060. doi: 10.1016/j.cjca.2015.02.034. [DOI] [PubMed] [Google Scholar]
- 48.Zheng Z, Jayaram R, Jiang L, Emberson J, Zhao Y, Li Q, Du J, Guarguagli S, Hill M, Chen Z, Collins R, Casadei B. Perioperative Rosuvastatin in Cardiac Surgery. N Engl J Med. 2016;374:1744–1753. doi: 10.1056/NEJMoa1507750. [DOI] [PubMed] [Google Scholar]
- 49.Billings FTt, Hendricks PA, Schildcrout JS, Shi Y, Petracek MR, Byrne JG, Brown NJ. High-Dose Perioperative Atorvastatin and Acute Kidney Injury Following Cardiac Surgery: A Randomized Clinical Trial. JAMA. 2016;315:877–888. doi: 10.1001/jama.2016.0548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Yusuf S, Bosch J, Dagenais G, et al. Cholesterol Lowering in Intermediate-Risk Persons without Cardiovascular Disease. N Engl J Med. 2016;374:2021–2031. doi: 10.1056/NEJMoa1600176. [DOI] [PubMed] [Google Scholar]
- 51.de Lemos JA, Blazing MA, Wiviott SD, et al. Early intensive vs a delayed conservative simvastatin strategy in patients with acute coronary syndromes: phase Z of the A to Z trial. JAMA. 2004;292:1307–1316. doi: 10.1001/jama.292.11.1307. [DOI] [PubMed] [Google Scholar]
- 52.Kinlay S, Schwartz GG, Olsson AG, Rifai N, Leslie SJ, Sasiela WJ, Szarek M, Libby P, Ganz P. High-dose atorvastatin enhances the decline in inflammatory markers in patients with acute coronary syndromes in the MIRACL study. Circulation. 2003;108:1560–1566. doi: 10.1161/01.CIR.0000091404.09558.AF. [DOI] [PubMed] [Google Scholar]
- 53.Werner C, Laufs U. Moving beyond the "LDL hypothesis". Vasa. 2015;44:333–340. doi: 10.1024/0301-1526/a000451. [DOI] [PubMed] [Google Scholar]
- 54.Maack C, Kartes T, Kilter H, Schafers HJ, Nickenig G, Bohm M, Laufs U. Oxygen free radical release in human failing myocardium is associated with increased activity of rac1-GTPase and represents a target for statin treatment. Circulation. 2003;108:1567–1574. doi: 10.1161/01.CIR.0000091084.46500.BB. [DOI] [PubMed] [Google Scholar]
- 55.Silverman MG, Ference BA, Im K, Wiviott SD, Giugliano RP, Grundy SM, Braunwald E, Sabatine MS. Association Between Lowering LDL-C and Cardiovascular Risk Reduction Among Different Therapeutic Interventions: A Systematic Review and Meta-analysis. JAMA. 2016;316:1289–1297. doi: 10.1001/jama.2016.13985. [DOI] [PubMed] [Google Scholar]
- 56.Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N Engl J Med. 2015;372:2387–2397. doi: 10.1056/NEJMoa1410489. [DOI] [PubMed] [Google Scholar]
- 57.The Lipid Research Clinics Coronary Primary Prevention Trial results I. Reduction in incidence of coronary heart disease. JAMA. 1984;251:351–364. doi: 10.1001/jama.1984.03340270029025. [DOI] [PubMed] [Google Scholar]
- 58.Buchwald H, Varco RL, Matts JP, Long JM, Fitch LL, Campbell GS, Pearce MB, Yellin AE, Edmiston WA, Smink RD, Jr, et al. Effect of partial ileal bypass surgery on mortality and morbidity from coronary heart disease in patients with hypercholesterolemia. Report of the Program on the Surgical Control of the Hyperlipidemias (POSCH) N Engl J Med. 1990;323:946–955. doi: 10.1056/NEJM199010043231404. [DOI] [PubMed] [Google Scholar]
- 59.Williams JK, Sukhova GK, Herrington DM, Libby P. Pravastatin has cholesterol-lowering independent effects on the artery wall of atherosclerotic monkeys. J Am Coll Cardiol. 1998;31:684–691. doi: 10.1016/s0735-1097(97)00537-8. [DOI] [PubMed] [Google Scholar]
- 60.Temel RE, Tang W, Ma Y, Rudel LL, Willingham MC, Ioannou YA, Davies JP, Nilsson LM, Yu L. Hepatic Niemann-Pick C1-like 1 regulates biliary cholesterol concentration and is a target of ezetimibe. J Clin Invest. 2007;117:1968–1978. doi: 10.1172/JCI30060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Gouni-Berthold I, Berthold HK, Gylling H, Hallikainen M, Giannakidou E, Stier S, Ko Y, Patel D, Soutar AK, Seedorf U, Mantzoros CS, Plat J, Krone W. Effects of ezetimibe and/or simvastatin on LDL receptor protein expression and on LDL receptor and HMG-CoA reductase gene expression: a randomized trial in healthy men. Atherosclerosis. 2008;198:198–207. doi: 10.1016/j.atherosclerosis.2007.09.034. [DOI] [PubMed] [Google Scholar]
- 62.Landmesser U, Bahlmann F, Mueller M, Spiekermann S, Kirchhoff N, Schulz S, Manes C, Fischer D, de Groot K, Fliser D, Fauler G, Marz W, Drexler H. Simvastatin versus ezetimibe: pleiotropic and lipid-lowering effects on endothelial function in humans. Circulation. 2005;111:2356–2363. doi: 10.1161/01.CIR.0000164260.82417.3F. [DOI] [PubMed] [Google Scholar]
- 63.Liu PY, Liu YW, Lin LJ, Chen JH, Liao JK. Evidence for statin pleiotropy in humans: differential effects of statins and ezetimibe on rho-associated coiled- coil containing protein kinase activity, endothelial function, and inflammation. Circulation. 2009;119:131–138. doi: 10.1161/CIRCULATIONAHA.108.813311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Fichtlscherer S, Schmidt-Lucke C, Bojunga S, Rossig L, Heeschen C, Dimmeler S, Zeiher AM. Differential effects of short-term lipid lowering with ezetimibe and statins on endothelial function in patients with CAD: clinical evidence for ’pleiotropic’ functions of statin therapy. Eur Heart J. 2006;27:1182–1190. doi: 10.1093/eurheartj/ehi881. [DOI] [PubMed] [Google Scholar]
- 65.Rudofsky G, Reismann P, Groener JB, Djuric Z, Fleming T, Metzner C, Grafe IA, Bierhaus A, Nawroth PP. Identical LDL-cholesterol lowering but non-identical effects on NF-kappaB activity: High dose simvastatin vs combination therapy with ezetimibe. Atherosclerosis. 2012;223:190–196. doi: 10.1016/j.atherosclerosis.2012.04.003. [DOI] [PubMed] [Google Scholar]
- 66.Matsue Y, Matsumura A, Suzuki M, Hashimoto Y, Yoshida M. Differences in action of atorvastatin and ezetimibe in lowering low-density lipoprotein cholesterol and effect on endothelial function: randomized controlled trial. Circ J. 2013;77:1791–1798. doi: 10.1253/circj.cj-13-0033. [DOI] [PubMed] [Google Scholar]
- 67.Kawagoe Y, Hattori Y, Nakano A, Aoki C, Tanaka S, Ohta S, Iijima T, Tomizawa A, Jojima T, Kase H, Kasai K. Comparative study between high-dose fluvastatin and low-dose fluvastatin and ezetimibe with regard to the effect on endothelial function in diabetic patients. Endocr J. 2011;58:171–175. doi: 10.1507/endocrj.k10e-289. [DOI] [PubMed] [Google Scholar]
- 68.Pesaro AE, Serrano CV, Jr, Fernandes JL, Cavalcanti AB, Campos AH, Martins HS, Maranhao RC, de Lemos JA, Souza HP, Nicolau JC. Pleiotropic effects of ezetimibe/simvastatin vs. high dose simvastatin. Int J Cardiol. 2012;158:400–404. doi: 10.1016/j.ijcard.2011.01.062. [DOI] [PubMed] [Google Scholar]
- 69.Westerink J, Deanfield JE, Imholz BP, Spiering W, Basart DC, Coll B, Kastelein JJ, Visseren FL. High-dose statin monotherapy versus low-dose statin/ezetimibe combination on fasting and postprandial lipids and endothelial function in obese patients with the metabolic syndrome: The PANACEA study. Atherosclerosis. 2013;227:118–124. doi: 10.1016/j.atherosclerosis.2012.11.028. [DOI] [PubMed] [Google Scholar]
- 70.Laufs U, Wassmann S, Hilgers S, Ribaudo N, Bohm M, Nickenig G. Rapid effects on vascular function after initiation and withdrawal of atorvastatin in healthy, normocholesterolemic men. Am J Cardiol. 2001;88:1306–1307. doi: 10.1016/s0002-9149(01)02095-1. [DOI] [PubMed] [Google Scholar]
- 71.Blom DJ, Hala T, Bolognese M, et al. A 52-week placebo-controlled trial of evolocumab in hyperlipidemia. N Engl J Med. 2014;370:1809–1819. doi: 10.1056/NEJMoa1316222. [DOI] [PubMed] [Google Scholar]
- 72.Robinson JG, Farnier M, Krempf M, et al. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N Engl J Med. 2015;372:1489–1499. doi: 10.1056/NEJMoa1501031. [DOI] [PubMed] [Google Scholar]
- 73.Nissen SE, Tuzcu EM, Schoenhagen P, Brown BG, Ganz P, Vogel RA, Crowe T, Howard G, Cooper CJ, Brodie B, Grines CL, DeMaria AN. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. JAMA. 2004;291:1071–1080. doi: 10.1001/jama.291.9.1071. [DOI] [PubMed] [Google Scholar]
- 74.Nissen SE, Nicholls SJ, Sipahi I, et al. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. JAMA. 2006;295:1556–1565. doi: 10.1001/jama.295.13.jpc60002. [DOI] [PubMed] [Google Scholar]
- 75.Sahebkar A, Di Giosia P, Stamerra CA, Grassi D, Pedone C, Ferretti G, Bacchetti T, Ferri C, Giorgini P. Effect of monoclonal antibodies to PCSK9 on high- sensitivity C-reactive protein levels: a meta-analysis of 16 randomized controlled treatment arms. Br J Clin Pharmacol. 2016;81:1175–1190. doi: 10.1111/bcp.12905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Goldstein JL, Brown MS. Regulation of the mevalonate pathway. Nature. 1990;343:425–430. doi: 10.1038/343425a0. [DOI] [PubMed] [Google Scholar]
- 77.Van Aelst L, D’Souza-Schorey C. Rho GTPases and signaling networks. Genes Dev. 1997;11:2295–2322. doi: 10.1101/gad.11.18.2295. [DOI] [PubMed] [Google Scholar]
- 78.Cho KJ, Hill MM, Chigurupati S, Du G, Parton RG, Hancock JF. Therapeutic levels of the hydroxmethylglutaryl-coenzyme A reductase inhibitor lovastatin activate ras signaling via phospholipase D2. Mol Cell Biol. 2011;31:1110–1120. doi: 10.1128/MCB.00989-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Laufs U, La Fata V, Plutzky J, Liao JK. Upregulation of endothelial nitric oxide synthase by HMG CoA reductase inhibitors. Circulation. 1998;97:1129–1135. doi: 10.1161/01.cir.97.12.1129. [DOI] [PubMed] [Google Scholar]
- 80.Laufs U, Liao JK. Post-transcriptional regulation of endothelial nitric oxide synthase mRNA stability by Rho GTPase. J Biol Chem. 1998;273:24266–24271. doi: 10.1074/jbc.273.37.24266. [DOI] [PubMed] [Google Scholar]
- 81.Awan Z, Seidah NG, MacFadyen JG, Benjannet S, Chasman DI, Ridker PM, Genest J. Rosuvastatin, proprotein convertase subtilisin/kexin type 9 concentrations, and LDL cholesterol response: the JUPITER trial. Clin Chem. 2012;58:183–189. doi: 10.1373/clinchem.2011.172932. [DOI] [PubMed] [Google Scholar]
- 82.Shimizu T, Liao JK. Rho Kinases and Cardiac Remodeling. Circ J. 2016;80:1491–1498. doi: 10.1253/circj.CJ-16-0433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Noma K, Oyama N, Liao JK. Physiological role of ROCKs in the cardiovascular system. Am J Physiol Cell Physiol. 2006;290:C661–668. doi: 10.1152/ajpcell.00459.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Eto M, Kozai T, Cosentino F, Joch H, Luscher TF. Statin prevents tissue factor expression in human endothelial cells: role of Rho/Rho-kinase and Akt pathways. Circulation. 2002;105:1756–1759. doi: 10.1161/01.cir.0000015465.73933.3b. [DOI] [PubMed] [Google Scholar]
- 85.Kataoka C, Egashira K, Inoue S, Takemoto M, Ni W, Koyanagi M, Kitamoto S, Usui M, Kaibuchi K, Shimokawa H, Takeshita A. Important role of Rho-kinase in the pathogenesis of cardiovascular inflammation and remodeling induced by long-term blockade of nitric oxide synthesis in rats. Hypertension. 2002;39:245–250. doi: 10.1161/hy0202.103271. [DOI] [PubMed] [Google Scholar]
- 86.Higashi M, Shimokawa H, Hattori T, Hiroki J, Mukai Y, Morikawa K, Ichiki T, Takahashi S, Takeshita A. Long-term inhibition of Rho-kinase suppresses angiotensin II-induced cardiovascular hypertrophy in rats in vivo: effect on endothelial NAD(P)H oxidase system. Circ Res. 2003;93:767–775. doi: 10.1161/01.RES.0000096650.91688.28. [DOI] [PubMed] [Google Scholar]
- 87.Hattori T, Shimokawa H, Higashi M, Hiroki J, Mukai Y, Tsutsui H, Kaibuchi K, Takeshita A. Long-term inhibition of Rho-kinase suppresses left ventricular remodeling after myocardial infarction in mice. Circulation. 2004;109:2234–2239. doi: 10.1161/01.CIR.0000127939.16111.58. [DOI] [PubMed] [Google Scholar]
- 88.Li Q, Xu Y, Li X, Guo Y, Liu G. Inhibition of Rho-kinase ameliorates myocardial remodeling and fibrosis in pressure overload and myocardial infarction: role of TGF-beta1-TAK1. Toxicol Lett. 2012;211:91–97. doi: 10.1016/j.toxlet.2012.03.006. [DOI] [PubMed] [Google Scholar]
- 89.Hata T, Soga J, Hidaka T, Idei N, Fujii Y, Fujimura N, Mikami S, Maruhashi T, Kihara Y, Chayama K, Kato H, Noma K, Liao JK, Higashi Y. Calcium channel blocker and Rho-associated kinase activity in patients with hypertension. J Hypertens. 2011;29:373–379. doi: 10.1097/HJH.0b013e328340902d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Do e Z, Fukumoto Y, Takaki A, Tawara S, Ohashi J, Nakano M, Tada T, Saji K, Sugimura K, Fujita H, Hoshikawa Y, Nawata J, Kondo T, Shimokawa H. Evidence for Rho-kinase activation in patients with pulmonary arterial hypertension. Circ J. 2009;73:1731–1739. doi: 10.1253/circj.cj-09-0135. [DOI] [PubMed] [Google Scholar]
- 91.Liu PY, Chen JH, Lin LJ, Liao JK. Increased Rho kinase activity in a Taiwanese population with metabolic syndrome. J Am Coll Cardiol. 2007;49:1619–1624. doi: 10.1016/j.jacc.2006.12.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Nohria A, Grunert ME, Rikitake Y, Noma K, Prsic A, Ganz P, Liao JK, Creager MA. Rho kinase inhibition improves endothelial function in human subjects with coronary artery disease. Circ Res. 2006;99:1426–1432. doi: 10.1161/01.RES.0000251668.39526.c7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Hung MJ, Cherng WJ, Hung MY, Kuo LT, Cheng CW, Wang CH, Yang NI, Liao JK. Increased leukocyte Rho-associated coiled-coil containing protein kinase activity predicts the presence and severity of coronary vasospastic angina. Atherosclerosis. 2012;221:521–526. doi: 10.1016/j.atherosclerosis.2012.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Nohria A, Prsic A, Liu PY, Okamoto R, Creager MA, Selwyn A, Liao JK, Ganz P. Statins inhibit Rho kinase activity in patients with atherosclerosis. Atherosclerosis. 2009;205:517–521. doi: 10.1016/j.atherosclerosis.2008.12.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Gabrielli L, Winter JL, Godoy I, McNab P, Padilla I, Cordova S, Rigotti P, Novoa U, Mora I, Garcia L, Ocaranza MP, Jalil JE. Increased rho-kinase activity in hypertensive patients with left ventricular hypertrophy. Am J Hypertens. 2014;27:838–845. doi: 10.1093/ajh/hpt234. [DOI] [PubMed] [Google Scholar]
- 96.Calo LA, Vertolli U, Pagnin E, Ravarotto V, Davis PA, Lupia M, Naso E, Maiolino G, Naso A. Increased rho kinase activity in mononuclear cells of dialysis and stage 3-4 chronic kidney disease patients with left ventricular hypertrophy: Cardiovascular risk implications. Life Sci. 2016;148:80–85. doi: 10.1016/j.lfs.2016.02.019. [DOI] [PubMed] [Google Scholar]
- 97.Ocaranza MP, Gabrielli L, Mora I, Garcia L, McNab P, Godoy I, Braun S, Cordova S, Castro P, Novoa U, Chiong M, Lavandero S, Jalil JE. Markedly increased Rho-kinase activity in circulating leukocytes in patients with chronic heart failure. Am Heart J. 2011;161:931–937. doi: 10.1016/j.ahj.2011.01.024. [DOI] [PubMed] [Google Scholar]
- 98.Dong M, Liao JK, Fang F, Lee AP, Yan BP, Liu M, Yu CM. Increased Rho kinase activity in congestive heart failure. Eur J Heart Fail. 2012;14(9):965–973. doi: 10.1093/eurjhf/hfs068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Do e Z, Fukumoto Y, Sugimura K, et al. Rho-kinase activation in patients with heart failure. Circ J. 2013;77:2542–2550. doi: 10.1253/circj.cj-13-0397. [DOI] [PubMed] [Google Scholar]
- 100.Ohnaka K, Shimoda S, Nawata H, Shimokawa H, Kaibuchi K, Iwamoto Y, Takayanagi R. Pitavastatin enhanced BMP-2 and osteocalcin expression by inhibition of Rho-associated kinase in human osteoblasts. Biochem Biophys Res Commun. 2001;287:337–342. doi: 10.1006/bbrc.2001.5597. [DOI] [PubMed] [Google Scholar]
- 101.Tramontano AF, O’Leary J, Black AD, Muniyappa R, Cutaia MV, El-Sherif N. Statin decreases endothelial microparticle release from human coronary artery endothelial cells: implication for the Rho-kinase pathway. Biochem Biophys Res Commun. 2004;320:34–38. doi: 10.1016/j.bbrc.2004.05.127. [DOI] [PubMed] [Google Scholar]
- 102.Gojo A, Utsunomiya K, Taniguchi K, Yokota T, Ishizawa S, Kanazawa Y, Kurata H, Tajima N. The Rho-kinase inhibitor, fasudil, attenuates diabetic nephropathy in streptozotocin-induced diabetic rats. Eur J Pharmacol. 2007;568:242–247. doi: 10.1016/j.ejphar.2007.04.011. [DOI] [PubMed] [Google Scholar]
- 103.Yamanouchi D, Banno H, Nakayama M, Sugimoto M, Fujita H, Kobayashi M, Kuwano H, Komori K. Hydrophilic statin suppresses vein graft intimal hyperplasia via endothelial cell-tropic Rho-kinase inhibition. J Vasc Surg. 2005;42:757–764. doi: 10.1016/j.jvs.2005.05.041. [DOI] [PubMed] [Google Scholar]
- 104.Kozai T, Eto M, Yang Z, Shimokawa H, Luscher TF. Statins prevent pulsatile stretch-induced proliferation of human saphenous vein smooth muscle cells via inhibition of Rho/Rho-kinase pathway. Cardiovasc Res. 2005;68:475–482. doi: 10.1016/j.cardiores.2005.07.002. [DOI] [PubMed] [Google Scholar]
- 105.Trebicka J, Hennenberg M, Laleman W, Shelest N, Biecker E, Schepke M, Nevens F, Sauerbruch T, Heller J. Atorvastatin lowers portal pressure in cirrhotic rats by inhibition of RhoA/Rho-kinase and activation of endothelial nitric oxide synthase. Hepatology. 2007;46:242–253. doi: 10.1002/hep.21673. [DOI] [PubMed] [Google Scholar]
- 106.McNeish AJ, Jimenez-Altayo F, Cottrell GS, Garland CJ. Statins and selective inhibition of Rho kinase protect small conductance calcium-activated potassium channel function (K(Ca)2.3) in cerebral arteries. PLoS One. 2012;7:e46735. doi: 10.1371/journal.pone.0046735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Ma MM, Li SY, Wang M, Guan YY. Simvastatin attenuated cerebrovascular cell proliferation in the development of hypertension through Rho/Rho-kinase pathway. J Cardiovasc Pharmacol. 2012;59:576–582. doi: 10.1097/FJC.0b013e318250ba2c. [DOI] [PubMed] [Google Scholar]
- 108.Rawlings R, Nohria A, Liu PY, Donnelly J, Creager MA, Ganz P, Selwyn A, Liao JK. Comparison of effects of rosuvastatin (10 mg) versus atorvastatin (40 mg) on rho kinase activity in caucasian men with a previous atherosclerotic event. Am J Cardiol. 2009;103:437–441. doi: 10.1016/j.amjcard.2008.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Brown JH, Del Re DP, Sussman MA. The Rac and Rho hall of fame: a decade of hypertrophic signaling hits. Circ Res. 2006;98:730–742. doi: 10.1161/01.RES.0000216039.75913.9e. [DOI] [PubMed] [Google Scholar]
- 110.Sawada N, Li Y, Liao JK. Novel aspects of the roles of Rac1 GTPase in the cardiovascular system. Curr Opin Pharmacol. 2010;10:116–121. doi: 10.1016/j.coph.2009.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Takemoto M, Node K, Nakagami H, Liao Y, Grimm M, Takemoto Y, Kitakaze M, Liao JK. Statins as antioxidant therapy for preventing cardiac myocyte hypertrophy. J Clin Invest. 2001;108:1429–1437. doi: 10.1172/JCI13350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Miller YI, Choi SH, Fang L, Tsimikas S. Lipoprotein modification and macrophage uptake: role of pathologic cholesterol transport in atherogenesis. Subcell Biochem. 2010;51:229–251. doi: 10.1007/978-90-481-8622-8_8. [DOI] [PubMed] [Google Scholar]
- 113.Wassmann S, Laufs U, Baumer AT, Muller K, Ahlbory K, Linz W, Itter G, Rosen R, Bohm M, Nickenig G. HMG-CoA reductase inhibitors improve endothelial dysfunction in normocholesterolemic hypertension via reduced production of reactive oxygen species. Hypertension. 2001;37:1450–1457. doi: 10.1161/01.hyp.37.6.1450. [DOI] [PubMed] [Google Scholar]
- 114.Custodis F, Eberl M, Kilter H, Bohm M, Laufs U. Association of RhoGDIalpha with Rac1 GTPase mediates free radical production during myocardial hypertrophy. Cardiovasc Res. 2006;71:342–351. doi: 10.1016/j.cardiores.2006.04.005. [DOI] [PubMed] [Google Scholar]
- 115.Antoniades C, Bakogiannis C, Tousoulis D, et al. Preoperative atorvastatin treatment in CABG patients rapidly improves vein graft redox state by inhibition of Rac1 and NADPH-oxidase activity. Circulation. 2010;122:S66–73. doi: 10.1161/CIRCULATIONAHA.109.927376. [DOI] [PubMed] [Google Scholar]
- 116.Antoniades C, Bakogiannis C, Leeson P, et al. Rapid, direct effects of statin treatment on arterial redox state and nitric oxide bioavailability in human atherosclerosis via tetrahydrobiopterin-mediated endothelial nitric oxide synthase coupling. Circulation. 2011;124:335–345. doi: 10.1161/CIRCULATIONAHA.110.985150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Adam O, Frost G, Custodis F, Sussman MA, Schafers HJ, Bohm M, Laufs U. Role of Rac1 GTPase activation in atrial fibrillation. J Am Coll Cardiol. 2007;50:359–367. doi: 10.1016/j.jacc.2007.03.041. [DOI] [PubMed] [Google Scholar]
- 118.Reilly SN, Jayaram R, Nahar K, Antoniades C, Verheule S, Channon KM, Alp NJ, Schotten U, Casadei B. Atrial sources of reactive oxygen species vary with the duration and substrate of atrial fibrillation: implications for the antiarrhythmic effect of statins. Circulation. 2011;124:1107–1117. doi: 10.1161/CIRCULATIONAHA.111.029223. [DOI] [PubMed] [Google Scholar]
- 119.Yano M, Matsumura T, Senokuchi T, et al. Statins activate peroxisome proliferator-activated receptor gamma through extracellular signal-regulated kinase 1/2 and p38 mitogen-activated protein kinase-dependent cyclooxygenase-2 expression in macrophages. Circ Res. 2007;100:1442–1451. doi: 10.1161/01.RES.0000268411.49545.9c. [DOI] [PubMed] [Google Scholar]
- 120.Paumelle R, Blanquart C, Briand O, Barbier O, Duhem C, Woerly G, Percevault F, Fruchart JC, Dombrowicz D, Glineur C, Staels B. Acute antiinflammatory properties of statins involve peroxisome proliferator-activated receptor-alpha via inhibition of the protein kinase C signaling pathway. Circ Res. 2006;98:361–369. doi: 10.1161/01.RES.0000202706.70992.95. [DOI] [PubMed] [Google Scholar]
- 121.Pucci A, Formato L, Muscio M, et al. PPARgamma in coronary atherosclerosis: in vivo expression pattern and correlations with hyperlipidemic status and statin treatment. Atherosclerosis. 2011;218:479–485. doi: 10.1016/j.atherosclerosis.2011.06.009. [DOI] [PubMed] [Google Scholar]
- 122.Corti R, Osende JI, Fallon JT, Fuster V, Mizsei G, Jneid H, Wright SD, Chaplin WF, Badimon JJ. The selective peroxisomal proliferator-activated receptor-gamma agonist has an additive effect on plaque regression in combination with simvastatin in experimental atherosclerosis: in vivo study by high-resolution magnetic resonance imaging. J Am Coll Cardiol. 2004;43:464–473. doi: 10.1016/j.jacc.2003.08.048. [DOI] [PubMed] [Google Scholar]
- 123.Chen M, Li H, Wang G, Shen X, Zhao S, Su W. Atorvastatin prevents advanced glycation end products (AGEs)-induced cardiac fibrosis via activating peroxisome proliferator-activated receptor gamma (PPAR-gamma) Metabolism. 2016;65:441–453. doi: 10.1016/j.metabol.2015.11.007. [DOI] [PubMed] [Google Scholar]
- 124.Bouitbir J, Charles AL, Echaniz-Laguna A, Kindo M, Daussin F, Auwerx J, Piquard F, Geny B, Zoll J. Opposite effects of statins on mitochondria of cardiac and skeletal muscles: a ’mitohormesis’ mechanism involving reactive oxygen species and PGC-1. Eur Heart J. 2012;33:1397–1407. doi: 10.1093/eurheartj/ehr224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Preiss D, Seshasai SR, Welsh P, et al. Risk of incident diabetes with intensive-dose compared with moderate-dose statin therapy: a meta-analysis. JAMA. 2011;305:2556–2564. doi: 10.1001/jama.2011.860. [DOI] [PubMed] [Google Scholar]
- 126.Gauthier TW, Scalia R, Murohara T, Guo JP, Lefer AM. Nitric oxide protects against leukocyte-endothelium interactions in the early stages of hypercholesterolemia. Arterioscler Thromb Vasc Biol. 1995;15:1652–1659. doi: 10.1161/01.atv.15.10.1652. [DOI] [PubMed] [Google Scholar]
- 127.Takemoto M, Sun J, Hiroki J, Shimokawa H, Liao JK. Rho-kinase mediates hypoxia-induced downregulation of endothelial nitric oxide synthase. Circulation. 2002;106:57–62. doi: 10.1161/01.cir.0000020682.73694.ab. [DOI] [PubMed] [Google Scholar]
- 128.Rikitake Y, Kim HH, Huang Z, Seto M, Yano K, Asano T, Moskowitz MA, Liao JK. Inhibition of Rho kinase (ROCK) leads to increased cerebral blood flow and stroke protection. Stroke. 2005;36:2251–2257. doi: 10.1161/01.STR.0000181077.84981.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Dimmeler S, Fleming I, Fisslthaler B, Hermann C, Busse R, Zeiher AM. Activation of nitric oxide synthase in endothelial cells by Akt-dependent phosphorylation. Nature. 1999;399:601–605. doi: 10.1038/21224. [DOI] [PubMed] [Google Scholar]
- 130.Wolfrum S, Dendorfer A, Rikitake Y, Stalker TJ, Gong Y, Scalia R, Dominiak P, Liao JK. Inhibition of Rho-kinase leads to rapid activation of phosphatidylinositol 3-kinase/protein kinase Akt and cardiovascular protection. Arterioscler Thromb Vasc Biol. 2004;24:1842–1847. doi: 10.1161/01.ATV.0000142813.33538.82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.van der Heijden M, Versteilen AM, Sipkema P, van Nieuw Amerongen GP, Musters RJ, Groeneveld AB. Rho-kinase-dependent F-actin rearrangement is involved in the inhibition of PI3-kinase/Akt during ischemia-reperfusion-induced endothelial cell apoptosis. Apoptosis. 2008;13:404–412. doi: 10.1007/s10495-007-0173-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Pelat M, Dessy C, Massion P, Desager JP, Feron O, Balligand JL. Rosuvastatin decreases caveolin-1 and improves nitric oxide-dependent heart rate and blood pressure variability in apolipoprotein E-/- mice in vivo. Circulation. 2003;107:2480–2486. doi: 10.1161/01.CIR.0000065601.83526.3E. [DOI] [PubMed] [Google Scholar]
- 133.Sen-Banerjee S, Mir S, Lin Z, Hamik A, Atkins GB, Das H, Banerjee P, Kumar A, Jain MK. Kruppel-like factor 2 as a novel mediator of statin effects in endothelial cells. Circulation. 2005;112:720–726. doi: 10.1161/CIRCULATIONAHA.104.525774. [DOI] [PubMed] [Google Scholar]
- 134.Bu DX, Tarrio M, Grabie N, Zhang Y, Yamazaki H, Stavrakis G, Maganto-Garcia E, Pepper-Cunningham Z, Jarolim P, Aikawa M, Garcia-Cardena G, Lichtman AH. Statin-induced Kruppel-like factor 2 expression in human and mouse T cells reduces inflammatory and pathogenic responses. J Clin Invest. 2010;120:1961–1970. doi: 10.1172/JCI41384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Giannotti G, Doerries C, Mocharla PS, et al. Impaired endothelial repair capacity of early endothelial progenitor cells in prehypertension: relation to endothelial dysfunction. Hypertension. 2010;55:1389–1397. doi: 10.1161/HYPERTENSIONAHA.109.141614. [DOI] [PubMed] [Google Scholar]
- 136.Vasa M, Fichtlscherer S, Adler K, Aicher A, Martin H, Zeiher AM, Dimmeler S. Increase in circulating endothelial progenitor cells by statin therapy in patients with stable coronary artery disease. Circulation. 2001;103:2885–2890. doi: 10.1161/hc2401.092816. [DOI] [PubMed] [Google Scholar]
- 137.Weis M, Heeschen C, Glassford AJ, Cooke JP. Statins have biphasic effects on angiogenesis. Circulation. 2002;105:739–745. doi: 10.1161/hc0602.103393. [DOI] [PubMed] [Google Scholar]
- 138.Koutouzis M, Nomikos A, Nikolidakis S, Tzavara V, Andrikopoulos V, Nikolaou N, Barbatis C, Kyriakides ZS. Statin treated patients have reduced intraplaque angiogenesis in carotid endarterectomy specimens. Atherosclerosis. 2007;192:457–463. doi: 10.1016/j.atherosclerosis.2007.01.035. [DOI] [PubMed] [Google Scholar]
- 139.Braun-Dullaeus RC, Mann MJ, Dzau VJ. Cell cycle progression: new therapeutic target for vascular proliferative disease. Circulation. 1998;98:82–89. doi: 10.1161/01.cir.98.1.82. [DOI] [PubMed] [Google Scholar]
- 140.Kobashigawa JA, Katznelson S, Laks H, Johnson JA, Yeatman L, Wang XM, Chia D, Terasaki PI, Sabad A, Cogert GA, et al. Effect of pravastatin on outcomes after cardiac transplantation. N Engl J Med. 1995;333:621–627. doi: 10.1056/NEJM199509073331003. [DOI] [PubMed] [Google Scholar]
- 141.Laufs U, Marra D, Node K, Liao JK. 3-Hydroxy-3-methylglutaryl-CoA reductase inhibitors attenuate vascular smooth muscle proliferation by preventing rho GTPase-induced down-regulation of p27(Kip1) J Biol Chem. 1999;274:21926–21931. doi: 10.1074/jbc.274.31.21926. [DOI] [PubMed] [Google Scholar]
- 142.Chen Z, Fukutomi T, Zago AC, Ehlers R, Detmers PA, Wright SD, Rogers C, Simon DI. Simvastatin reduces neointimal thickening in low-density lipoprotein receptor-deficient mice after experimental angioplasty without changing plasma lipids. Circulation. 2002;106:20–23. doi: 10.1161/01.cir.0000022843.76104.01. [DOI] [PubMed] [Google Scholar]
- 143.Chandrasekar B, Mummidi S, Mahimainathan L, Patel DN, Bailey SR, Imam SZ, Greene WC, Valente AJ. Interleukin-18-induced human coronary artery smooth muscle cell migration is dependent on NF-kappaB- and AP-1-mediated matrix metalloproteinase-9 expression and is inhibited by atorvastatin. J Biol Chem. 2006;281:15099–15109. doi: 10.1074/jbc.M600200200. [DOI] [PubMed] [Google Scholar]
- 144.Li M, Liu Y, Dutt P, Fanburg BL, Toksoz D. Inhibition of serotonin-induced mitogenesis, migration, and ERK MAPK nuclear translocation in vascular smooth muscle cells by atorvastatin. Am J Physiol Lung Cell Mol Physiol. 2007;293:L463–471. doi: 10.1152/ajplung.00133.2007. [DOI] [PubMed] [Google Scholar]
- 145.Wang SM, Tsai YJ, Jiang MJ, Tseng YZ. Studies on the function of rho A protein in cardiac myofibrillogenesis. J Cell Biochem. 1997;66:43–53. [PubMed] [Google Scholar]
- 146.Satoh M, Ogita H, Takeshita K, Mukai Y, Kwiatkowski DJ, Liao JK. Requirement of Rac1 in the development of cardiac hypertrophy. Proc Natl Acad Sci U S A. 2006;103:7432–7437. doi: 10.1073/pnas.0510444103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Nagase M, Fujita T. Role of Rac1-mineralocorticoid-receptor signalling in renal and cardiac disease. Nat Rev Nephrol. 2013;9:86–98. doi: 10.1038/nrneph.2012.282. [DOI] [PubMed] [Google Scholar]
- 148.Tanaka S, Fukumoto Y, Nochioka K, Minami T, Kudo S, Shiba N, Takai Y, Williams CL, Liao JK, Shimokawa H. Statins exert the pleiotropic effects through small GTP-binding protein dissociation stimulator upregulation with a resultant Rac1 degradation. Arterioscler Thromb Vasc Biol. 2013;33:1591–1600. doi: 10.1161/ATVBAHA.112.300922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Kudo S, Satoh K, Nogi M, Suzuki K, Sunamura S, Omura J, Kikuchi N, Kurosawa R, Satoh T, Minami T, Ikeda S, Miyata S, Shimokawa H. SmgGDS as a Crucial Mediator of the Inhibitory Effects of Statins on Cardiac Hypertrophy and Fibrosis: Novel Mechanism of the Pleiotropic Effects of Statins. Hypertension. 2016;67:878–889. doi: 10.1161/HYPERTENSIONAHA.115.07089. [DOI] [PubMed] [Google Scholar]
- 150.Ma J, Wang Y, Zheng D, Wei M, Xu H, Peng T. Rac1 signalling mediates doxorubicin-induced cardiotoxicity through both reactive oxygen species-dependent and -independent pathways. Cardiovasc Res. 2013;97:77–87. doi: 10.1093/cvr/cvs309. [DOI] [PubMed] [Google Scholar]
- 151.Antoniades C, Demosthenous M, Reilly S, et al. Myocardial redox state predicts in-hospital clinical outcome after cardiac surgery effects of short-term pre-operative statin treatment. J Am Coll Cardiol. 2012;59:60–70. doi: 10.1016/j.jacc.2011.08.062. [DOI] [PubMed] [Google Scholar]
- 152.Del Re DP, Miyamoto S, Brown JH. RhoA/Rho kinase up-regulate Bax to activate a mitochondrial death pathway and induce cardiomyocyte apoptosis. J Biol Chem. 2007;282:8069–8078. doi: 10.1074/jbc.M604298200. [DOI] [PubMed] [Google Scholar]
- 153.Haudek SB, Gupta D, Dewald O, Schwartz RJ, Wei L, Trial J, Entman ML. Rho kinase-1 mediates cardiac fibrosis by regulating fibroblast precursor cell differentiation. Cardiovasc Res. 2009;83:511–518. doi: 10.1093/cvr/cvp135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Okamoto R, Li Y, Noma K, Hiroi Y, Liu PY, Taniguchi M, Ito M, Liao JK. FHL2 prevents cardiac hypertrophy in mice with cardiac-specific deletion of ROCK2. FASEB J. 2013;27:1439–1449. doi: 10.1096/fj.12-217018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Laufs U, Fata VL, Liao JK. Inhibition of 3-hydroxy-3-methylglutaryl (HMG)-CoA reductase blocks hypoxia-mediated down-regulation of endothelial nitric oxide synthase. J Biol Chem. 1997;272:31725–31729. doi: 10.1074/jbc.272.50.31725. [DOI] [PubMed] [Google Scholar]
- 156.Di Napoli P, Taccardi AA, Grilli A, De Lutiis MA, Barsotti A, Felaco M, De Caterina R. Chronic treatment with rosuvastatin modulates nitric oxide synthase expression and reduces ischemia-reperfusion injury in rat hearts. Cardiovasc Res. 2005;66:462–471. doi: 10.1016/j.cardiores.2005.02.008. [DOI] [PubMed] [Google Scholar]
- 157.De Caterina R, Libby P, Peng HB, Thannickal VJ, Rajavashisth TB, Gimbrone MA, Jr, Shin WS, Liao JK. Nitric oxide decreases cytokine-induced endothelial activation. Nitric oxide selectively reduces endothelial expression of adhesion molecules and proinflammatory cytokines. J Clin Invest. 1995;96:60–68. doi: 10.1172/JCI118074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158.Jones SP, Teshima Y, Akao M, Marban E. Simvastatin attenuates oxidant-induced mitochondrial dysfunction in cardiac myocytes. Circ Res. 2003;93:697–699. doi: 10.1161/01.RES.0000097262.21507.DF. [DOI] [PubMed] [Google Scholar]
- 159.Node K, Fujita M, Kitakaze M, Hori M, Liao JK. Short-term statin therapy improves cardiac function and symptoms in patients with idiopathic dilated cardiomyopathy. Circulation. 2003;108:839–843. doi: 10.1161/01.CIR.0000084539.58092.DE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Horwich TB, MacLellan WR, Fonarow GC. Statin therapy is associated with improved survival in ischemic and non-ischemic heart failure. J Am Coll Cardiol. 2004;43:642–648. doi: 10.1016/j.jacc.2003.07.049. [DOI] [PubMed] [Google Scholar]
- 161.Kjekshus J, Apetrei E, Barrios V, et al. Rosuvastatin in older patients with systolic heart failure. N Engl J Med. 2007;357:2248–2261. doi: 10.1056/NEJMoa0706201. [DOI] [PubMed] [Google Scholar]
- 162.Tavazzi L, Maggioni AP, Marchioli R, Barlera S, Franzosi MG, Latini R, Lucci D, Nicolosi GL, Porcu M, Tognoni G. Effect of rosuvastatin in patients with chronic heart failure (the GISSI-HF trial): a randomised, double-blind, placebo-controlled trial. Lancet. 2008;372:1231–1239. doi: 10.1016/S0140-6736(08)61240-4. [DOI] [PubMed] [Google Scholar]
- 163.Aoki I, Aoki N, Kawano K, Shimoyama K, Maki A, Homori M, Yanagisawa A, Yamamoto M, Kawai Y, Ishikawa K. Platelet-dependent thrombin generation in patients with hyperlipidemia. J Am Coll Cardiol. 1997;30:91–96. doi: 10.1016/s0735-1097(97)00129-0. [DOI] [PubMed] [Google Scholar]
- 164.Laufs U, Gertz K, Huang P, Nickenig G, Bohm M, Dirnagl U, Endres M. Atorvastatin upregulates type III nitric oxide synthase in thrombocytes, decreases platelet activation, and protects from cerebral ischemia in normocholesterolemic mice. Stroke. 2000;31:2442–2449. doi: 10.1161/01.str.31.10.2442. [DOI] [PubMed] [Google Scholar]
- 165.Haramaki N, Ikeda H, Takenaka K, Katoh A, Sugano R, Yamagishi S, Matsuoka H, Imaizumi T. Fluvastatin alters platelet aggregability in patients with hypercholesterolemia: possible improvement of intraplatelet redox imbalance via HMG-CoA reductase. Arterioscler Thromb Vasc Biol. 2007;27:1471–1477. doi: 10.1161/ATVBAHA.106.128793. [DOI] [PubMed] [Google Scholar]
- 166.Ali FY, Armstrong PC, Dhanji AR, Tucker AT, Paul-Clark MJ, Mitchell JA, Warner TD. Antiplatelet actions of statins and fibrates are mediated by PPARs. Arterioscler Thromb Vasc Biol. 2009;29:706–711. doi: 10.1161/ATVBAHA.108.183160. [DOI] [PubMed] [Google Scholar]
- 167.Pignatelli P, Carnevale R, Pastori D, Cangemi R, Napoleone L, Bartimoccia S, Nocella C, Basili S, Violi F. Immediate antioxidant and antiplatelet effect of atorvastatin via inhibition of Nox2. Circulation. 2012;126:92–103. doi: 10.1161/CIRCULATIONAHA.112.095554. [DOI] [PubMed] [Google Scholar]
- 168.Tousoulis D, Psarros C, Demosthenous M, Patel R, Antoniades C, Stefanadis C. Innate and adaptive inflammation as a therapeutic target in vascular disease: the emerging role of statins. J Am Coll Cardiol. 2014;63:2491–2502. doi: 10.1016/j.jacc.2014.01.054. [DOI] [PubMed] [Google Scholar]
- 169.Dichtl W, Dulak J, Frick M, Alber HF, Schwarzacher SP, Ares MP, Nilsson J, Pachinger O, Weidinger F. HMG-CoA reductase inhibitors regulate inflammatory transcription factors in human endothelial and vascular smooth muscle cells. Arterioscler Thromb Vasc Biol. 2003;23:58–63. doi: 10.1161/01.atv.0000043456.48735.20. [DOI] [PubMed] [Google Scholar]
- 170.Rezaie-Majd A, Maca T, Bucek RA, Valent P, Muller MR, Husslein P, Kashanipour A, Minar E, Baghestanian M. Simvastatin reduces expression of cytokines interleukin-6, interleukin-8, and monocyte chemoattractant protein-1 in circulating monocytes from hypercholesterolemic patients. Arterioscler Thromb Vasc Biol. 2002;22:1194–1199. doi: 10.1161/01.atv.0000022694.16328.cc. [DOI] [PubMed] [Google Scholar]
- 171.Jougasaki M, Ichiki T, Takenoshita Y, Setoguchi M. Statins suppress interleukin-6-induced monocyte chemo-attractant protein-1 by inhibiting Janus kinase/signal transducers and activators of transcription pathways in human vascular endothelial cells. Br J Pharmacol. 2010;159:1294–1303. doi: 10.1111/j.1476-5381.2009.00612.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172.Luan Z, Chase AJ, Newby AC. Statins inhibit secretion of metalloproteinases-1, -2, -3, and -9 from vascular smooth muscle cells and macrophages. Arterioscler Thromb Vasc Biol. 2003;23:769–775. doi: 10.1161/01.ATV.0000068646.76823.AE. [DOI] [PubMed] [Google Scholar]
- 173.Kagami S, Owada T, Kanari H, Saito Y, Suto A, Ikeda K, Hirose K, Watanabe N, Iwamoto I, Nakajima H. Protein geranylgeranylation regulates the balance between Th17 cells and Foxp3+ regulatory T cells. Int Immunol. 2009;21:679–689. doi: 10.1093/intimm/dxp037. [DOI] [PubMed] [Google Scholar]
- 174.Kim YC, Kim KK, Shevach EM. Simvastatin induces Foxp3+ T regulatory cells by modulation of transforming growth factor-beta signal transduction. Immunology. 2010;130:484–493. doi: 10.1111/j.1365-2567.2010.03269.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 175.Sato K, Nuki T, Gomita K, Weyand CM, Hagiwara N. Statins reduce endothelial cell apoptosis via inhibition of TRAIL expression on activated CD4 T cells in acute coronary syndrome. Atherosclerosis. 2010;213:33–39. doi: 10.1016/j.atherosclerosis.2010.03.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 176.Wang S, Dangerfield JP, Young RE, Nourshargh S. PECAM-1, alpha6 integrins and neutrophil elastase cooperate in mediating neutrophil transmigration. J Cell Sci. 2005;118:2067–2076. doi: 10.1242/jcs.02340. [DOI] [PubMed] [Google Scholar]
- 177.Hwang SJ, Ballantyne CM, Sharrett AR, Smith LC, Davis CE, Gotto AM, Jr, Boerwinkle E. Circulating adhesion molecules VCAM-1, ICAM-1, and E-selectin in carotid atherosclerosis and incident coronary heart disease cases: the Atherosclerosis Risk In Communities (ARIC) study. Circulation. 1997;96:4219–4225. doi: 10.1161/01.cir.96.12.4219. [DOI] [PubMed] [Google Scholar]
- 178.Marx N, Sukhova GK, Collins T, Libby P, Plutzky J. PPARalpha activators inhibit cytokine-induced vascular cell adhesion molecule-1 expression in human endothelial cells. Circulation. 1999;99:3125–3131. doi: 10.1161/01.cir.99.24.3125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179.Wojciak-Stothard B, Williams L, Ridley AJ. Monocyte adhesion and spreading on human endothelial cells is dependent on Rho-regulated receptor clustering. J Cell Biol. 1999;145:1293–1307. doi: 10.1083/jcb.145.6.1293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 180.Wei H, Fang L, Song J, Chatterjee S. Statin-inhibited endothelial permeability could be associated with its effect on PECAM-1 in endothelial cells. FEBS Lett. 2005;579:1272–1278. doi: 10.1016/j.febslet.2005.01.020. [DOI] [PubMed] [Google Scholar]
- 181.Yaghi S, Elkind MS. Lipids and Cerebrovascular Disease: Research and Practice. Stroke. 2015;46:3322–3328. doi: 10.1161/STROKEAHA.115.011164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 182.LaRosa JC, Grundy SM, Waters DD, Shear C, Barter P, Fruchart JC, Gotto AM, Greten H, Kastelein JJ, Shepherd J, Wenger NK. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med. 2005;352:1425–1435. doi: 10.1056/NEJMoa050461. [DOI] [PubMed] [Google Scholar]
- 183.Everett BM, Glynn RJ, MacFadyen JG, Ridker PM. Rosuvastatin in the prevention of stroke among men and women with elevated levels of C-reactive protein: justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) Circulation. 2010;121:143–150. doi: 10.1161/CIRCULATIONAHA.109.874834. [DOI] [PubMed] [Google Scholar]
- 184.Amarenco P, Bogousslavsky J, Callahan A, 3rd, Goldstein LB, Hennerici M, Rudolph AE, Sillesen H, Simunovic L, Szarek M, Welch KM, Zivin JA. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355:549–559. doi: 10.1056/NEJMoa061894. [DOI] [PubMed] [Google Scholar]
- 185.Ridker PM, Thuren T, Zalewski A, Libby P. Interleukin-1beta inhibition and the prevention of recurrent cardiovascular events: rationale and design of the Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS) Am Heart J. 2011;162:597–605. doi: 10.1016/j.ahj.2011.06.012. [DOI] [PubMed] [Google Scholar]
- 186.Everett BM, Pradhan AD, Solomon DH, Paynter N, Macfadyen J, Zaharris E, Gupta M, Clearfield M, Libby P, Hasan AA, Glynn RJ, Ridker PM. Rationale and design of the Cardiovascular Inflammation Reduction Trial: a test of the inflammatory hypothesis of atherothrombosis. Am Heart J. 2013;166:199–207.e115. doi: 10.1016/j.ahj.2013.03.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 187.Massaro M, Zampolli A, Scoditti E, Carluccio MA, Storelli C, Distante A, De Caterina R. Statins inhibit cyclooxygenase-2 and matrix metalloproteinase-9 in human endothelial cells: anti-angiogenic actions possibly contributing to plaque stability. Cardiovasc Res. 2010;86:311–320. doi: 10.1093/cvr/cvp375. [DOI] [PubMed] [Google Scholar]
- 188.Bourcier T, Libby P. HMG CoA reductase inhibitors reduce plasminogen activator inhibitor-1 expression by human vascular smooth muscle and endothelial cells. Arterioscler Thromb Vasc Biol. 2000;20:556–562. doi: 10.1161/01.atv.20.2.556. [DOI] [PubMed] [Google Scholar]
- 189.Mulhaupt F, Matter CM, Kwak BR, Pelli G, Veillard NR, Burger F, Graber P, Luscher TF, Mach F. Statins (HMG-CoA reductase inhibitors) reduce CD40 expression in human vascular cells. Cardiovasc Res. 2003;59:755–766. doi: 10.1016/s0008-6363(03)00515-7. [DOI] [PubMed] [Google Scholar]