

Abstract
Objective:
Extracorporeal membrane oxygenation (ECMO) is used to provide cardiorespiratory support during cardiopulmonary resuscitation (extracorporeal cardiopulmonary resuscitation; ECPR) unresponsive to conventional methods. In this study, the results of ECPR in a cardiac arrest setting after cardiac surgery in children were analyzed.
Methods:
In this retrospective cohort study, between November 2010 and June 2014, 613 congenital heart operations were performed by the same surgical team. Medical records of all the patients who experienced cardiac arrest and ECPR in an early postoperative period (n=25; 4%) were analyzed. Their ages were between 2 days and 4.5 years (median: 3 months). Sixteen patients had palliative procedures. In 88% of the patients, cardiac arrest episodes occurred in the first 24 h after operation. Mechanical support was provided by cardiopulmonary bypass only (n=10) or by ECMO (n=15) during CPR.
Results:
The CPR duration until commencing mechanical support was <20 min in two patients, 20–40 min in 11 patients, and >40 min in 12 patients. Eleven patients (44%) were weaned successfully from ECMO and survived more than 7 days. Five of them (20%) could be discharged. The CPR duration before ECMO (p=0.01) and biventricular physiology (p=0.022) was the key factor affecting survival. The follow-up duration was a mean of 15±11.9 months. While four patients were observed to have normal neuromotor development, one patient died of cerebral bleeding 6 months after discharge.
Conclusion:
Postoperative cardiac arrest usually occurs in the first 24 h after operation. ECPR provides a second chance for survival in children who have had cardiac arrest. Shortening the duration of CPR before ECMO might increase survival rates. (Anatol J Cardiol 2017; 17: 328-33)
Keywords: congenital heart disease, children, extracorporeal membrane oxygenation, cardiopulmonary resuscitation
Introduction
Children undergoing congenital heart surgery usually experience a critical period of time in the intensive care unit until hemodynamic stability can be achieved. Despite advances in critical care and monitoring facilities, a considerable number of patients may suffer from cardiac arrest during the postoperative period. Although the prevention of cardiac arrest is the main goal, it is not always possible. The prevalence of postoperative cardiac arrest after congenital heart surgery varies between 1.5 and 6% (1, 2). The treatment of cardiac arrest is therefore of vital importance, but even in the best centers, survival rates are around 10–20% by conventional cardiopulmonary resuscitation (CPR) methods. In 1992, a report by del Nido et al. (3) showed that extracorporeal membrane oxygenation (ECMO) support could be utilized as a rescue therapy during CPR (extracorporeal CPR; ECPR) in children with cardiac disease who had cardiopulmonary arrest and who failed to respond to conventional CPR-promoted survival. Recent reports have demonstrated that the use of ECPR techniques may increase survival rates to 33–51% in children (4, 5).
However, ECPR techniques are difficult to perform and require significant resources and an experienced team. Only a few centers in Turkey have this facility (6). In this study, we reviewed our 5 years’ experience of performing ECPR, according to the protocol developed for this study.
Methods
In this cohort study the medical reports of pediatric patients who received ECPR between November 2010 and June 2014 were retrospectively reviewed. Patients who underwent ECMO support due to a failure to wean them off from cardiopulmonary bypass or low cardiac output and patients who had a long period of conventional therapy, sepsis, and multiorgan failure were excluded from the study. During this period, the total number of congenital heart operations performed by our surgical team was 613. Twenty-five of them (4%) underwent ECPR. Their ages ranged from 2 days to 4.5 years old (median: 3 months). Ten patients were neonates, while 12 patients were infants. Eighteen of them were boys and seven girls. Their operative data are summarized in Table 1. Sixteen of the patients underwent palliative procedures, while the remaining patients had corrective operations. The patients’ Aristotle basic and comprehensive scores ranged from 6 to 11 (mean: 7.4±1.7) and from 6 to 13.5 (mean: 8.7±2.2), respectively. During the study period, all the patients who had cardiac arrest during early postoperative period were treated according to the protocol summarized in Figure 1–3. A flowchart showing the postoperative cardiac arrest protocol was hung on the wall in the intensive care unit, and detailed simulations were carried out several times to ensure everyone knew the protocol and to prevent collisions between personnel and an unnecessary waste of vital time.
Table 1.
Operative data of the patients
| Pathology/procedure | No | Survival |
|---|---|---|
| Systemic-pulmonary shunt | 6 | 1 |
| Total repair of TOF (1 with absent PV) | 5 | 3 |
| Pulmonary banding (1 bilateral banding) | 4 | – |
| Norwood stage 1 procedure | 2 | – |
| Supravalvular aortic stenosis | 1 | – |
| Truncus arteriosus | 1 | – |
| AVSD + PS repair | 1 | – |
| Arterial switch + VSD + IAA repair | 1 | 1 |
| Others | 4 | |
| Total | 25 |
AVSD - atrioventricular septal defect; IAA - interrupted aortic arch; PS - pulmonary stenosis; PV - pulmonary valve; TOF - tetralogy of Fallot; VSD - ventricular septal defect
Figure 1.
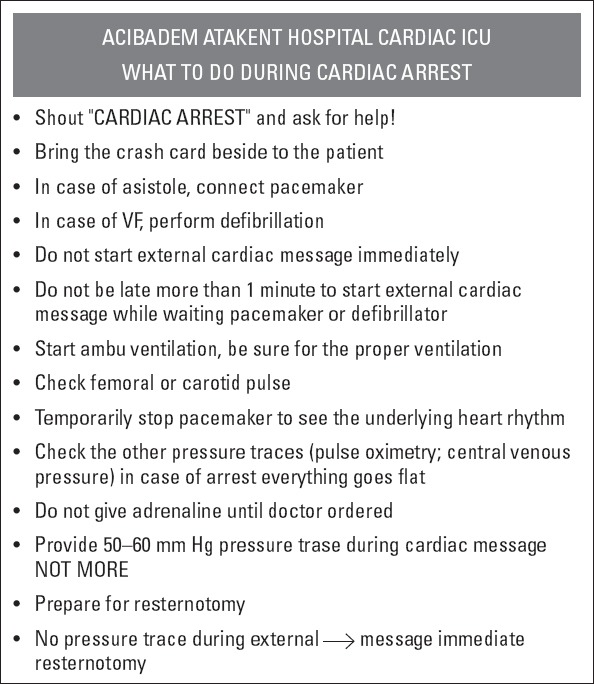
What to do during cardiac arrest
Figure 2.

Postoperative cardiac arrest protocol
Figure 3.
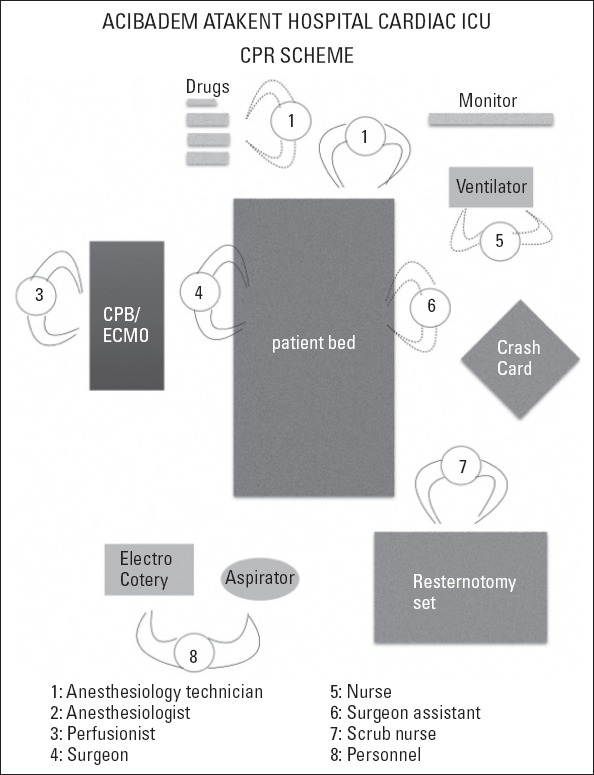
Bed-site organization scheme during ECPR
All the cannulations were performed using the ascending aorta and right atrium by reopening the sternal wound in the intensive care unit. Standard cardiopulmonary bypass (CPB) cannulas (Medtronic Inc., Minneapolis, Minnesota, USA) were used that were suitable for the patients’ body surface area to provide full flow support. When ECMO was used, veno-arterial support was accomplished in all the patients with the Medos ECMO system (Medos GmbH, Heilbronn, Germany). Heparin infusion was started after hemostasis was achieved. The ACT times were kept between 180 and 220 s with the continuous infusion of heparin during ECMO support, and then checked every 4–6 h. The ventricular function was evaluated every day by transthoracic echocardiography. When the ventricular function and hemodynamic parameters improved, the ECMO flow was gradually decreased to 50% and then 33% for several hours. Ventilation and inotropic support was optimized before weaning the patient off support. Successful weaning from ECPR was accepted after 1 week survival after weaning from support. All complications during and after ECPR were recorded. A follow-up was carried out for all the surviving patients. The patients’ families were informed as soon as possible when ECMO was started for the patients. Potential complications, expected survival, and expected ECMO duration were told in detail, including the expected termination time in case of severe complications and a failure to wean the patient off support. The Institutional Ethics Committee approved the study protocol.
Statistical analysis
Statistical analysis was performed using the SPSS version 11.5 for Windows software program (SPSS Inc., Chicago, IL, USA). All the data are given as the mean±standard deviation and median. The Mann–Whitney U test was used to compare the mean values between the groups, while a chi-square and Fisher’s exact test were used to compare the rates between the groups. A p value of <0.05 was considered to be statistically significant.
Results
Eleven patients (44%) were successfully weaned off ECPR, and five of them (20%) were discharged. Twelve of the cardiac arrest episodes (48%) occurred unexpectedly in patients who had stable hemodynamic conditions before cardiac arrest, while the others had already borderline hemodynamic conditions, such as elevated lactate levels, high inotropic doses, or malign dysrhythmias. Most of the cardiac arrest episodes occurred in the first 24 h (22/25; 88%). Two patients had cardiac arrest at postoperative day 2 and one patient at postoperative day 4. The timings of the cardiac arrests and survival were not statistically significant.
According to our protocol, 10 of the patients (40%) underwent CPB support only, for 2–6 h. Although four of them were successfully weaned off support (40%), none of them could be discharged (0%). In 11 patients (44%), we performed CPB support first and then mechanical support was continued with ECMO. Six of them were weaned off support successfully (54.5%), and three patients could be discharged (27.2%). For the remaining four patients (16%), ECMO support was instituted immediately after arrest; two of them were weaned off support successfully and both patients could be discharged (50%). The duration of ECMO support was between 36 h and 9 days (median: 3 days). The effect of the mode of support on survival was not statistically significant (p=0.077).
The duration of CPR before mechanical support was <20 min in two patients (both survived, 100%), 20–40 min in 11 patients (two survived, 18%), and >40 min in 12 patients (one survived, 8%). The duration of CPR was statistically significant on survival (p=0.01). While four of the nine patients (44.4%) who had corrective operations survived after ECPR, only one of the sixteen patients (6.2%) who had palliative procedures survived to discharge. The effect of corrective biventricular operation on survival was statistically significant (p=0.022). According to the blood gas analysis before cardiac arrest, serum lactate and blood pH levels were not significantly different between surviving and non-surviving patients (mean 5.39±3.08 vs. 6.07±3.44 and 7.34±0.14 vs. 7.30±0.12, respectively).
Only one of the ten neonates survived after ECPR, while four out of twelve infants survived (33.3%). None survived among the three children who underwent ECPR (0%) (p=NS). All the statistical data are summarized in Table 2.
Table 2.
Statistical data of the patients
| Non-survived | Survived | P | |
|---|---|---|---|
| Duration of CPR and mortality | |||
| <20 min | – | 2 | |
| 20–40 min | 9 | 2 | 0.01* |
| >40 min | 11 | 1 | |
| Mode of support and mortality | |||
| CPB only | 10 | – | |
| CPB then ECMO | 8 | 3 | 0.077* |
| ECMO | 2 | 2 | |
| Surgical procedure and mortality | |||
| Biventricular correction | 5 | 4 | |
| Palliation | 15 | 1 | 0.022* |
| Age and mortality | |||
| Neonate | 9 | 1 | |
| Infant | 8 | 4 | NS* |
| Children | 3 | 0 | |
| Timing of cardiac arrest and mortality | |||
| Postoperative day 1 | 17 | 5 | |
| Postoperative day 2 | 2 | – | |
| Postoperative day 4 | 1 | – | NS* |
| pH before mechanical support (mean±SD) | 7.30±0.12 | 7.34±0.14 | NS# |
| Lactate level before mechanical support (mean±SD) | 6.07±3.44 | 5.39±3.08 | NS# |
CPB - cardiopulmonary bypass; CPR - cardiopulmonary resuscitation; ECMO - extracorporeal membrane oxygenation; NS - not significant; SD - standard deviation. Statistical method: *Chi-square test; #Mann -Whitney U test
Severe bleeding and massive blood transfusion was necessary in five of the patients. One patient had gastrointestinal bleeding. None of the patients with bleeding complications survived. Renal dysfunction and renal replacement therapy were a rule for all the non-surviving patients. Other complications are shown in Table 3. Among the surviving patients, two had pneumonia, two had transient renal dysfunction, one had sepsis, and two needed a long duration of mechanical ventilation (>7 days). Two of the patients had mild neurologic dysfunction during discharge because of hypoxic encephalopathy. The median duration in the intensive care unit (ICU) stay of the surviving patients was 38 days (14–52 days). The median duration for hospital stay was 43 days (16–65 days). Nevertheless, the median duration of ICU stay of the non-surviving patients was 5 days (1–25 days).
Table 3.
Complications after ECPR
| n | % | |
|---|---|---|
| Renal dysfunction | 22 | 88 |
| Bleeding | 5 | 20 |
| Ventricular dysfunction | 5 | 20 |
| Sepsis, multiorgan failure | 4 | 16 |
| Low cardiac output | 3 | 12 |
| Severe neurologic impairment | 2 | 8 |
| Mediastinitis | 1 | 4 |
| Purpura fulminans | 1 | 4 |
All surviving patients were followed up for a mean duration of 15±11.9 months. One patient who had mild neurological deficit died 6 months after discharge, because of cerebral bleeding. Another patient with a mild neurologic deficit improved significantly, and the others were well with normal neuromotor development at the end of the follow-up period.
Discussion
In this retrospective cohort study, several important findings are documented. Most cardiac arrest episodes occurred in the period of the first 24 h after surgery. Some of them could be prevented or anticipated. Early intervention by mechanical support, for instance, may positively affect the survival, albeit most patients who need ECPR, usually need a few days of support for hemodynamic stability to be achieved.
Over the past decade, the advantage of ECPR in children having a cardiac arrest following the surgical correction of congenital heart disease (CHD) has become well recognized and its utilization has increased considerably (1–8). In 2010, pediatric advanced life support guidelines accepted ECPR as a class IIa indication of children in cardiac arrest refractory to standard resuscitation attempts, with a potentially reversible cause of arrest (9). Undoubtedly, the deployment of ECPR requires an enormous commitment and use of resources. After modern ECMO systems became available in Turkey in 2010, their usage has increased in congenital heart surgery centers thanks to education programs and reimbursement facilities (10). Despite increased experience with ECPR, ideal patient candidates have not been well identified owing to a multitude of factors affecting their outcomes, in addition to institutional variations in resources and management strategies.
One of the most important factors affecting survival is the duration of CPR (11–13). Many strategies have been developed to keep the duration of CPR as short as possible before commencing ECMO. For instance, all equipment and staff should be readily available in the intensive care unit at all times. A small emergency resternotomy set should be available containing the instruments necessary to perform the resternotomy. This should include a disposable scalpel, an all-in-one drape, a wire cutter, a heavy needle holder, and a single-piece sternal retractor (14). Resternotomy is indicated for children in whom resuscitative efforts are likely to last more than 5–10 min, in order to perform an internal cardiac massage and a rapid institution of ECMO (14). In modern high-volume cardiac centers, a pre-primed ECMO set is always present in the intensive care unit to prevent an unnecessary waste of time for the institution and for priming of the ECMO circuit. In our clinic, we usually try to keep at least one ECMO system in the ICU, but it is not always possible. Therefore, an available pre-primed ECMO set is not always present, due to the availability and cost. The cost of ECMO application is approximately 10 times more expensive than a standard CPB system. This is why we usually use CPB first, and then transfer to the ECMO when available. A short duration of CPB (2–6 h) is sometimes enough to provide stable hemodynamics after cardiac arrest, but according to our results, although four out of the ten patients were successfully weaned off CPB support, none of them could be discharged. After these results, we changed our protocol and now we start to perform ECMO support first whenever possible. We think that at least 2–3 days of mechanical support is usually necessary for recovery. Nevertheless, some authors have reported better results (15, 16). In some patients with borderline hemodynamics, we usually keep ready a crystalloid-primed CPB system in advance, i.e., for the next day’s operations, and use it in case of cardiac arrest at night. This method may significantly reduce the intervention time in a cardiac arrest setting while also avoiding an unnecessary waste of resources. In our series of tests, two patients with <20 min of CPR duration before mechanical support survived to discharge without significant sequela, while among another eleven patients who had >40 min of CPR duration, only one patient could be discharged.
The goal of reducing the ECMO initiation time for patients experiencing cardiac arrest appears self-evident as the duration of conventional CPR directly correlates with mortality and adverse neurologic outcomes (17). In addition, a recent meta-analysis of 288 ECPR patients reported that a CPR duration >30 min was an independent risk factor for mortality (4). In addition, an emphasis on the performance of high-quality CPR is necessary, as some studies have not shown a survival benefit from a reduced CPR duration (18, 19), suggesting the quality of pre-ECMO CPR may be as important as the duration of CPR (12).
Similar to our results, the Extracorporeal Life Support Organization (ELSO) study of pediatric cardiac patients requiring ECPR found that single ventricle physiology, a history of Norwood type palliation, and an arterial pH <7.01 were associated with increased mortality (18). Although speculative, it appears that patient selection for ECPR and the quality of CPR are more likely to influence mortality than CPR duration.
Utilizing the Extracorporeal Life Support Organization registry, Barrett et al. (20) reported a 22% incidence of CNS injury in ECPR patients. Patients with less severe metabolic acidosis before ECMO and an uncomplicated ECMO course were more likely to avoid neurological injury (18). Overall, the development of any type of complications among patients who have experienced ECPR is high (59%), with neurological complications being the most commonly reported (27%). After survival, a neurological complication would have the biggest impact on the quality of life for patients discharged alive with it (21). In our study, two out of the five surviving patients (40%) had a mild neurologic injury.
Other complications included renal injury, pulmonary hemorrhage, pneumothorax that required treatment, occurrence of arrhythmias, need for CPR during ECMO support, gastrointestinal hemorrhage, and hyperbilirubinemia. Of note, bloodstream infection, mechanical complications, thrombus in the ECMO circuit, and surgical or cannula site bleeding are the other important factors affecting survival (11). In our series, the most encountered complications were bleeding, renal dysfunction, and infectious complications.
We always do transthoracic cannulation for ECPR among patients after cardiac surgery. This is expected to be associated with better survival rates because it allows for open cardiac massage before cannulation and may allow more rapid ECMO deployment. However, the downsides of this approach are possibly a higher risk of bleeding and mediastinal infection after open chest cannulation (22). We encountered severe bleeding in six patients and mediastinitis in one patient, none of whom survived.
In this study, most of the cardiac arrest episodes occurred in the period of the first 24 h after cardiac surgery which indicated the importance of this period for hemodynamic stability and close monitoring. Although almost half of our patients had cardiac arrest unexpectedly, others had some clues for approaching cardiac arrest, such as elevated lactate levels, mild to moderate acidosis, or a necessity for high inotropic doses. For those patients with borderline hemodynamics, ECMO support could be performed before developing cardiac arrest. Nevertheless, it is not an easy decision, considering the risks of ECMO application. Delayed chest closure may be performed in patients who have borderline hemodynamics to prevent tight mediastinal syndrome or atypical tamponade. This may reduce the risk of cardiac arrest and low cardiac output. We use this strategy very liberally. In our recent study, we performed delayed chest closure in 48.4% of the neonates and early infants after cardiac surgery (23).
An institution-specific CPR protocol should be present in every cardiac ICU, because of the differences in staff and equipment resources. Our CPR protocol is shown in Figure 1–3. Regular staff education and cardiac arrest simulations may facilitate the intervention and prevent unnecessary collisions during CPR.
Information about the patients’ families is also very important for assessing potential complications, expected survival, and expected ECMO duration. The most difficult decision is the termination of support in the case of neurologically intact patients whose cardiac function is unexpected to recover. For these patients, the further therapeutic step should be cardiac transplantation or application of a long-term ventricular assist device. Actually this is the only way to improve the survival in patients who have undergone ECMO support (4, 11). In this study, we did not have such a patient, but it is a possibility. Therefore, some affiliations should be instituted for further therapies and heart transplantation and long-term assistance device facilities for children should be improved in our country.
Study limitations
This case series is subject to many limitations inherent in all retrospective observational studies. The small cohort size, the low number of events, and the multiple variables in this heterogeneous group of patients preclude sophisticated statistical analyses and limit the power of the study to identify clinically significant risk factors.
Conclusion
Our study demonstrates the importance of having a structured institutional ECPR protocol in salvaging children having refractory cardiac arrest following the surgical repair of CHD. The timely application of ECPR is essential to minimize organ injury and to enhance the chance of recovery. ECMO complications, particularly bleeding, and neurologic, renal, and pulmonary complications are frequent. ECPR has a potential to improve survival in children who experience cardiac arrest after cardiac surgery and to give them a second chance. Further studies should be planned for defining patient selection criteria for ECPR application.
Footnotes
Conflict of interest: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding: The authors received no financial support for the research and/or authorship of this article.
Peer-review: Externally peer-reviewed.
Authorship contributions: Concept- E.E.; Design – E.E.; Data collection &/or processing – S.A., D.S., F.A., O.Y., B.K.; Analysis &/or interpretation – E.E.; Literature search – O.Y., D.S., İ.H.D.; Writing – E.E.; Critical review – E.Ö.
References
- 1.Ahmadi AR, Aarabi MY. Postoperative cardiac arrest in children with congenital heart abnormalities. ARYA Atheroscler. 2013;9:145–9. [PMC free article] [PubMed] [Google Scholar]
- 2.Rhodes JF, Blaufox AD, Seiden HS, Asnes JD, Gross RP, Rhodes JP, et al. Cardiac arrest in infants after congenital heart surgery. Circulation. 1999;100:194–9. doi: 10.1161/01.cir.100.suppl_2.ii-194. [DOI] [PubMed] [Google Scholar]
- 3.Del Nido PJ, Dalton HJ, Tomson AE, Siewers RD. Extracorporeal membrane oxygenator rescue in children during cardiac arrest after cardiac surgery. Circulation. 1992;86:300–4. [PubMed] [Google Scholar]
- 4.Tajik M, Cardarelli MG. Extracorporeal membrane oxygenation after cardiac arrest in children: what do we know? Eur J Cardiothorac Surg. 2008;33:409–17. doi: 10.1016/j.ejcts.2007.12.018. [DOI] [PubMed] [Google Scholar]
- 5.Prodhan P, Fiser RT, Dyamenahalli U, Gossett J, Imamura M, Jaquiss RDB, et al. Outcomes after extracorporeal cardiopulmonary resuscitation (ECPR) following refractory pediatric cardiac arrest in the intensive care unit. Resuscitation. 2009;80:1124–9. doi: 10.1016/j.resuscitation.2009.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sarıoğlu T, Yalçınbaş YK, Erek E, Arnaz A, Türkekul Y, Narin B, et al. Results of pediatric mechanical assist for postcardiotomy ventricular failure and cardiac arrest. Turk Gogus Kalp Dama. 2014;22:1–6. [Google Scholar]
- 7.Aharon AS, Drinkwater DC, Churchwell KB, Quisling SV, Reddy VS, Taylor M, et al. Extracorporeal membrane oxygenation in children after repair of congenital cardiac lesions. Ann Thorac Surg. 2001;72:2095–101. doi: 10.1016/s0003-4975(01)03209-x. [DOI] [PubMed] [Google Scholar]
- 8.Wolf MJ, Kanter KR, Kirshbom PM, Kogon BE, Wagoner SF. Extracorporeal cardiopulmonary resuscitation for pediatric cardiac patients. Ann Thorac Surg. 2012;94:874–9. doi: 10.1016/j.athoracsur.2012.04.040. [DOI] [PubMed] [Google Scholar]
- 9.Kleinman ME, Chameides L, Schexnayder SM, Samson RA, Hazincki MF, Atkins DL, et al. 2010 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care science. Part 14: Pediatric advanced life support. Circulation. 2010;122:876–908. doi: 10.1161/CIRCULATIONAHA.110.971101. [DOI] [PubMed] [Google Scholar]
- 10.Erek E, Haydın S, Onan B, Onan IS, Yazıcı P, Koçyiğit O, et al. Extracorporeal life support experiences of a new congenital heart center in Turkey. Artificial Organs. 2013;37:29–34. doi: 10.1111/aor.12023. [DOI] [PubMed] [Google Scholar]
- 11.Thiagarajan RR, Laussen PC, Rycus PT, Bartlett RH, Bratton SL. Extracorporeal membrane oxygenation to aid cardiopulmonary resuscitation in infants and children. Circulation. 2007;116:1693–700. doi: 10.1161/CIRCULATIONAHA.106.680678. [DOI] [PubMed] [Google Scholar]
- 12.Turek JW, Andersen ND, Lawson DS, Bonadonna D, Turley RS, Peters MA, et al. Outcomes before and after implementation of a pediatric rapid response extracorporeal membrane oxygenation program. Ann Thorac Surg. 2013;95:2140–7. doi: 10.1016/j.athoracsur.2013.01.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Alsoufi B, Awan A, Manlhiot C, Gue hef A, Al-Halees Z, Al-Ahmadi M, et al. Results of rapid-response extracorporeal cardiopulmonary resuscitation in children with refractory cardiac arrest following cardiac surgery. Eur J Cardiothorac Surg. 2014;45:268–75. doi: 10.1093/ejcts/ezt319. [DOI] [PubMed] [Google Scholar]
- 14.Dunning J, Fabbri A, Kolh PH, Levine A, Lockowandt U, Mackay J, et al. Guideline for resuscitation in cardiac arrest after cardiac surgery. Eur J Cardiothorac Surg. 2009;36:3–28. doi: 10.1016/j.ejcts.2009.01.033. [DOI] [PubMed] [Google Scholar]
- 15.Wallmuller C, Sterz F, Testori C, Schober A, Stratil P, Hörburger D, et al. Emergency cardio-pulmonary bypass in cardiac arrest: seventeen years of experience. Resuscitation. 2013;84:326–30. doi: 10.1016/j.resuscitation.2012.05.029. [DOI] [PubMed] [Google Scholar]
- 16.Rousou JA, Engelman RM, Flack JE, Deaton DW, Owen SG. Emergency cardiopulmonary bypass in the cardiac surgical unit can be a lifesaving measure in postoperative cardiac arrest. Circulation. 1994;90:1280–4. [PubMed] [Google Scholar]
- 17.Slonim AD, Patel KM, Ruttimann UE, Pollack MM. Cardiopulmonary resuscitation in pediatric intensive care units. Crit Care Med. 1997;25:1951–5. doi: 10.1097/00003246-199712000-00008. [DOI] [PubMed] [Google Scholar]
- 18.Kane DA, Thiagarajan RR, Wypij D, Scheurer MA, Fynn-Thomson F, Emani S, et al. Rapid-response extracorporeal membrane oxygenation to support cardiopulmonary resuscitation in children with cardiac disease. Circulation. 2010;122:241–8. doi: 10.1161/CIRCULATIONAHA.109.928390. [DOI] [PubMed] [Google Scholar]
- 19.Huang SC, Wu ET, Wang CC, Chen YS, Chang CI, Chiu IS, et al. Eleven years of experience with extracorporeal cardiopulmonary resuscitation for pediatric patients with in-hospital cardiac arrest. Resuscitation. 2012;83:710–4. doi: 10.1016/j.resuscitation.2012.01.031. [DOI] [PubMed] [Google Scholar]
- 20.Barrett CS, Bratton SL, Salvin JW, Laussen PC, Rycus PT, Thiagarajan RR. Neurological injury after extracorporeal membrane oxygenation use to aid pediatric cardiopulmonary resuscitation. Pediatric Crit Care Med. 2009;10:445–51. doi: 10.1097/PCC.0b013e318198bd85. [DOI] [PubMed] [Google Scholar]
- 21.Hraska V, Ksellman A, Haun C. Patient selection criteria are needed for extracorporeal cardiopulmonary resuscitation following cardiac surgery. Eur J Cardiothorac Surg. 2014;45:276–7. doi: 10.1093/ejcts/ezt361. [DOI] [PubMed] [Google Scholar]
- 22.Tsukahara K, Toida C, Muguruma T. Current experience and limitations of extracorpaoreal cardiopulmonary resuscitation for cardiac arrest in children: a single-center retrospective study. J Intensive care. 2014;2:68. doi: 10.1186/s40560-014-0068-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Erek E, Yalçınbaş YK, Turkekul Y, Saygılı A, Ulukol A, Sarıoğlu A, et al. Indications and risks OD delayed sternal closure after open heart surgery in neonates and early infants. World J Pediatr Congenit Heart Surg. 2012;3:229–35. doi: 10.1177/2150135111432771. [DOI] [PubMed] [Google Scholar]