

Abstract
Background and Aims:
Bispectral index (BIS) values may be anaesthetic agent-specific, depending on their ability to suppress the electroencephalogram (EEG) signals. We carried out a prospective, randomised clinical trial to study the effect of nitrous oxide (N2O) on the BIS values at an equi-minimum alveolar concentration (MAC) of sevoflurane and desflurane.
Methods:
Sixty adult patients undergoing spine surgery were randomised into two groups; Group S (sevoflurane; n = 30) and Group D (desflurane; n = 30) for the maintenance of anaesthesia in oxygen and air or oxygen and N2O mixture (FiO2-0.4) (Stage 1). BIS and fraction of inspired and end-tidal concentration of agents were noted at 1.0 MAC. In Stage 2, air or N2O was discontinued and the other carrier gas was introduced. At steady state of this carrier gas, values were again noted as in Stage 1. Statistical analysis was performed using two-way analysis of variance followed by Bonferroni correction, and Student's t-test for paired data. P<0.05 was considered statistically significant.
Results:
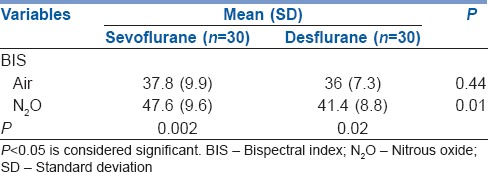
With air-oxygen as the carrier gas, sevoflurane and desflurane resulted in comparable BIS values (P = 0.44). With addition of 60% N2O, there was a significant increase in BIS values at 1.0 MAC for both the agents. Furthermore, higher BIS values were observed with sevoflurane compared to desflurane (P = 0.01).
Conclusion:
Sevoflurane and desflurane at equi-MAC concentration exert similar effect on BIS values when used with air-oxygen. N2O results in higher BIS values; this effect is more pronounced in combination with sevoflurane.
Keywords: Bispectral index, desflurane, minimum alveolar concentration, nitrous oxide, sevoflurane
INTRODUCTION
Minimum alveolar concentration (MAC) is a measure of potency of inhalational anaesthetics. Therefore, equi-MAC concentrations of different anaesthetics should have a similar potency in suppressing responses to painful stimuli. Bispectral index (BIS) is an EEG-derived value that indicates the degree of hypnosis under anaesthesia. Based on this EEG-derived index, the same value should indicate the same level of unconsciousness for all anaesthetics. However, it is not true as different anaesthetic agents affect the EEG to a variable extent. Earlier studies have shown that BIS values at equi-MAC concentrations of different agents are not similar.[1,2,3,4] BIS values may be drug specific depending on the ability of the anaesthetic to suppress the EEG signals.
Sevoflurane and desflurane are commonly used inhalational agents preferred for their early awakening characteristic. Their effect on EEG is more or less similar when used at 1 MAC level in combination with oxygen and air.[5] At higher MACs, desflurane may significantly suppress EEG activity, whereas sevoflurane may be associated with spike activity. Nitrous oxide (N2O) when added to volatile agent decreases MAC requirement of inhalational anaesthetics. It also suppresses low-frequency EEG power thus enhancing higher-frequency EEG activity which may interfere with EEG monitoring parameters.[6] Hence, due to the variable effect of N2O on EEG, its presence can also affect BIS, thereby increasing the value of this index. BIS values <40 indicate a deep hypnotic level and is associated with increased mortality and morbidity.[7] Hence, it is essential to know the BIS values of commonly used agents at equi-MAC concentrations. Comparison of equi-MAC BIS values of desflurane and sevoflurane, both in the absence and presence of N2O, has not been studied yet. We carried out a prospective, randomised clinical trial to study the effect of N2O on the BIS values at an equi-MAC dose (1 MAC) of sevoflurane and desflurane during the maintenance phase of general anaesthesia.
METHODS
After approval was obtained from the Institute's Ethics Committee and informed consent from the patient, sixty adult patients (American Society of Anesthesiologists physical status I or II), aged 18–60 years, undergoing spine surgery were enrolled for this study. Exclusion criteria included patients with body weight more than 20% of ideal body weight, patients on hypnotics and antidepressants, patients addicted to alcohol, patients with cardiac diseases and neurologic disorders and those receiving β-blocker drugs. In the operation room (OR), monitoring of electrocardiogram, pulse-oximetry and non-invasive blood pressure was started. Age of the patient was entered in monitor to obtain accurate age-corrected MAC values. The disposable BIS sensor (BIS Quatro, Covidien, USA) was applied on the right forehead of the patient after skin preparation in accordance with the manufacturer's instruction and connected to the BIS monitor. General anaesthesia was induced with fentanyl 2 μg/kg and propofol 1.5–2 mg/kg. Tracheal intubation was facilitated with rocuronium 1 mg/kg. A nasopharyngeal probe was placed for temperature monitoring. Mechanical ventilation was adjusted to maintain end-tidal carbon dioxide concentration between 34 and 36 mmHg. Intermittent boluses of fentanyl 1 μg/kg and rocuronium 0.05 mg/kg were administered for maintenance of anaesthesia. Baseline heart rate (HR) and mean arterial blood pressure (MAP) were recorded along with BIS value before induction of general anaesthesia. The patients were randomised on the basis of computer-generated randomisation chart and allocated to groups using sequentially arranged, opaque, sealed envelope technique. Patients received either sevoflurane (Group S; n = 30) or desflurane (Group D; n = 30) for the maintenance of anaesthesia in oxygen and air or oxygen and N2O mixture (FiO2-0.4) (Stage 1). The sequence of carrier gases was also randomised on the basis of computer-generated randomisation table. A constant fresh gas flow of 3 L/min (higher flow rate for achieving MAC rapidly) was maintained throughout the study period. The surgery was allowed to start before recording of data. The HR, MAP, BIS, fractions of inspired and end-tidal concentration of agent were noted at 1.0 MAC, every minute for 5 min and then a mean of these five readings was obtained and noted. End-tidal concentration of the gases was monitored on the standard monitor available in the OR. A steady state of 10 min was allowed at target MAC concentration before data were recorded, to ensure equilibration of the anaesthetic to the brain. The primary objective of the study was to observe any difference in BIS values at equi-MAC values of two inhalational anaesthetics. Blood pressure was increased with bolus injection of mephentermine sulphate if value decreased by 20% from the initial MAP. In Stage 2, air or N2O was discontinued and the other carrier gas was introduced. At steady state of second carrier gas, values were again noted as in Stage 1, keeping the MAC of volatile agent constant at 1.0 MAC.
Based on a previous published study,[3] for detecting a difference of five points in the BIS values between the study groups, a sample size of thirty patients per group was required for the study to have power of 90% (β = 0.10) at a confidence interval limits (α = 0.05). Data were analysed using software STATA 9.0 (College Station, TX, USA). Data were expressed as mean (standard deviation). Age, body weight and sex of patients and the baseline values of HR, MAP and BIS in the two groups were compared by two-way analysis of variance followed by Bonferroni correction. At 1.0 MAC fractions of each volatile agent, the parameters tabulated during air/oxygen were compared with those during N2O/oxygen using Student's t-test for all paired data. The P < 0.05 was considered statistically significant.
RESULTS
All patients completed the study and none were excluded from the final analysis. The demographic characteristic and values of HR and MAP were comparable between both the groups [Tables 1 and 2]. The inspired end-tidal values of sevoflurane and desflurane with or without N2O varied in both the groups so as to achieve 1.0 MAC [Table 2]. With air-oxygen as the carrier gas, sevoflurane and desflurane resulted in comparable BIS values (Group S = 37.8 ± 9.9 vs. Group D = 36 ± 7.3 [P = 0.44]) [Table 3]. With addition of 60% N2O, there was significant increase in BIS values at 1.0 MAC for both sevoflurane and desflurane. We also noted a difference in the BIS values when compared between groups at 1.0 MAC with higher BIS values in sevoflurane group (Group S = 47.6 ± 9.6 vs. Group D = 41.4 ± 8.8 [P = 0.01]) [Table 3].
Table 1.
Demographic characters of the patients
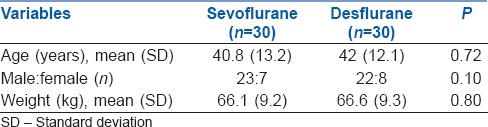
Table 2.
Physiologic data during the study period
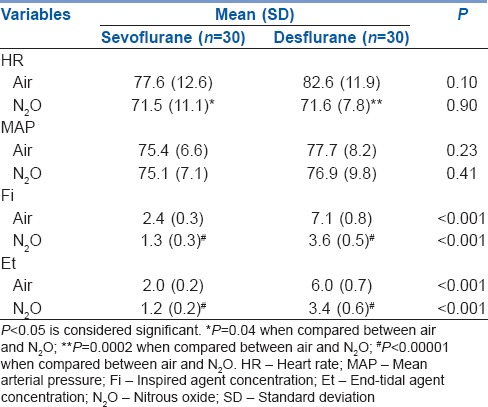
Table 3.
Bispectral index values at 1 minimum alveolar concentration of volatile anaesthetics, in presence and absence of nitrous oxide
DISCUSSION
In our study, when N2O was added as a carrier gas, we noted a statistically significant difference in BIS values between the two agents at equi-MAC concentration. N2O resulted in higher BIS values and this effect was more pronounced when used in combination with sevoflurane. This effect can also be due to the greater hypnotic effect of desflurane than sevoflurane during equipotent anaesthesia.[4] We also noted that with addition of N2O, BIS values increased in both sevoflurane and desflurane groups at 1.0 MAC concentrations. However, we did not observe such difference when air was used as carrier gas. With addition of N2O, the overall requirement of inhalational anaesthetics also decreases. Therefore, higher BIS values seen in the N2O group can be the combined effect of the decrease in the suppressant effect of these inhalational anaesthetic agents on EEG, along with a higher frequency EEG activity produced by N2O.
Different inhalational anaesthetic agents produce dissimilar BIS values at an equal depth of anaesthesia. BIS values were measured at equi-MAC concentration of halothane and isoflurane in 34 patients undergoing spinal surgery. The authors found that at any given MAC concentration, BIS values were significantly lower under isoflurane compared to halothane anaesthesia.[1] This effect can be explained by different action of inhalational anaesthetic agents on EEG. In another study, the authors found that desflurane produced a greater hypnotic effect than sevoflurane during equipotent anaesthesia.[4] The authors found that BIS values recorded were significantly lower in the desflurane group than the sevoflurane group. However, in our study, when we compared the effect of sevoflurane and desflurane on BIS values, we found them to be comparable at equi-MAC concentrations in both groups when air was used as a carrier gas.
Desflurane produces a dose-dependent increase in HR. Unlike in desflurane/N2O group, raised HR in desflurane/air group can possibly be due to the higher anaesthetic agent required to attain 1.0 MAC. As the MAC value of both agents is different (sevoflurane - 1.8, desflurane - 6.6), the Fi required for achieving equi-MAC concentration will also be different [Table 1]. Similarly, the difference between the inspired and end-tidal values of two agents can also be explained due to the second gas effect exerted by N2O [Table 1].
N2O when used as a carrier gas during maintenance of anaesthesia also affects the EEG activity and therefore the BIS value. Administration of N2O to healthy young adult volunteers resulted in increase in high-frequency and θ-range activity of the EEG, but it did not alter BIS value.[8] On the contrary, in another study, authors observed that BIS was higher when isoflurane was used in combination with N2O than when it was used without N2O.[9] Similar effect was also observed in an another study, where entropy values increased with addition of N2O to 1.0 MAC isoflurane and sevoflurane. This raises the possibility of misinterpretation of anaesthetic hypnosis.[3] Notably, N2O significantly modulates EEG activity when used in conjunction with other volatile anaesthetic agents, resulting in higher frequency EEG activity.
BIS values for inhaled anaesthetics are agent specific and administration of inhaled anaesthetics based on equi-MAC values can result in an unnecessarily long duration of deep hypnosis during anaesthesia and possible neurotoxic effects in vulnerable patients. The increase in BIS values with addition of N2O in this study is probably related to the neurostimulant properties of N2O. BIS Vista monitor has demonstrated good correlation and high discriminative power in depicting a mean cerebral flow velocities decline that can serve as an indicator of decline in cerebral activity during cross-clamping of aorta.[10] It is also well demonstrated in literature that inhalation of N2O can increase cerebral flow velocities coupled to rise in cerebral consumption of oxygen (CMRO2). These effects possibly could justify the increase in BIS values during the addition of N2O.
Our data support that at equi-MAC concentrations of various anaesthetic agents; BIS values differ. Hence, MAC specifies the ability of an agent to cause immobility during surgery and poorly correlates with the degree of hypnosis caused by the same agent. Anaesthetic agents variably affect the spinal mechanisms of immobility and cerebral mechanisms of hypnosis.[11] This may be responsible for difference in BIS values observed between agents at equi-MAC concentrations. The change though statistically significant may not be clinically significant as BIS was within the acceptable range of depth of anaesthesia. The results of this study reiterate that BIS values should be interpreted with caution depending on the type of anaesthetic agents used.
CONCLUSION
Sevoflurane and desflurane at equi-MAC concentration exert similar effect on BIS values when used in conjunction with air. N2O results in higher BIS values and this effect is more pronounced when used in combination with sevoflurane.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Umamaheswara Rao GS, Ali Z, Ramamoorthy M, Patil J. Equi-MAC concentrations of halothane and isoflurane do not produce similar bispectral index values. J Neurosurg Anesthesiol. 2007;19:93–6. doi: 10.1097/ANA.0b013e31803062f9. [DOI] [PubMed] [Google Scholar]
- 2.Schwab HS, Seeberger MD, Eger EI, 2nd, Kindler CH, Filipovic M. Sevoflurane decreases bispectral index values more than does halothane at equal MAC multiples. Anesth Analg. 2004;99:1723–7. doi: 10.1213/01.ANE.0000136467.47996.70. [DOI] [PubMed] [Google Scholar]
- 3.Prabhakar H, Ali Z, Bithal PK, Singh GP, Laithangbam PK, Dash HH. EEG entropy values during isoflurane, sevoflurane and halothane anesthesia with and without nitrous oxide. J Neurosurg Anesthesiol. 2009;21:108–11. doi: 10.1097/ANA.0b013e318192d60e. [DOI] [PubMed] [Google Scholar]
- 4.Kim JK, Kim DK, Lee MJ. Relationship of bispectral index to minimum alveolar concentration during isoflurane, sevoflurane or desflurane anaesthesia. J Int Med Res. 2014;42:130–7. doi: 10.1177/0300060513505525. [DOI] [PubMed] [Google Scholar]
- 5.Purdon PL, Sampson A, Pavone KJ, Brown EN. Clinical electroencephalography for anesthesiologists: Part I: Background and basic signatures. Anesthesiology. 2015;123:937–60. doi: 10.1097/ALN.0000000000000841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Foster BL, Liley DT. Nitrous oxide paradoxically modulates slow electroencephalogram oscillations: Implications for anesthesia monitoring. Anesth Analg. 2011;113:758–65. doi: 10.1213/ANE.0b013e318227b688. [DOI] [PubMed] [Google Scholar]
- 7.Leslie K, Myles PS, Forbes A, Chan MT. The effect of bispectral index monitoring on long-term survival in the B-aware trial. Anesth Analg. 2010;110:816–22. doi: 10.1213/ANE.0b013e3181c3bfb2. [DOI] [PubMed] [Google Scholar]
- 8.Rampil IJ, Kim JS, Lenhardt R, Negishi C, Sessler DI. Bispectral EEG index during nitrous oxide administration. Anesthesiology. 1998;89:671–7. doi: 10.1097/00000542-199809000-00017. [DOI] [PubMed] [Google Scholar]
- 9.Sebel PS, Lang E, Rampil IJ, White PF, Cork R, Jopling M, et al. A multicenter study of bispectral electroencephalogram analysis for monitoring anesthetic effect. Anesth Analg. 1997;84:891–9. doi: 10.1097/00000539-199704000-00035. [DOI] [PubMed] [Google Scholar]
- 10.Dahaba AA, Xue JX, Hua Y, Liu QH, Xu GX, Liu YM, et al. The utility of using the bispectral index-Vista for detecting cross-clamping decline in cerebral blood flow velocity. Neurosurgery. 2010;67(3 Suppl Operative: ons102-7) doi: 10.1227/01.NEU.0000383152.50183.81. [DOI] [PubMed] [Google Scholar]
- 11.Jinks SL, Martin JT, Carstens E, Jung SW, Antognini JF. Peri-MAC depression of a nociceptive withdrawal reflex is accompanied by reduced dorsal horn activity with halothane but not isoflurane. Anesthesiology. 2003;98:1128–38. doi: 10.1097/00000542-200305000-00015. [DOI] [PubMed] [Google Scholar]