

Abstract
Nasal columella defects can significantly impair aesthetic appearance. Columella reconstruction can be very challenging for surgeons, especially if due to cocaine abuse. The case of a 32-year-old male patient with subtotal columellar necrosis secondary to cocaine abuse is presented. An inferiorly based philtral advancement flap was performed to cover the defect. Aesthetic outcome was the primary goal of surgery. Reconstruction led to good aesthetic and functional results.
KEY WORDS: Acquired nose deformities, cocaine-related disorders, rhinoplasty, surgical flaps
INTRODUCTION
Cocaine inhalation produces inflammation, ischaemia[1] and apoptosis[2] on the nasal mucosa, besides direct traumatic effect of its crystals. Therefore, chronic abuse causes progressive damage to nasal mucosa and perichondrium resulting in ischaemic necrosis. Damages range from small nasal septum perforation to destruction of entire osteocartilaginous nasal scaffold, sinuses and palate with external deformities.[1]
Depending on cocaine insufflation habits, nasal columella can be significantly exposed to cocaine-induced effects. Columella defects are associated with significant cosmetic and functional deformity. Its reconstruction is considered challenging because of its peculiar structure, limited adjacent skin availability and tenuous vascularity.[3]
We present the case of a successful columellar reconstruction using a philtrum-based subnasale flap in a 32-year-old male patient with severe cocaine-induced deficit of nasal columella associated with nasal septum perforation.
CASE REPORT
A 32-year-old male patient was referred to our department for cocaine-induced nose destruction. We observed a full-thickness defect on nasal columella in its posterior aspect, 1 cm in size, associated with a large, contiguous septal perforation, starting in the membranous septum and extending posteriorly. The columellar septum was partially preserved and covered with normal mucosa. Destruction of inferior and middle turbinates was also observed. Nasal tip projection was still maintained, although the substantial absence of columella support [Figure 1a].
Figure 1.

Nasal columella defect associated with a large, contiguous septal perforation after cocaine-induced nose destruction, in a 32-year-old male patient. Nasal tip projection was preserved. (a) Cosmetic result six months after columella reconstruction with a philtrum-based skin flap. (b) Aesthetic outcome two years after surgical reconstruction in profile (c) and worm’s-eye view (d) Tip projection is preserved; no upper lip protrusion is noticeable
The patient referred 18-month period of total abstinence, and his main complaint was aesthetic appearance, besides moderate and inconsequential nasal obstruction. He was using prosthesis to hide the defect with acceptable cosmetic results [Figure 2]. However, he was strongly motivated to reconstructive surgery and committed to cocaine-free life. He expected a satisfactory aesthetic outcome, at least comparable to his appearance with prosthesis, without taking the chance of evident scarring or bulging.
Figure 2.

Preoperative cosmetic result with columellar prosthesis on
Before planning surgery, we required a 1-year endoscopic follow-up with screening for urinary cocaine metabolites every 3 months to demonstrate long-term abstinence. Thereafter, one-stage reconstruction of columella was performed under general anaesthesia. Incision started in the subnasale region, extending 1 cm downwards to the philtrum. Laterally to the designed flap, we defined and removed two small Burrow's triangles to advance the skin flap [Figures 3 and 4a]. A 1 cm × 1 cm philtrum-based flap was raised and subsequently folded in a hemi-tubular structure to reconstruct posterior aspect of columella; it was harvested on skin only without using any cartilage grafts. Random ascending branches of superior labial arteries provided blood supply. An anterosuperiorly based random mucosal flap dissected from the mucosa covering the remaining portion of columellar septum (the anterior margin of septal perforation) was harvested to complete superiorly the hemi-tubular structure created with the skin flap [Figure 4a]. Anterior margin of the skin flap was sutured to the remaining portion of columellar skin [Figure 4b]. Lateral Burrow's incisions were directly sutured. Sutures were performed using 5-0 Monocryl (Ethicon, Inc., Somerville, NJ, USA). Membranous-cartilaginous septal defect was not reconstructed at the same time. The patient recovered uneventfully with no postoperative complications. Two years after surgery, he showed good aesthetic and functional results; tip projection was preserved and upper lip was not protruding. Cosmetic result was considered satisfactory by both patient and surgeon [Figure 1b–d].
Figure 3.
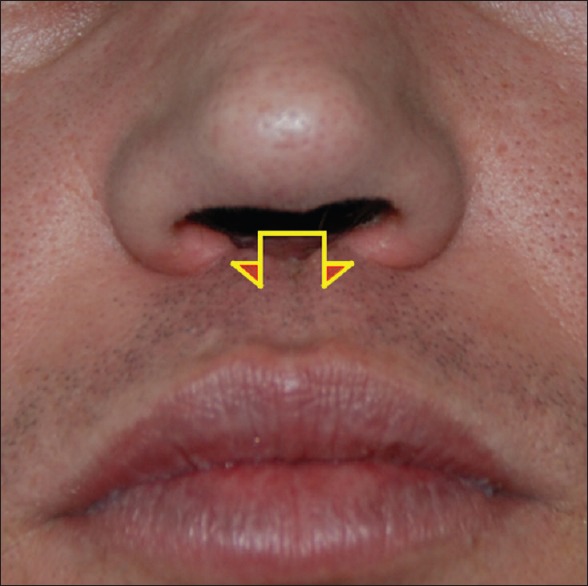
Drawing of the incision lines used to harvest the inferiorly based philtral advancement flap with the two Burrow's triangles excised laterally to the designed flap
Figure 4.
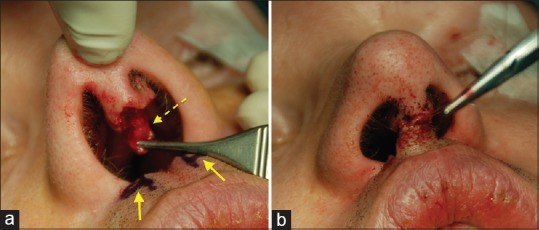
Intraoperative view. Two Burrow's triangles were excised laterally to the designed advancement flap (continuous arrows). A 1 cm × 1 cm philtrum-based advancement skin flap was defined. An anterosuperiorly based random mucosal flap dissected from the mucosa covering the remaining portion of the columellar septum was harvested (dotted arrow). (a) The philtral flap is folded together with the mucosal flap in a tubular structure to reconstruct posterior aspect of columella; anterior margin of the skin flap was then sutured to the remaining portion of columellar skin (b)
DISCUSSION
The nose is a fundamental aesthetic structure: Its defects result in severe aesthetic and functional deformities. Nasal reconstruction is much more complex in cocaine abusers because of mucosal inflammation, ischaemia and apoptosis that could impair tissues healing ability. Timing and extent of surgery must always be planned very carefully when dealing with cocaine-induced defects.
Patient's commitment to cocaine-free life is crucial to long-term surgical success:[4] pre-operative follow-up with a periodical screen for urinary cocaine metabolites becomes mandatory to demonstrate a long period of total abstinence.
Defects of nasal columella can be repaired using skin grafts, composite grafts or several flaps including nasolabial, nasofacial sulcus and forehead ones,[3] depending on the size of defect and concurrent loss of cartilaginous tissue. Ayhan et al.[5] first proposed a classification of columellar defects and reported good results using full-thickness skin grafts or chondrocutaneous grafts when nasal columella was the only nasal subunit involved. More recently Margulis et al.[6] proposed a V-Y flap from the philtrum for reconstruction of partial or subtotal columellar defects. Jung et al.[7] reported 20 cases of subnasale flap for columella reconstruction. For most severe cases, a free radial forearm flap can be used to reconstruct the inner nasal lining,[8] and a free rectus abdominis flap has been proposed for destructive midfacial lesions.[9] Cartilage and bone grafts may be necessary to reconstruct nasal scaffold.[4]
To best of our knowledge, the only report of a columellar reconstruction in a cocaine abuser was proposed by Benito-Ruiz et al.[10] A free flap from the first web space of the foot and a costal cartilage graft were used to reconstruct the deficit. However, this flap seems afflicted by greater morbidity compared to local flaps and its bulk compromises aesthetic outcome.
In this case, we preferred an inferiorly based philtral advancement flap. It has several advantages: it can be elevated from the same visual field of the defect itself, and the shortness of the flap virtually guarantees its survival,[7] especially in cocaine-damaged tissues. This flap also maximises cosmetic results because of its lower morbidity and scarring compared with other flaps. Moreover, it provides perfect colour matching and no subcutaneous unpleasant lump. We did not use a V-Y flap from the philtrum to avoid evident scarring in the midline.
The subnasale flap is generally raised from nasal floor skin[7] to prevent the risk of upper lip protrusion. Since he was a former cocaine abuser, we could not use vestibular skin because of evident scars. We raised a flap from philtrum with same size of the defect: this helped us minimising skin deficit to philtrum itself and not determining upper lip protrusion.
This flap is very easy to harvest, it is based on random blood supply and does not necessarily require a cartilage graft; support to the tip of the nose will be provided by the lateral crura of the alar cartilages.
Nose reconstruction can be very challenging in cocaine abusers due to the collapse of nasal framework. Columellar defects are frequently associated with other nasal subunit deficits, as in cocaine-induced midline destructive lesions.[1] He was presented with a subtotal defect of nasal columella associated with a large, contiguous septal perforation starting in the membranous septum and extending posteriorly. The columellar septum was partially preserved and covered with normal mucosa: this allows us to dissecting a random mucosal flap from the mucosa covering the remaining portion of columellar septum (the anterior margin of septal perforation) and folding it together with the philtral flap in a complete tubular structure. The external appearance of nasal tip and dorsum was not affected. Since patient's main complaint was aesthetic deformity and he referred only moderate nasal obstruction, he firmly refused any major surgical procedures.
We discussed with the patient about a concomitant septal reconstruction. This further procedure would have required a cartilage graft harvested from a distant site and skin/mucosal coverage. However, as well as vestibular skin, nasal mucosa is generally damaged in a cocaine abuser; therefore, nasal mucosal flaps may be less reliable. Other types of reconstruction needed major surgical procedures. The patient informed about the increased morbidity and the possibility of septal reconstruction failure, preferred to limit the procedure to nasal columella reconstruction.
CONCLUSIONS
An inferiorly-based philtral advancement flap can be raised to reconstruct partial or subtotal columellar defects, even if associated with contiguous nasal septum perforation. It allows good aesthetic and functional outcome. There is no need for cartilaginous grafts if nasal tip projection is preserved. This peculiar flap can be chosen in patients with high surgical expectations because of its low morbidity, minimal scarring and easiness of harvesting technique. In cocaine abusers, it can be raised from philtral skin with satisfactory aesthetic results.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Trimarchi M, Bussi M, Sinico RA, Meroni P, Specks U. Cocaine-induced midline destructive lesions – An autoimmune disease? Autoimmun Rev. 2013;12:496–500. doi: 10.1016/j.autrev.2012.08.009. [DOI] [PubMed] [Google Scholar]
- 2.Trimarchi M, Miluzio A, Nicolai P, Morassi ML, Bussi M, Marchisio PC. Massive apoptosis erodes nasal mucosa of cocaine abusers. Am J Rhinol. 2006;20:160–4. [PubMed] [Google Scholar]
- 3.Sherris DA, Fuerstenberg J, Danahey D, Hilger PA. Reconstruction of the nasal columella. Arch Facial Plast Surg. 2002;4:42–6. doi: 10.1001/archfaci.4.1.42. [DOI] [PubMed] [Google Scholar]
- 4.Guyuron B, Afrooz PN. Correction of cocaine-related nasal defects. Plast Reconstr Surg. 2008;121:1015–23. doi: 10.1097/01.prs.0000299464.02430.78. [DOI] [PubMed] [Google Scholar]
- 5.Ayhan M, Sevin A, Aytug Z, Gorgu M, Erdogan B. Reconstruction of congenital and acquired columellar defects: Clinical review of 38 patients. J Craniofac Surg. 2007;18:1500–3. doi: 10.1097/SCS.0b013e318053430b. [DOI] [PubMed] [Google Scholar]
- 6.Margulis A, Icekson M, Billig A, Armon N, Neuman R, Adler N. Practical classification of columellar defects and surgical algorithm for their treatment. J Plast Reconstr Aesthet Surg. 2013;66:577–9. doi: 10.1016/j.bjps.2012.09.037. [DOI] [PubMed] [Google Scholar]
- 7.Jung DH, Lansangan LJ, Choi JM, Jang TY, Lee JJ. Subnasale flap for correction of columellar deformity. Plast Reconstr Surg. 2007;119:885–90. doi: 10.1097/01.prs.0000251997.02810.38. [DOI] [PubMed] [Google Scholar]
- 8.Wehrens KM, Hawinkels H, Fresow RN, van der Hulst RR, Boeckx WD. Reconstruction of the nose after cocaine abuse. J Plast Reconstr Aesthet Surg. 2009;62:532–4. doi: 10.1016/j.bjps.2007.10.021. [DOI] [PubMed] [Google Scholar]
- 9.Caputo G, Fiorino F, Barbieri F, Barisoni D. Mid-face reconstruction with free rectus abdominis flap: Report on a case of chronic cocaine abuse. J Plast Reconstr Aesthet Surg. 2008;61:1107–9. doi: 10.1016/j.bjps.2007.12.061. [DOI] [PubMed] [Google Scholar]
- 10.Benito-Ruiz J, Raigosa M, Yoon TS. Columella reconstruction using a free flap from the first web space of the foot. Ann Plast Surg. 2012;69:279–82. doi: 10.1097/SAP.0b013e31822af8b9. [DOI] [PubMed] [Google Scholar]