

Abstract
Purpose
An innovative methodology using naturalistic driving data was used to examine the association between visual sensory and visual-cognitive function and rates of future crash or near-crash involvement among older drivers.
Methods
The Strategic Highway Research Program (SHRP2) Naturalistic Driving Study was used for this prospective analysis. The sample consisted of N = 659 drivers aged ≥70 years and study participation lasted 1 or 2 years for most participants. Distance and near visual acuity, contrast sensitivity, peripheral vision, visual processing speed, and visuospatial skills were assessed at baseline. Crash and near-crash involvement were based on video recordings and vehicle sensors. Poisson regression models were used to generate crude and adjusted rate ratios (RRs) and 95% confidence intervals, while accounting for person-miles of travel.
Results
After adjustment, severe impairment of the useful field of view (RR = 1.33) was associated with an increased rate of near-crash involvement. Crash, severe crash, and at-fault crash involvement were associated with impaired contrast sensitivity in the worse eye (RRs = 1.38, 1.54, and 1.44, respectively) and far peripheral field loss in both eyes (RRs = 1.74, 2.32, and 1.73, respectively).
Conclusions
Naturalistic driving data suggest that contrast sensitivity in the worse eye and far peripheral field loss in both eyes elevate the rates of crash involvement, and impaired visual processing speed elevates rates of near-crash involvement among older drivers. Naturalistic driving data may ultimately be critical for understanding the relationship between vision and driving safety.
Keywords: naturalistic driving, older drivers, vision, crash, near-crash
Driving is a highly complex task that relies on a variety of visual and cognitive functions.1 A large body of work has demonstrated that older drivers with visual sensory,2–5 visual processing speed,5–7 and visuospatial ability7 impairments are at increased risk for collision involvement. However, most population-based research studies on these risk factors for crash involvement have used accident reports submitted by police agencies to the state office in charge of overseeing these events.2–7 While accident reports provide a wealth of information on the circumstances of the crash (e.g., place, weather, vehicles involved), they may systematically omit less serious crashes, near-misses,8 or any crash event where police do not come to the scene; thus, outcome events are likely incomplete and biased.9 In addition, epidemiologic studies on visual risk factors for collision involvement conducted thus far do not have objectively measured driving exposure (miles driven), but rather rely on subjective driving exposure as reported by the driver.5,10 Research using a naturalistic driving methodology offers an opportunity to overcome these limitations.
Naturalistic driving data are generated by participants driving their own vehicles during the course of their everyday life over long observation periods. Vehicles are unobtrusively equipped with sensors and video cameras, which record vehicle kinematics, GPS, presence of nearby objects, and the roadway environment. These studies are innovative because they provide an unprecedented level of detail on the occurrence of safety critical events such as crashes and near-crashes. Prior studies on vision and driving using naturalistic driving methods have not examined visual risk factors for crash and near-crash events.11–20 Therefore, the purpose of this study was to examine the association between visual sensory and visual-cognitive function and rates of crash or near-crash involvement among older drivers using a naturalistic study design.
Methods
Data Acquisition
This study used data from the Strategic Highway Research Program 2 (SHRP2) Naturalistic Driving Study, the largest naturalistic driving study conducted to date.21 The SHRP2 Naturalistic Driving Study was implemented through the Federal Highway Administration of the US Department of Transportation and the Transportation Research Board.22,23 Virginia Tech Transportation Institute (VTTI; Blacksburg, VA, USA) was the primary contractor for this study.
Study Sample
Details of the SHRP2 purpose, study design, enrollment procedures, and data collection methods have been published previously.22–24 The study involved a sample of drivers from six US sites (Bloomington, IN, USA; State College, PA, USA; Tampa Bay, FL, USA; Buffalo, NY, USA; Durham, NC, USA; Seattle, WA, USA), representing a wide range of geographies, weather, state laws, road types, and road usage. Participants were recruited through a combination of random-digit dialing, random-digit dialing of individuals who were believed to own an eligible vehicle, and public advertising.22 More than 18,000 individuals were recruited for screening.22 Potential participants were contacted by the Virginia Tech Center for Survey Research with a telephone call to discuss the study protocol and confirm eligibility. Individuals who were licensed drivers, drove at least 3 days per week, planned to keep the vehicle for the duration of the study (i.e., 1 or 2 more years for most participants), and had an eligible and mechanically sound vehicle were eligible to participate.22 Consenting and eligible participants completed a standard intake process during a single in-person visit at regional study sites. Participants were enrolled from October 2010 through December 2013 and were followed up over time, most participating 1 to 2 years. The final SHRP2 sample included 3541 drivers aged 16 to 98 years. For the current analysis, the sample was limited to drivers aged ≥70 years (N = 659), since the focus of the study is on older drivers and the rate of crash involvement and older driver fatalities does not markedly begin to increase until the 70s.25,26 This study was approved by the Institutional Review Board at the University of Alabama at Birmingham and followed the tenets of the Declaration of Helsinki.
Data Collection
At the enrollment visit, the personal vehicle of each participant was installed with a data acquisition system (DAS) that captured continuous driving data anytime the vehicle was operating. Participants were instructed to drive their vehicles as they normally would while enrolled in the study. Results from similar naturalistic driving studies demonstrate that participants adapt relatively quickly to the instrumented vehicle, engage in generally normal driving activities, and are not unduly influenced by the equipment installed in their vehicles.27,28 The DAS included four video cameras (forward and rear view, view of the driver's face, and view over the driver's right shoulder) and a suite of vehicle sensors including accelerometers, GPS, and forward radar. At regular intervals, video and sensor data were transmitted from the vehicle to VTTI for data processing and quality control.22 The number of miles driven during each trip was based on the odometer or, if unavailable, other sources (e.g., GPS data).
At enrollment, participants also completed questionnaires on demographic characteristics (e.g., age, sex, ethnicity, race, education), driving history (e.g., self-reported prior crash involvement in previous 3 years), and self-reported medical conditions. Specifically, participants were asked to report any hearing, heart, brain, vascular, nervous system and sleep, respiratory, metabolic, kidney, muscle and movement disorders, cancer, psychiatric conditions, or other medical conditions that may affect their driving. To create an estimate of health status for this analysis,29,30 the number of reported medical conditions was summed and could range from 0 to 12, giving one point for each condition. The clock drawing test was used as a general cognitive screener.31 A score of >2 errors of a possible 6 indicated cognitive impairment.31 The Sensation Seeking Scale survey, previously associated with collision involvement,32 assessed the participant's sensory stimulation preferences, with higher scores indicating a desire for sensation and lower scores reflecting a more cautious predilection. Participants performed a timed rapid pace walk to assess the time needed to walk 10 feet and back; impairment was defined as >7 seconds.33
Visual sensory testing was completed at enrollment by using the Optec 6500 P (Stereo Optical Co., Inc., Chicago, IL, USA).34 Distance and near binocular visual acuity under photopic conditions were recorded as a Snellen fraction and converted to log minimum angle resolvable (logMAR) for the purposes of this analysis. Testing was undertaken with the habitual refractive correction used when driving. Visual acuity impairment for distance or near was defined as >0.3 logMAR (worse than 20/40 acuity). Contrast sensitivity was assessed for each eye separately under photopic conditions (85 cd/m2) for a 6 cycles per degree (cyc/deg) grating, which is near the peak of the contrast sensitivity function.2,3 Contrast sensitivity impairment for each eye was defined as <1.5 log sensitivity.35 If participants were unable to see the target at the highest contrast level (representing a log contrast sensitivity of 1.08), a score of 0.78 was assigned. This was implemented so participants with poor contrast sensitivity were not excluded in the analysis.35 Peripheral vision for each eye was assessed by determining if a participant could detect a small target flashed nasally at 45° and temporally at 55°, 70°, and 85° on the horizontal meridian. Peripheral vision impairment was defined in two ways: as those drivers unable to see the target temporally at 70° or 85° (1) in either eye and (2) in both eyes.
Tests of visual-cognitive function included visual processing speed under divided attention conditions and the visual perception of spatial relationships. Visual processing speed under divided attention was examined by the useful field of view (UFOV) subtest 2.36 Impaired UFOV performance was defined as moderate slowing in visual processing speed of 150 to 350 ms and severe slowing in visual processing speed of >350 ms.7 Visual processing speed under divided attention was also assessed by using the DrivingHealth Inventory37 version of Trails B, a touch screen test that also relies on problem solving, executive function, and working memory.38 Impaired performance on Trails B was defined as scores ≥2.47 minutes.7,39 Spatial ability was assessed by using the DrivingHealth Inventory37 version of the Motor-Free Visual Perception Test (MVPT) Visual Closure Subtest.40 Impaired MVPT performance was defined as fewer than eight cards correct.7
All methods described above for data collection were part of the SHRP2 design. To ensure consistency across the six data collection sites, VTTI provided an in-depth training to site contractor personnel on all study protocols, including the collection of participant functional assessment data and the installation, maintenance, and de-installation of DAS kits. The entire suite of assessments was designed to be precisely replicable across the six data collection sites and to be conducted within a 2-hour window, coinciding with vehicle installation.22
The primary outcomes of interest were crash and near-crash involvement. Crashes were defined as events where the subject vehicle had contact with any object (including other vehicles, pedestrians, cyclists, or animals), at any speed, including nonpremeditated departures from the roadway where at least one tire leaves the paved or intended travel surface of the road. Near-crashes were defined as any circumstance that required a rapid evasive maneuver by the subject vehicle or any other vehicle, pedestrian, cyclist, or animals to avoid a crash. Crash and near-crash events were identified via a variety of means described in detail elsewhere.41 VTTI research staff first performed a Rapid Driver Identification task to identify trip files where the driver was the consenting participant and to remove trip files from nonconsenting drivers.42 Then, trained VTTI analysts reviewed video data when vehicle physical sensors detected (1) large changes in speed or position of the car with respect to the road, (2) activation of advanced safety systems (e.g., antilock braking), (3) the participant pushed the critical incident button to flag an event, or (4) the analysts detected an event.41 A short window of video surrounding the possible event was extracted and reviewed by trained analysts at VTTI to verify and classify as a crash or near-crash event.43 Crash events were further categorized according to the severity of the event, based on the magnitude of the vehicle dynamics, the presumed amount of property damage, knowledge of human injuries (often unknown in this data set), and the level of risk posed to the drivers and other road users. Severity level was coded only for crash events and included (I) severe crashes (i.e., with airbag deployment, injury, rollover, change in velocity, or towing), (II) police-reportable crashes (e.g., includes a minimum of $1500 worth of property damage as estimated from video), (III) minor crashes involving physical contact with another object but with minimal damage, and (IV) low-risk tire strike crashes. The VTTI analysts coding crash and near-crash events were unaware of the participant's status on any variables collected at the enrollment visit. Intrarater agreement on classifying events was periodically assessed with the VTTI analysts. As compared to an expert rater, the overall agreement was 88% for crash and near-crash events.41 If there was more than one sequence in the crash event (e.g., a subject almost rear ends a lead vehicle and then is rear ended by the following vehicle), then the first sequence was defined as a near-crash and the second sequence was defined as a crash. For the purpose of this analysis, a “more severe” approach was used in that the more severe crash between the first and second sequence was used to classify the event as a whole. All crash events included levels I to IV and “major” crash events included levels I to III. At-fault status of the driver was determined by VTTI analysts for crash and near-crash events and was only coded if there was observable evidence in the video that the driver committed an error that led to the event.
Statistical Analysis
Baseline demographic, medical, driving, and behavioral characteristics were compared between those with and without vision impairment. Non–vision-related factors associated with any type of visual impairment were defined as confounders because they may also contribute to crash risk and included age, sex, race, education, number of medical conditions, cognitive impairment status, rapid walk status, sensation-seeking score, and prior motor vehicle collision (MVC) involvement. The time scale for calculation of rates was person-miles, which is a more accurate representation of driving exposure than person-time.44 Poisson regression models were used to generate crude and adjusted rate ratios (RRs) and corresponding 95% confidence intervals (CIs) associated with each visual function and crash involvement, taking into account all crashes a participant incurred. The dispersion of the data was checked to ensure assumptions of Poisson regression were met. Models used a log link function and the log of miles driven was used as an offset. For all analyses, a two-sided P value of <0.05 was considered statistically significant. Models were rerun by using major crashes (levels I–III), at-fault crashes, and near-crash events.
Results
There were 659 adults aged ≥70 years enrolled in SHRP2 (Table 1). Participants included 300 women (45.5%) and 359 men (54.5%). Approximately two-thirds were aged 70 to 79 years and one-third were 80 years and older. Roughly 90% had some college education or more. Most were white (96.3%) and non-Hispanic (98.7%). Approximately 17% of the sample reported prior crash involvement in the previous 3 years. Fifty-four percent had three or fewer medical comorbidities. The mean rapid walk time was 6.39 seconds, ranging from 2.68 to 15.69 seconds. Sensation-seeking scores ranged from 0 to 28 (mean 10.26).
Table 1.
Baseline Characteristics of Older Drivers in SHRP2 (N = 659)
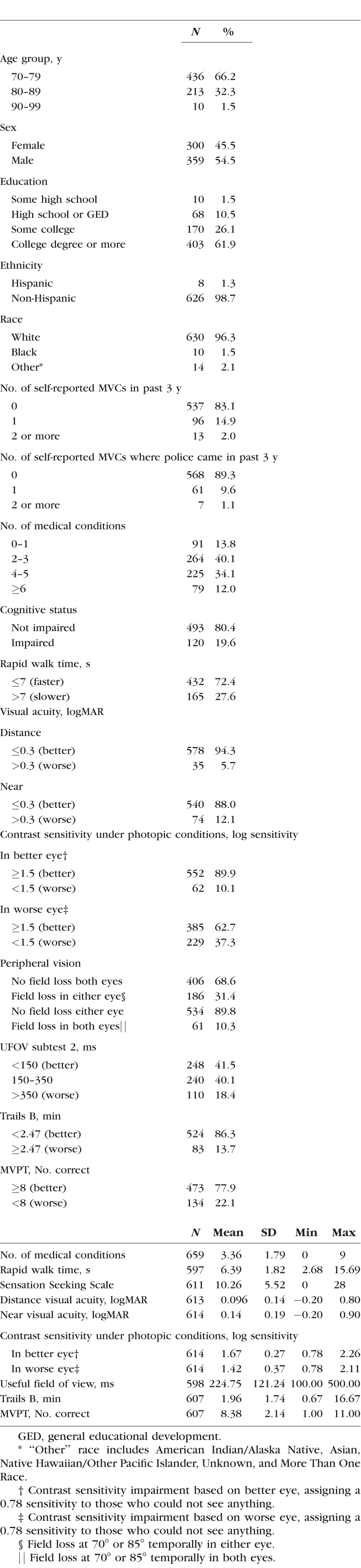
All visual sensory and visual-cognitive measurements were missing for 6.5% (n = 43) of the older drivers. Compared to participants who were missing all vision data, participants with no missing vision data or who were only missing a subset of the vision data were more likely to be male and have higher education. Most drivers in the sample had a distance and near logMAR value ≤ 0.3 (94.3% and 88.0%, respectively, meaning visual acuity of 20/40 or better). Approximately 10% of the sample had contrast sensitivity scores worse than 1.5 when using the better eye and 37% had contrast sensitivity scores worse than 1.5 when using the worse eye. Approximately one-third (31.4%) of the sample had peripheral field loss at 70° or 85° in either eye, whereas only 10% had field loss in both eyes. Visual processing speed per UFOV subtest 2 was slow (>350 ms) in 18.4% of the sample and 13.7% per Trails B. Visual-spatial ability impairment per the MVPT was observed in 22.1%.
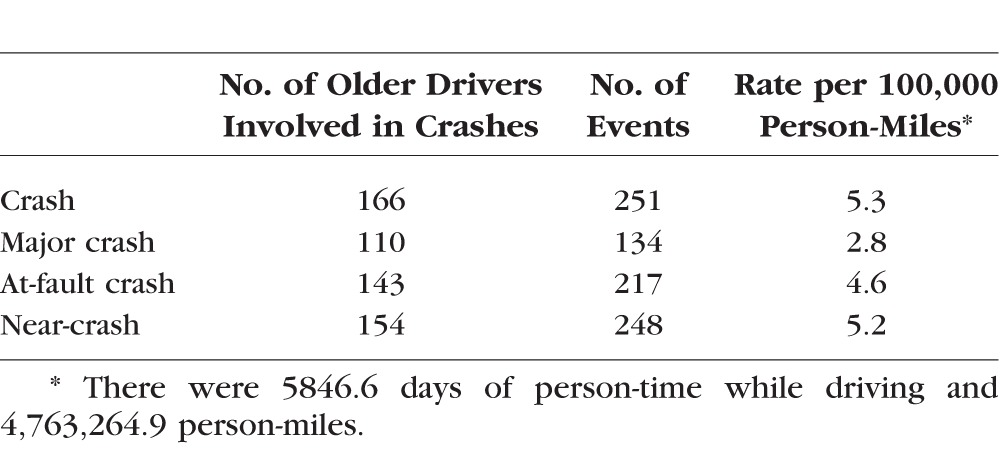
During 4.8 million miles of follow-up over the 3-year study period, approximately one-quarter of older drivers were crash involved (n = 166) (Table 2). Among these drivers, there were 251 crashes for a rate of 5.3 crashes per 100,000 miles traveled. Eighteen crashes were level I severity (most severe), 17 level II, 99 level III, and 117 level IV (least severe). There were 154 older drivers involved in a near-crash. Among these drivers, there were 248 near-crashes for a rate of 5.2 near-crashes per 100,000 miles traveled.
Table 2.
Number and Rates of Crash, Major Crash, At-Fault Crash, and Near-Crash Involvement During the SHRP2 Study (N = 659)
Impaired near and distance visual acuity were not associated with any type of crash or near-crash event (Table 3). Impaired contrast sensitivity in the worse eye, but not the better eye, was associated with higher rates of crash involvement (adjusted RR = 1.38; 95% CI, 1.05–1.81), major crash involvement (adjusted RR = 1.54; 95% CI, 1.07–2.23), and at-fault crash involvement (adjusted RR = 1.44; 95% CI, 1.08–1.93). Since it was possible that the rates of crash involvement depended on the number of eyes with impaired contrast sensitivity, another analysis was examined to compare rates of crash and near-crash involvement among those with neither eye impaired (n = 385) to those with one eye (n = 167) or both eyes (n = 62) impaired. Compared to participants with neither eye impaired, participants with one eye impaired were more likely to have a crash (adjusted RR = 1.39; 95% CI, 1.03–1.88), major crash (adjusted RR = 1.56; 95% CI, 1.04–2.34), and at-fault crash (adjusted RR = 1.44; 95% CI, 1.04–2.00). The RRs were similar when comparing participants with two eyes impaired to neither eye impaired; however, the 95% CIs included 1.0 (data not shown). Peripheral vision impairment in either eye was associated with a higher rate of major crash involvement (adjusted RR = 1.53; 95% CI, 1.02–2.29), whereas peripheral vision impairment in both eyes was associated with an increased rate of crash involvement (adjusted RR = 1.74; 95% CI, 1.18–2.56), major crash involvement (adjusted RR = 2.32; 95% CI, 1.40–3.83), and at-fault crash involvement (adjusted RR = 1.73; 95% CI, 1.14–2.61).
Table 3.
Crude and Adjusted Association Between Vision Impairment and Rates of Any Crash, Major Crash, At-Fault Crash, and Near-Crash Involvement

For those with severe slowing in visual processing speed (>350 ms) per UFOV, crude rates of crash, major crash, and at-fault crash were 1.57 to 2.23 times higher than for those who took less than 150 ms; however, after adjusting, these associations were no longer statistically significant. Severe UFOV impairment was significantly associated with near-crash involvement even after adjusting for potential confounders (adjusted RR = 1.33; 95% CI, 1.19–1.49). Rates of crash and at-fault crash involvement were approximately 40% higher for those with impairment on Trails B; however, these associations were not statistically significant after adjustment. Participants with impaired MVPT scores had significantly lower rates of crash (adjusted RR = 0.59; 95% CI, 0.40–0.88) and at-fault crash (adjusted RR = 0.50; 95% CI, 0.32–0.78) involvement than those without an impairment.
Discussion
The current study implemented a novel approach to studying vision and driver safety in older drivers by using naturalistic driving data, thus avoiding the methodologic pitfalls associated with accident reports that have been routinely used in most previous epidemiologic studies on vision and collision involvement. Additionally, an advantage of the naturalistic driving methodology is that it generates an objective measurement of driving exposure (i.e., miles driven), rather than a subjective self-report measure. Consistent with earlier work,5,45 impaired visual acuity was not associated with crash involvement (regardless of type). Our results go beyond previous studies and suggest that UFOV impairment is associated with near-crash involvement. This may suggest that UFOV impairment places older drivers at risk of performing a rapid evasive maneuver to avoid a crash but without actually inciting any contact with another object, yet little information exists in the literature on risk factors for near-crash involvement to provide context for our finding. Near-crash events (e.g., an aggressive left turn leading to oversteering and causing conflict with oncoming vehicles) may be more reflective of on-road driver performance than driver safety per se.46,47
Contrast sensitivity impairment in the worse eye, but not the better functioning eye, was associated with higher rates of crash, major crash, and at-fault crash involvement even after adjustment for other factors. These results are consistent with prior studies finding that associations between collisions and the worse functioning eye are stronger than that with the better functioning eye.2,3,48,49 For drivers with cataract, Owsley et al.2 have found that contrast sensitivity in the worse eye is more strongly associated with at-fault crash involvement than in the better functioning eye. Similarly, a stronger association with crash involvement for the worse functioning eye has also been found by McGwin et al.50 reporting that visual field loss in the eye with more severe field loss is associated with increased risk of crash involvement. Rubin et al.5 have found that contrast sensitivity impairment is not associated with crash involvement; however, drivers with poor contrast sensitivity are much less likely to drive and are more likely to cease driving during the 8-year follow-up period, and thus by removing themselves from the road, may truncate the study's ability to examine the association between contrast sensitivity and collision involvement. In addition, Rubin et al.5 use a self-reported estimate of miles driven during the year before the baseline examination, unlike the present study that used objectively measured driving exposure.
Drivers with field loss at 70° or 85° in both eyes had rates of crash, major crash, and at-fault crash involvement that were approximately two times higher than those without this field loss. Despite using a single-intensity test target to define field impairment, the magnitude of the association between field loss and crash risk is consistent with prior work using a full-threshold measurement procedure.4 In addition, field loss at 70° or 85° in one eye only was associated with major crash involvement. These field loss findings are consistent with driving performance studies showing that peripheral vision impairment hampers lane positioning and obstacle and pedestrian detection.51–53
The current study found that drivers with slowed visual processing speed as measured by the UFOV subtest 2 were almost two times more likely to incur crash, major crash, at-fault crash, and near-crash events, consistent with previously published rate-ratio estimates.6,7 However, in this study these associations did not remain after adjusting for potentially confounding factors, unlike most previous studies.5–7,45,54,55 Some prior studies reporting associations between UFOV and crash involvement have been based on small samples or convenience samples, whereas a prior study reporting no association is based on a population-based sample of older drivers.56 Interestingly, rates of near-crash involvement remained significantly (69%) higher after adjustment for those with severely impaired UFOV scores. Also unlike other studies,7,56 impaired Trails B was not associated with higher rates of crash involvement regardless of type or with near-crash involvement after adjustment. It is possible the current study adjusted for factors not included in previous studies, yet even when age was the only covariate in the model (data not shown), the association between crash involvement (all types) and UFOV and Trails B performance was not statistically significant. Selection bias may have biased associations toward the null; older adults with functional impairments are less likely to be participants in research.57–59 It seems that this selection bias would be operative for most studies in the older driver literature and not unique to our study. Yet, in studies using naturalistic driving methods there may be a greater predilection for functionally impaired older drivers to decline participation, since their actual on-road behavior will be recorded. Another possible explanation is that the risk factors for crash and near-crash events as defined in naturalistic driving studies may be different from those using accident reports. Prior work suggests crash events defined in different ways can have different visual risk factors.30,60
Our analyses indicated that older drivers with impairments in spatial ability (MVPT test) were less likely to be crash involved or at-fault for a crash, in contrast to previous studies showing a positive7 or no association.56 An explanation remains elusive, although one could speculate that older adults with deficits in their spatial availabilities may be more conservative in where and when they drive. Older adults tend to avoid driving in unfamiliar areas and when visibility is challenging,61–63 a phenomenon that could be accentuated in those with challenges in processing spatial information.
The percentage of participants who incurred at least one crash (25%) was much higher in this study than studies using accident reports generated by the police.5 Minor collisions are not always reported to the police, which may account for this difference. Severity level I or II crashes in the SHRP2 classification system are those that would most likely be police reported22; and 5.3% of the participants in our analysis had these types of crashes.5 This is comparable to the 6.7% of participants with crashes in the prospective population-based study by Rubin et al.5 In addition, given the number of miles traveled, the rate of crashes coded with a severity level I or II was 0.73 per 100,000 person-miles, which is only slightly higher than population-based studies based on police-reported accidents.64 These estimates provide some external validity to the SHRP2 estimates as compared to other population-based samples of a similar age group.
The results of this study must be interpreted in light of strengths and limitations. A major strength was that this is the first large-scale multisite study using naturalistic driving methodology to examine the association between visual function and crash risk in older drivers. The assessment of crash involvement was based on video recordings and vehicle sensors, so it was not subject to recall bias or limited to only police-reported crashes. In SHRP2 identification of a crash or near-crash event is predicated on the assumption that the vehicle sensors detected it. It is certainly possible that not all crash or near-crash events were detected by the sensor algorithms and thus not included in this analysis; however, a systematic approach was used to identify events so it is likely any missing events were similar between those with and without vision impairment. At-fault status was determined by trained analysts at VTTI who evaluated video recordings of the actual crash event. Unlike police who arrive at the scene after the crash event and thus did not witness it, the analyst can watch the video of the event. Driving exposure was measured objectively from the vehicle, so it is not subject to recall bias like self-reported annual mileage. While the Optec 6500 P instrument may be amenable to use in a motor vehicle licensing setting, it does not have design characteristics for visual acuity and other psychophysical testing that are preferable for clinical eye research,65 so the results may not be generalizable to vision assessments administered in more controlled settings. Nevertheless, the reliability of the instrument is high35 and visual functions were assessed at the beginning of the study, so there is little reason to suspect misclassification bias. However, it is possible vision status may have changed between enrollment and the end of follow-up and would have biased the estimates toward the null. Crashes were defined prospectively and trained analysts were masked to the visual function status of the participant at baseline, so there is little reason to suspect differential bias between those who did and did not crash. The sample was largely white non-Hispanic and highly educated, so the generalizability to other race/ethnicities or populations with lower educational attainment is unknown, a topic for further study. This study adjusted for a number of important nonvisual confounding factors known to affect crash risk in older drivers, a strength of the study design. The role of many other contrast sensitivity test conditions measured in SHRP2 as related to collision involvement by older drivers was not addressed in this report, but will be the subject of a future report. Adjustment for multiple comparisons was not performed. Adjusting for multiple comparisons can result in a higher type II error rate by artificially setting the bar for statistical significance very high.66–68 While it is more conservative than the conventional P < 0.05, applying adjustment factors hampers researchers from exploring an association further. Instead future research should investigate these statistical associations to see if the pattern persists in other large naturalistic driving studies that have assessed visual function among older drivers.69
In conclusion, this naturalistic driving study afforded the opportunity to study the relationship between vision and driving in older drivers where outcome events are not limited by the accident report surveillance submitted by police officers and driver self-reports of driving exposure (mileage). Findings suggest that older drivers with impaired contrast sensitivity in the worse eye and far peripheral vision in both eyes have significantly higher rates of crash involvement than those without these impairments. In addition, impaired UFOV was associated with higher rates of near-crash involvement. The differing results between the current study and prior studies using accident reports may be derived from how an adverse crash event is defined. Research using naturalistic driving methods is relatively new, but may ultimately be critical for understanding the veridical relationship between vision and driving safety.
Acknowledgments
Supported by National Institutes of Health (NIH) Grants R21EY027817, R01EY018966, P30AG22838, P30EY003039, EyeSight Foundation of Alabama, and Research to Prevent Blindness.
Disclosure: C. Huisingh, None; E.B. Levitan, None; M.R. Irvin, None; P. MacLennan, None; V. Wadley, None; C. Owsley, None
References
- 1. Anstey KJ,, Horswill MS,, Wood JM,, Hatherly C. The role of cognitive and visual abilities as predictors in the Multifactorial Model of Driving Safety. Accid Anal Prev. 2012; 45: 766–774. [DOI] [PubMed] [Google Scholar]
- 2. Owsley C,, Stalvey B,, Wells J,, Sloane M,, McGwin G. Visual risk factors for crash involvement in older drivers with cataract. Arch Ophthalmol. 2001; 119: 881–887. [DOI] [PubMed] [Google Scholar]
- 3. Green KA,, McGwin G,, Owsley C. Associations between visual, hearing, and dual sensory impairments and history of motor vehicle collision involvement of older drivers. J Am Geriatr Soc. 2013; 61: 252–257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Huisingh C,, McGwin G,, Wood JM,, Owsley C. The driving visual field and a history of motor vehicle collision involvement in older drivers: a population-based examination. Invest Ophthalmol Vis Sci. 2015; 56: 132–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Rubin G,, Ng E,, Bandeen-Roche K,, et al. A prospective, population-based study of the role of visual impairment in motor vehicle crashes among older drivers: the SEE study. Invest Ophthalmol Vis Sci. 2007; 48: 1483–1491. [DOI] [PubMed] [Google Scholar]
- 6. Owsley C,, Ball K,, McGwin G,, et al. Visual processing impairment and risk of motor vehicle crash among older adults. JAMA. 1998; 279: 1083–1088. [DOI] [PubMed] [Google Scholar]
- 7. Ball K,, Roenker D,, Wadley V,, et al. Can high-risk older drivers be identified through performance-based measures in a department of motor vehicles setting? J Am Geriatr Soc. 2006; 54: 77–84. [DOI] [PubMed] [Google Scholar]
- 8. Owsley C,, McGwin G., Jr. Vision and driving. Vision Res. 2010; 50: 2348–2361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Owsley C,, Wood JM,, McGwin G., Jr. A roadmap for interpreting the literature on vision and driving. Surv Ophthalmol. 2015; 60: 250–262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Owsley C,, Stalvey B,, Wells J,, Sloane ME. Older drivers and cataract: driving habits and crash risk. J Gerontol A Biol Sci Med Sci. 1999; 54A: M203–M211. [DOI] [PubMed] [Google Scholar]
- 11. Charlton JL,, Catchlove M,, Scully M,, Koppel S,, Newstead S. Older driver distraction: a naturalistic study of behaviour at intersections. Accid Anal Prev. 2013; 58: 271–278. [DOI] [PubMed] [Google Scholar]
- 12. Liang Y,, Lee JD,, Yekhshatyan L. How dangerous is looking away from the road: algorithms predict crash risk from glance patterns in naturalistic driving. Hum Factors. 2012; 54: 1104–1116. [DOI] [PubMed] [Google Scholar]
- 13. Munro CA,, Jefferys J,, Gower EW,, et al. Predictors of lane-change errors in older drivers. J Am Geriatr Soc. 2010; 58: 457–464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. West SK,, Hahn DV,, Baldwin KC,, et al. Older drivers and failure to stop at red lights. J Gerontol A Biol Sci Med Sci. 2010; 65: 179–183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Wong J-T,, Huang S-H. Attention allocation patterns in naturalistic driving. Accid Anal Prev. 2013; 58: 140–147. [DOI] [PubMed] [Google Scholar]
- 16. Agramunt S,, Meuleners L,, Chow KC,, Ng JQ,, Morlet N. A validation study comparing self-reported travel diaries and objective data obtained from in-vehicle monitoring devices in older drivers with bilateral cataract [published online ahead of print October 25, 2016] Accid Anal Prev. doi:10.1016/j.aap.2016.10.021. [DOI] [PubMed] [Google Scholar]
- 17. Chevalier A,, Chevalier AJ,, Clarke E,, et al. Naturalistic rapid deceleration data: drivers aged 75 years and older. Data Brief. 2016; 9: 909–916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Chevalier A,, Coxon K,, Chevalier AJ,, et al. Predictors of older drivers' involvement in rapid deceleration events. Accid Anal Prev. 2017; 98: 312–319. [DOI] [PubMed] [Google Scholar]
- 19. Fitch GM,, Bartholomew PR,, Hanowski RJ,, Perez MA. Drivers' visual behavior when using handheld and hands-free cell phones. J Safety Res. 2015; 54: 105–108. [DOI] [PubMed] [Google Scholar]
- 20. Morando A,, Victor T,, Dozza M. Drivers anticipate lead-vehicle conflicts during automated longitudinal control: sensory cues capture driver attention and promote appropriate and timely responses. Accid Anal Prev. 2016; 97: 206–219. [DOI] [PubMed] [Google Scholar]
- 21. Transportation Research Board of the National Academies of Science. Virginia Tech Transportation Institute. The 2nd strategic highway research program naturalistic driving study insight dataset. Available at: https://insight.shrp2nds.us/home. Accessed April 11, 2016. [Google Scholar]
- 22. Dingus T,, Hankey J,, Antin J,, et al. Naturalistic Driving Study: Technical Coordination and Quality Control. Washington, DC: Transportation Research Board; 2015. S2-S06-RW-1. [Google Scholar]
- 23. Antin J,, Lee S,, Hankey J,, Dingus T. Design of the In-Vehicle Driving Behavior and Crash Risk Study. Washington, DC: Transportation Research Board; 2011. S2-S05-RR-1. [Google Scholar]
- 24. Committee for the Strategic Highway Research Program 2: Implementation. Implementing the Results of the Second Strategic Highway Research Program: Saving Lives, Reducing Congestion, and Improving Quality of Life. Washington, DC: US Department of Transportation; 2009. Special report 296. [Google Scholar]
- 25. National Highway Traffic and Safety Administration. Addressing the Safety Issues Related to Younger and Older Driver—A Report to Congress. Washington, DC: US Department of Transportation; 1993. [Google Scholar]
- 26. Cicchino JB,, McCartt AT. Trends in older driver crash involvement rates and survivability in the United States: an update. Accid Anal Prev. 2014; 72: 44–54. [DOI] [PubMed] [Google Scholar]
- 27. Stutts J,, Feaganes J,, Reinfurt D,, et al. Driver's exposure to distractions in their natural driving environment. Accid Anal Prev. 2005; 37: 1093–1101. [DOI] [PubMed] [Google Scholar]
- 28. Dingus T,, Klauer S,, Neale V,, et al. The 100-Car Naturalistic Driving Study, Phase II: Results of the 100-Car Field Experiment. Washington, DC: Department of Transportation, National Highway Traffic Safety Administration; 2006. [Google Scholar]
- 29. Owsley C,, McGwin G,, Searcey K. A population-based examination of the visual and ophthalmological characteristics of licensed drivers aged 70 and older. J Gerontol A Biol Sci Med Sci. 2013; 68: 567–573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Owsley C,, McGwin G, Jr,, Ball K. Vision impairment, eye disease, and injurious motor vehicle crashes in the elderly. Ophthalmic Epidemiol. 1998; 5: 101–113. [DOI] [PubMed] [Google Scholar]
- 31. Shulman KI,, Shedletsky R,, Silver IL. The challenge of time: clock-drawing and cognitive function in the elderly. Int J Geriatr Psychiatry. 1986; 1: 135–140. [Google Scholar]
- 32. Jonah BA. Sensation seeking and risky driving: a review and synthesis of the literature. Accid Anal Prev. 1997; 29: 651–665. [DOI] [PubMed] [Google Scholar]
- 33. Marottoli R,, Cooney L,, Wagner R,, Doucette J,, Tinetti M. Predictors of automobile crashes and moving violations among elderly drivers. Ann Intern Med. 1994; 121: 842–846. [DOI] [PubMed] [Google Scholar]
- 34. Stereo Optical Co., Inc. Reference and Instruction Manual Optec 6500 Vision Tester. Chicago, IL: Stereo Optical Co., Inc.; 2004. [Google Scholar]
- 35. Hohberger B,, Laemmer R,, Adler W,, Juenemann AG,, Horn FK. Measuring contrast sensitivity in normal subjects with OPTEC 6500: influence of age and glare. Graefes Arch Clin Exp Ophthalmol. 2007; 245: 1805–1814. [DOI] [PubMed] [Google Scholar]
- 36. Edwards J,, Ross L,, Wadley V,, et al. The useful field of view test: normative data for older adults. Arch Clin Neuropsychol. 2006; 21: 275–286. [DOI] [PubMed] [Google Scholar]
- 37. Staplin L,, Lococo K,, Gish K,, Decina L. Model Driver Screening and Evaluation Program Final Technical Report. Washington, DC: National Highway Traffic Safety Administration; 2003. DOT HS 809 582. [Google Scholar]
- 38. Reitan RM. The relationship of the Trail Making Test to organic brain damage. J Consult Psychol. 1955; 19: 393–394. [DOI] [PubMed] [Google Scholar]
- 39. Goode K,, Ball K,, Sloane M,, et al. Useful field of view and other neurocognitive indicators of crash risk in older adults. J Clin Psychol Med Settings. 1998; 5: 425–440. [Google Scholar]
- 40. Colarusso R,, Hammill D. Motor-Free Visual Perception Test. Los Angeles: Western Psychological Services; 1972. [Google Scholar]
- 41. Hankey JM,, Perez MA,, McClafferty J. Description of the SHRP2 Naturalistic Database and the Crash, Near-Crash, and Baseline Datasets. Blacksburg, VA: Virginia Tech Transportation Institute; 2016. [Google Scholar]
- 42. McClafferty J,, Perez MA,, Hankey JM. Identification of Consented Driver Trips in the SHRP2 Naturalistic Driving Study Data Set. Blacksburg, VA: Virginia Tech Transportation Institute; 2015. [Google Scholar]
- 43. Virginia Tech Transportation Institute. SHRP2 Researcher Dictionary for Safety Critical Event Video Reduction Data. Version 4.1. Blacksburg, VA: Virginia Tech Transportation Institute; 2015. [Google Scholar]
- 44. Chipman ML,, MacGregor CG,, Smiley AM,, Lee-Gosselin M. The role of exposure in comparisons of crash risk among different drivers and driving environments. Accid Anal Prev. 1993; 25: 207–211. [DOI] [PubMed] [Google Scholar]
- 45. Cross JM,, McGwin G,, Rubin GS,, et al. Visual and medical risk factors for motor vehicle collision involvement among older drivers. Br J Ophthalmol. 2009; 93: 400–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Higgins KE,, Wood J,, Tait A. Vision and driving: selective effect of optical blur on different driving tasks. Hum Factors. 1998; 40: 224–232. [DOI] [PubMed] [Google Scholar]
- 47. Higgins KE,, Wood JM. Predicting components of closed road driving performance from vision tests. Optom Vis Sci. 2005; 82: 647–656. [DOI] [PubMed] [Google Scholar]
- 48. Owsley C. Vision and driving in the elderly. Optom Vis Sci. 1994; 71: 727–735. [DOI] [PubMed] [Google Scholar]
- 49. Sims RV,, Owsley C,, Allman RM,, Ball K,, Smoot TM. A preliminary assessment of the medical and functional factors associated with vehicle crashes by older adults. J Am Geriatr Soc. 1998; 46: 556–561. [DOI] [PubMed] [Google Scholar]
- 50. McGwin G,, Xie A,, Mays A,, et al. Visual field defects and the risk of motor vehicle collisions among patients with glaucoma. Invest Ophthalmol Vis Sci. 2005; 46: 4437–4441. [DOI] [PubMed] [Google Scholar]
- 51. Wood JM,, Troutbeck RJ. Effect of restriction of the binocular visual field on driving performance. Ophthalmic Physiol Opt. 1992; 12: 291–298. [PubMed] [Google Scholar]
- 52. Haymes SA,, LeBlanc RP,, Nicolela MT,, Chiasson LA,, Chauhan BC. Glaucoma and on-road driving performance. Invest Ophthalmol Vis Sci. 2008; 49: 3035–3041. [DOI] [PubMed] [Google Scholar]
- 53. Bowers A,, Peli E,, Elgin J,, McGwin G, Jr,, Owsley C. On-road driving with moderate visual field loss. Optom Vis Sci. 2005; 82: 657–667. [DOI] [PubMed] [Google Scholar]
- 54. Owsley C,, Ball K,, Sloane M,, Roenker D,, Bruni J. Visual/cognitive correlates of vehicle accidents in older drivers. Psychol Aging. 1991; 6: 403–415. [DOI] [PubMed] [Google Scholar]
- 55. Ball K,, Owsley C,, Sloane M,, Roenker D,, Bruni J. Visual attention problems as a predictor of vehicle crashes in older drivers. Invest Ophthalmol Vis Sci. 1993; 34: 3110–3123. [PubMed] [Google Scholar]
- 56. Friedman C,, McGwin G,, Ball K,, Owsley C. Association between higher order visual processing abilities and a history of motor vehicle collision involvement by drivers ages 70 and over. Invest Ophthalmol Vis Sci. 2013; 54: 778–782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Norton MC,, Breitner J,, Welsh KA,, Wyse BW. Characteristics of nonresponders in a community survey of the elderly. J Am Geriatr Soc. 1994; 42: 1252–1256. [DOI] [PubMed] [Google Scholar]
- 58. Hébert R,, Bravo G,, Korner-Bitensky N,, Voyer L. Refusal and information bias associated with postal questionnaires and face-to-face interviews in very elderly subjects. J Clin Epidemiol. 1996; 49: 373–381. [DOI] [PubMed] [Google Scholar]
- 59. Launer LJ,, Wind AW,, Deeg DJ. Nonresponse pattern and bias in a community-based cross-sectional study of cognitive functioning among the elderly. Am J Epidemiol. 1994; 139: 803–812. [DOI] [PubMed] [Google Scholar]
- 60. McGwin G,, Owsley C,, Ball K. Identifying crash involvement among older drivers: agreement between self-report and state records. Accid Anal Prev. 1998; 30: 781–791. [DOI] [PubMed] [Google Scholar]
- 61. Freeman EE,, Muñoz B,, Turano KA,, West SK. Measures of visual function and their association with driving modification in older adults. Invest Ophthalmol Vis Sci. 2006; 47: 514–520. [DOI] [PubMed] [Google Scholar]
- 62. Ball K,, Owsley C,, Stalvey B,, et al. Driving avoidance and functional impairment in older drivers. Accid Anal Prev. 1998; 30: 313–322. [DOI] [PubMed] [Google Scholar]
- 63. Lyman J,, McGwin G,, Sims R. Factors related to driving difficulty and habits in older drivers. Accid Anal Prev. 2001; 33: 413–421. [DOI] [PubMed] [Google Scholar]
- 64. Blunck H,, Owsley C,, MacLennan P,, McGwin G. Driving with pets as a risk factor for motor vehicle collisions among older drivers. Accid Anal Prev. 2013; 58: 70–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Ferris FL,, Kassoff A,, Bresnick GH,, Bailey I. New visual acuity charts for clinical research. Am J Ophthalmol. 1982; 94: 91–96. [PubMed] [Google Scholar]
- 66. Savitz DA,, Olshan AF. Multiple comparisons and related issues in the interpretation of epidemiologic data. Am J Epidemiol. 1995; 142: 904–908. [DOI] [PubMed] [Google Scholar]
- 67. Rothman KJ. No adjustments are needed for multiple comparisons. Epidemiology. 1990; 1: 43–46. [PubMed] [Google Scholar]
- 68. Huisingh C,, McGwin G. An analysis of the use of multiple comparison corrections in ophthalmology research. Invest Ophthalmol Vis Sci. 2012; 53: 4777–4777. [DOI] [PubMed] [Google Scholar]
- 69. Council of Deputy Ministers Responsible for Transportation and Highway Safety. Canada Naturalistic Driving Study (CNDS). 2017. Available at: http://www.canada-nds.net/index.html. Accessed June 6, 2017. [Google Scholar]