

Abstract
INTRODUCTION:
Shoulder dystocia is one of the obstetric emergencies that are accompanied to serious risks for mother and fetus. It necessitates making the method of training of shoulder dystocia management more efficient, i.e., better management and giving services with higher quality. Thus, this study was carried out to compare the impact of training by simulation and oral technique on the skill of the employed midwives in obstetric clinics at Mashhad city (Iran) in shoulder dystocia management during 2012.
METHODS:
The current research is a double-group clinical trial that was conducted on 51 members of the employed midwives in the obstetric clinic at Mashhad city in 2012. The questionnaire of personal specification and awareness about shoulder dystocia and practical examination (objective-structured clinical examination) were employed as tools for data collection. The learners were divided into two groups by randomized allocation. Training was done by the presentation of lecture in the oral content group and a short movie was displayed at the end of it. The shoulder dystocia management technique was simulated in another group and through role-playing of instructor application of moulage (station) training was conducted. The period of the training course (4 h) and content of the educational workshop was identical for both groups. The practical examination was held for the learners before and immediately after training course. The given data were analyzed by means of statistical descriptive tests including Mann–Whitney U-test and Wilcoxon test via SPSS software (version 16). The significance level was considered as (P < 0.05) in all cases.
RESULTS:
The total mean score was significantly increased for the variable of shoulder dystocia management skill after intervention in both groups (P < 0.0001). Similarly, the results of Mann–Whitney U-test statistical tests indicated that total mean score for the variable of shoulder dystocia management skill after the intervention was significantly greater in simulation group than in an oral group (P = 0.040).
CONCLUSION:
Training in simulated delivery room by means of role-playing is an efficient method for training shoulder dystocia management skill, so it is recommended to use this program in the training of this skill.
Keywords: Midwife, role-playing, shoulder dystocia, simulation, training
Introduction
Shoulder dystocia is one of the unpredictable midwifery urgencies that occur in about 2% of deliveries[1] and it is followed by some maternal side-effects, postobstetric hemorrhage, uterine atony, vaginal rupture and neonatal encephalopathic hypoxic-ischemic side symptoms, clavicle bone fracture, ribs, humerus bone, and permanent trauma in brachial bundle of nerves.[2,3] The trauma in brachial bundle of nerves is most morbid lesion of shoulder dystocia (4–40%);[4] that in more than a half of cases it takes place due to inappropriate management of shoulder dystocia.[5] The results of studies indicate that mismanagement of shoulder dystocia is due to low level of self-confidence and poor skill of obstetrician operators. The midwife is the obstetric operator in 45% of cases for morbidity of shoulder dystocia.[6]
The proper and prompt decision-making and appropriate clinical performance are some part of the necessary skills for the midwife.[7] Similarly, taking suitable measures for care and therapy depends on knowledge and practice of midwife.[8] Therefore, quality of midwifery training may deeply affect on presentation of above skills and the efficient education may lead to improvement of the quality of midwifery services and increase in efficiency and effectiveness in cares and productivity in healthcare medical system.[8,9] Thus, making effort to improve the quality of midwifery training may play a determinant role in the health of the community, quality of care, and reduced the related rates of morbidity and mortality to shoulder dystocia[6] while achieving this objective definitely requires a comprehensive educational system.[10] Nowadays, education and training course is presented mainly by traditional method and via lecture (oral) technique by the teacher in this country. The educational aids are less used in oral training, and the amount of available information is much higher than potential and capability of the learner. The learners lack the experience of training in an active learning environment, and they acquire their skill on a real patient after passing their theoretical lessons.[11,12] Genarally, in training oral method of shoulder dystocia management the real environment and clinical presence of the patient is the first opportunity for the learner to use his/her scientific memorized knowledge to manage shoulder dystocia.[2,13] As a result, they lack adequate clinical skills and readiness to encounter the unexpected problems.[14,15] Thus, employing the alternate educational techniques and utilization from the methods by which the learner can personally acquire the knowledge and skill is necessary. Adaptation of educational techniques based on personal learning may have the highest and foremost impact in their learning[14,16] including simulation that is one of the methods based on personal learning. Through providing the conditions similar to real world situation, simulation technique puts the opportunity for exercise and repetition at learner's disposal.[2,13] Likewise, training by simulation technique leads to increase self-confidence and facilitates acquisition of the needed capability and reduces time of training.[16] Nevertheless, so far there is no reliable and adequate information regarding the impacts of training by means of simulation method.[17,18] Based on the results of study carried out by Goffman et al. to determine skill of gynecology and midwifery residents in shoulder dystocia management using simulation technique, those residents who had been trained by this educational method had significantly higher scores in terms of time of intervention for removal of dystocia, conducting maneuvers, and general practice.[13] The results of the study that was carried out by Comeau and Craig (2014) showed that simulation training technique might not improve the quality of reporting shoulder dystocia.[19] With respect to necessity of midwife's skill for prediction and favorable shoulder dystocia management as well as given qualitative studies which have been reported in this field and their findings contradicted to the results of this investigation the present research was carried out to compare two educational methods including by simulated and oral techniques and their effect on skill of midwives that are employed in obstetric center at Mashhad city and in shoulder dystocia management in 2012.
Methods
This study of clinical trial was conducted with two groups on 54 members of the employed midwives in obstetric centers at Mashhad city after receiving the permission from Ethics Committee of Mashhad University of Medical Sciences in 2012. The sample size was estimated using means formula at 99% level of confidence and test power (99%) in any group as 24 participants so that given exclusion of 10% of that sample this size was considered 27 participant in any group. Two participants in oral group and one member in simulated group were excluded from study during this study because they did not participate in posttest. Primarily for sampling, the educational workshop was held by expressing target group and day for holding this course in which the researchers were the scientific secretaries of that workshop and it was recorded in permanent educational system and midwives enrolled in it via system. Then, based on available method of sampling and inclusion criteria, the qualified samples were divided by means of randomized allocation and using lottery technique into two simulated and oral training groups in 1st and 2nd days, respectively. The inclusion criteria of the study comprised consent to participate in research; having at least BA degree in midwifery and the exclusion criteria from study consisted of nonparticipation in all educational phases or examinations of the given course; experience in exposure to shoulder dystocia during studied period; occurrence of inadvertent accidents during holding educational sessions and course examinations. Personal specifications questionnaire, awareness inventory about shoulder dystocia management, and practical examination (objective-structured clinical examination) were tools for data collection to evaluate skill in shoulder dystocia management, and also consent form of educational course and the related practical exam.
Personal specifications questionnaire included some questions about age, marital status, educational degree, working experience in clinical field and attendance in shoulder dystocia management workshops and the awareness inventory consisted of 15 questions regarding theoretical contents about shoulder dystocia. The practical test (objective-structured clinical examination) included assessment of shoulder dystocia management maneuvers and the related communicational skills. Evaluation of shoulder dystocia management maneuvers comprised four items and assessment of skill consisted of six items. The lowest acquired score from any item was considered as zero and the highest score was 1 for any item so that the minimum total score was zero and the maximum total score was deemed as 10. The checklist of observation of practical test (objective-structured clinical examination) was designed according to World Health Organization checklist concerning prophylaxis and control of shoulder dystocia and important guidelines of national guidance instructions for presentation of midwifery and obstetrics services in mother-friendly hospital and based on the consensus of the relevant academic teachers. Validity of questionnaires and practical test observation checklist (objective-structured clinical examination) was evaluated using content-validity method and reliability of observation checklist for objective-structured clinical examination and awareness inventory was confirmed through determination of internal consistency via., Cronbach alpha coefficient respectively as α = 0.82 and α = 0.78.
Similarly, the rate of consent from educational course and practical examination in this study was evaluated according to Likert 5-scale spectrum based on choices ranged from strongly agree[5] to strongly disagree.[1] This is a standardized form and former sources and studies have been used to prepare it. It should be noted that the day before holding workshop, the examiners played the related roles along with midwifery instructor for coordination and proper execution of role in the simulated obstetric room to exercise the needed skills and their competency in role-playing and evaluation was confirmed.
Then, the researcher initially explained about the goal and method of study and dealt with acquiring informed consent from qualified midwives in this study during both days of holding workshop after attendance in study site. Afterward, the personal specifications questionnaire and awareness inventory about shoulder dystocia management were completed by the studied units and they passed a pretest practical examination (objective-structured clinical examination) regarding shoulder dystocia management. The studied sample was initially entered in the simulated obstetric room at clinical skills center during pretest and the simulated scenario was put at their disposal. This scenario included history of a woman during delivery (age: 35, 90 min during exercise for delivery, an hour abnormal glucose concentration test). A midwifery student play the role that she was playing role of a woman during delivery in half-seat status on gynecological bed while she was upset and sought for help and moulage with fetus was placed in front of her and an obstetrician assistant directed shoulders of fetus by a strip fastened around the neck of fetus. The research unit should continue delivery process (exit of shoulders) and notice shoulder dystocia in exposure to delivery from shoulder and manage it during 5 min. In the case of achievement in practice by the midwife in shoulder dystocia successful management and exiting of shoulders, and or passing through this process more than 5 min to exit shoulders, and or confession of the given midwife to lack of her ability to manage dystocia, the examination was stopped. Midwife's skills for existing shoulder and her communication skills were assessed according to observation checklist by examiner. Likewise, one person as midwife and two other persons as gynecologist and pediatrician attended in the simulated obstetric room where they assisted the midwife if she asked them for help. Training course started for 4 h after assessment (simulated training in 1st day and oral training in 2nd day). After the end of training session, the training consent form was filled out by the research units and posttest was also administered after the end of training. The educational contents were presented to oral training group by means of lecture along with power-point software and then the training movie was played that was published by college of gynecologists and midwifery (about 10 min) and the last 1/2 h of training session was devoted to question and answer (total training period: 4 h). The training consent form was completed by the studied units at the end of training session and they also passed posttest at the end of training session.
Initially, a synopsis of educational content was presented by short lecture (1/2 h) in simulated training group at clinical skills center and then management of this technique was executed in a simulated obstetric room by researcher on moulage station and explained simultaneously. Similarly, the needed communication skills for management of dystocia were trained through role-playing of researcher (the responsible individual for delivery) with other persons that played roles of delivery subject, midwife, obstetrician, and pediatrician specialists. Afterward, midwives exercised in a simulated environment and received the needed feedback from the instructor (total training period: 4 h). After the end of training session, the training consent form was completed by the studied units. The training content was the same in both groups and it was prepared according to national guiding instruction for presentation of midwifery and obstetric services in mother-friendly hospitals [Figure 1].
Figure 1.
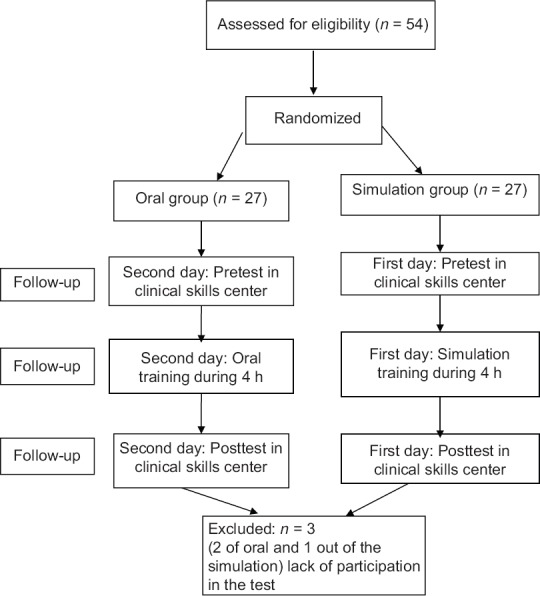
CONSORT flow chart of participants
Both groups passed posttest similar to pretest immediately after training. Similarly, the training consent form was filled out by the studied units after the end of posttest. The results of post- and pre-test in two groups were analyzed by means of accurate statistical test of Fisher, t-test, Mann–Whitney U-test and Wilcoxon test using SPSS (version 16 IBM Company, Armonk, NY, U.S.A) software. The significance level was considered as P < 0.05 in all cases.
Results
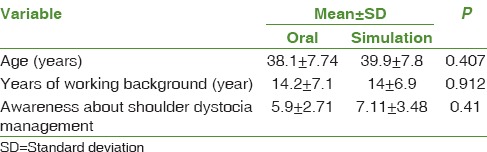
Two groups were homogeneous in terms of mean and standard deviation, age, working background in clinical field and awareness about shoulder dystocia management [Table 1]. The majority of studied units had BA degree in midwifery and only 7.2% of them in simulated training group and about 4.2% of them in oral training group had MA degree in midwifery. The results of Fisher's accurate test indicated that both groups were homogenous in terms of this variable (P = 0.756). About 93.8% of the studied units had no background for participation in shoulder dystocia management training workshop.
Table 1.
Distribution frequency in the research units based on age and working background in obstetric center and awareness about shoulder dystocia management in both simulated and oral training groups
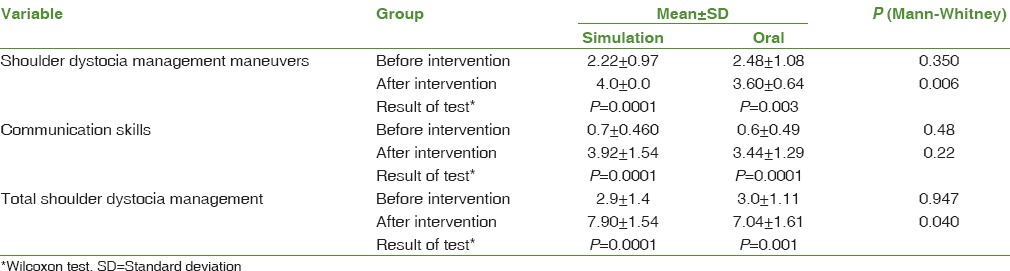
The total mean score of variable of shoulder dystocia management skill after intervention was increased significantly in both groups (P < 0.0001). Similarly, the results of statistical Mann–Whitney U-test group showed in comparison between two groups that the postintervention total mean score was significantly higher in the simulated training group than oral training group (P = 0.040).
The mean score for evaluation of shoulder dystocia management maneuvers after intervention had been significantly increased in both groups. Likewise, regarding inter-group comparison, the results of statistical Mann–Whitney U-test indicated that the mean score of evaluation of shoulder dystocia management of postintervention maneuvers was significantly greater in the simulated training group than in oral training group (P = 0.006).
The mean score for variable of shoulder dystocia communication skill in both groups was significantly increased after intervention (P < 0.0001), but there was no statistical significant difference between two groups (P = 0.22) [Table 2].
Table 2.
Mean and standard deviation for score of evaluation of shoulder dystocia management maneuvers, communication skills for shoulder dystocia management in the research units before and after intervention in two simulated and oral training groups
Likewise, the mean scores of variable of postintervention awareness in the simulated and oral training groups were 13.44 ± 1.79 and 11.55 ± 1.81 respectively where there was significant difference among two groups (P = 0.042).
The mean score for variable of consent from training had no statistical significant among two simulated and oral training groups (P < 0.05) and the midwives evaluated training course very positively. One hundred percentage of midwives agreed and strongly agreed with training course.
Discussion
The findings of this study showed that both training methods (simulation and oral) might increase skill of midwife in shoulder dystocia management but midwife's skill in shoulder dystocia management in the simulated training group has been greater than in the oral training group. Reynolds et al. conducted a study in order to determine the effect of the simulated training technique on shoulder dystocia management on 63 midwifery students in Portugal. The results indicated that the shoulder dystocia management was significantly higher in the simulated training group than in oral training group.[20] The results of study done by Crofts et al. (2006) showed that training on mannequin might lead to improvement of shoulder dystocia management and also it reduced time interval among exiting of head and shoulder as well as pressure on head for exit[6] so that this finding is consistent with the results of the present study. Training leads to improvement of skill, thinking potential, rising capability for design, and execution of care plans.[21] There are undeniable evidences that similar to delivery management and its relevant processes, training of practical skills causes increasing mental readiness and pervasive capability in doing clinical measures properly in exposure to emergency and real situations.[22] On the other hand, similar to simulation, presentation of training by means of active training techniques and based on personal experiences of learners may increase performance and skill remarkably.[11] One can refer to application of question and answer as the factors for efficiency of oral training in the present study. Question and answer may activate mind and lead to active training in the learners.[23] The communication skills in shoulder dystocia management after intervention were significantly increased in both training methods (simulation and oral) in the present study but there was no significant difference between mean scores of communication skills in shoulder dystocia management in both simulated and oral training groups.
The results of study carried out by Deering et al. on 33 female residents in USA showed that the simulated training might significantly increased communication skills in shoulder dystocia management compared to control group 2 weeks after training.[2] The reason for this difference of this finding from the results of present study may be due to difference in time interval among pretraining and posttest. Posttest was done 2 weeks after training in Daring's investigation but in the present study posttest was held immediately after the end of training course. However, change in mental dimension might be created immediately after intervention but these changes may not endure and they may approach to the previous level before training during subsequent follow-up processes.[24,25]
Based on principles for learning adults, creation of opportunity and allowing students to employ and execute their learned contents and knowledge in a clinical situation and showing that in which fields their knowledge and skill may be defective can create strong drive for learning[26] and it is recommended to adapt more active educational methods in training the students and also it is suggested to implement some studies to determine the impact of the simulated training technique on retention of skill for shoulder dystocia management. One of the constraints in this research was implementation of this study on the employed midwives in public sectors.
Conclusion
The results of this study indicated that training increased shoulder dystocia management skill in midwives. This improvement of skill was further in simulated training group than in oral training group. Therefore, it is obvious that application of more efficient training techniques and improving training level in midwives may lead to upgrading process of presentation of healthcare services and enhancement and increase in giving services to mothers and their neonates and this will cause improvement of health level among mothers and newborns and enhancement of health indices.
Financial support and sponsorship
Mashhad University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This study is part of a research proposal approved by the Mashhad University of Medical Sciences with Code No. 89914 which was performed with financial support of the Research Council of the University. This research is registered in the Iranian Registry of Clinical Trials with the IRCT2015081410661N4 code. We are greatly thankful for participants, the testers, Women's Health Research Center, and respected staff of Mashhad Nursing and Midwifery school.
References
- 1.Crofts JF, Fox R, Ellis D, Winter C, Hinshaw K, Draycott TJ. Observations from 450 shoulder dystocia simulations: Lessons for skills training. Obstet Gynecol. 2008;112:906–12. doi: 10.1097/AOG.0b013e3181865f55. [DOI] [PubMed] [Google Scholar]
- 2.Deering S, Poggi S, Macedonia C, Gherman R, Satin AJ. Improving resident competency in the management of shoulder dystocia with simulation training. Obstet Gynecol. 2004;103:1224–8. doi: 10.1097/01.AOG.0000126816.98387.1c. [DOI] [PubMed] [Google Scholar]
- 3.Cuningham FG, Leveno KJ, Bloom SL, Hauth JC, Rouse DJ, Spong CY. Williams Obstetrics. New York: McGrawhill; 2010. [Google Scholar]
- 4.Dajani NK, Magann EF. Complications of shoulder dystocia. Semin Perinatol. 2014;38:201–4. doi: 10.1053/j.semperi.2014.04.005. [DOI] [PubMed] [Google Scholar]
- 5.McFarland MB, Langer O, Piper JM, Berkus MD. Perinatal outcome and the type and number of maneuvers in shoulder dystocia. Int J Gynaecol Obstet. 1996;55:219–24. doi: 10.1016/s0020-7292(96)02766-x. [DOI] [PubMed] [Google Scholar]
- 6.Crofts JF, Bartlett C, Ellis D, Hunt LP, Fox R, Draycott TJ. Training for shoulder dystocia: A trial of simulation using low-fidelity and high-fidelity mannequins. Obstet Gynecol. 2006;108:1477–85. doi: 10.1097/01.AOG.0000246801.45977.c8. [DOI] [PubMed] [Google Scholar]
- 7.Ramezani M, Kermanshahi S. A survey of the quality of clinical education in nursing. Jahrom Med J. 2011;9:9–12. [Google Scholar]
- 8.Rahimikian F, Mirmolaei T, Samizadeh Z, Shirazi M, Mehran A. Evaluation of knowledge and practice of newly graduated midwives in normal vaginal delivery in hospitals affiliated to Tehran university of medical sciences. Iran J Med Educ. 2007;7:51–7. [Google Scholar]
- 9.Modares M, Mirmolaee ST, Mirmohammadalie M, Valizadeh MA, Ziyaee M, Hashemi FA. The Effects of Education on the Use of Partogram to Control the Quality of Care Offered by Midwives. Research Journal of Biological Sciences. 2009;4:152. [Google Scholar]
- 10.Borotis S, Poulymenakou A. E-learning readiness components: Key issues to consider before adopting e-learning interventions. In: Nall J, Robson R, editors. Proceedings of World Conference on, E-Learning in Corporate G, Healthcare, and Higher Education. Chesapeake, VA: AACE; 2004. pp. 1622–9. [Google Scholar]
- 11.Erfanian F, Khadivzadeh T, Khadem N, Khajedelooie M. The effect of teaching by role playing on students’ counseling and screening skills toward IUD clients. Iranian J Med Educ 2008. 2009;8:275–83. [Google Scholar]
- 12.Kordi M, Rashidi Fakari F, Mazloum SR, Khadivzadeh T, Akhlaghi F. Comparison between the efficacy of web-based, simulation and conventional training on knowledge and skills retention of midwifery students in management of postpartum hemorrhage. Iran J Obstet Gyneocol Infertil. 2014;16:8–14. [Google Scholar]
- 13.Goffman D, Heo H, Chazotte C, Merkatz IR, Bernstein PS. Using simulation training to improve shoulder dystocia documentation. Obstet Gynecol. 2008;112:1284–7. doi: 10.1097/AOG.0b013e31818c177b. [DOI] [PubMed] [Google Scholar]
- 14.Blue AV, Stratton TD, Plymale M, DeGnore LT, Schwartz RW, Sloan DA. The effectiveness of the structured clinical instruction module. Am J Surg. 1998;176:67–70. doi: 10.1016/s0002-9610(98)00109-3. [DOI] [PubMed] [Google Scholar]
- 15.Kooiker CH, Scutchfield FD. Barriers to prescribing the Copper T 380A intrauterine device by physicians. West J Med. 1990;153:279–82. [PMC free article] [PubMed] [Google Scholar]
- 16.Hamilton R. Nurses’ knowledge and skill retention following cardiopulmonary resuscitation training: A review of the literature. J Adv Nurs. 2005;51:288–97. doi: 10.1111/j.1365-2648.2005.03491.x. [DOI] [PubMed] [Google Scholar]
- 17.Issenberg SB, McGaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ. Features and uses of high-fidelity medical simulations that lead to effective learning: A BEME systematic review. Med Teach. 2005;27:10–28. doi: 10.1080/01421590500046924. [DOI] [PubMed] [Google Scholar]
- 18.Gaba DM. The future vision of simulation in health care. Qual Saf Health Care. 2004;13(Suppl 1):i2–10. doi: 10.1136/qshc.2004.009878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Comeau R, Craig C. Does teaching of documentation of shoulder dystocia delivery through simulation result in improved documentation in real life? J Obstet Gynaecol Can. 2014;36:258–65. doi: 10.1016/S1701-2163(15)30635-6. [DOI] [PubMed] [Google Scholar]
- 20.Reynolds A, Ayres-de-Campos D, Pereira-Cavaleiro A, Ferreira-Bastos L. Simulation for teaching normal delivery and shoulder dystocia to midwives in training. Educ Health (Abingdon) 2010;23:405. [PubMed] [Google Scholar]
- 21.Amini A, Hassanzadeh Salmasi S, Shaghaghi A, Safaii N, Sedaghat K. The effect of clinical skills training on medical students clinical competencies in the management of vaginal delivery. Iran J Med Educ. 2005;5:7–12. [Google Scholar]
- 22.Sharemi H, Asgari F. A training course on basic gynecological clinical skills and its effect on medical student's performance in Guilan university of medical sciences. Iran J Med Educ. 2011;11:111–9. [Google Scholar]
- 23.Woolliscroft JO. Medical student clinical education. International Handbook of Research in Medical Education. Springer Netherlands. 2002:365–80. [Google Scholar]
- 24.Craik FI, Lockhart RS. Levels of processing: A framework for memory research. J Verbal Learning Verbal Behav. 1972;11:671–84. [Google Scholar]
- 25.Petty RE, Cacioppo JT. Attitudes and Persuasion: Classic and Contemporary Approaches. Dubuque Westview Press. 1981 [Google Scholar]
- 26.Rochester S, Kilstoff K, Scott G. Learning from success: Improving undergraduate education through understanding the capabilities of successful nurse graduates. Nurse Educ Today. 2005;25:181–8. doi: 10.1016/j.nedt.2004.12.002. [DOI] [PubMed] [Google Scholar]