

Abstract
Background and Aims:
Confirmation of correct endotracheal tube placement is essential immediately after intubation for general anaesthesia. In this study, we have compared upper airway ultrasonography (USG) with reference to capnography for rapid confirmation of endotracheal tube placement after general anaesthesia.
Methods:
A prospective, single centre, observational study was conducted on 100 patients requiring tracheal intubation for general anaesthesia. Both capnography and upper airway USG were performed immediately after intubation to confirm the endotracheal tube (ETT) placement. Sensitivity, specificity, and positive and negative predictive values of upper airway USG were determined against capnography as the reference method. Agreement between the methods and time required to determine ETT placement by the two methods were assessed with kappa statistics and Student's t-test.
Results:
Upper airway USG detected all five cases of oesophageal intubation, but could not detect five patients with correct tracheal intubation. Upper airway USG had a sensitivity of 96.84% (95% confidence interval [CI]: 94.25%–96.84%), specificity of 100% (95% CI: 50.6%–100%), positive predictive value of 100% (95% CI: 97.3%–100%) and negative predictive value of 62.5% (95% CI: 31.6%–62.5%). Kappa value was found to be 0.76, indicating a good agreement between upper airway USG and capnography for confirmation of ETT placement. Time taken for confirmation of ETT by capnography was 8.989 ± 1.043 s vs. 12.0 ± 1.318 s for upper airway USG (P < 0.001).
Conclusion:
Both capnography and upper airway USG may be used as primary procedures for the confirmation of ETT placement.
Keywords: Capnography, general anaesthesia, tracheal intubation, upper airway ultrasonography
INTRODUCTION
In operation theatre settings, tracheal intubation is generally performed to maintain and protect the airway during general anaesthesia. Confirmation of correct endotracheal tube (ETT) placement is essential immediately after intubation. Failure to diagnose oesophageal intubation can be disastrous. The incidence of oesophageal intubation was reported at 6% in emergency conditions and 1.75% in the elective setting.[1] Oesophageal intubation is one of the main causes of accidents leading to death or neurologic damage. An investigation of anaesthesia mortality revealed that 69% of the deaths were related to airway management, with oesophageal intubation as one of the contributing factors.[2] Direct visualisation of the ETT passing through the glottis is often applied in practice, but it is not always possible, especially if laryngoscopy is difficult. The alternative methods of confirmation include auscultation, observation of chest movements, observation of condensation in the ETT, and increasing heart rate. None of these indirect methods have been proven to be fully reliable, especially under emergency conditions. End-tidal carbon dioxide (ETCO2) is the gold standard for identifying oesophageal intubation. Capnography has also been found to be the best method for rapid assessment of ETT position.[3] Capnography has 100% sensitivity and 100% specificity in verifying the correct ETT location which shows that waveform capnography can be considered as the standard method for the primary verification of ETT location.[4] Several studies of upper airway ultrasonography (USG) confirmation of ETT position provided promising results in a cadaver model or in patients under controlled operating room conditions.[5,6,7] In this prospective, observational study, we have compared upper airway USG with reference to capnography (the gold standard method) for rapid confirmation of endotracheal tube placement after general anaesthesia.
METHODS
A prospective, single centre, observational study was conducted on 100 patients who required intubation for general anaesthesia during elective and emergency surgeries, after approval of the scientific and ethics committee. Informed consent was taken from all the participants before enrolment. Patients with anatomic neck distortion, American Society of Anesthesiologists Grades 4, 5, limited neck extension, history of difficult tracheal intubation, abnormal airway anatomy (e.g., Mallampati class of 4, thyromental distance <6 cm, inter-incisor gap <3 cm, cervical spine disease), high risk of aspiration and severe cardiac, pulmonary, hepatic, renal or coagulative disease were excluded from the study.
A single sonographer (researcher) identified all intubations. The sonographer was an anaesthesiologist who was experienced in performing airway ultrasound. Upper airway USG was performed with a commercially available ultrasound machine (SONOSITE-M™ SonoSite, Bothell, WA, USA). The linear ultrasound transducer of frequency 9–12 MHz was used to perform the study. The sonographer was blinded to the intubation done by the laryngoscopist. The sonographer and the laryngoscopist did not communicate with each other verbally or visually. The ultrasound probe was placed transversely on the neck anteriorly, superior to the suprasternal notch before intubation. Immediately after intubation, the transducer probe was used to visualise the endotracheal tube in the tracheal longitudinal and transverse views [Figures 1 and 2]. The probe was then moved to the left to look at the oesophagus to see whether it was empty or distended by ETT.
Figure 1.
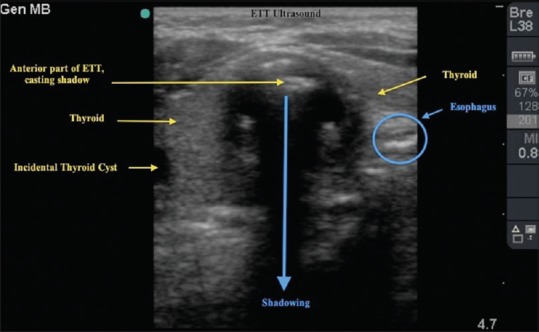
Ultrasound image after tracheal intubation showing posterior shadowing in trachea and oesophagus which is empty
Figure 2.
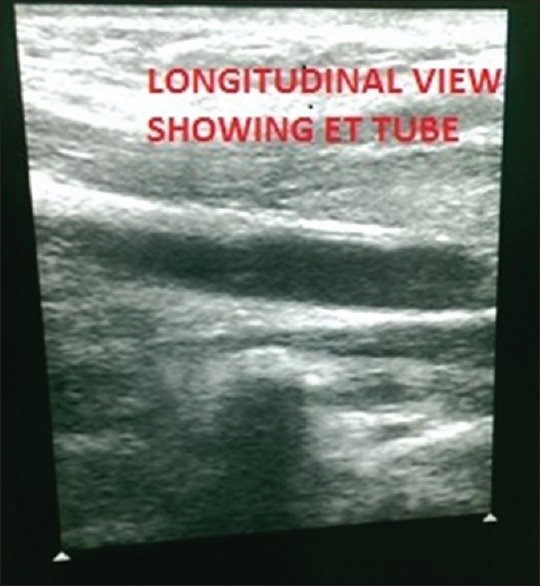
Ultrasound image after tracheal intubation in longitudinal view showing the presence of endotracheal tube
Data were entered into MS Excel and analysed in SPSS 24.0 IBM Analytic software (SPSS Inc., Chicago, Illinois, USA). Quantitative data were expressed as mean, range and standard deviation, whereas qualitative data were expressed as relative frequencies (n/N). We compared the number of tracheal intubations detected upper airway USG with that detected by capnography using the Chi-square test. Using kappa statistics, we determined the strength of agreement between airway upper airway USG and capnography. P < 0.05 was considered statistically significant. Confirmation times taken by the methods were noted. Both the methods (capnography and upper airway USG) were applied to all the patients in the group.
Sensitivity, specificity, positive and negative predictive values of airway upper airway USG were determined against capnography as the gold standard to confirm tracheal intubation.
RESULTS
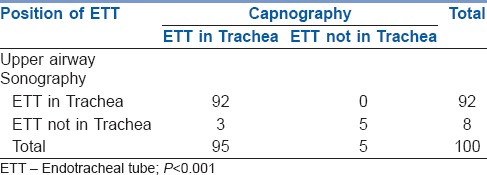
The mean distribution of age was 38.87 ± 11.969 years and mean weight 65.49 ± 13.78 kg. Out of the 100 intubated patients’ capnography was able to detect endotracheal intubation in 95 patients and oesophageal intubation in five patients. Upper airway USG also detected oesophageal placement of the ETT in those 5 patients. However, upper airway USG could not detect the ETT placement in three patients in whom a typical waveform was seen on capnography [P < 0.001, Table 1].
Table 1.
2 × 2 Table used to determine the sensitivity and specificity of upper airway ultrasonography in comparison to capnography
To detect tracheal intubation, upper airway USG had a sensitivity of 96.84% (95% CI: 94.25%–96.84%), specificity of 100% (95% CI: 50.6%–100%), positive predictive value of 100% (95% CI: 97.3%–100%) and negative predictive value of 62.5% (95% CI: 31.6%–62.5%) when compared with waveform capnography. Kappa value was 0.762 indicating a good agreement between upper airway USG and capnography in the confirmation of ETT placement.
Capnography took 8.99 ± 1.043 s for the confirmation of correct ETT placement, and upper airway USG took 12.0 ± 1.318 s for the confirmation of correct ETT placement. This difference of 3.01 s was highly significant (P < 0.001).
DISCUSSION
This study shows a good agreement, with a kappa value of 0.762, between upper airway ultrasound and waveform capnography and also quick mean confirmation times of both the methods (approximately, 9 s for capnography and 12 s for upper airway USG). Upper airway USG detected all five oesophageal intubations but did not detect three out of 95 tracheal intubations (false negatives). Therefore, this study suggests that upper airway USG may be used in the primary confirmation of endotracheal tube placement; it accurately identified oesophageal placement, but was less accurate in identifying tracheal intubation compared to capnography. Both techniques are time-saving, safe and faster than other techniques such as chest radiographs.[8] This study covers a variety of patients who differ significantly in age, weight and surgeries they underwent. Upper airway USG can be advantageous in situations involving low cardiac output, bronchoconstriction or other situations in which capnography or ETCO2 might be fallacious.[9] Thus, upper airway USG might be the method of choice in the primary verification of ETT location in upper airway in such conditions. Upper airway USG also has few disadvantages as seen in the study. Upper airway USG misidentified three tracheal intubations (three false negatives) which were identified as positive by waveform capnography. These subjects were found to be overweight or obese (118 kg, 82 kg and 86 kg) with more subcutaneous fat in the neck region which might have made identification of the hyperechoic comet tail shape, posterior shadowing in the transverse view difficult and therefore the ETT placement was not detected. Another limitation is that upper airway USG is operator dependent; hence its repeatability and generalisability needs to be further studied.
The rate of oesophageal intubation during the initial intubation was 5% (5 out of 100 cases). Upper airway USG detected all five oesophageal intubations which did not show any waveform on capnography. Therefore, upper airway USG was found to be 100% specific for diagnosing oesophageal intubation. The main strengths of our study are its prospective nature, and that a single operator performed all ultrasounds.
The sensitivity and specificity of upper airway USG for diagnosing tracheal intubation when referenced to capnography were 96.8% and 100%, respectively. This is similar to the results obtained by previous studies.[10,11,12,13,14,15] In our study, upper airway USG misidentified three cases (three false negatives) which were tested to be positive by capnography. In one study, two of the false negatives patients observed were found to have subcutaneous emphysema due to pneumothorax which made the identification of the two hyperechoic lines difficult.[9]
Our study also showed that upper airway USG and capnography have quick mean times of 12 s and 9 s respectively which is comparable to the results of the previous studies.[9,10,13]
The reliability of quantitative capnography is a suspect in some low pulmonary flow condition like cardiac arrest or severe shock. In such conditions, low pulmonary flow will not disturb upper airway USG images. Therefore, upper airway USG may be used in such conditions to confirm the ETT placement. After intubation, there are primary and secondary verifications of endotracheal tube. Primary verifications are defined as procedures performed before the endotracheal tube is secured. Our study showed that upper airway ultrasound is a direct method that visualises the upper airway structures in real time to identify endotracheal tube location. It also determines whether tube is in the trachea or the oesophagus after intubation. Capnography is also a direct method that detects the amount of carbon dioxide in the exhaled air. Our study showed that both the methods have a good accuracy, good correlation, good agreement and quick confirmation times.
Ultrasound is becoming very important in upper airway management especially in emergency settings.[11] This is because it is easy to carry, relatively cheap, has a proven record of safety, and does not cause pain.[14] Capnography is not always available in emergency settings and peripheral centres. In such settings, ultrasound can be used for the verification of ETT placement. In overweight and obese patients, upper airway USG has been shown to be superior to auscultation in speed and accuracy in detection of placement of endotracheal.[15]
CONCLUSION
Upper airway USG is as accurate as capnography in diagnosing oesophageal intubation. Both airway upper airway USG and capnography have good agreement and quick confirmation times, though capnography is about 3 s quicker. Both capnography and upper airway USG can be used as primary procedures for confirmation of ETT placement.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We are very thankful to Dr. Rajeshwar Rao, Consultant Anaesthesiologist at Department of Anaesthesia in Yashoda Hospital for his suggestion and guidance. We are also thankful to Mr. Murli Mohan Khetan for his help in statistical analysis. We gratefully acknowledge management of the hospital for their valuable support.
REFERENCES
- 1.Mort TC. Unplanned tracheal extubation outside the operating room: A quality improvement audit of hemodynamic and tracheal airway complications associated with emergency tracheal reintubation. Anesth Analg. 1998;86:1171–6. doi: 10.1097/00000539-199806000-00006. [DOI] [PubMed] [Google Scholar]
- 2.Cook TM, Woodall N, Frerk C. Fourth National Audit Project. Major complications of airway management in the UK: Results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: Anaesthesia. Br J Anaesth. 2011;106:617–31. doi: 10.1093/bja/aer058. [DOI] [PubMed] [Google Scholar]
- 3.Bozeman WP, Hexter D, Liang HK, Kelen GD. Esophageal detector device versus detection of end-tidal carbon dioxide level in emergency intubation. Ann Emerg Med. 1996;27:595–9. doi: 10.1016/s0196-0644(96)70162-2. [DOI] [PubMed] [Google Scholar]
- 4.Grmec S. Comparison of three different methods to confirm tracheal tube placement in emergency intubation. Intensive Care Med. 2002;28:701–4. doi: 10.1007/s00134-002-1290-x. [DOI] [PubMed] [Google Scholar]
- 5.Kundra P, Mishra SK, Ramesh A. Ultrasound of the airway. Indian J Anaesth. 2011;55:456–62. doi: 10.4103/0019-5049.89868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chou EH, Dickman E, Tsou PY, Tessaro M, Tsai YM, Ma MH, et al. Ultrasonography for confirmation of endotracheal tube placement: A systematic review and meta-analysis. Resuscitation. 2015;90:97–103. doi: 10.1016/j.resuscitation.2015.02.013. [DOI] [PubMed] [Google Scholar]
- 7.Chou H-C, Chong K-M, Sim S-S, Ma MH-M, Liu S-H, Chen N-C, et al. Real-time tracheal ultrasonography for confirmation of endotracheal tube placement during cardiopulmonary resuscitation. Resuscitation. 2013;84:1708–12. doi: 10.1016/j.resuscitation.2013.06.018. [DOI] [PubMed] [Google Scholar]
- 8.Chenkin J, McCartney CJ, Jelic T, Romano M, Heslop C, Bandiera G, et al. Defining the learning curve of point-of-care ultrasound for confirming endotracheal tube placement by emergency physicians. Crit Ultrasound J. 2015;7:14. doi: 10.1186/s13089-015-0031-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Adi O, Chuan TW, Rishya M. A feasibility study on bedside upper airway ultrasonography compared to waveform capnography for verifying endotracheal tube location after intubation. Crit Ultrasound J. 2013;5:7. doi: 10.1186/2036-7902-5-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Muslu B, Sert H, Kaya A, Demircioglu RI, Gozdemir M, Usta B, Boynukalin KS. Use of sonography for rapid identification of esophageal and tracheal intubations in adult patients. J Ultrasound Med. 2011;30:671–6. doi: 10.7863/jum.2011.30.5.671. [DOI] [PubMed] [Google Scholar]
- 11.Chou HC, Tseng WP, Wang CH, Ma MH, Wang HP, Huang PC, et al. Tracheal rapid ultrasound exam (T.R.U.E) for confirming endotracheal tube placement during emergency intubation. Resuscitation. 2011;82:1279–84. doi: 10.1016/j.resuscitation.2011.05.016. [DOI] [PubMed] [Google Scholar]
- 12.Takeda T, Tanigawa K, Tanaka H, Hayashi Y, Goto E, Tanaka K. The assessment of three methods to verify tracheal tube placement in the emergency setting. Resuscitation. 2003;56:153–7. doi: 10.1016/s0300-9572(02)00345-3. [DOI] [PubMed] [Google Scholar]
- 13.Werner SL, Smith CE, Goldstein JR, Jones RA, Cydulka RK. Pilot study to evaluate the accuracy of ultrasonography in confirming endotracheal tube placement. Ann Emerg Med. 2007;49:75–80. doi: 10.1016/j.annemergmed.2006.07.004. [DOI] [PubMed] [Google Scholar]
- 14.Sustic A. Role of ultrasound in the airway management of critically ill patients. Crit Care Med. 2007;35(5 Suppl):S173–7. doi: 10.1097/01.CCM.0000260628.88402.8A. [DOI] [PubMed] [Google Scholar]
- 15.Rajan S, Surendran J, Paul J, Kumar L. Rapidity and efficacy of ultrasonographic sliding lung sign and auscultation in confirming endotracheal intubation in overweight and obese patients. Indian J Anaesth. 2017;61:230–4. doi: 10.4103/0019-5049.202164. [DOI] [PMC free article] [PubMed] [Google Scholar]